Impact of Long-Term Supplementation with Fish Oil in Individuals with Non-Alcoholic Fatty Liver Disease: A Double Blind Randomized Placebo Controlled Clinical Trial


 , and
, and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Interventions
2.3. Transient Hepatic Elastography
2.4. Sample Collection
2.5. Biochemical Tests
2.6. RNA Extraction, Real-Time PCR, and miR-122 Relative Expression
2.7. Assessment of Fatty Acid Composition of Red Blood Cells (RBC)
2.8. Anthropometric Assessment
2.9. Statistical Analysis
3. Results
3.1. Baseline Characteristics of the Subjects
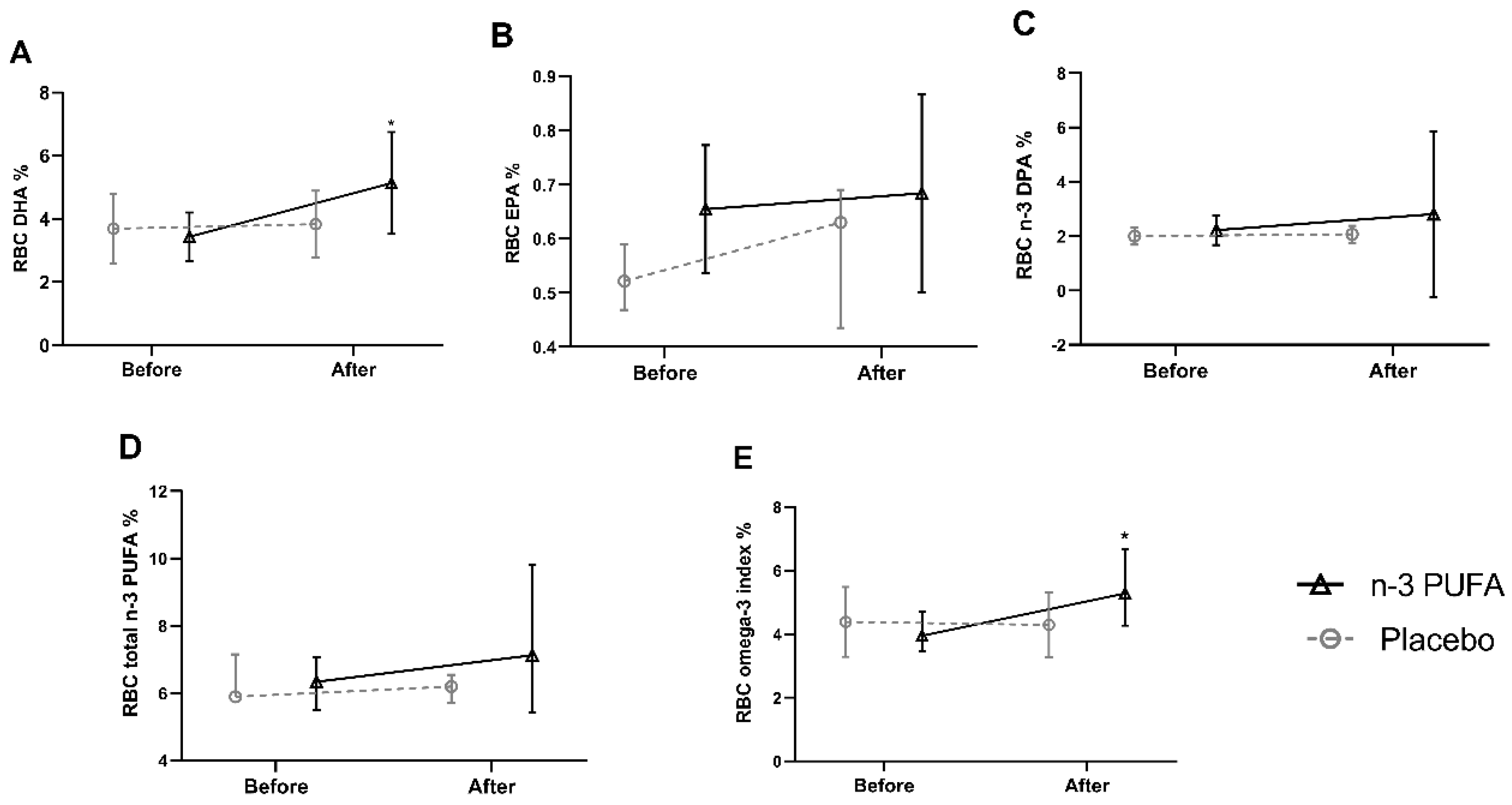
3.2. n-3 PUFA in RBC
3.3. Anthropometric, Biochemical, and Clinical Data
3.4. Evaluation of the Effects of Intervention on Circulating miR-122 Expression
4. Discussion
Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Younossi, Z.M.; Koenig, A.B.; Abdelatif, D.; Fazel, Y.; Henry, L.; Wymer, M. Global epidemiology of nonalcoholic fatty liver disease—Meta-analytic assessment of prevalence, incidence, and outcomes. Hepatology 2016, 64, 73–84. [Google Scholar] [CrossRef] [Green Version]
- Ekstedt, M.; Hagström, H.; Nasr, P.; Fredrikson, M.; Stål, P.; Kechagias, S.; Hultcrantz, R. Fibrosis stage is the strongest predictor for disease-specific mortality in NAFLD after up to 33 years of follow-up. Hepatology 2015, 61, 1547–1554. [Google Scholar] [CrossRef] [Green Version]
- Buzzetti, E.; Pinzani, M.; Tsochatzis, E.A. The multiple-hit pathogenesis of non-alcoholic fatty liver disease (NAFLD). Metabolism 2016, 65, 1038–1048. [Google Scholar] [CrossRef] [PubMed]
- Cansanção, K.; Monteiro, L.S.; Leite, N.C.; Dávalos, A.; Do Carmo, M.D.G.T.; Ferreira Peres, W.A. Advanced liver fibrosis is independently associated with palmitic acid and insulin levels in patients with non-alcoholic fatty liver disease. Nutrients 2018, 10, 1586. [Google Scholar] [CrossRef] [Green Version]
- Yasutake, K.; Kohjima, M.; Kotoh, K.; Nakashima, M.; Nakamuta, M.; Enjoji, M. Dietary habits and behaviors associated with nonalcoholic fatty liver disease. World J. Gastroenterol. 2014, 20, 1756–1767. [Google Scholar] [CrossRef] [PubMed]
- Dudekula, A.; Rachakonda, V.; Shaik, B.; Behari, J. Weight loss in nonalcoholic fatty liver disease patients in an ambulatory care setting is largely unsuccessful but correlates with frequency of clinic visits. PLoS ONE 2014, 9, e111808. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cicero, A.F.G.; Colletti, A.; Bellentani, S. Nutraceutical approach to non-alcoholic fatty liver disease (NAFLD): The available clinical evidence. Nutrients 2018, 10, 1153. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saeed, N.M.; Mansour, A.M.; Allam, S. Lycopene induces insulin signaling and alleviates fibrosis in experimental model of non-alcoholic fatty liver disease in rats. PharmaNutrition 2020, 14, 100225. [Google Scholar] [CrossRef]
- Sofi, F.; Giangrandi, I.; Cesari, F.; Corsani, I.; Abbate, R.; Gensini, G.F.; Casini, A. Effects of a 1-year dietary intervention with n-3 polyunsaturated fatty acid-enriched olive oil on non-alcoholic fatty liver disease patients: A preliminary study. Int. J. Food Sci. Nutr. 2010, 61, 792–802. [Google Scholar] [CrossRef]
- Zhu, F.S.; Liu, S.; Chen, X.M.; Huang, Z.G.; Zhang, D.W. Effects of n-3 polyunsaturated fatty acids from seal oils on nonalcoholic fatty liver disease associated with hyperlipidemia. World J. Gastroenterol. 2008, 14, 6395–6400. [Google Scholar] [CrossRef]
- Capanni, M.; Calella, F.; Biagini, M.R.; Genise, S.; Raimondi, L.; Bedogni, G.; Svegliati-Baroni, G.; Sofi, F.; Milani, S.; Abbate, R.; et al. Prolonged n-3 polyunsaturated fatty acid supplementation ameliorates hepatic steatosis in patients with non-alcoholic fatty liver disease: A pilot study. Aliment. Pharmacol. Ther. 2006, 23, 1143–1151. [Google Scholar] [CrossRef]
- Qin, Y.; Zhou, Y.; Chen, S.H.; Zhao, X.L.; Ran, L.; Zeng, X.L.; Wu, Y.; Chen, J.L.; Kang, C.; Shu, F.R.; et al. Fish oil supplements lower serum lipids and glucose in correlation with a reduction in plasma fibroblast growth factor 21 and prostaglandin E2 in nonalcoholic fatty liver disease associated with hyperlipidemia: A randomized clinical trial. PLoS ONE 2015, 10, e0133496. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, N.; Sano, K.; Horiuchi, A.; Tanaka, E.; Kiyosawa, K.; Aoyama, T. Highly purified eicosapentaenoic acid treatment improves nonalcoholic steatohepatitis. J. Clin. Gastroenterol. 2008, 42, 413–418. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Spadaro, L.; Magliocco, O.; Spampinato, D.; Piro, S.; Oliveri, C.; Alagona, C.; Papa, G.; Rabuazzo, A.M.; Purrello, F. Effects of n-3 polyunsaturated fatty acids in subjects with nonalcoholic fatty liver disease. Dig. Liver Dis. 2008, 40, 194–199. [Google Scholar] [CrossRef] [PubMed]
- Tobin, D.; Brevik-Andersen, M.; Qin, Y.; Innes, J.K.; Calder, P.C. Evaluation of a high concentrate omega-3 for correcting the omega-3 fatty acid nutritional deficiency in non-alcoholic fatty liver disease (CONDIN). Nutrients 2018, 10, 1126. [Google Scholar] [CrossRef] [Green Version]
- Li, Y.H.; Yang, L.H.; Sha, K.H.; Liu, T.G.; Zhang, L.G.; Liu, X.X. Efficacy of poly-unsaturated fatty acid therapy on patients with nonalcoholic steatohepatitis. World J. Gastroenterol. 2015, 21, 7008–7013. [Google Scholar] [CrossRef]
- Scorletti, E.; Byrne, C.D. Omega-3 fatty acids, hepatic lipid metabolism, and nonalcoholic fatty liver disease. Annu. Rev. Nutr. 2013, 33, 231–248. [Google Scholar] [CrossRef]
- Wang, H.; Shao, Y.; Yuan, F.; Feng, H.; Li, N.; Zhang, H.; Wu, C.; Liu, Z. Fish oil feeding modulates the expression of hepatic MicroRNAs in a western-style diet-induced nonalcoholic fatty liver disease rat model. Biomed. Res. Int. 2017, 2017, 2503847. [Google Scholar] [CrossRef] [Green Version]
- Yip, P.K.; Bowes, A.L.; Hall, J.C.E.; Burguillos, M.A.; Richard Ip, T.H.; Baskerville, T.; Liu, Z.H.; Mohamed, M.A.E.K.; Getachew, F.; Lindsay, A.D.; et al. Docosahexaenoic acid reduces microglia phagocytic activity via miR-124 and induces neuroprotection in rodent models of spinal cord contusion injury. Hum. Mol. Genet. 2019, 28, 2427–2448. [Google Scholar] [CrossRef]
- Choi, J.E.; Kim, E.Y.; Park, Y. N-3 PUFA improved pup separation-induced postpartum depression via serotonergic pathway regulated by miRNA. J. Nutr. Biochem. 2020, 84, 108417. [Google Scholar] [CrossRef]
- Dongiovanni, P.; Meroni, M.; Longo, M.; Fargion, S.; Fracanzani, A.L. MiRNA signature in NAFLD: A turning point for a non-invasive diagnosis. Int. J. Mol. Sci. 2018, 19, 3966. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gjorgjieva, M.; Sobolewski, C.; Dolicka, D.; Correia De Sousa, M.; Foti, M. MiRNAs and NAFLD: From pathophysiology to therapy. Gut 2019, 68, 2065–2079. [Google Scholar] [CrossRef] [PubMed]
- Lagos-Quintana, M.; Rauhut, R.; Yalcin, A.; Meyer, J.; Lendeckel, W.; Tuschl, T. Identification of tissue-specific microRNAs from mouse. Curr. Biol. 2002, 12, 735–739. [Google Scholar] [CrossRef] [Green Version]
- Jampoka, K.; Muangpaisarn, P.; Khongnomnan, K.; Treeprasertsuk, S.; Tangkijvanich, P.; Payungporn, S. Serum miR-29a and miR-122 as Potential Biomarkers for Non-Alcoholic Fatty Liver Disease (NAFLD). MicroRNA 2018, 7, 215–222. [Google Scholar] [CrossRef]
- Esau, C.; Davis, S.; Murray, S.F.; Yu, X.X.; Pandey, S.K.; Pear, M.; Watts, L.; Booten, S.L.; Graham, M.; McKay, R.; et al. miR-122 regulation of lipid metabolism revealed by in vivo antisense targeting. Cell Metab. 2006, 3, 87–98. [Google Scholar] [CrossRef] [Green Version]
- Hendy, O.M.; Rabie, H.; El Fouly, A.; Abdel-Samiee, M.; Abdelmotelb, N.; Elshormilisy, A.A.; Allam, M.; Ali, S.T.; Mohamed, N.; El-Deen, B.; et al. The circulating micro-RNAs (−122, −34a and −99a) as predictive biomarkers for non-alcoholic fatty liver diseases. Diabetes Metab. Syndr. Obes. Targets Ther. 2019, 12, 2715–2723. [Google Scholar] [CrossRef] [Green Version]
- Tan, Y.; Ge, G.; Pan, T.; Wen, D.; Gan, J. A pilot study of serum micrornas panel as potential biomarkers for diagnosis of nonalcoholic fatty liver disease. PLoS ONE 2014, 9, e105192. [Google Scholar] [CrossRef] [Green Version]
- Miyaaki, H.; Ichikawa, T.; Kamo, Y.; Taura, N.; Honda, T.; Shibata, H.; Milazzo, M.; Fornari, F.; Gramantieri, L.; Bolondi, L.; et al. Significance of serum and hepatic microRNA-122 levels in patients with non-alcoholic fatty liver disease. Liver Int. 2014, 34, e302–e307. [Google Scholar] [CrossRef]
- Ye, D.; Zhang, T.; Lou, G.; Xu, W.; Dong, F.; Chen, G.; Liu, Y. Plasma miR-17, miR-20a, miR-20b and miR-122 as potential biomarkers for diagnosis of NAFLD in type 2 diabetes mellitus patients. Life Sci. 2018, 208, 201–207. [Google Scholar] [CrossRef]
- Eddowes, P.J.; Sasso, M.; Allison, M.; Tsochatzis, E.; Anstee, Q.M.; Sheridan, D.; Guha, I.N.; Cobbold, J.F.; Deeks, J.J.; Paradis, V.; et al. Accuracy of FibroScan Controlled Attenuation Parameter and Liver Stiffness Measurement in Assessing Steatosis and Fibrosis in Patients With Nonalcoholic Fatty Liver Disease. Gastroenterology 2019, 156, 1717–1730. [Google Scholar] [CrossRef] [Green Version]
- López de las Hazas, M.C.; Gil-Zamorano, J.; Cofán, M.; Mantilla-Escalante, D.C.; Garcia-Ruiz, A.; del Pozo-Acebo, L.; Pastor, O.; Yañez-Mo, M.; Mazzeo, C.; Serra-Mir, M.; et al. One-year dietary supplementation with walnuts modifies exosomal miRNA in elderly subjects. Eur. J. Nutr. 2020, 59, 1–13. [Google Scholar] [CrossRef]
- American Oil Chemists’ Society (AOCS) Official Method Ce 2c-11. Direct Methylation of Lipids in Foods by Acid-Alkali. In Official Methods and Recommended Practices of the AOCS; AOCS: Urbana, IL, USA, 2017. [Google Scholar]
- Assumpção, R.P.; Mucci, D.B.; Fonseca, F.C.P.; Marcondes, H.; Sardinha, F.L.C.; Citelli, M.; Tavares do Carmo, M.G. Fatty acid profile of maternal and fetal erythrocytes and placental expression of fatty acid transport proteins in normal and intrauterine growth restriction pregnancies. Prostaglandins Leukot. Essent. Fat. Acids 2017, 125, 24–31. [Google Scholar] [CrossRef]
- Lohman, T.G.; Roche, A.F.; Martorell, R. (Eds.) Anthropometric Standardization Reference Manual; Human Kinetics Books: Champaign, IL, USA, 1988; ISBN 9780873221214. [Google Scholar]
- Bergman, R.N.; Stefanovski, D.; Buchanan, T.A.; Sumner, A.E.; Reynolds, J.C.; Sebring, N.G.; Xiang, A.H.; Watanabe, R.M. A better index of body adiposity. Obesity 2011, 19, 1083–1089. [Google Scholar] [CrossRef] [PubMed]
- Nobili, V.; Carpino, G.; Alisi, A.; De Vito, R.; Franchitto, A.; Alpini, G.; Onori, P.; Gaudio, E. Role of docosahexaenoic acid treatment in improving liver histology in pediatric nonalcoholic fatty liver disease. PLoS ONE 2014, 9, e88005. [Google Scholar] [CrossRef] [PubMed]
- Pacifico, L.; Bonci, E.; Di Martino, M.; Versacci, P.; Andreoli, G.; Silvestri, L.M.; Chiesa, C. A double-blind, placebo-controlled randomized trial to evaluate the efficacy of docosahexaenoic acid supplementation on hepatic fat and associated cardiovascular risk factors in overweight children with nonalcoholic fatty liver disease. Nutr. Metab. Cardiovasc. Dis. 2015, 25, 734–741. [Google Scholar] [CrossRef]
- Parker, H.M.; O’Connor, H.T.; Keating, S.E.; Cohn, J.S.; Garg, M.L.; Caterson, I.D.; George, J.; Johnson, N.A. Efficacy of the Omega-3 Index in predicting non-alcoholic fatty liver disease in overweight and obese adults: A pilot study. Br. J. Nutr. 2015, 114, 780–787. [Google Scholar] [CrossRef] [Green Version]
- Kwo, P.Y.; Cohen, S.M.; Lim, J.K. ACG Clinical Guideline: Evaluation of Abnormal Liver Chemistries. Am. J. Gastroenterol. 2017, 112, 18–35. [Google Scholar] [CrossRef]
- Vimalraj, S. Alkaline phosphatase: Structure, expression and its function in bone mineralization. Gene 2020, 754, 144855. [Google Scholar] [CrossRef]
- Zhou, Y.J.; Zou, H.; Zheng, J.N.; Zou, T.T.; Vitale, A.; Miele, L.; Van Poucke, S.; Liu, W.Y.; Shen, S.; Zhang, D.C.; et al. Serum alkaline phosphatase, a risk factor for non-alcoholic fatty liver, but only for women in their 30s and 40s: Evidence from a large cohort study. Expert Rev. Gastroenterol. Hepatol. 2017, 11, 269–276. [Google Scholar] [CrossRef]
- Kocabay, G.; Telci, A.; Tutuncu, Y.; Tiryaki, B.; Ozel, S.; Çevikbaş, U.; Okten, A.; Satman, I. Alkaline phosphatase: Can it be considered as an indicator of liver fibrosis in non-alcoholic steatohepatitis with type 2 diabetes? Bratisl Lek List. 2011, 112, 626–629. [Google Scholar]
- Okamoto, K.; Koda, M.; Okamoto, T.; Onoyama, T.; Miyoshi, K.; Kishina, M.; Matono, T.; Kato, J.; Tokunaga, S.; Sugihara, T.; et al. Serum miR-379 expression is related to the development and progression of hypercholesterolemia in non-alcoholic fatty liver disease. PLoS ONE 2020, 15, e0219412. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tovo, C.V.; Villela-Nogueira, C.A.; Leite, N.C.; Panke, C.L.; Port, G.Z.; Fernandes, S.; Buss, C.; Coral, G.P.; Cardoso, A.C.; Cravo, C.M.; et al. Transient hepatic elastography has the best performance to evaluate liver fibrosis in non-alcoholic fatty liver disease (NAFLD). Ann. Hepatol. 2019, 18, 445–449. [Google Scholar] [CrossRef] [PubMed]
- Oeda, S.; Takahashi, H.; Imajo, K.; Seko, Y.; Ogawa, Y.; Moriguchi, M.; Yoneda, M.; Anzai, K.; Aishima, S.; Kage, M.; et al. Accuracy of liver stiffness measurement and controlled attenuation parameter using FibroScan® M/XL probes to diagnose liver fibrosis and steatosis in patients with nonalcoholic fatty liver disease: A multicenter prospective study. J. Gastroenterol. 2020, 55, 428–440. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Yang, X.; Shi, H.; Dong, L.; Bai, J. Effect of α-linolenic acid on endoplasmic reticulum stress-mediated apoptosis of palmitic acid lipotoxicity in primary rat hepatocytes. Lipids Health Dis. 2011, 10, 122. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baselga-Escudero, L.; Blade, C.; Ribas-Latre, A.; Casanova, E.; Suárez, M.; Torres, J.L.; Salvadó, M.J.; Arola, L.; Arola-Arnal, A. Resveratrol and EGCG bind directly and distinctively to miR-33a and miR-122 and modulate divergently their levels in hepatic cells. Nucleic Acids Res. 2014, 42, 882–892. [Google Scholar] [CrossRef] [Green Version]
- de Sousa, M.C.; Gjorgjieva, M.; Dolicka, D.; Sobolewski, C.; Foti, M. Deciphering miRNAs’ action through miRNA editing. Int. J. Mol. Sci. 2019, 20, 6249. [Google Scholar] [CrossRef] [Green Version]
- Baranova, A.; Maltseva, D.; Tonevitsky, A. Adipose may actively delay progression of NAFLD by releasing tumor-suppressing, anti-fibrotic miR-122 into circulation. Obes. Rev. 2019, 20, 108–118. [Google Scholar] [CrossRef] [Green Version]
- Yamada, H.; Suzuki, K.; Ichino, N.; Ando, Y.; Sawada, A.; Osakabe, K.; Sugimoto, K.; Ohashi, K.; Teradaira, R.; Inoue, T.; et al. Associations between circulating microRNAs (miR-21, miR-34a, miR-122 and miR-451) and non-alcoholic fatty liver. Clin. Chim. Acta 2013, 424, 99–103. [Google Scholar] [CrossRef]
- Cheung, O.; Puri, P.; Eicken, C.; Contos, M.J.; Mirshahi, F.; Maher, J.W.; Kellum, J.M.; Min, H.; Luketic, V.A.; Sanyal, A.J. Nonalcoholic steatohepatitis is associated with altered hepatic MicroRNA expression. Hepatology 2008, 48, 1810–1820. [Google Scholar] [CrossRef] [Green Version]
- Vogt, J.; Sheinson, D.; Katavolos, P.; Irimagawa, H.; Tseng, M.; Alatsis, K.R.; Proctor, W.R. Variance component analysis of circulating miR-122 in serum from healthy human volunteers. PLoS ONE 2019, 14, e0220406. [Google Scholar] [CrossRef] [Green Version]
- Church, R.J.; Kullak-Ublick, G.A.; Aubrecht, J.; Bonkovsky, H.L.; Chalasani, N.; Fontana, R.J.; Goepfert, J.C.; Hackman, F.; King, N.M.P.; Kirby, S.; et al. Candidate biomarkers for the diagnosis and prognosis of drug-induced liver injury: An international collaborative effort. Hepatology 2019, 69, 760–773. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Variables | Placebo Group (n = 11) | n-3 PUFA Group (n = 13) | p Value | ||
|---|---|---|---|---|---|
| Sex, M/F | 8/3 | 9/4 | 0.851 | ||
| Age, yr | 55.00 | 52.00–74.00 | 62.00 | 52.00–68.00 | 0.910 |
| BMI (kg/m2) | 31.20 | 28.82–35.19 | 29.62 | 26.60–35.79 | 0.691 |
| WC (cm) | 104.90 | 98.00–112.50 | 109.00 | 91.50–116.00 | 0.955 |
| BAI | 34.62 | 30.60–40.12 | 39.31 | 32.05–42.20 | 0.277 |
| WHtR | 0.63 | 0.57–0.65 | 0.68 | 0.55–0.72 | 0.820 |
| ALT (U/L) | 30.00 | 22.00–32.00 | 24.00 | 16.00–41.00 | 0.494 |
| AST (U/L) | 20.00 | 18.00–24.00 | 27.00 | 16.00–33.00 | 0.531 |
| GGT (U/L) | 42.00 | 26.00–62.00 | 53.00 | 35.00–88.00 | 0.150 |
| ALP (U/L) | 78.00 | 52.00–114.00 | 92.00 | 58.00–140 | 0.392 |
| Fasting glucose (mg/dL) | 147.00 | 96.00–186.00 | 100.00 | 96.00–146.00 | 0.167 |
| HbA1c % | 7.30 | 5.90–8.20 | 7.20 | 5.80–7.70 | 0.608 |
| TC (mg/dL) | 187.00 | 146.00–203.00 | 197.00 | 155.00–247.00 | 0.252 |
| LDL (mg/dL) | 91.00 | 62.00–125.00 | 87.00 | 72.00–160.00 | 0.531 |
| HDL (mg/dL) | 46.00 | 40.00–49.00 | 47.00 | 39.00–59.00 | 0.608 |
| TG (mg/dL) | 166.00 | 104.00–260.00 | 182.00 | 121.00–241.00 | 1.000 |
| CAP baseline (dB/m) | 271.00 | 239.00–334.00 | 330.00 | 281.00–369.00 | 0.167 |
| Liver fibrosis (kPa) | 5.00 | 4.00–5.60 | 6.00 | 5.00–7.00 | 0.072 |
| Placebo Group (n = 11) | n-3 PUFA Group (n = 13) | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Variables | Baseline | Post-Treatment | p Value | Baseline | Post-Treatment | p Value | ||||
| Median | IQR | Median | IQR | Median | IQR | Median | IQR | |||
| BMI (kg/m2) | 31.20 | 28.82–31.19 | 31.39 | 27.76–35.17 | 0.799 | 32.89 | 28.26–37.18 | 32.84 | 28.27–37.17 | 0.917 |
| WC (cm) | 104.90 | 98.00–112.50 | 105.00 | 97.50–113.00 | 0.476 | 111.00 | 93.00–116.25 | 99.50 | 92.50–120.00 | 0.906 |
| BAI | 34.62 | 30.60–40.12 | 35.11 | 31.41–39.44 | 0.130 | 39.85 | 34.02–44.31 | 38.86 | 33.48–44.93 | 0.432 |
| WHtR | 0.63 | 0.57–0.65 | 0.64 | 0.56–0.66 | 0.633 | 0.69 | 0.56–0.72 | 0.66 | 0.55–0.73 | 0.751 |
| ALT (U/L) | 30.00 | 22.00–32.00 | 31.00 | 22.00–39.00 | 0.540 | 30.00 | 18.50–42.50 | 35.50 | 17.00–42.00 | 0.753 |
| AST (U/L) | 20.00 | 18.00–24.00 | 24.00 | 17.00–25.00 | 0.644 | 30.00 | 17.00–33.50 | 29.00 | 21.00–32.50 | 0.889 |
| GGT (U/L) | 42.00 | 26.00–62.00 | 34.00 | 22.00–45.00 | 0.139 | 50.00 | 35.50–70.00 | 42.50 | 30.00–57.00 | 0.382 |
| ALP (U/L) | 78.00 | 52.00–114.00 | 61.00 | 47.00–79.00 | 0.333 | 93.00 | 70.50–157.50 | 57.00 | 44.75–73.50 | 0.002 * |
| Fasting glucose (mg/dL) | 147.00 | 96.00–186.00 | 108.00 | 100.00–147.00 | 0.102 | 100.00 | 96.00–143.50 | 119.50 | 89.50–157.00 | 0.132 |
| HbA1c % | 7.30 | 5.90–8.20 | 6.90 | 6.20–7.70 | 0.332 | 6.30 | 5.80–7.75 | 6.60 | 5.90–8.84 | 0.694 |
| TC (mg/dL) | 187.00 | 146.00–203.00 | 155.00 | 144.00–182.00 | 0.445 | 197.00 | 152.50–247.50 | 167.50 | 131.25–180.00 | 0.115 |
| LDL (mg/dL) | 91.00 | 62.00–125.00 | 79.00 | 67.00–95.00 | 0.445 | 87.00 | 74.50–160.50 | 84.50 | 63.25–92.50 | 0.162 |
| HDL (mg/dL) | 46.00 | 40.00–49.00 | 46.00 | 36.00–51.00 | 0.474 | 47.00 | 41.50–59.50 | 45.50 | 42.00-–52.00 | 0.238 |
| TG (mg/dL) | 166.00 | 104.00–260.00 | 126.00 | 119.00–224.00 | 0.203 | 168.00 | 118.00–226.50 | 147.50 | 91.75–192.50 | 0.208 |
| CAP (dBm/min) | 271.00 | 239.00–334.00 | 310.00 | 267.00–354.00 | 0.374 | 330.00 | 281.00–369.50 | 313.00 | 251.00–337.00 | 0.060 |
| Liver fibrosis (kPa) | 5.00 | 4.00–5.60 | 5.60 | 4.40–6.20 | 0.211 | 6.80 | 5.60–7.60 | 6.10 | 4.55–7.40 | 0.039 * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cansanção, K.; Citelli, M.; Carvalho Leite, N.; López de las Hazas, M.-C.; Dávalos, A.; Tavares do Carmo, M.d.G.; Peres, W.A.F. Impact of Long-Term Supplementation with Fish Oil in Individuals with Non-Alcoholic Fatty Liver Disease: A Double Blind Randomized Placebo Controlled Clinical Trial. Nutrients 2020, 12, 3372. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12113372
Cansanção K, Citelli M, Carvalho Leite N, López de las Hazas M-C, Dávalos A, Tavares do Carmo MdG, Peres WAF. Impact of Long-Term Supplementation with Fish Oil in Individuals with Non-Alcoholic Fatty Liver Disease: A Double Blind Randomized Placebo Controlled Clinical Trial. Nutrients. 2020; 12(11):3372. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12113372
Chicago/Turabian StyleCansanção, Kátia, Marta Citelli, Nathalie Carvalho Leite, María-Carmen López de las Hazas, Alberto Dávalos, Maria das Graças Tavares do Carmo, and Wilza Arantes Ferreira Peres. 2020. "Impact of Long-Term Supplementation with Fish Oil in Individuals with Non-Alcoholic Fatty Liver Disease: A Double Blind Randomized Placebo Controlled Clinical Trial" Nutrients 12, no. 11: 3372. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12113372