Association between Serum Vitamin B12 and Global DNA Methylation in Colorectal Cancer Patients

 , , ,
, , ,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Biochemical Determinations
2.3. DNA Extraction from Biological Samples, Bisulfite Reaction, and Pyrosequencing
2.4. Statistical Analysis
3. Results
3.1. General Characteristics of CRC Patients by Serum Vitamin B12 Status
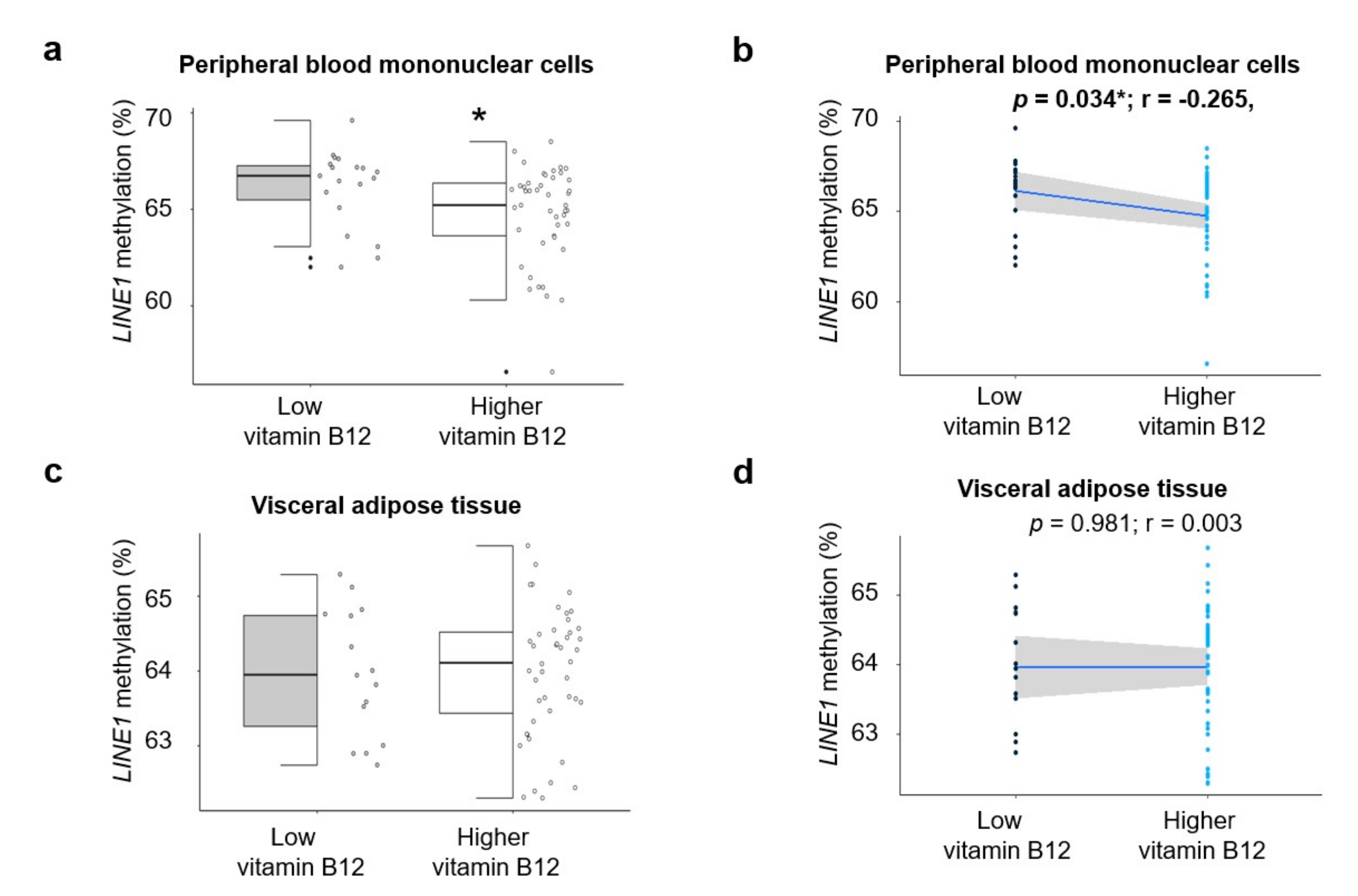
3.2. Association between Global Methylation Study (LINE1) and Circulating Levels of Vitamin B12 in CRC Patients
3.3. Association between Methylation of LINE1 and Biochemical Variables According to the 25th Percentile of Vitamin B12
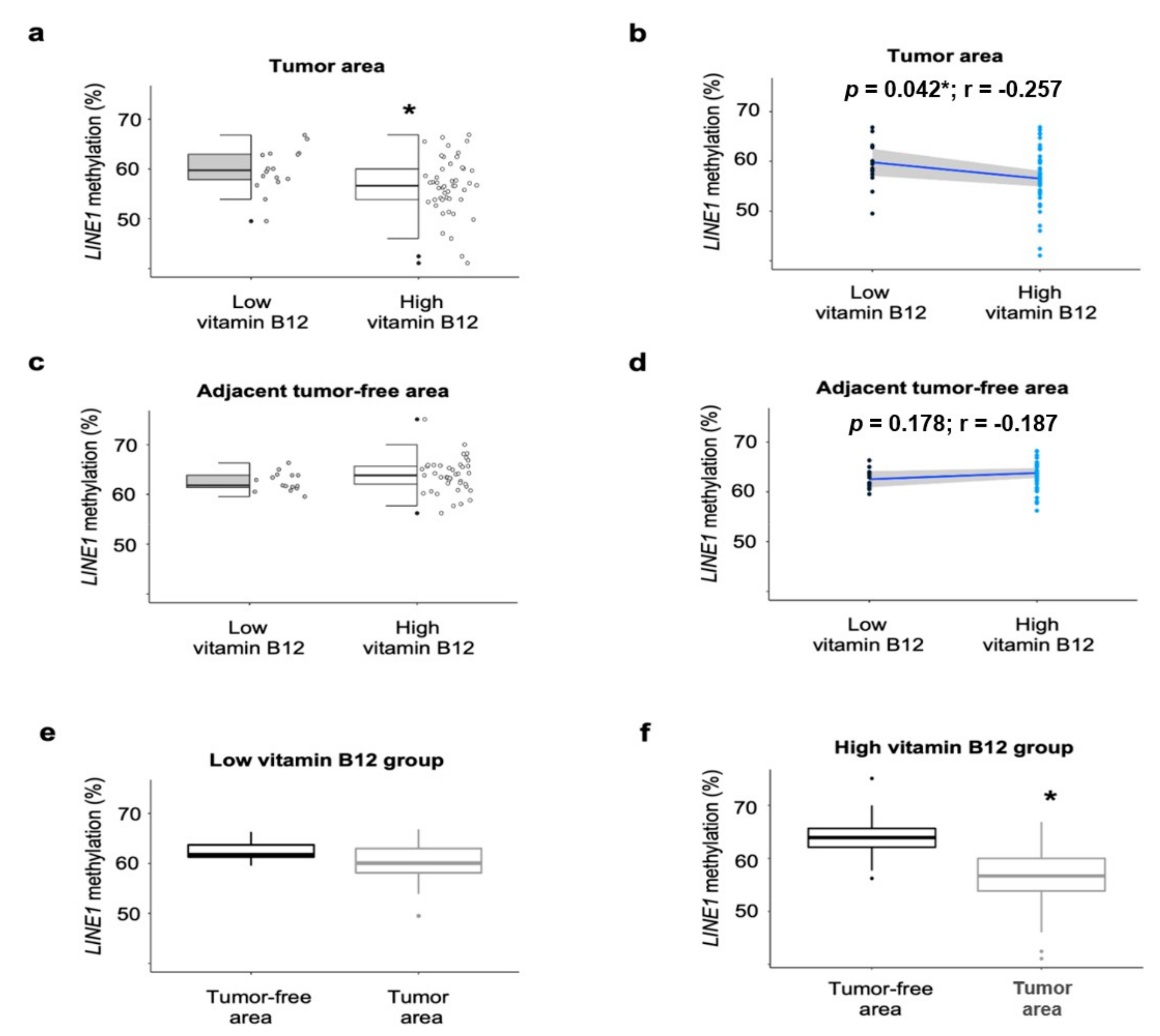
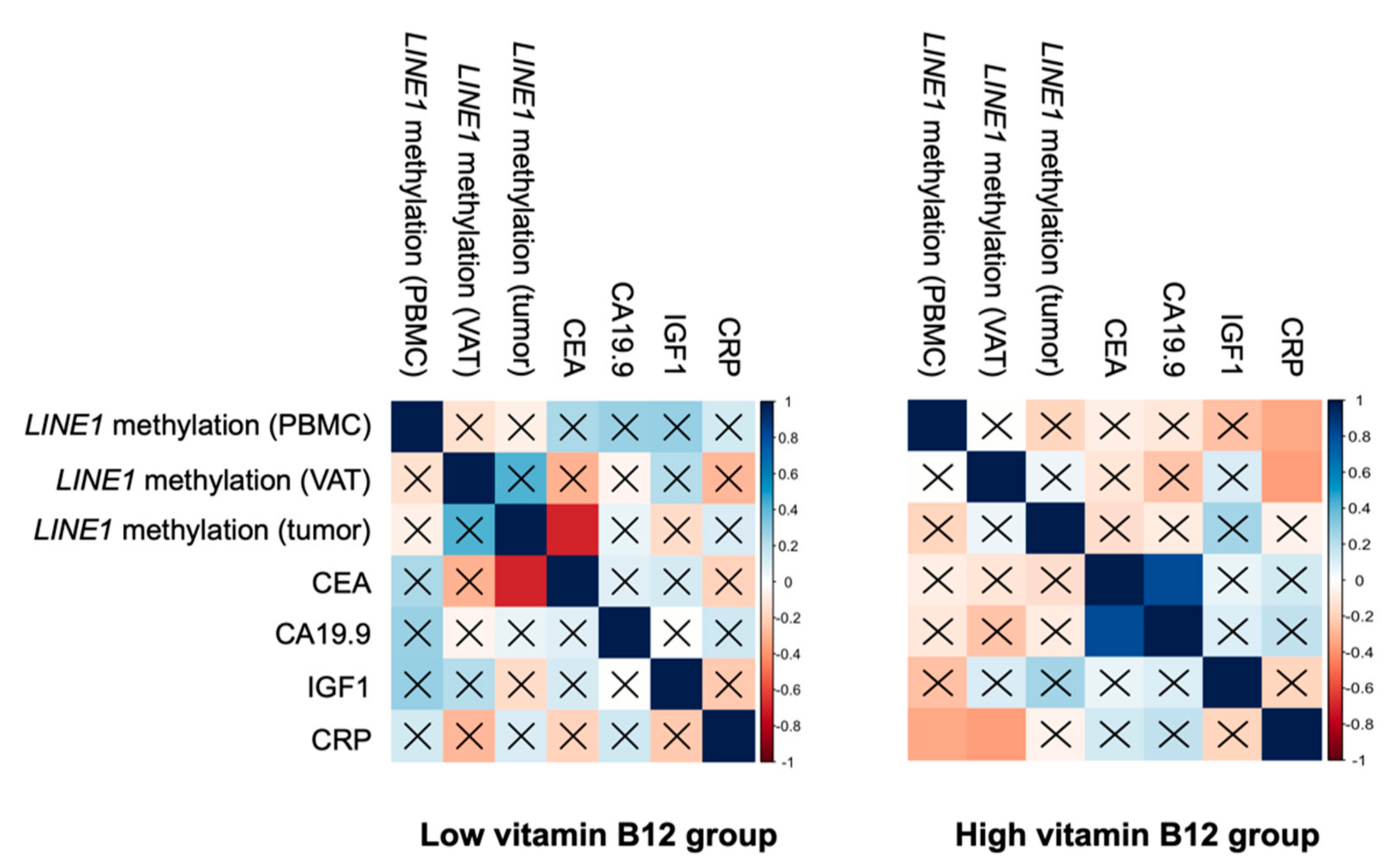
3.4. Association between Methylation of LINE1 and Tumoral and Inflammatory Markers According to the Circulating Levels of Vitamin B12
3.5. Regression Analyses between Methylation of LINE1 and Vitamin B12
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Wagner, C. Biochemical role of folate in cellular metabolism. Clin. Res. Regul. Aff. 2001, 18, 161–180. [Google Scholar] [CrossRef]
- Brunaud, L.; Alberto, J.-M.; Ayav, A.; Gérard, P.; Namour, F.; Antunes, L.; Braun, M.; Bronowicki, J.-P.; Bresler, L.; Guéant, J.-L. Effects of Vitamin B12 and Folate Deficiencies on DNA Methylation and Carcinogenesis in Rat Liver. Clin. Chem. Lab. Med. 2003, 41, 1012–1019. [Google Scholar] [CrossRef]
- Amenyah, S.D.; Hughes, C.F.; Ward, M.; Rosborough, S.; Deane, J.; Thursby, S.-J.; Walsh, C.P.; Kok, D.E.; Strain, J.J.; McNulty, H.; et al. Influence of nutrients involved in one-carbon metabolism on DNA methylation in adults—A systematic review and meta-analysis. Nutr. Rev. 2020, 78, 647–666. [Google Scholar] [CrossRef] [PubMed]
- Yadav, D.K.; Shrestha, S.; Lillycrop, K.A.; Joglekar, C.V.; Pan, H.; Holbrook, J.D.; Fall, C.H.; Yajnik, C.S.; Chandak, G.R. Vitamin B12supplementation influences methylation of genes associated with Type 2 diabetes and its intermediate traits. Epigenomics 2018, 10, 71–90. [Google Scholar] [CrossRef] [PubMed]
- Kok, D.E.G.; Dhonukshe-Rutten, R.A.M.; Lute, C.; Heil, S.G.; Uitterlinden, A.G.; Van Der Velde, N.; Van Meurs, J.B.J.; Van Schoor, N.M.; Hooiveld, G.J.E.J.; De Groot, L.C.P.G.M.; et al. The effects of long-term daily folic acid and vitamin B12 supplementation on genome-wide DNA methylation in elderly subjects. Clin. Epigenetics 2015, 7, 1–14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mandaviya, P.R.; Joehanes, R.; Brody, J.A.; Castillo-Fernandez, J.; Dekkers, K.F.; Do, A.N.; Graff, M.; Hänninen, I.K.; Tanaka, T.; Jonge, E.A.L.D.; et al. Association of dietary folate and vitamin B-12 intake with genome-wide DNA methylation in blood: A large-scale epigenome-wide association analysis in 5841 individuals. Am. J. Clin. Nutr. 2019, 110, 437–450. [Google Scholar] [CrossRef]
- Banjari, I.; Hjartåker, A. Dietary sources of iron and vitamin B12: Is this the missing link in colorectal carcinogenesis? Med. Hypotheses 2018, 116, 105–110. [Google Scholar] [CrossRef]
- Dahlin, A.M.; Van Guelpen, B.; Hultdin, J.; Johansson, I.; Hallmans, G.; Palmqvist, R. Plasma vitamin B12 concentrations and the risk of colorectal cancer: A nested case-referent study. Int. J. Cancer 2007, 122, 2057–2061. [Google Scholar] [CrossRef]
- Gylling, B.; Van Guelpen, B.; Schneede, J.; Hultdin, J.; Ueland, P.M.; Hallmans, G.; Johansson, I.; Palmqvist, R. Low Folate Levels Are Associated with Reduced Risk of Colorectal Cancer in a Population with Low Folate Status. Cancer Epidemiol. Biomark. Prev. 2014, 23, 2136–2144. [Google Scholar] [CrossRef] [Green Version]
- Le Marchand, L.; White, K.K.; Nomura, A.M.; Wilkens, L.R.; Selhub, J.S.; Tiirikainen, M.; Goodman, M.T.; Murphy, S.P.; Henderson, B.E.; Kolonel, L.N. Plasma Levels of B Vitamins and Colorectal Cancer Risk: The Multiethnic Cohort Study. Cancer Epidemiol. Biomark. Prev. 2009, 18, 2195–2201. [Google Scholar] [CrossRef] [Green Version]
- Araghi, S.O.; Jong, J.C.K.-D.; Van Dijk, S.C.; Swart, K.M.; Van Laarhoven, H.W.; Van Schoor, N.M.; De Groot, L.C.P.G.M.; Lemmens, V.; Stricker, B.H.; Uitterlinden, A.G.; et al. Folic Acid and Vitamin B12 Supplementation and the Risk of Cancer: Long-term Follow-up of the B Vitamins for the Prevention of Osteoporotic Fractures (B-PROOF) Trial. Cancer Epidemiol. Biomark. Prev. 2019, 28, 275–282. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sanchez, H.; Hossain, M.B.; Lera, L.; Hirsch, S.; Albala, C.; Uauy, R.; Broberg, K.; Ronco, A.M. High levels of circulating folate concentrations are associated with DNA methylation of tumor suppressor and repair genes p16, MLH1, and MGMT in elderly Chileans. Clin. Epigenetics 2017, 9, 1–11. [Google Scholar] [CrossRef] [Green Version]
- Wolters, M.; Ströhle, A.; Hahn, A. Cobalamin: A critical vitamin in the elderly. Prev. Med. 2004, 39, 1256–1266. [Google Scholar] [CrossRef]
- Boughanem, H.; Cabrera-Mulero, A.; Millán-Gómez, M.; Garrido-Sánchez, L.; Cardona, F.; Tinahones, F.J.; Moreno-Santos, I.; Macías-González, M.; Mulero, C.; Millán-Gómez, M.; et al. Transcriptional Analysis of FOXO1, C/EBP- and PPAR-2 Genes and Their association with Obesity-Related Insulin Resistance. Genes 2019, 10, 706. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moreno-Santos, I.; Castellano, D.; Lara, M.F.; Fernández-García, J.C.; Tinahones, F.J.; Macias-Gonzalez, M. IGFBP-3 Interacts with the Vitamin D Receptor in Insulin Signaling Associated with Obesity in Visceral Adipose Tissue. Int. J. Mol. Sci. 2017, 18, 2349. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bairaktari, E.T.; Seferiadis, K.I.; Elisaf, M.S. Evaluation of Methods for the Measurement of Low-Density Lipoprotein Cholesterol. J. Cardiovasc. Pharmacol. Ther. 2005, 10, 45–54. [Google Scholar] [CrossRef] [PubMed]
- Matthews, D.R.; Hosker, J.P.; Rudenski, A.S.; Naylor, B.A.; Treacher, D.F.; Turner, R.C. Homeostasis model assessment: Insulin resistance and β-cell function from fasting plasma glucose and insulin concentrations in man. Diabetologia 1985, 28, 412–419. [Google Scholar] [CrossRef] [Green Version]
- McKay, J.A.; Groom, A.; Potter, C.; Coneyworth, L.J.; Ford, D.; Mathers, J.C.; Relton, C.L. Genetic and Non-Genetic Influences during Pregnancy on Infant Global and Site Specific DNA Methylation: Role for Folate Gene Variants and Vitamin B12. PLoS ONE 2012, 7, e33290. [Google Scholar] [CrossRef]
- Cabrera-Mulero, A.; Crujeiras, A.B.; Izquierdo, A.G.; Torres, E.; Ayers, D.; Casanueva, F.F.; Tinahones, F.J.; Morcillo, S.; Macias-Gonzalez, M. Novel SFRP2 DNA Methylation Profile Following Neoadjuvant Therapy in Colorectal Cancer Patients with Different Grades of BMI. J. Clin. Med. 2019, 8, 1041. [Google Scholar] [CrossRef] [Green Version]
- Swets, M.; Zaalberg, A.; Boot, A.; Van Wezel, T.; Frouws, M.A.; Bastiaannet, E.; Gelderblom, H.; Van De Velde, C.; Kuppen, P.J.K. Tumor LINE-1 Methylation Level in Association with Survival of Patients with Stage II Colon Cancer. Int. J. Mol. Sci. 2016, 18, 36. [Google Scholar] [CrossRef] [Green Version]
- Byström, P.; Björkegren, K.; Larsson, A.; Johansson, L.; Berglund, Å. Serum vitamin B12 and folate status among patients with chemotherapy treatment for advanced colorectal cancer. Upsala J. Med. Sci. 2009, 114, 160–164. [Google Scholar] [CrossRef] [PubMed]
- Oh, H.K.; Lee, J.Y.; Eo, W.K.; Yoon, S.W.; Han, S.N. Elevated Serum Vitamin B12 Levels as a Prognostic Factor for Survival Time in Metastatic Cancer Patients: A Retrospective Study. Nutr. Cancer 2017, 70, 37–44. [Google Scholar] [CrossRef] [Green Version]
- Sun, N.-H.; Huang, X.-Z.; Wang, S.-B.; Li, Y.; Wang, L.-Y.; Wang, H.-C.; Zhang, C.-W.; Zhang, C.; Liu, H.-P.; Wang, Z.-N. A dose–response meta-analysis reveals an association between vitamin B12 and colorectal cancer risk. Public Health Nutr. 2015, 19, 1446–1456. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, Y.; Yu, Q.; Zhu, Z.; Zhang, J.; Chen, M.; Tang, P.; Li, K. Vitamin and multiple-vitamin supplement intake and incidence of colorectal cancer: A meta-analysis of cohort studies. Med. Oncol. 2015, 32, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.; Fang, Y.-J.; Feng, X.-L.; Abulimiti, A.; Huang, C.-Y.; Luo, H.; Zhang, N.-Q.; Chen, Y.-M.; Zhang, C.-X. Higher intakes of dietary vitamin D, calcium and dairy products are inversely associated with the risk of colorectal cancer: A case–control study in China. Br. J. Nutr. 2019, 123, 699–711. [Google Scholar] [CrossRef] [PubMed]
- Key, T.J.; Appleby, P.N.; Masset, G.; Brunner, E.J.; Cade, J.E.; Greenwood, D.C.; Stephen, A.M.; Kuh, D.; Bhaniani, A.; Powell, N.; et al. Vitamins, minerals, essential fatty acids and colorectal cancer risk in the United Kingdom Dietary Cohort Consortium. Int. J. Cancer 2012, 131, E320–E325. [Google Scholar] [CrossRef] [PubMed]
- Eussen, S.J.; Vollset, S.E.; Hustad, S.; Øivind, M.; Meyer, K.; Fredriksen, Å; Ueland, P.M.; Jenab, M.; Slimani, N.; Boffetta, P.; et al. Plasma vitamins B2, B6, and B12, and related genetic variants as predictors of colorectal cancer risk. Cancer Epidemiol. Biomark. Prev. 2010, 19, 2549–2561. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Figueiredo, J.C.; Levine, A.J.; Grau, M.V.; Øivind, M.; Ueland, P.M.; Ahnen, D.J.; Barry, E.L.; Tsang, S.; Munroe, D.; Ali, I.; et al. Vitamins B2, B6, and B12 and Risk of New Colorectal Adenomas in a Randomized Trial of Aspirin Use and Folic Acid Supplementation. Cancer Epidemiol. Biomark. Prev. 2008, 17, 2136–2145. [Google Scholar] [CrossRef] [Green Version]
- Van Wijngaarden, J.P.; Swart, K.M.A.; Enneman, A.W.; Dhonukshe-Rutten, R.A.M.; Van Dijk, S.C.; Ham, A.C.; Brouwer-Brolsma, E.M.; Van Der Zwaluw, N.L.; Sohl, E.; Van Meurs, J.B.J.; et al. Effect of daily vitamin B-12 and folic acid supplementation on fracture incidence in elderly individuals with an elevated plasma homocysteine concentration: B-PROOF, a randomized controlled trial. Am. J. Clin. Nutr. 2014, 100, 1578–1586. [Google Scholar] [CrossRef] [Green Version]
- Lippi, G.; Mattiuzzi, C.; Cervellin, G. Meat consumption and cancer risk: A critical review of published meta-analyses. Crit. Rev. Oncol. 2016, 97, 1–14. [Google Scholar] [CrossRef]
- Roman-Garcia, P.; Quiros-Gonzalez, I.; Mottram, L.; Lieben, L.; Sharan, K.; Wangwiwatsin, A.; Tubio, J.; Lewis, K.; Wilkinson, D.; Santhanam, B.; et al. Vitamin B12–dependent taurine synthesis regulates growth and bone mass. J. Clin. Investig. 2014, 124, 2988–3002. [Google Scholar] [CrossRef] [PubMed]
- Li, Z.; Gueant-Rodriguez, R.-M.; Quilliot, D.; Sirveaux, M.-A.; Meyre, D.; Gueant, J.-L.; Brunaud, L. Folate and vitamin B12 status is associated with insulin resistance and metabolic syndrome in morbid obesity. Clin. Nutr. 2018, 37, 1700–1706. [Google Scholar] [CrossRef] [PubMed]
- Madhu, S. Vitamin B12 and diabetes risk—Myth or reality. Int. J. Diabetes Dev. Ctries. 2020, 40, 1–3. [Google Scholar] [CrossRef] [Green Version]
- Vigneri, P.; Tirrò, E.; Pennisi, M.S.; Massimino, M.; Stella, S.; Romano, C.; Manzella, L. The Insulin/IGF System in Colorectal Cancer Development and Resistance to Therapy. Front. Oncol. 2015, 5, 230. [Google Scholar] [CrossRef] [Green Version]
- Yao, S.; Hu, Q.; Kerns, S.; Yan, L.; Onitilo, A.A.; Misleh, J.; Young, K.; Lei, L.; Bautista, J.; Mohamed, M.; et al. Impact of chemotherapy for breast cancer on leukocyte DNA methylation landscape and cognitive function: A prospective study. Clin. Epigenetics 2019, 11, 45. [Google Scholar] [CrossRef]
- Forster, V.J.; McDonnell, A.; Theobald, R.; McKay, J.A. Effect of methotrexate/vitamin B12on DNA methylation as a potential factor in leukemia treatment-related neurotoxicity. Epigenomics 2017, 9, 1205–1218. [Google Scholar] [CrossRef] [Green Version]
- Mokarram, P.; Naghibalhossaini, F.; Firoozi, M.S.; Malek-Hosseini, S.A.; Izadpanah, A.; Salahi, H.; Talei, A.; Mojallal, M. Methylenetetrahydrofolate reductase C677T genotype affects promoter methylation of tumor-specific genes in sporadic colorectal cancer through an interaction with folate/vitamin B12 status. World J. Gastroenterol. 2008, 14, 3662–3671. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Variables | Low Serum Vitamin B12 | High Serum Vitamin B12 |
|---|---|---|
| n (%) | 19 (23.8) | 61 (76.2) |
| Age (years) | 68.21 ± 10.33 | 67.38 ± 10.91 |
| Sex (males/females) | 16/3 | 21/40 * |
| BMI (kg/m2) | 26.74 ± 3.02 | 27.53 ± 4.36 |
| Fasting glucose (mg/dL) | 134.63 ± 66.92 | 121.68 ± 52.07 |
| Fasting insulin (μUI/mL) | 4.95 ± 3.36 | 6.65 ± 5.36 |
| HOMA-IR | 1.62 ± 1.48 | 2.10 ± 2.05 |
| Triglycerides (mg/dL) | 167.95 ± 75.51 | 158.73 ± 82.13 |
| Total cholesterol (mg/dL) | 160.00 ± 24.30 | 175.47 ± 44.65 |
| HDL-c (mg/dL) | 37.36 ± 11.78 | 42.49 ± 14.64 |
| LDL-c (mg/dL) | 91.04 ± 25.12 | 106.28 ± 35.30 * |
| CEA (mg/dL) | 5.88 ± 13.23 | 4.97 ± 8.17 |
| CA 19.9 (U/mL) | 18.63 ± 21.36 | 20.92 ± 30.96 |
| IGF1 (ng/mL) | 97.66 ± 39.92 | 137.56 ± 74.91 * |
| CRP (mg/L) | 6.03 ± 4.56 | 9.77 ± 12.99 |
| Vitamin B12 (pg/mL) | 199.79 ± 49.14 | 507.02 ± 337.83 ** |
| LINE1 Methylation | Age | BMI | Glucose | Insulin | HOMA-IR | TG | TC | LDL-c | HDL-c |
|---|---|---|---|---|---|---|---|---|---|
| Low vitamin B12 group | |||||||||
| PBMCs | 0.13 | −0.07 | −0.19 | −0.41 | −0.53 | 0.10 | 0.36 | 0.16 | -0.26 |
| VAT | 0.49 | −0.10 | −0.20 | 0.31 | 0.22 | −0.32 | −0.49 | −0.09 | 0.18 |
| Tumor area | −0.03 | −0.24 | −0.01 | −0.04 | −0.06 | −0.04 | −0.27 | 0.26 | −0.02 |
| High vitamin B12 group | |||||||||
| PBMCs | −0.09 | 0.03 | 0.04 | 0.10 | 0.10 | −0.12 | −0.21 | −0.16 | 0.16 |
| VAT | <0.01 | −0.27 | −0.22 | −0.32 | −0.31 | 0.02 | −0.02 | −0.03 | 0.12 |
| Tumor area | −0.02 | 0.15 | −0.16 | 0.25 | 0.19 | 0.26 | 0.08 | 0.14 | 0.17 |
| Variables | Both Sexes | Men Only | ||
|---|---|---|---|---|
| Low Vitamin B12 β (SE) | High Vitamin B12 β (SE) | Low Vitamin B12 β (SE) | High Vitamin B12 β (SE) | |
| LINE1 methylation: PBMCs | r2 = 0.32; p = 0.07 | r2 = −0.10; p = 0.99 | r2 = 0.38; p = 0.17 | r2 = −0.30; p = 0.51 |
| Age | 0.09 (0.04) | −0.00 (0.03) | 0.22 (0.04) | −0.08 (0.05) |
| Sex | −3.48 (1.16) * | −0.11 (0.71) | NA | NA |
| BMI | 0.05 (0.15) | 0.00 (0.08) | 0.00 (0.13) | 0.11 (0.18) |
| Neoadjuvant therapy | −0.07 (1.01) | −0.16 (0.78) | 0.13 (0.86) | −0.15 (1.67) |
| LINE1 methylation: tumor area | r2 = 0.51; p = 0.03 * | r2 = 0.18; p = 0.01 * | r2 = 0.64; p = 0.03 * | r2 = 0.32; p = 0.46 |
| Age | 0.05 (0.10) | 0.03 (0.07) | 0.07 (0.12) | 0.12 (0.16) |
| Sex | 2.63 (2.80) | −0.57 (1.65) | NA | NA |
| BMI | −0.85 (0.39) | 0.16 (0.18) | −0.88 (0.43) | −1.53 (1.61) |
| Neoadjuvant therapy | 7.80 (1.99) * | 5.99 (1.87) * | 7.87 (2.12) * | 8.92 (5.91) |
| Variables | Both Sexes | Men Only |
|---|---|---|
| OR (CI 95%) r2 = 0.22 | OR (CI 95%) r2 = 0.35 | |
| Age | 1.01 (0.94–1.07) | 0.98 (0.91–1.06) |
| Sex | 2.15 (0.51–11.91) | NA |
| Tumor LINE1 methylation | 0.82 * (0.70–0.95) * | 0.74 (0.57–0.90) * |
| CEA | 0.96 (0.91–1.03) | 0.90 (0.77–1.00) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Boughanem, H.; Hernandez-Alonso, P.; Tinahones, A.; Babio, N.; Salas-Salvadó, J.; Tinahones, F.J.; Macias-Gonzalez, M. Association between Serum Vitamin B12 and Global DNA Methylation in Colorectal Cancer Patients. Nutrients 2020, 12, 3567. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12113567
Boughanem H, Hernandez-Alonso P, Tinahones A, Babio N, Salas-Salvadó J, Tinahones FJ, Macias-Gonzalez M. Association between Serum Vitamin B12 and Global DNA Methylation in Colorectal Cancer Patients. Nutrients. 2020; 12(11):3567. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12113567
Chicago/Turabian StyleBoughanem, Hatim, Pablo Hernandez-Alonso, Alberto Tinahones, Nancy Babio, Jordi Salas-Salvadó, Francisco J. Tinahones, and Manuel Macias-Gonzalez. 2020. "Association between Serum Vitamin B12 and Global DNA Methylation in Colorectal Cancer Patients" Nutrients 12, no. 11: 3567. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12113567