The Associations of Dietary Iron, Zinc and Magnesium with Metabolic Syndrome in China’s Mega Cities

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
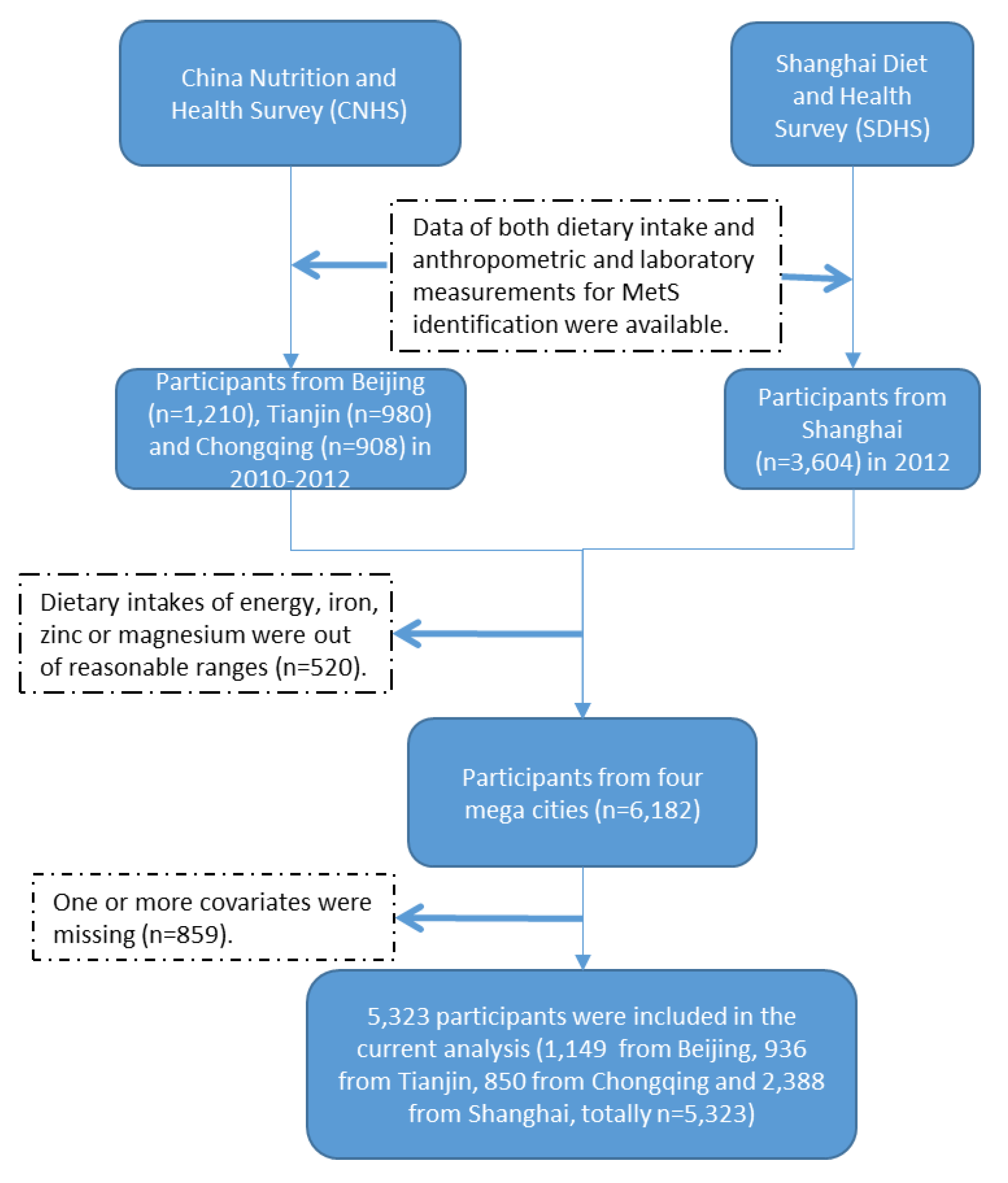
2.1. Study Population
2.2. Dietary Assessment
2.3. Potential Confounders
2.4. Anthropometric and Laboratory Measurements
2.5. Statistical Analyses
3. Results
3.1. Characteristics of the Participants and Correlations of Dietary Iron, Zinc and Magnesium Intakes
3.2. The Associations of Dietary Iron, Zinc and Magnesium with MetS
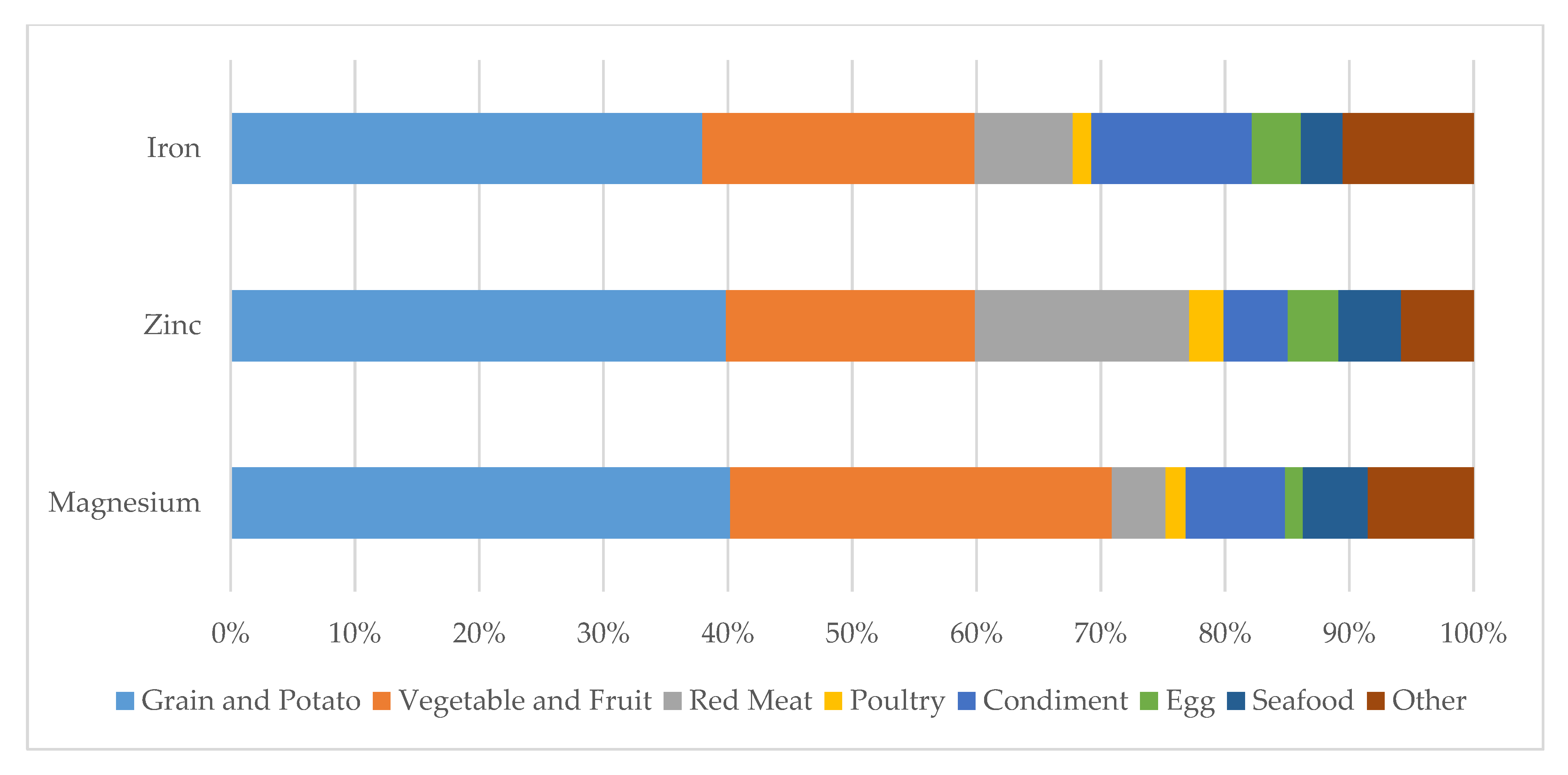
3.3. The Associations of Dietary Sources of Iron, Zinc and Magnesium with MetS
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Grundy, S.M.; Cleeman, J.I.; Daniels, S.R.; Donato, K.A.; Eckel, R.H.; Franklin, B.A.; Gordon, D.J.; Krauss, R.M.; Savage, P.J.; Smith, S.J.; et al. Diagnosis and management of the metabolic syndrome: An American heart association/national heart, lung, and blood institute scientific statement. Circulation 2005, 112, 2735–2752. [Google Scholar] [CrossRef] [Green Version]
- Gu, D.; Reynolds, K.; Wu, X.; Chen, J.; Duan, X.; Reynolds, R.F.; Whelton, P.K.; He, J. Prevalence of the metabolic syndrome and overweight among adults in China. Lancet 2005, 365, 1398–1405. [Google Scholar] [CrossRef]
- Li, Y.; Zhao, L.; Yu, D.; Wang, Z.; Ding, G. Metabolic syndrome prevalence and its risk factors among adults in China: A nationally representative cross-sectional study. PLoS ONE 2018, 13, e199293. [Google Scholar] [CrossRef]
- Munoz, M.; Garcia-Erce, J.A.; Remacha, A.F. Disorders of iron metabolism. Part 1: Molecular basis of iron homoeostasis. J. Clin. Pathol. 2011, 64, 281–286. [Google Scholar] [CrossRef] [PubMed]
- Zhu, Z.; Wu, F.; Lu, Y.; Wu, C.; Wang, Z.; Zang, J.; Guo, C.; Jia, X.; Yao, J.; Peng, H.; et al. Total and nonheme dietary iron intake is associated with metabolic syndrome and its components in chinese men and women. Nutrients 2018, 10, 1663. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dos Santos Vieira, D.; Hermes Sales, C.; Galvão Cesar, C.; Marchioni, D. Influence of Haem, Non-Haem, and Total Iron Intake on Metabolic Syndrome and Its Components: A Population-Based Study. Nutrients 2018, 10, 314. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Esfandiar, Z.; Hosseini-Esfahani, F.; Mirmiran, P.; Habibi-Moeini, A.S.; Azizi, F. Red meat and dietary iron intakes are associated with some components of metabolic syndrome: Tehran lipid and glucose study. J. Transl. Med. 2019, 17, 313. [Google Scholar] [CrossRef]
- King, J.C.; Brown, K.H.; Gibson, R.S.; Krebs, N.F.; Lowe, N.M.; Siekmann, J.H.; Raiten, D.J. Biomarkers of nutrition for development (BOND)-Zinc review. J. Nutr. 2016, 146, 858S–885S. [Google Scholar] [CrossRef] [Green Version]
- Powell, S.R. The antioxidant properties of zinc. J. Nutr. 2000, 130, 1447S–1454S. [Google Scholar] [CrossRef] [Green Version]
- Hennig, B.; Wang, Y.; Ramasamy, S.; McClain, C.J. Zinc deficiency alters barrier function of cultured porcine endothelial cells. J. Nutr. 1992, 122, 1242–1247. [Google Scholar] [CrossRef]
- Freitas, E.P.; Cunha, A.T.; Aquino, S.L.; Pedrosa, L.F.; Lima, S.C.; Lima, J.G.; Almeida, M.G.; Sena-Evangelista, K.C. Zinc status biomarkers and cardiometabolic risk factors in metabolic syndrome: A case control study. Nutrients 2017, 9, 175. [Google Scholar] [CrossRef] [PubMed]
- Guerrero-Romero, F.; Jaquez-Chairez, F.O.; Rodríguez-Morán, M. Magnesium in metabolic syndrome: A review based on randomized, double-blind clinical trials. Magnes. Res. 2016, 29, 146–153. [Google Scholar] [CrossRef] [PubMed]
- Cole, C.R.; Grant, F.K.; Swaby-Ellis, E.D.; Smith, J.L.; Jacques, A.; Northrop-Clewes, C.A.; Caldwell, K.L.; Pfeiffer, C.M.; Ziegler, T.R. Zinc and iron deficiency and their interrelations in low-income African American and Hispanic children in Atlanta. Am. J. Clin. Nutr. 2010, 91, 1027–1034. [Google Scholar] [CrossRef] [Green Version]
- Lee, D.H.; Folsom, A.R.; Jacobs, D.J. Iron, zinc, and alcohol consumption and mortality from cardiovascular diseases: The Iowa women’s health study. Am. J. Clin. Nutr. 2005, 81, 787–791. [Google Scholar] [CrossRef] [Green Version]
- Lim, K.; Booth, A.; Szymlek-Gay, E.; Gibson, R.; Bailey, K.; Irving, D.; Nowson, C.; Riddell, L. Associations between Dietary Iron and Zinc Intakes, and between Biochemical Iron and Zinc Status in Women. Nutrients 2015, 7, 2983–2999. [Google Scholar] [CrossRef] [Green Version]
- De Oliveira Otto, M.C.; Alonso, A.; Lee, D.; Delclos, G.L.; Bertoni, A.G.; Jiang, R.; Lima, J.A.; Symanski, E.; Jacobs, D.R.; Nettleton, J.A. Dietary intakes of zinc and heme iron from red meat, but not from other sources, are associated with greater risk of metabolic syndrome and cardiovascular disease. J. Nutr. 2012, 142, 526–533. [Google Scholar] [CrossRef] [Green Version]
- Yang, Y.; Wang, G.; Pan, X. Chinese Food Composition Book 2, 1st ed.; Peking University Medical Press: Beijing, China, 2005; pp. 75–216. ISBN 9787810716789. [Google Scholar]
- Yang, Y.; Wang, G.; Pan, X. Chinese Food Composition Book 1, 2nd ed.; Peking University Medical Press: Beijing, China, 2009; pp. 45–192. ISBN 9787811167276. [Google Scholar]
- Gong, W.; Liu, A.; Yao, Y.; Ma, Y.; Ding, C.; Song, C.; Yuan, F.; Zhang, Y.; Feng, G.; Chen, Z.; et al. Nutrient supplement use among the chinese population: A cross-sectional study of the 2010–2012 china nutrition and health surveillance. Nutrients 2018, 10, 1733. [Google Scholar] [CrossRef] [Green Version]
- Monsen, E.R.; Hallberg, L.; Layrisse, M.; Hegsted, D.M.; Cook, J.D.; Mertz, W.; Finch, C.A. Estimation of available dietary iron. Am. J. Clin. Nutr. 1978, 31, 134. [Google Scholar] [CrossRef]
- Pretorius, B.; Schonfeldt, H.C.; Hall, N. Total and haem iron content lean meat cuts and the contribution to the diet. Food Chem. 2016, 193, 97–101. [Google Scholar] [CrossRef] [Green Version]
- Chinese Nutrition Society. Chinese Dietary Reference Intakes; Science Press: Beijing, China, 2014. [Google Scholar]
- Choi, J.S.; Koh, I.; Lee, H.J.; Kim, W.H.; Song, J. Effects of excess dietary iron and fat on glucose and lipid metabolism. J. Nutr. Biochem. 2013, 24, 1634–1644. [Google Scholar] [CrossRef]
- Hansen, J.B.; Moen, I.W.; Mandrup-Poulsen, T. Iron: The hard player in diabetes pathophysiology. Acta Physiol. 2014, 210, 717–732. [Google Scholar] [CrossRef] [PubMed]
- Suarez Ortegón, M.F.; Ordoñez Betancourth, J.E.; Aguilar De Plata, C. Dietary zinc intake is inversely associated to metabolic syndrome in male but not in female urban adolescents. Am. J. Hum. Biol. 2013, 25, 550–554. [Google Scholar] [CrossRef] [PubMed]
- He, J.; Shen, X.; Fang, A.; Song, J.; Li, H.; Guo, M.; Li, K. Association between predominantly plant-based diets and iron status in Chinese adults: A cross-sectional analysis. Brit. J. Nutr. 2016, 116, 1621–1632. [Google Scholar] [CrossRef] [Green Version]
- Sarrafzadegan, N.; Khosravi-Boroujeni, H.; Lotfizadeh, M.; Pourmogaddas, A.; Salehi-Abargouei, A. Magnesium status and the metabolic syndrome: A systematic review and meta-analysis. Nutrition 2016, 32, 409–417. [Google Scholar] [CrossRef] [Green Version]
- Li, Q.; Chen, Y.; Fu, H.; Cui, Z.; Shi, L.; Wang, L.; Liu, Z. Health risk of heavy metals in food crops grown on reclaimed tidal flat soil in the Pearl River Estuary, China. J. Hazard. Mater. 2012, 227-228, 148–154. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Characteristics | All | Male | Female | |
|---|---|---|---|---|
| n (%) | 5323 (100.00) | 2386 (44.83) | 2937 (55.17) | |
| Age, % | ||||
| 18–44 years | 26.22 | 24.33 | 27.72 | |
| 45–59 years | 38.56 | 37.15 | 39.68 | |
| 60+ years | 35.22 | 38.52 | 32.60 | |
| Smoking Status, % | ||||
| Never smoker | 68.18 | 36.69 | 93.36 | |
| Former smoker | 5.72 | 10.48 | 1.91 | |
| Current smoker | 26.10 | 52.83 | 4.73 | |
| Region, % | ||||
| Central City | 41.02 | 40.31 | 41.59 | |
| Fringe Area | 27.73 | 27.10 | 28.24 | |
| Outskirt | 31.25 | 32.59 | 30.18 | |
| Physical Activity Level, % | ||||
| Sedentary | 80.75 | 73.37 | 86.65 | |
| Moderate | 15.41 | 21.05 | 10.90 | |
| Vigorous | 3.84 | 5.58 | 2.45 | |
| Intended Physical Exercises, % | 24.97 | 24.24 | 25.54 | |
| Alcohol Use, % | ||||
| lifetime abstainers | 71.08 | 50.49 | 87.53 | |
| non-heavy drinkers | 22.11 | 36.13 | 10.90 | |
| infrequent heavy drinkers | 3.80 | 7.12 | 1.16 | |
| frequent heavy drinkers | 3.01 | 6.26 | 0.41 | |
| Years of Education, % | ||||
| under 6 years | 8.40 | 4.26 | 11.72 | |
| 6 years | 20.92 | 20.75 | 21.05 | |
| 9 years | 33.41 | 34.73 | 32.36 | |
| 12 years | 22.26 | 23.14 | 21.56 | |
| 15 years | 8.23 | 9.33 | 7.36 | |
| over 15 years | 6.78 | 7.80 | 5.96 | |
| Dietary Intake, means ± SD | ||||
| Energy, kcal/day | 1771.11 ± 582.02 | 1921.61 ± 610.97 | 1650.80 ± 527.90 | |
| Total Iron, mg/day | 17.65 ± 6.18 | 18.82 ± 6.26 | 16.72 ± 5.96 | |
| Haem iron, mg/day | 1.24 ± 0.95 | 1.32 ± 0.96 | 1.18 ± 0.93 | |
| Non-haem iron, mg/day | 16.41 ± 5.81 | 17.50 ± 5.93 | 15.54 ± 5.57 | |
| Iron from Red Meat, mg/day | 1.18 ± 1.19 | 1.34 ± 1.31 | 1.05 ± 1.06 | |
| Iron from Grain and Potato, mg/day | 6.73 ± 3.36 | 7.44 ± 3.48 | 6.17 ± 3.14 | |
| Iron from Vegetables and Fruit, mg/day | 3.88 ± 2.83 | 3.95 ± 2.89 | 3.82 ± 2.78 | |
| Total Zinc, mg/day | 9.17 ± 3.21 | 9.89 ± 3.29 | 8.60 ± 3.03 | |
| Zinc from Red Meat, mg/day | 1.52 ± 1.47 | 1.73 ± 1.62 | 1.35 ± 1.31 | |
| Zinc from Grain and Potato, mg/day | 3.67 ± 1.68 | 4.06 ± 1.73 | 3.36 ± 1.58 | |
| Zinc from Vegetables and Fruit, mg/day | 1.83 ± 1.62 | 1.86 ± 1.66 | 1.81 ± 1.59 | |
| Total Magnesium, mg/day | 253.27 ± 98.74 | 267.15 ± 98.93 | 242.17 ± 97.19 | |
| Magnesium from Red Meat, mg/day | 10.66 ± 9.83 | 12.19 ± 10.97 | 9.44 ± 8.63 | |
| Magnesium from Grain and Potato, mg/day | 102.38 ± 58.88 | 111.26 ± 59.10 | 95.28 ± 57.74 | |
| Magnesium from Vegetables and Fruit, mg/day | 77.65 ± 57.35 | 78.31 ± 58.86 | 77.12 ± 56.11 | |
| Metabolic Syndrome, % | 34.49 | 29.48 | 38.49 | |
| Metabolic Syndrome’s components, % | ||||
| Elevated blood pressure | 53.55 | 57.09 | 50.72 | |
| Elevated waist circumference | 42.53 | 32.17 | 50.82 | |
| Elevated fasting glucose | 34.81 | 36.00 | 33.86 | |
| Elevated triglycerides | 29.06 | 30.98 | 27.52 | |
| Reduced HDL-C | 36.15 | 25.27 | 44.86 | |
| Total Iron | Haem Iron | Non-haem Iron | Zinc | Magnesium | |
|---|---|---|---|---|---|
| Total Iron | 1 | 0.42 | 0.99 | 0.71 | 0.82 |
| Haem Iron | 1 | 0.31 | 0.54 | 0.31 | |
| Nonhaem Iron | 1 | 0.68 | 0.82 | ||
| Zinc | 1 | 0.79 | |||
| Magnesium | 1 |
| Quartiles of Dietary Iron, Zinc or Magnesium (mg/day), ORs (95% CI) | ||||||
|---|---|---|---|---|---|---|
| Q1 | Q2 | Q3 | Q4 | p-Value for Trend | ||
| n | 1330 | 1331 | 1331 | 1331 | ||
| Total Iron | ||||||
| < 13.14 | (13.14, 16.73) | (16.73, 21.41) | ≥ 21.41 | |||
| Model 1 | Reference | 1.23(1.05, 1.45) | 1.24(1.06, 1.46) | 1.17(1.00, 1.37) | 0.03 | |
| Model 2 | Reference | 1.27(1.07, 1.51) | 1.31(1.08, 1.59) | 1.32(1.05, 1.64) | 0.02 | |
| Model 3 | Reference | 1.35(1.10, 1.65) | 1.47(1.15, 1.88) | 1.60(1.21, 2.11) | 0.01 | |
| Haem Iron | ||||||
| < 0.61 | (0.61, 1.05) | (1.05, 1.66) | ≥ 1.66 | |||
| Model 1 | Reference | 0.82(0.70, 0.96) | 0.72(0.61, 0.84) | 0.67(0.57, 0.78) | < 0.01 | |
| Model 2 | Reference | 0.81(0.69, 0.96) | 0.69(0.58, 0.82) | 0.68(0.57, 0.82) | < 0.01 | |
| Model 3 | Reference | 0.84(0.71, 1.00) | 0.75(0.62, 0.91) | 0.78(0.63, 0.96) | 0.03 | |
| Non-haem Iron | ||||||
| < 12.21 | (12.21, 15.50) | (15.50, 19.96) | ≥ 19.96 | |||
| Model 1 | Reference | 1.34(1.14, 1.57) | 1.33(1.13, 1.56) | 1.23(1.05, 1.45) | < 0.01 | |
| Model 2 | Reference | 1.39(1.17, 1.65) | 1.42(1.17, 1.72) | 1.35(1.08, 1.69) | < 0.01 | |
| Model 3 | Reference | 1.46(1.19, 1.79) | 1.54(1.21, 1.96) | 1.53(1.16, 2.02) | < 0.01 | |
| Zinc | ||||||
| < 6.87 | (6.87, 8.69) | (8.69, 11.19) | ≥ 11.19 | |||
| Model 1 | Reference | 1.01(0.86, 1.17) | 0.85(0.73, 1.00) | 0.80(0.68, 0.94) | 0.01 | |
| Model 2 | Reference | 0.95(0.81, 1.13) | 0.80(0.66, 0.96) | 0.69(0.55, 0.86) | < 0.01 | |
| Model 3 | Reference | 0.76(0.63, 0.92) | 0.55(0.44, 0.69) | 0.46(0.35, 0.61) | < 0.01 | |
| Magnesium (mg/day) | ||||||
| < 182.98 | (182.98, 235.03) | (235.03, 304.34) | ≥ 304.34 | |||
| Model 1 | Reference | 0.97(0.83, 1.13) | 0.86(0.73, 1.00) | 0.80(0.68, 0.94) | < 0.01 | |
| Model 2 | Reference | 1.08(0.91, 1.29) | 1.31(1.09, 1.58) | 1.13(0.91, 1.41) | 0.03 | |
| Model 3 | Reference | 1.11(0.90, 1.36) | 1.42(1.12, 1.81) | 1.32(0.99, 1.75) | 0.02 | |
| Quartiles of Dietary Iron, Zinc or Magnesium (mg/day), ORs (95% CI) | |||||||
|---|---|---|---|---|---|---|---|
| Q1 | Q2 | Q3 | Q4 | p-Value for Trend | |||
| n | 1330 | 1331 | 1331 | 1331 | |||
| Dietary Source of Red Meat | |||||||
| Iron | |||||||
| < 0.35 | (0.35, 0.91) | (0.91, 1.65) | ≥ 1.65 | ||||
| Model 1 | Reference | 0.80(0.69, 0.93) | 0.76(0.65, 0.89) | 0.65(0.56, 0.76) | < 0.01 | ||
| Model 2 | Reference | 0.79(0.67, 0.93) | 0.81(0.68, 0.96) | 0.74(0.62, 0.88) | < 0.01 | ||
| Model 3 | Reference | 0.81(0.53, 1.25) | 0.96(0.58, 1.60) | 1.03(0.59, 1.82) | 0.47 | ||
| Zinc | |||||||
| < 0.45 | (0.45, 1.18) | (1.18, 2.21) | ≥ 2.21 | ||||
| Model 1 | Reference | 0.85(0.73, 0.99) | 0.73(0.62, 0.85) | 0.65(0.56, 0.76) | < 0.01 | ||
| Model 2 | Reference | 0.84(0.72, 0.99) | 0.77(0.65, 0.91) | 0.74(0.62, 0.88) | < 0.01 | ||
| Model 3 | Reference | 0.97(0.59, 1.60) | 0.70(0.39, 1.26) | 0.71(0.38, 1.34) | 0.21 | ||
| Magnesium | |||||||
| < 3.33 | (3.33, 8.53) | (8.53, 15.60) | ≥ 15.60 | ||||
| Model 1 | Reference | 0.79(0.68, 0.93) | 0.83(0.71, 0.96) | 0.62(0.53, 0.72) | < 0.01 | ||
| Model 2 | Reference | 0.81(0.68, 0.95) | 0.85(0.72, 1.00) | 0.71(0.60, 0.85) | < 0.01 | ||
| Model 3 | Reference | 1.01(0.64, 1.59) | 1.20(0.71, 2.03) | 0.97(0.54, 1.74) | 0.29 | ||
| Dietary Source of Grain and Potato | |||||||
| Iron | |||||||
| < 4.45 | (4.45, 6.14) | (6.14, 8.26) | ≥ 8.26 | ||||
| Model 1 | Reference | 1.25(1.06, 1.47) | 1.52(1.29, 1.78) | 1.63(1.39, 1.92) | < 0.01 | ||
| Model 2 | Reference | 1.32(1.11, 1.57) | 1.72(1.44, 2.05) | 2.08(1.71, 2.53) | < 0.01 | ||
| Model 3 | Reference | 1.04(0.82, 1.32) | 1.09(0.81, 1.46) | 1.19(0.84, 1.67) | 0.77 | ||
| Zinc | |||||||
| < 2.55 | (2.55, 3.38) | (3.38, 4.49) | ≥ 4.49 | ||||
| Model 1 | Reference | 1.11(0.95, 1.31) | 1.32(1.13, 1.55) | 1.27(1.08, 1.48) | < 0.01 | ||
| Model 2 | Reference | 1.14(0.96, 1.35) | 1.45(1.21, 1.72) | 1.63(1.34, 2.00) | < 0.01 | ||
| Model 3 | Reference | 0.74(0.60, 0.92) | 0.68(0.52, 0.88) | 0.59(0.43, 0.81) | 0.01 | ||
| Magnesium | |||||||
| < 62.55 | (62.55, 89.87) | (89.87, 125.86) | ≥ 125.86 | ||||
| Model 1 | Reference | 1.37(1.16, 1.61) | 1.78(1.51, 2.10) | 2.02(1.71, 2.37) | < 0.01 | ||
| Model 2 | Reference | 1.46(1.22, 1.74) | 2.08(1.74, 2.48) | 2.60(2.14, 3.16) | < 0.01 | ||
| Model 3 | Reference | 1.69(1.35, 2.13) | 2.57(1.95, 3.39) | 3.26(2.36, 4.50) | < 0.01 | ||
| Dietary Source of Vegetables and Fruit | |||||||
| Iron | |||||||
| < 2.15 | (2.15, 3.54) | (3.54, 5.51) | ≥ 5.51 | ||||
| Model 1 | Reference | 0.86(0.74, 1.01) | 0.89(0.76, 1.04) | 0.81(0.69, 0.95) | 0.07 | ||
| Model 2 | Reference | 0.83(0.67, 1.03) | 0.76(0.61, 0.95) | 0.69(0.55, 0.87) | 0.01 | ||
| Model 3 | Reference | 0.93(0.67, 1.30) | 0.88(0.59, 1.32) | 0.77(0.48, 1.24) | 0.72 | ||
| Zinc | |||||||
| < 0.82 | (0.82, 1.38) | (1.38, 2.36) | ≥ 2.36 | ||||
| Model 1 | Reference | 1.03(0.88, 1.20) | 0.97(0.83, 1.14) | 0.82(0.70, 0.96) | 0.07 | ||
| Model 2 | Reference | 0.94(0.80, 1.11) | 0.90(0.76, 1.07) | 0.68(0.57, 0.81) | < 0.01 | ||
| Model 3 | Reference | 1.06(0.78, 1.43) | 1.16(0.78, 1.72) | 1.03(0.62, 1.69) | 0.78 | ||
| Magnesium | |||||||
| < 38.60 | (38.60, 63.36) | (63.36, 101.58) | ≥ 101.58 | ||||
| Model 1 | Reference | 1.02(0.87, 1.19) | 0.95(0.81, 1.11) | 0.96(0.82, 1.12) | 0.76 | ||
| Model 2 | Reference | 0.92(0.78, 1.08) | 0.83(0.70, 0.98) | 0.76(0.63, 0.90) | 0.01 | ||
| Model 3 | Reference | 0.80(0.58, 1.09) | 0.71(0.48, 1.05) | 0.86(0.54, 1.36) | 0.24 | ||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhu, Z.; He, Y.; Wu, F.; Zhao, L.; Wu, C.; Lu, Y.; Zang, J.; Wang, Z.; Sun, J.; Huang, J.; et al. The Associations of Dietary Iron, Zinc and Magnesium with Metabolic Syndrome in China’s Mega Cities. Nutrients 2020, 12, 659. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12030659
Zhu Z, He Y, Wu F, Zhao L, Wu C, Lu Y, Zang J, Wang Z, Sun J, Huang J, et al. The Associations of Dietary Iron, Zinc and Magnesium with Metabolic Syndrome in China’s Mega Cities. Nutrients. 2020; 12(3):659. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12030659
Chicago/Turabian StyleZhu, Zhenni, Yuna He, Fan Wu, Liyun Zhao, Chunfeng Wu, Ye Lu, Jiajie Zang, Zhengyuan Wang, Jing Sun, Jian Huang, and et al. 2020. "The Associations of Dietary Iron, Zinc and Magnesium with Metabolic Syndrome in China’s Mega Cities" Nutrients 12, no. 3: 659. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12030659