Exploring Rural Adolescents’ Dietary Diversity and Its Socioeconomic Correlates: A Cross-Sectional Study from Matlab, Bangladesh

 ,
,  , and
, and
Abstract
:1. Introduction
2. Materials and Methods
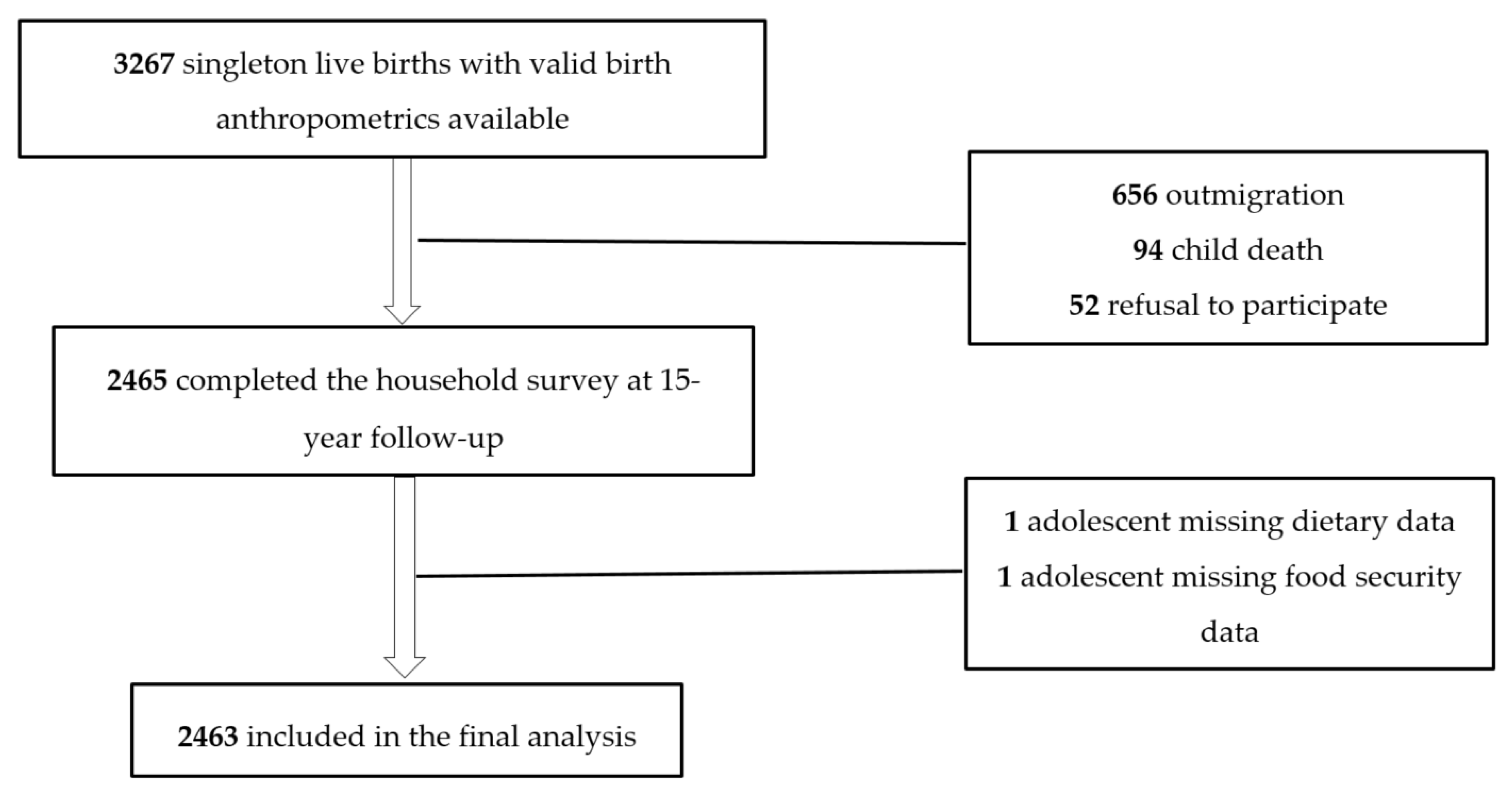
2.1. Study Design, Participants, and Setting
2.2. Data Collection
2.3. Assessment of Dietary Diversity
2.4. Assessment of Explanatory Variables
2.4.1. Socioeconomic Status (SES)
2.4.2. Household Food Security
2.4.3. Maternal and Adolescent Education
2.4.4. Gender and Ownership of Land
2.5. Statistical Analysis
2.6. Ethical Considerations
3. Results
3.1. DDS Among Adolescents and Proportion of Inadequate DD by Socio-Demographic Variables
3.2. Consumption Proportion of Different Foods and Its Socioeconomic and Gender Stratification
3.3. Factors Associated with Inadequate DD
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Sawyer, S.M.; Afifi, R.A.; Bearinger, L.H.; Blakemore, S.-J.; Dick, B.; Ezeh, A.C.; Patton, G.C. Adolescence: A foundation for future health. Lancet 2012, 379, 1630–1640. [Google Scholar] [CrossRef]
- Patton, G.C.; Sawyer, S.M.; Santelli, J.S.; Ross, D.A.; Afifi, R.; Allen, N.B.; Arora, M.; Azzopardi, P.; Baldwin, W.; Bonell, C.; et al. Our future: A Lancet commission on adolescent health and wellbeing. Lancet 2016, 387, 2423–2478. [Google Scholar] [CrossRef] [Green Version]
- Corkins, M.R.; Daniels, S.R.; de Ferranti, S.D.; Golden, N.H.; Kim, J.H.; Magge, S.N.; Schwarzenberg, S.J. Nutrition in children and adolescents. Med. Clin. N. Am. 2016, 100, 1217–1235. [Google Scholar] [CrossRef]
- Spear, B.A. Adolescent growth and development. J. Am. Diet. Assoc. 2002, S102, S23–S29. [Google Scholar] [CrossRef]
- Akseer, N.; Al-Gashm, S.; Mehta, S.; Mokdad, A.; Bhutta, Z.A. Global and regional trends in the nutritional status of young people: A critical and neglected age group: Global and regional trends in the nutritional status of young people. Ann. N. Y. Acad. Sci. 2017, 1393, 3–20. [Google Scholar] [CrossRef] [Green Version]
- Prentice, A.M.; Ward, K.A.; Goldberg, G.R.; Jarjou, L.M.; Moore, S.E.; Fulford, A.J.; Prentice, A. Critical windows for nutritional interventions against stunting. Am. J. Clin. Nutr. 2013, 97, 911–918. [Google Scholar] [CrossRef] [Green Version]
- Georgiadis, A.; Benny, L.; Duc, L.T.; Galab, S.; Reddy, P.; Woldehanna, T. Growth recovery and faltering through early adolescence in low- and middle-income countries: Determinants and implications for cognitive development. Soc. Sci. Med. 2017, 179, 81–90. [Google Scholar] [CrossRef]
- Myatt, M.; Khara, T.; Schoenbuchner, S.; Pietzsch, S.; Dolan, C.; Lelijveld, N.; Briend, A. Children who are both wasted and stunted are also underweight and have a high risk of death: A descriptive epidemiology of multiple anthropometric deficits using data from 51 countries. Arch. Public Health 2018, 76, 28. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Guideline: Implementing Effective Actions for Improving Adolescent Nutrition; Department of Nutrition for Health and Development, WHO: Geneva, Switzerland, 2018; ISBN 978-92-4-151370-8. [Google Scholar]
- MCH Services Unit. DGFP. MoHFW. Government of the People’s Republic of Bangladesh. National Strategy for Adolescent Health 2017–2030; DGFP: Dhaka, Bangladesh, 2016. [Google Scholar]
- Headey, D.; Hoddinott, J.; Ali, D.; Tesfaye, R.; Dereje, M. The Other Asian Enigma: Explaining the rapid reduction of undernutrition in Bangladesh. World Dev. 2015, 66, 749–761. [Google Scholar] [CrossRef] [Green Version]
- Christian, P.; Smith, E.R. Adolescent Undernutrition: Global burden, physiology, and nutritional risks. Ann. Nutr. Metab. 2018, 72, 316–328. [Google Scholar] [CrossRef]
- Alam, N.; Roy, S.K.; Ahmed, T.; Ahmed, A.S. Nutritional status, dietary intake, and relevant knowledge of adolescent girls in rural Bangladesh. J. Health Popul. Nutr. 2010, 28. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stanaway, J.D.; Afshin, A.; Gakidou, E.; Lim, S.S.; Abate, D.; Abate, K.H.; Abbafati, C.; Abbasi, N.; Abbastabar, H.; Abd-Allah, F.; et al. Global, regional, and national comparative risk assessment of 84 behavioural, environmental and occupational, and metabolic risks or clusters of risks for 195 countries and territories, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2018, 392, 1923–1994. [Google Scholar] [CrossRef] [Green Version]
- Rahman, S.; Islam, M.T.; Alam, D.S. Obesity and overweight in Bangladeshi children and adolescents: A scoping review. BMC Public Health 2014, 14. [Google Scholar] [CrossRef] [PubMed]
- United Nations. Transforming Our World: The 2030 Agenda for Sustainable Development; UN: New York, NY, USA, 2015. [Google Scholar]
- Ruel, M.T. Operationalizing dietary diversity: A review of measurement issues and research priorities. J. Nutr. 2003, 133, 3911S–3926S. [Google Scholar] [CrossRef] [PubMed]
- Krebs-Smith, S.M.; Smiciklas-Wright, H.; Guthrie, H.A.; Krebs-Smith, J. The effects of variety in food choices on dietary quality. J. Am. Diet. Assoc. 1987, 87, 897–903. [Google Scholar]
- Arimond, M.; Wiesmann, D.; Becquey, E.; Carriquiry, A.; Daniels, M.C.; Deitchler, M.; Fanou-Fogny, N.; Joseph, M.L.; Kennedy, G.; Martin-Prevel, Y.; et al. Simple food group diversity indicators predict micronutrient adequacy of women’s diets in 5 diverse, resource-poor settings1234567. J. Nutr. 2010, 140, 2059S–2069S. [Google Scholar] [CrossRef] [Green Version]
- Kennedy, G.L.; Pedro, M.R.; Seghieri, C.; Nantel, G.; Brouwer, I. Dietary diversity score is a useful indicator of micronutrient intake in non-breast-feeding Filipino children. J. Nutr. 2007, 137, 472–477. [Google Scholar] [CrossRef] [Green Version]
- Mirmiran, P.; Azadbakht, L.; Esmaillzadeh, A.; Azizi, F. Dietary diversity score in adolescents A good indicator of the nutritional adequacy of diets: Tehran lipid and glucose study. Asia Pac. J. Clin. Nutr. 2004, 13, 56–60. [Google Scholar]
- Hatløy, A.; Torheim, L.E.; Oshaug, A. Food variety—A good indicator of nutritional adequacy of the diet? A case study from an urban area in Mali, West Africa. Eur. J. Clin. Nutr. 1998, 52, 891–898. [Google Scholar] [CrossRef] [Green Version]
- Nguyen, P.H.; Huybregts, L.; Sanghvi, T.G.; Tran, L.M.; Frongillo, E.A.; Menon, P.; Ruel, M.T. Dietary diversity predicts the adequacy of micronutrient intake in pregnant adolescent girls and women in Bangladesh, but use of the 5-group cutoff poorly identifies individuals with inadequate intake. J. Nutr. 2018, 148, 790–797. [Google Scholar] [CrossRef] [Green Version]
- Mridha, M.K.; Matias, S.L.; Arnold, C.D.; Dewey, K.G. Factors associated with nutritional status and dietary practices of Bangladeshi adolescents in early pregnancy. Ann. N. Y. Acad. Sci. 2018, 1416, 66–76. [Google Scholar] [CrossRef] [Green Version]
- Na, M.; Mehra, S.; Christian, P.; Ali, H.; Shaikh, S.; Shamim, A.A.; Labrique, A.B.; Klemm, R.D.; Wu, L.S.; West, K.P. Maternal dietary diversity decreases with household food insecurity in rural Bangladesh: A longitudinal analysis. J. Nutr. 2016, 146, 2109–2116. [Google Scholar] [CrossRef] [Green Version]
- Harris-Fry, H.; Azad, K.; Kuddus, A.; Shaha, S.; Nahar, B.; Hossen, M.; Younes, L.; Costello, A.; Fottrell, E. Socio-economic determinants of household food security and women’s dietary diversity in rural Bangladesh: A cross-sectional study. J. Health Popul. Nutr. 2015, 33, 2. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sinharoy, S.S.; Waid, J.L.; Haardörfer, R.; Wendt, A.; Gabrysch, S.; Yount, K.M. Women’s dietary diversity in rural Bangladesh: Pathways through women’s empowerment. Matern. Child. Nutr. 2018, 14, e12489. [Google Scholar] [CrossRef] [Green Version]
- Ali, N.B.; Tahsina, T.; Hoque, D.M.E.; Hasan, M.M.; Iqbal, A.; Huda, T.M.; El Arifeen, S. Association of food security and other socio-economic factors with dietary diversity and nutritional statuses of children aged 6–59 months in rural Bangladesh. PLoS ONE 2019, 14, e0221929. [Google Scholar] [CrossRef] [Green Version]
- Persson, L.Å.; Arifeen, S.; Ekström, E.-C.; Rasmussen, K.M.; Frongillo, E.A.; Yunus, M. MINIMat Study team, for the effects of prenatal micronutrient and early food supplementation on maternal hemoglobin, birth weight, and infant mortality among children in Bangladesh: The MINIMat Randomized Trial. JAMA 2012, 307, 2050–2059. [Google Scholar] [CrossRef] [Green Version]
- Arifeen, S.E.; Ekström, E.-C.; Frongillo, E.A.; Hamadani, J.; Khan, A.I.; Naved, R.T.; Rahman, A.; Raqib, R.; Rasmussen, K.M.; Selling, K.E.; et al. Cohort profile: The maternal and infant nutrition interventions in the Matlab (MINIMat) cohort in Bangladesh. Int. J. Epidemiol. 2018. [Google Scholar] [CrossRef] [Green Version]
- Alam, N.; Ali, T.; Razzaque, A.; Rahman, M.; Zahirul Haq, M.; Saha, S.K.; Ahmed, A.; Sarder, A.; Moinuddin Haider, M.; Yunus, M.; et al. Health and demographic surveillance system (HDSS) in Matlab, Bangladesh. Int. J. Epidemiol. 2017, 46, 809–816. [Google Scholar] [CrossRef] [Green Version]
- Health Systems and Population Studies Division. Icddr,b Health and Demographic Surveillance System Matlab: Registration of Health and Demographic Events 2016; HDSS Annual Reports; Icddr,b: Dhaka, Bangladesh, 2018; Volume 51, ISBN 978-984-551-374-6. [Google Scholar]
- Islam, M.R.; Trenholm, J.; Rahman, A.; Pervin, J.; Ekström, E.C.; Rahman, S.M. Sociocultural Influences on Dietary Practices and Physical Activity Behaviors of Rural Adolescents—A qualitative exploration. Nutrients 2019, 11, 2916. [Google Scholar] [CrossRef] [Green Version]
- FAO and FHI 360. Minimum Dietary Diversity for Women: A Guide for Measurement; FAO: Rome, Italy, 2016. [Google Scholar]
- Arimond, M.; Wiesmann, D.; Becquey, E.; Carriquiry, A.; Daniels, M.; Deitchler, M.; Fanou, N.; Ferguson, E.; Joseph, M.; Kennedy, G.; et al. Dietary Diversity as a Measure of the Micronutrient Adequacy of Women’s Diets in Resource-Poor Areas: Summary of Results from Five Sites; FHI 360: Washington, DC, USA, 2011; p. 97. [Google Scholar]
- Custodio, E.; Kayitakire, F.; Thomas, A.-C. Exploring the New Indicator Minimum Dietary Diversity-Women. Results from Burkina Faso; Joint Research Centre, European Commission: Luxembourg, 2016; ISBN 978-92-79-54686-0. [Google Scholar]
- Birru, S.M.; Tariku, A.; Belew, A.K. Improved dietary diversity of school adolescent girls in the context of urban Northwest Ethiopia: 2017. Ital. J. Pediatr. 2018, 44, 48. [Google Scholar] [CrossRef] [Green Version]
- Kennedy, G.; Ballard, T.; Dop, M.-C. Guidelines for Measuring Household and Individual Dietary Diversity; FAO: Rome, Italy, 2011; ISBN 978-92-5-106749-9. [Google Scholar]
- Martin-Prevel, Y.; Becquey, E.; Arimond, M. Food group diversity indicators derived from qualitative list-based questionnaire misreported some foods compared to same indicators derived from quantitative 24-hour recall in urban Burkina Faso. J. Nutr. 2010, 140, 2086S–2093S. [Google Scholar] [CrossRef] [Green Version]
- Vyas, S.; Kumaranayake, L. Constructing socio-economic status indices: How to use principal components analysis. Health Policy Plan. 2006, 21, 459–468. [Google Scholar] [CrossRef] [Green Version]
- Coates, J.; Swindale, A.; Bilinsky, P. Household Food Insecurity Access Scale (HFIAS) for Measurement of Food Access: Indicator Guide (v.3); FHI 360/FANTA: Washington, DC, USA, 2007; p. 29. [Google Scholar]
- Frongillo, E.A. Development and validation of an experience-based measure of household food insecurity within and across seasons in Northern Burkina Faso1,2. J. Nutr. 2006, 136, 1409S–1419S. [Google Scholar] [CrossRef] [Green Version]
- Leroy, J.L.; Ruel, M.; Sununtnasuk, C.; Ahmed, A. Understanding the determinants of adolescent nutrition in Bangladesh: Adolescents’ nutritional status in Bangladesh. Ann. N. Y. Acad. Sci. 2018, 1416, 18–30. [Google Scholar] [CrossRef] [Green Version]
- Naher, F.; Barkat-e-Khuda; Ahmed, S.S.; Hossain, M. How nutrition-friendly are agriculture and health policies in Bangladesh? Food Nutr. Bull. 2014, 35, 133–146. [Google Scholar] [CrossRef] [Green Version]
- Mellendick, K.; Shanahan, L.; Wideman, L.; Calkins, S.; Keane, S.; Lovelady, C. Diets rich in fruits and vegetables are associated with lower cardiovascular disease risk in adolescents. Nutrients 2018, 10, 136. [Google Scholar] [CrossRef] [Green Version]
- Peltzer, K.; Pengpid, S. Fruits and vegetables consumption and associated factors among in-school adolescents in five Southeast Asian countries. Int. J. Environ. Res. Public. Health 2012, 9, 3575–3587. [Google Scholar] [CrossRef]
- Darmon, N.; Drewnowski, A. Contribution of food prices and diet cost to socioeconomic disparities in diet quality and health: A systematic review and analysis. Nutr. Rev. 2015, 73, 643–660. [Google Scholar] [CrossRef]
- Bel-Serrat, S.; Mouratidou, T.; Jiménez-Pavón, D.; Huybrechts, I.; Cuenca-García, M.; Mistura, L.; Gottrand, F.; González-Gross, M.; Dallongeville, J.; Kafatos, A.; et al. Is dairy consumption associated with low cardiovascular disease risk in European adolescents? Results from the HELENA Study: Cardiovascular risk and dairy consumption. Pediatr. Obes. 2014, 9, 401–410. [Google Scholar] [CrossRef]
- Racey, M.; Bransfield, J.; Capello, K.; Field, D.; Kulak, V.; Machmueller, D.; Preyde, M.; Newton, G. Barriers and facilitators to intake of dairy products in adolescent males and females with different levels of habitual intake. Glob. Pediatr. Health 2017, 4. [Google Scholar] [CrossRef] [Green Version]
- Vakili, M.; Abedi, P.; Sharifi, M.; Hosseini, M. Dietary diversity and its related factors among adolescents: A survey in Ahvaz-Iran. Glob. J. Health Sci. 2013, 5, 181–186. [Google Scholar] [CrossRef]
- Mayén, A.-L.; Marques-Vidal, P.; Paccaud, F.; Bovet, P.; Stringhini, S. Socioeconomic determinants of dietary patterns in low- and middle-income countries: A systematic review. Am. J. Clin. Nutr. 2014, 100, 1520–1531. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vereecken, C.; Pedersen, T.P.; Ojala, K.; Krolner, R.; Dzielska, A.; Ahluwalia, N.; Giacchi, M.; Kelly, C. Fruit and vegetable consumption trends among adolescents from 2002 to 2010 in 33 countries. Eur. J. Public Health 2015, 25, 16–19. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wheeler, E.F.; Abdullah, M. Seasonal variations, and the intra-household distribution of food in a Bangladeshi village. Am. J. Clin. Nutr. 1985, 41, 1305–1313. [Google Scholar] [CrossRef] [Green Version]
- Harris-Fry, H.; Shrestha, N.; Costello, A.; Saville, N.M. Determinants of intra-household food allocation between adults in South Asia — A systematic review. Int. J. Equity Health 2017, 16, 107. [Google Scholar] [CrossRef]
- Ganesan, S.; Ravishankar, S.L.; Ramalingam, S. Are body image issues affecting our adolescents? A cross-sectional study among college going adolescent girls. Indian J. Community Med. Off. Publ. Indian Assoc. Prev. Soc. Med. 2018, 43, S42–S46. [Google Scholar] [CrossRef]
- Mallick, N.; Ray, S.; Mukhopadhyay, S. Eating behaviours and body weight concerns among adolescent girls. Adv. Public Health 2014, 2014, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Weichselbaum, E. Nutrition and Teenagers/Young Adults. In Public Health Nutrition; Buttriss, J.L., Welch, A.A., Kearney, J.M., Lanham-New, S.A., Eds.; The Nutrition Society Textbook Series; John Wiley & Sons: Chichester, UK, 2017; pp. 159–174. ISBN 978-1-118-66097-3. [Google Scholar]
- Aurino, E. Do boys eat better than girls in India? Longitudinal evidence on dietary diversity and food consumption disparities among children and adolescents. Econ. Hum. Biol. 2017, 25, 99–111. [Google Scholar] [CrossRef] [PubMed]
- Aurino, E.; Fernandes, M.; Penny, M.E. The nutrition transition and adolescents’ diets in low- and middle-income countries: A cross-cohort comparison. Public Health Nutr. 2017, 20, 72–81. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rao, M.; Afshin, A.; Singh, G.; Mozaffarian, D. Do healthier foods and diet patterns cost more than less healthy options? A systematic review and meta-analysis. BMJ Open 2013, 3, e004277. [Google Scholar] [CrossRef] [PubMed]
- Bashir, M.K.; Schilizzi, S. Determinants of rural household food security: A comparative analysis of African and Asian studies: Determinants of rural household food security. J. Sci. Food Agric. 2013, 93, 1251–1258. [Google Scholar] [CrossRef] [PubMed]
- Belachew, T.; Lindstrom, D.; Gebremariam, A.; Hogan, D.; Lachat, C.; Huybregts, L.; Kolsteren, P. Food Insecurity, Food Based Coping Strategies and Suboptimal Dietary Practices of Adolescents in Jimma Zone Southwest Ethiopia. PLoS ONE 2013, 8, e57643. [Google Scholar] [CrossRef] [Green Version]
- Schwei, R.J.; Tesfay, H.; Asfaw, F.; Jogo, W.; Busse, H. Household dietary diversity, vitamin A consumption and food security in rural Tigray, Ethiopia. Public Health Nutr. 2017, 20, 1540–1547. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thorne-Lyman, A.L.; Valpiani, N.; Sun, K.; Semba, R.D.; Klotz, C.L.; Kraemer, K.; Akhter, N.; de Pee, S.; Moench-Pfanner, R.; Sari, M.; et al. Household dietary diversity and food expenditures are closely linked in rural Bangladesh, increasing the risk of malnutrition due to the financial crisis. J. Nutr. 2010, 140, 182S–188S. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- James P Grant School of Public Health; National Nutrition Services. State of Food Security and Nutrition in Bangladesh 2015; State of Food Security and Nutrition in Bangladesh; NNS, Directorate General of Health Services: Dhaka, Bangladesh, 2016; ISBN 978-984-34-0976-8. [Google Scholar]
- Blum, L.S.; Khan, R.; Sultana, M.; Soltana, N.; Siddiqua, Y.; Khondker, R.; Sultana, S.; Tumilowicz, A. Using a gender lens to understand eating behaviours of adolescent females living in low-income households in Bangladesh. Matern. Child. Nutr. 2019, 15. [Google Scholar] [CrossRef]
- Abizari, A.-R.; Ali, Z. Dietary patterns and associated factors of schooling Ghanaian adolescents. J. Health Popul. Nutr. 2019, 38, 5. [Google Scholar] [CrossRef] [Green Version]
- Taher, A.K.; Evans, N.; Evans, C.E. The cross-sectional relationships between consumption of takeaway food, eating meals outside the home and diet quality in British adolescents. Public Health Nutr. 2019, 22, 63–73. [Google Scholar] [CrossRef]
- Rashid, D.A.; Smith, L.C.; Rahman, T. Determinants of dietary quality: Evidence from Bangladesh. World Dev. 2011, 39, 2221–2231. [Google Scholar] [CrossRef] [Green Version]
- Semba, R.D.; de Pee, S.; Sun, K.; Sari, M.; Akhter, N.; Bloem, M.W. Effect of parental formal education on risk of child stunting in Indonesia and Bangladesh: A cross-sectional study. Lancet 2008, 371, 322–328. [Google Scholar] [CrossRef]
- Sraboni, E.; Quisumbing, A. Women’s empowerment in agriculture and dietary quality across the life course: Evidence from Bangladesh. Food Policy 2018, 81, 21–36. [Google Scholar] [CrossRef]
- Hebert, J.R.; Clemow, L.; Pbert, L.; Ockene, I.S.; Ockene, J.K. Social desirability bias in dietary self-report may compromise the validity of dietary intake measures. Int. J. Epidemiol. 1995, 24, 389–398. [Google Scholar] [CrossRef] [PubMed]
- Teufel, N.I. Development of culturally competent food-frequency questionnaires. Am. J. Clin. Nutr. 1997, 65, 1173S–1178S. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tamiru, D.; Argaw, A.; Gerbaba, M.; Nigussie, A.; Ayana, G.; Belachew, T. Improving dietary diversity of school adolescents through school based nutrition education and home gardening in Jimma Zone: Quasi-experimental design. Eat. Behav. 2016, 23, 180–186. [Google Scholar] [CrossRef]
- Ridoutt, B.; Bogard, J.R.; Dizyee, K.; Lim-Camacho, L.; Kumar, S. Value chains and diet quality: A review of impact pathways and intervention strategies. Agriculture 2019, 9, 185. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Food Group | Individual Food Items in the Group |
|---|---|
| Grains, white roots, and tubers and plantains | Rice- cooked (bhat) and fried, puffed rice (muri), panta, wheat bread, paratha, chapatti, luchi, other items made from milled grains, maize, cassava, taro (kochu mukhi), green banana. |
| Vitamin A-rich vegetables, tubers, and fruits 1 | Carrot, pumpkin, orange-fleshed sweet potato, mango (ripe), papaya (ripe), hog plum, watermelon. |
| Dark green leafy vegetables (DGLV) | Red amaranth, taro leaves, spinach, bottle guard leaves, mustard leaves, other locally available shaak. |
| Other vegetables | Tomato, gourd, brinjal, zhinga, long bean, cucumber, teasle gourd, wax gourd, green papaya, cabbage, cauliflower, radish. |
| Other fruits | Guava, banana, orange, apple, boroi, grapes, jackfruit, other fruits that are not vitamin A-rich. |
| Flesh and organ meat | Chicken, duck, beef, sheep, goat, pigeon, and liver, kidney, or any other organ meat. |
| Eggs | Chicken, duck, or quail eggs. |
| Fish | Rohu (Rui), chitol, mrigal, shing, gojar, taki, puti, tilapia, pangasius, hilsa, kajuli, bashpata, koi, rani, bou, dry fish, prawn, etcetera. |
| Legumes, nuts, and seeds | Beans, peas, lentils, hyacinth beans, pea seeds, groundnuts, peanuts. |
| Milk products | Milk, yoghurt, shemai, shuji, payesh, khir, paneer, or other foods made with milk. |
| Characteristic | n (%) (N = 2463) |
|---|---|
| Gender: | |
| Girls | 1261 (51.2) |
| Boys | 1202 (48.8) |
| Adolescents’ education (completed years of formal education): | |
| Primary (1–5 years), non-formal, illiterate | 490 (19.9) |
| Secondary (6–12 years) | 1973 (80.1) |
| Maternal education (completed years of formal education): | |
| No education | 493 (20.0) |
| Primary (1–5 years) | 868 (35.2) |
| Secondary and above (≥ 6 years) | 1102 (44.7) |
| Household food security: | |
| Food insecure | 1327 (53.9) |
| Food secure | 1136 (46.1) |
| Household source of drinking water: | |
| Safe sources (piped or tube-well water) | 2434 (98.8) |
| Other sources (rain or surface water) | 29 (1.2) |
| Household electricity coverage | 2166 (87.9) |
| Family ownership of farming land | 1290 (52.3) |
| Family ownership of livestock | 1753 (71.2) |
| Dietary Diversity Score (DDS) | Mean ± SD | p-Value 1 |
|---|---|---|
| Overall | 4.84 ± 1.51 | -- |
| By gender: | ||
| Boys | 4.92 ± 1.56 | <0.01 * |
| Girls | 4.76 ± 1.46 | |
| By socioeconomic status (SES): | <0.0001 * | |
| Poorest | 4.55 ± 1.48 | |
| Middle-status | 4.84 ± 1.44 | |
| Richest | 5.13 ± 1.56 | |
| Proportion of inadequate DD (DDS < 5) | n (%, 95% CI) | p-value 2 |
| Overall | 1042 (42.31, 40.36–44.26) | - |
| Gender: | ||
| Boy (n = 1202) | 480 (39.9, 37.2–42.7) | 0.019 * |
| Girl (n = 1261) | 562 (44.6, 41.8–47.3) | |
| SES: | ||
| Poorest (n = 822) Middle-status (n = 819) | 418 (50.9, 47.4–54.3) 333 (40.7, 37.3–44.0) | <0.0001 * |
| Richest (n = 822) | 291 (35.4, 32.1–38.7) | |
| Household food security: | ||
| Food insecure (n = 1327) | 625 (47.1, 44.4–49.8) | <0.0001 * |
| Food secure (n = 1136) | 417 (36.7, 33.9–39.5) | |
| Adolescents’ education: | ||
| Primary, non-formal, illiterate (n = 490) | 189 (38.6, 34.3–42.9) | 0.062 |
| Secondary (n = 1973) | 853 (43.2, 41.0–45.4) | |
| Maternal education: | ||
| No education (n = 493) | 246 (49.9, 45.5–54.3) | <0.001 * |
| Primary (n = 868) | 380 (43.8, 40.5–47.1) | |
| Secondary and above (n = 1102) | 416 (37.7, 34.8–40.6) |
| Food Group | Adolescents Who Consumed Item/s from the Group n (% of Total in That Gender or SES Category, 95% CI) | |||||||
|---|---|---|---|---|---|---|---|---|
| Overall (n = 2463) | Boy (n = 1202) | Girl (n = 1261) | p-Value 1 | Poorest (n = 822) | Middle-Status (n = 819) | Richest (n = 822) | p-Value 1 | |
| Grains, white roots and tubers, and plantains | 2461 (99.9, 99.8–100) | 1200 (99.8, 99.6–100) | 1261 (100) | 0.147 | 822 (100) | 818 (99.9, 99.6–100) | 821 (99.9, 99.6–100) | 0.606 |
| Vitamin A-rich vegetables, tubers, and fruits | 774 (31.4, 29.6–33.2) | 372 (30.9, 28.3–33.6) | 402 (31.9, 29.3–34.5) | 0.619 | 236 (28.7, 25.6–31.8) | 262 (31.9, 28.8–35.2) | 276 (33.6, 30.3–36.8) | 0.095 |
| DGLV 2 | 660 (26.8, 25.0–28.5) | 294 (24.5, 22.0–26.9) | 366 (29.0, 26.5–31.5) | 0.011 * | 218 (26.5, 23.5–29.5) | 236 (28.8, 25.7–31.9) | 206 (25.1, 22.1–28.0) | 0.224 |
| Other vegetables | 1496 (60.7, 58.8–62.7) | 724 (60.2, 57.5–62.9) | 772 (61.2, 58.5–63.9) | 0.616 | 491 (59.7, 56.4–63.1) | 497 (60.7, 57.3–64.0) | 508 (61.8, 58.5–65.1) | 0.691 |
| Other fruits | 1112 (45.1, 43.2–47.1) | 550 (45.8, 42.9–48.6) | 562 (44.6, 41.8–47.3) | 0.553 | 319 (38.8, 35.5–42.1) | 391 (47.7, 44.3–51.2) | 402 (48.9, 45.5–52.3) | <0.0001 * |
| Flesh and organ meat | 868 (35.2, 33.3–37.1) | 457 (38.0, 35.3–40.8) | 411 (32.6, 30.0–35.2) | 0.005 * | 226 (27.5, 24.4–30.5) | 290 (35.4, 32.1–38.7) | 352 (42.8, 39.4–46.2) | <0.0001 * |
| Eggs | 860 (34.9, 33.0–36.8) | 457 (38.0, 35.3–40.8) | 403 (31.9, 29.4–34.5) | 0.002 * | 246 (29.9, 26.8–33.1) | 267 (32.6, 29.4–35.8) | 347 (42.2, 38.8–45.6) | <0.0001 * |
| Fish | 1802 (73.2, 71.4–74.9) | 872 (72.5, 70.0–75.1) | 930 (73.8, 71.3–76.2) | 0.499 | 611 (74.3, 71.3–77.3) | 564 (68.9, 65.7–72.0) | 627 (76.3, 73.4–79.2) | 0.002 * |
| Legumes, nuts, and seeds | 1138 (46.2, 44.2–48.2) | 581 (48.3, 45.5–51.2) | 557 (44.2, 41.4–46.9) | 0.038 * | 363 (44.2, 40.8–47.6) | 383 (46.8, 43.3–50.2) | 392 (47.7, 44.3–51.1) | 0.331 |
| Milk products | 751 (30.5, 28.7–32.3) | 409 (34.0, 31.3–36.7) | 342 (27.1, 24.7–29.6) | <0.001 * | 207 (25.2, 22.2–28.1) | 260 (31.7, 28.6–34.9) | 284 (34.5, 31.3–37.8) | <0.001 * |
| Variables | Inadequate DD (DDS < 5) | |||
|---|---|---|---|---|
| Crude Analysis 1 | Adjusted Analysis 2,3 | |||
| Crude OR (95% CI) 4 | Adjusted OR (95% CI) | |||
| Gender: | ||||
| Boy (Ref.) | ||||
| Girl | 1.21 (1.03–1.42) * | 1.10 (0.93–1.29) | ||
| SES: | ||||
| Richest (Ref.) | ||||
| Middle-status | 1.25 (1.02–1.53) * | 1.13 (0.92–1.40) | ||
| Poorest | 1.89 (1.55–2.30) * | 1.59 (1.27–2.00) * | ||
| Household food security: | ||||
| Food secure (Ref.) | ||||
| Food insecure | 1.54 (1.31–1.81) * | 1.34 (1.13–1.59) * | ||
| Adolescents’ education: | ||||
| Primary, non-formal, illiterate (Ref.) | ||||
| Secondary | 1.21 (0.99–1.49) | 1.38 (1.11–1.71) * | ||
| Maternal education: | ||||
| No education (Ref.) | ||||
| Primary | 0.78 (0.63–0.98) * | 0.85 (0.67–1.06) | ||
| Secondary and above | 0.61 (0.49–0.75) * | 0.76 (0.60–0.96) * | ||
| Stratified analysis: by gender | ||||
| Crude ORboy (95% CI) | Adjusted 5 ORboy (95% CI) | Crude ORgirl(95% CI) | Adjusted 5 ORgirl (95% CI) | |
| SES: | ||||
| Richest (Ref.) | ||||
| Middle-status | 1.33 (1.01–1.76) * | 1.19 (0.89–1.60) | 1.17 (0.88–1.56) | 1.07 (0.79–1.44) |
| Poorest | 1.77 (1.32–2.37) * | 1.53 (1.09–2.14) * | 1.93 (1.47–2.54) * | 1.63 (1.20–2.22) * |
| Household food security: | ||||
| Food secure (Ref.) | ||||
| Food insecure | 1.41 (1.12–1.78) * | 1.26 (0.99–1.61) | 1.63 (1.30–2.05) * | 1.42 (1.12–1.81) * |
| Adolescents’ education: | ||||
| Primary, non-formal, illiterate (Ref.) | ||||
| Secondary | 1.08 (0.83–1.40) | 1.32 (1.00–1.75) | 1.34 (0.96–1.87) | 1.44 (1.03–2.03) * |
| Maternal education: | ||||
| No education (Ref.) | ||||
| Primary | 0.85 (0.61–1.17) | 0.91 (0.65–1.27) | 0.72 (0.53–0.98) * | 0.79 (0.58–1.09) |
| Secondary and above | 0.61 (0.45–0.83) * | 0.72 (0.51–1.02) | 0.61 (0.45–0.83) * | 0.79 (0.57–1.10) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Islam, M.R.; Rahman, S.M.; Tarafder, C.; Rahman, M.M.; Rahman, A.; Ekström, E.-C. Exploring Rural Adolescents’ Dietary Diversity and Its Socioeconomic Correlates: A Cross-Sectional Study from Matlab, Bangladesh. Nutrients 2020, 12, 2230. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12082230
Islam MR, Rahman SM, Tarafder C, Rahman MM, Rahman A, Ekström E-C. Exploring Rural Adolescents’ Dietary Diversity and Its Socioeconomic Correlates: A Cross-Sectional Study from Matlab, Bangladesh. Nutrients. 2020; 12(8):2230. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12082230
Chicago/Turabian StyleIslam, Mohammad Redwanul, Syed Moshfiqur Rahman, Chandan Tarafder, Md. Monjur Rahman, Anisur Rahman, and Eva-Charlotte Ekström. 2020. "Exploring Rural Adolescents’ Dietary Diversity and Its Socioeconomic Correlates: A Cross-Sectional Study from Matlab, Bangladesh" Nutrients 12, no. 8: 2230. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12082230