The Effects of Intermittent Fasting Combined with Resistance Training on Lean Body Mass: A Systematic Review of Human Studies


Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Sources
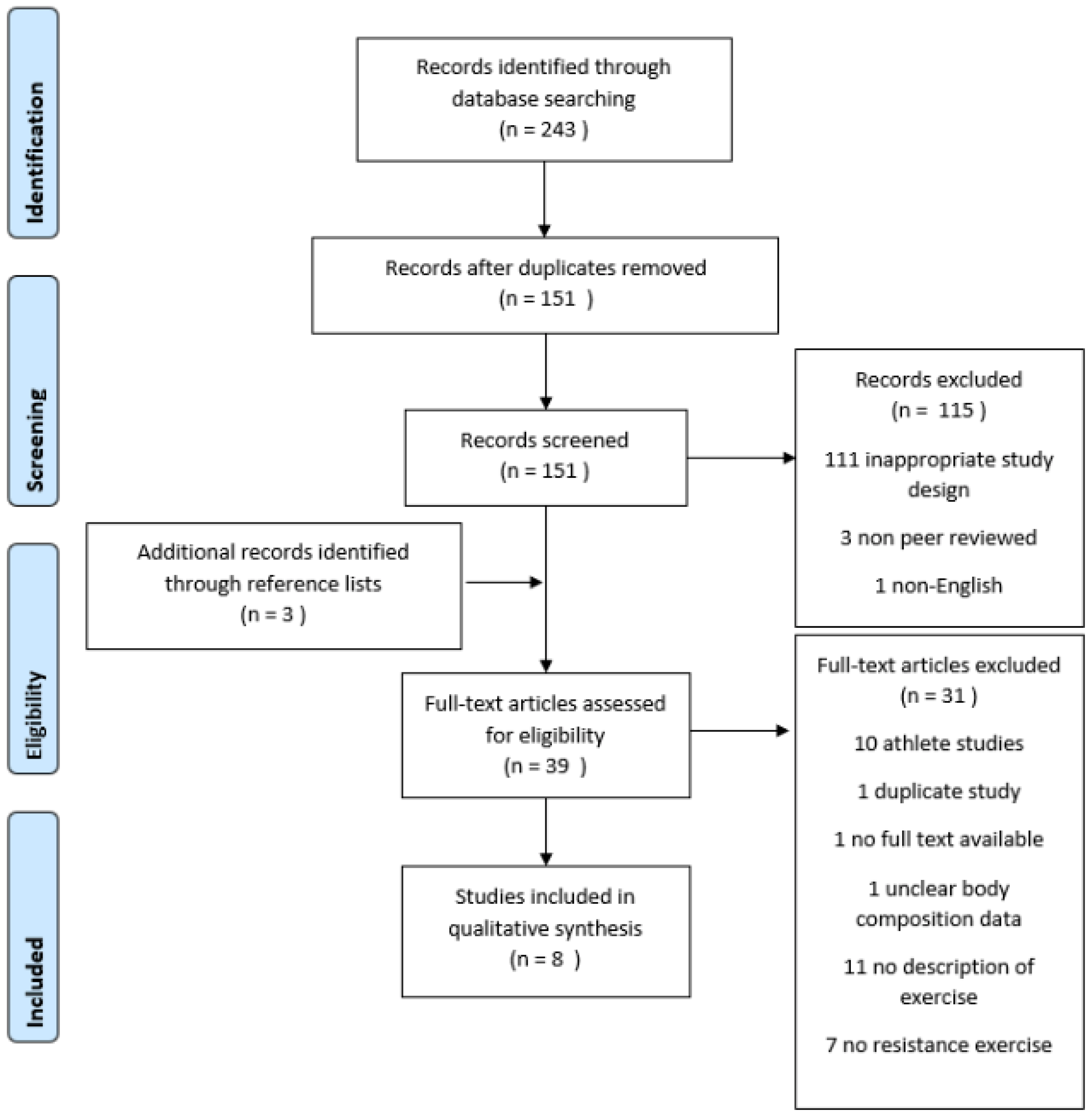
2.2. Study Selection
2.3. Data Extraction
2.4. Quality Appraisal
3. Results
3.1. Intervention Period
3.2. Participant Characteristics
3.3. Intervention—Fasting Protocol
3.4. Intervention—Resistance Training Protocol
3.5. Effects of TRF on LBM, Body Weight and Fat
3.6. Effect of Modified ADF on LBM, Body Weight and Fat
3.7. Effect of Ramadan Fasting on LBM, Body Weight and Fat
3.8. Methods of Anthropometrical Assessment
3.9. Reported Adherence to Dietary Protocols
3.10. Quality Appraisal
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Harvie, M.; Howell, A. Potential Benefits and Harms of Intermittent Energy Restriction and Intermittent Fasting Amongst Obese, Overweight and Normal Weight Subjects—A Narrative Review of Human and Animal Evidence. Behav. Sci. 2017, 7, 4. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Trepanowski, J.F.; Bloomer, R.J. The impact of religious fasting on human health. Nutr. J. 2010, 9, 57. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Adawi, M.; Damiani, G.; Bragazzi, N.L.; Bridgewood, C.; Pacifico, A.; Conic, R.R.; Morrone, A.; Malagoli, P.; Pigatto, P.D.; Amital, H.; et al. The impact of intermittent fasting (Ramadan fasting) on psoriatic arthritis disease activity, enthesitis, and dactylitis: A multicentre study. Nutrients 2019, 11, 601. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Damiani, G.; Watad, A.; Bridgewood, C.; Pigatto, P.D.; Pacifico, A.; Malagoli, P.; Bragazzi, N.L.; Adawi, M. The impact of ramadan fasting on the reduction of PASI score, in moderate-to-severe psoriatic patients: A real-life multicenter study. Nutrients 2019, 11, 277. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Damiani, G.; Mahroum, N.; Pigatto, P.D.; Pacifico, A.; Malagoli, P.; Tiodorovic, D.; Conic, R.R.; Amital, H.; Bragazzi, N.L.; Watad, A.; et al. The safety and impact of a model of intermittent, time-restricted circadian fasting (“ramadan fasting”) on hidradenitis suppurativa: Insights from a multicenter, observational, cross-over, pilot, exploratory study. Nutrients 2019, 11, 1781. [Google Scholar] [CrossRef] [Green Version]
- de Cabo, R.; Mattson, M.P. Effects of intermittent fasting on health, aging, and disease. N. Engl. J. Med. 2019, 381, 2541–2551. [Google Scholar] [CrossRef] [PubMed]
- Hector, A.J.; McGlory, C.; Damas, F.; Mazara, N.; Baker, S.K.; Phillips, S.M. Pronounced energy restriction with elevated protein intake results in no change in proteolysis and reductions in skeletal muscle protein synthesis that are mitigated by resistance exercise. FASEB J. 2018, 32, 265–275. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Burd, N.A.; Tang, J.E.; Moore, D.R.; Phillips, S.M. Exercise training and protein metabolism: Influences of contraction, protein intake, and sex-based differences. J. Appl. Physiol. 2009, 106, 1692–1701. [Google Scholar] [CrossRef]
- Carbone, J.W.; McClung, J.P.; Pasiakos, S.M. Recent advances in the characterization of skeletal muscle and whole-body protein responses to dietary protein and exercise during negative energy balance. Adv. Nutr. 2019, 10, 70–79. [Google Scholar] [CrossRef]
- Rennie, M.J.; Edwards, R.H.T.; Halliday, D.; Matthews, D.E.; Wolman, S.L.; Millward, D.J. Muscle protein synthesis measured by stable isotope techniques in man: The effects of feeding and fasting. Clin. Sci. 1982, 63, 519–523. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Elia, M. Organ and tissue contribution to metabolic rate. In Energy Metabolism: Tissue Determinants and Cellular Corollaries; Kinney, J.M., Tucker, H.N., Eds.; Raven Press: New York, NY, USA, 1992; pp. 61–80. [Google Scholar]
- Leibel, R.L.; Rosenbaum, M.; Hirsch, J. Changes in energy expenditure resulting from altered body weight. N. Engl. J. Med. 1995, 332, 621–628. [Google Scholar] [CrossRef]
- Carey, D.G.; Pliego, G.J.; Raymond, R.L.; Skau, K.B. Body composition and metabolic changes following bariatric surgery: Effects on fat mass, lean mass and basal metabolic rate. Obes. Surg. 2006, 16, 469–477. [Google Scholar] [CrossRef] [PubMed]
- Gupta, P.; Lanca, C.; Gan, A.T.; Soh, P.; Thakur, S.; Tao, Y.; Kumari, N.; Man, R.; Fenwick, E.; Lamoureux, E.L. The association between body composition using dual energy X-ray absorptiometry and type-2 diabetes: A systematic review and meta-analysis of observational studies. Sci. Rep. 2019, 9, 12634. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ho-Pham, L.T.; Nguyen, U.D.; Nguyen, T.V. Association between lean mass, fat mass, and bone mineral density: A meta-analysis. J. Clin. Endocrinol. Metab. 2014, 99, 30–38. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McGregor, R.A.; Cameron-Smith, D.; Poppitt, S.D. It is not just muscle mass: A review of muscle quality, composition and metabolism during ageing as determinants of muscle function and mobility in later life. Longev. Healthspan 2014, 3, 9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zibellini, J.; Seimon, R.V.; Lee, C.M.Y.; Gibson, A.A.; Hsu, M.S.H.; Sainsbury, A. Effect of diet-induced weight loss on muscle strength in adults with overweight or obesity—A systematic review and meta-analysis of clinical trials. Obes. Rev. 2016, 17, 647–663. [Google Scholar] [CrossRef] [PubMed]
- Chaston, T.; Dixon, J.; O’brien, P. Changes in fat-free mass during significant weight loss: A systematic review. Int. J. Obes. 2007, 31, 743–750. [Google Scholar] [CrossRef] [Green Version]
- Miller, C.T.; Fraser, S.F.; Levinger, I.; Straznicky, N.E.; Dixon, J.B.; Reynolds, J.; Selig, S.E. The effects of exercise training in addition to energy restriction on functional capacities and body composition in obese adults during weight loss: A systematic review. PLoS ONE 2013, 8, e81692. [Google Scholar] [CrossRef] [Green Version]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; The PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [Green Version]
- Keenan, S.; Belski, R. The Impact of Intermittent Fasting Combined with Exercise on Body Composition in Non-Athlete Populations: A Systematic Review. PROSPERO 2018 CRD42018103867. Available online: https://www.crd.york.ac.uk/prospero/display_record.php?ID=CRD42018103867 (accessed on 5 August 2020).
- Downs, S.H.; Black, N. The feasibility of creating a checklist for the assessment of the methodological quality both of randomised and non-randomised studies of health care interventions. J. Epidemiol. Community Health 1998, 52, 377–384. [Google Scholar] [CrossRef] [Green Version]
- Alhamdan, B.; Garcia-Alvarez, A.; Alzahrnai, A.; Karanxha, J.; Stretchberry, D.R.; Contrera, K.J.; Utria, A.F.; Cheskin, L.J. Alternate-day versus daily energy restriction diets: Which is more effective for weight loss? A systematic review and meta-analysis. Obes. Sci. Pract. 2016, 2, 293–302. [Google Scholar] [CrossRef] [PubMed]
- Moro, T.; Tinsley, G.; Bianco, A.; Marcolin, G.; Pacelli, Q.F.; Battaglia, G.; Palma, A.; Gentil, P.; Neri, M.; Paoli, A. Effects of eight weeks of time-restricted feeding (16/8) on basal metabolism, maximal strength, body composition, inflammation, and cardiovascular risk factors in resistance-trained males. J. Transl. Med. 2016, 14, 290. [Google Scholar] [CrossRef] [PubMed]
- Tinsley, G.M.; Forsse, J.S.; Butler, N.K.; Paoli, A.; Bane, A.A.; La Bounty, P.M.; Morgan, G.B.; Grandjean, P.W. Time-restricted feeding in young men performing resistance training: A randomized controlled trial. Eur. J. Sport Sci. 2017, 17, 200–207. [Google Scholar] [CrossRef] [PubMed]
- Tinsley, G.M.; Moore, M.L.; Graybeal, A.J.; Paoli, A.; Youngdeok, K.; Gonzales, J.U.; Harry, J.R.; VanDusseldorp, T.A.; Kennedy, D.N.; Cruz, M.R. Time-restricted feeding plus resistance training in active females: A randomized trial. Am. J. Clin. Nutr. 2019, 110, 628–640. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stratton, M.T.; Tinsley, G.M.; Alesi, M.G.; Hester, G.M.; Olmos, A.A.; Serafini, P.R.; Modjeski, A.S.; Mangine, G.T.; King, K.; Savage, S.N.; et al. Four Weeks of Time-Restricted Feeding Combined with Resistance Training Does Not Differentially Influence Measures of Body Composition, Muscle Performance, Resting Energy Expenditure, and Blood Biomarkers. Nutrients 2020, 12, 1126. [Google Scholar] [CrossRef]
- Oh, M.; Kim, S.; An, K.Y.; Min, J.; Yang, H.I.; Lee, J.; Lee, M.K.; Kim, D.; Lee, H.; Lee, J.W.; et al. Effects of alternate day calorie restriction and exercise on cardio-metabolic risk factors in overweight and obese adults: An exploratory randomized controlled study. BMC Public Health 2018, 18, 1124. [Google Scholar] [CrossRef]
- Trabelsi, K.; Stannard, S.R.; Ghlissi, Z.; Maughan, R.J.; Kallel, C.; Jamoussi, K.; Zeghal, K.M.; Hakim, A. Effect of fed-versus fasted state resistance training during Ramadan on body composition and selected metabolic parameters in bodybuilders. J. Int. Soc. Sports Nutr. 2013, 10, 23. [Google Scholar] [CrossRef] [Green Version]
- Trabelsi, K.; Stannard, S.R.; Maughan, R.J.; Jammoussi, K.; Zeghal, K.M.; Hakim, A. Effects of resistance training during Ramadan on body composition and markers of renal function, metabolism, inflammation, and immunity in recreational bodybuilders. Int. J. Sport Nutr. Exerc. Metabol. 2012, 22, 267–275. [Google Scholar] [CrossRef]
- Stannard, S.R.; Thompson, M.W. The effect of participation in Ramadan on substrate selection during submaximal cycling exercise. J. Sci. Med. Sport 2008, 11, 510–517. [Google Scholar] [CrossRef]
- Methenitis, S. A brief review on concurrent training: From laboratory to the field. Sports 2018, 6, 127. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Slater, G.J.; Dieter, B.P.; Marsh, D.J.; Helms, E.R.; Shaw, G.; Iraki, J. Is an Energy Surplus Required to Maximize Skeletal Muscle Hypertrophy Associated With Resistance Training. Front. Nutr. 2019, 6, 131. [Google Scholar] [CrossRef]
- Fry, A.C. The role of resistance exercise intensity on muscle fibre adaptations. Sports Med. 2004, 34, 663–679. [Google Scholar] [CrossRef] [PubMed]
- Schoenfeld, B.J. The mechanisms of muscle hypertrophy and their application to resistance training. J. Strength Cond. Res. 2010, 24, 2857–2872. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grgic, J.; Schoenfeld, B.J.; Latella, C. Resistance training frequency and skeletal muscle hypertrophy: A review of available evidence. J. Sci. Med. Sport 2019, 22, 361–370. [Google Scholar] [CrossRef] [PubMed]
- Stokes, T.; Hector, A.J.; Morton, R.W.; McGlory, C.; Phillips, S.M. Recent perspectives regarding the role of dietary protein for the promotion of muscle hypertrophy with resistance exercise training. Nutrients 2018, 10, 180. [Google Scholar] [CrossRef] [Green Version]
- Stote, K.S.; Baer, D.J.; Spears, K.; Paul, D.R.; Harris, K.G.; Rumpler, W.V.; Strycula, P.; Najjer, S.S.; Ferrucci, L.; Ingram, D.K.; et al. A controlled trial of reduced meal frequency without caloric restriction in healthy, normal-weight, middle-aged adults. Am. J. Clin. Nutr. 2007, 85, 981–988. [Google Scholar] [CrossRef]
- Beer, S.F.; Bircham, P.M.M.; Bloom, S.R.; Clark, P.M.; Hales, C.N.; Hughes, C.M.; Jones, C.T.; Marsh, D.R.; Raggatt, P.R.; Findlay, A.L.R. The effect of a 72-h fast on plasma levels of pituitary, adrenal, thyroid, pancreatic and gastrointestinal hormones in healthy men and women. J. Endocrinol. 1989, 120, 337–350. [Google Scholar] [CrossRef]


{kind=link}
| Author, Year | Participant Baseline Characteristics | Drop Outs (Final Number of Completers) | Duration of Study | Description of Fasting | Description of Exercise | Weight Change | Body Composition Changes | Method of Anthropometric Assessment | Quality Score (Downs and Black) | Fasted During Exercise? |
|---|---|---|---|---|---|---|---|---|---|---|
| Time Restricted Feeding Studies | ||||||||||
| Moro et al. (2016) [24] | n = 34 Male Resistance trained (at least 3–5 times/week for 5 years) Time restricted feeding group n = 17 29.9 ± 4.1 years old BMI 26.5 kg/m2 * BF% 13.0% * Control diet group n = 17 28.5 ± 3.5 years old BMI 27.2 kg/m2 * BF% 13.2% * | NR—assumed full completion | 8 weeks | Time restricted feeding 100% of energy needs consumed over 3 meals in an 8 h window (1 p.m., 4 p.m. and 8 p.m.), 20 g of whey protein after training Control 100% of energy needs consumed over 3 meals across the day (8 a.m., 1 p.m. and 8 p.m.), 20 g of whey protein after training | Both groups 3 resistance sessions/week, split routine, 6–8 repetitions at 85–90% of 1 RM to failure, supervised sessions, conducted between 4–6 p.m. | Time restricted feeding ↓ 1.0 kg Control ↑ 0.2 kg | Time restricted feeding LBM ↑ 0.6 kg (NS) FM ↓ 1.6 kg Control LBM ↑ 0.5 kg (NS) FM ↓ 0.3 kg (NS) | DXA | 18 | No |
| Tinsley et al. (2017) [25] | n = 28 Male Both groups recreationally active; have not followed a consistent RT programme over previous 3 months Time restricted feeding group n = 14 22.9 ± 4.0 years old BMI 27.2 kg/m2 * BF% 21.3 ± 5.4% Normal diet group n = 14 22.0 ± 2.4 years old BMI 24.3 kg/m2 * BF% 18.7 ± 3.8% | Time restricted feeding group 1 (13 completers) Normal diet group 5 (9 completers) | 8 weeks | Time restricted feeding 4 days/week (non-training days) all energy consumed in a 4 h window between 4 p.m. and midnight 3 days/week ad libitum Normal diet Usual dietary patterns | Both groups 3 resistance sessions/week on non-consecutive days, alternating upper and lower body, 8–12 reps to failure, 4 sets of each exercise | Time restricted feeding ↓ 1.0 kg (NS) Normal diet ↑ 3.0 kg (NS) Analysis based on n = 10 for time restricted feeders and n = 8 normal diet due to exclusion for low compliance | Time restricted feeding LBM ↓ 0.2 kg (NS) FM ↓ 0.6 kg (NS) Normal diet LBM ↑ 2.3 kg (NS) FM ↑ 0.8 kg (NS) Analysis based on n = 10 for time restricted feeders and n = 8 normal diet due to exclusion for low compliance | DXA | 16 | No |
| Tinsley et al. (2019) [26] | n = 40 Female Resistance trained (2 to 4 sessions per week for at least 1 year); BF% less than 33% Time restricted feeding group n = 13 23.3 ± 1.5 years old BMI 23.8 kg/m2 * BF% 28.4 ± 1.5% Time restricted feeding group plus HMB n = 13 22.3 ± 3.4 years old BMI 22.9 kg/m2 * BF% 28.7 ± 1.5% Control diet group n = 14 22.6 ± 2.7 years old BMI 22.5 kg/m2 * BF% 29.3 ± 1.5% | Time restricted feeding group 1 (12 completers) Time restricted feeding group plus HMB 3 (10 completers) Control diet group 5 (9 completers) | 8 weeks | Time restricted feeding All energy consumed between 12 p.m. and 8 p.m. each day, prescribed energy deficit of 250 kcal and protein of ≥1.4 g/kg/d. Instructed to consume whey protein supplement each day to achieve protein target Time restricted feeding plus HMB Same as time restricted feeding group, plus 3 g/day HMB Control diet group Energy and protein targets as per the time restricted feeding group, however instructed to consume breakfast upon waking, and continue eating at self-selected intervals | All groups 3 resistance sessions/week on non-consecutive days, alternating 2 different upper and lower body sessions Conducted between 12 p.m. and 6 p.m. | Time restricted feeding group ↑ 0.6 kg Time restricted feeding group plus HMB ↑ 0.6 kg Control diet group ↑ 1.1 kg Data from ITT analysis. Results significant for all groups combined | Time restricted feeding group FM ↓ 0.4 kg LBM ↑ 0.9 kg BF% ↓ 0.8% Time restricted feeding group plus HMB FM ↓ 0.7 kg LBM ↑ 1.2 kg BF% ↓ 1.4% Control diet group FM ↑ 0.4 kg LBM ↑ 0.9 kg BF% ↑ 0.1% Data from ITT analysis. Results significant for all groups combined | 4C | 20 | No |
| Stratton et al. (2020) [27] | n = 32 Male Recreationally trained (2–4 sessions per week for at least 6 months) Time restricted feeding group n = 13 22.9 ± 3.6 years old BMI 25.9 kg/m2 * BF% 19.9 ± 8.3% Control diet group n = 13 22.5 ± 2.2 years old BMI 26.4 kg/m2 * BF% 18.9 ± 7.4% | Time restricted feeding group 0 (16 completers Control diet group 2 (14 completers) | 4 weeks | Time restricted feeding All energy consumed between 12 p.m. and 8 p.m., or 1 m and 9 p.m. each day, prescribed 25% energy deficit and protein intake of 1.8 g/kg/d. Provided 50 g whey protein supplement on training days. Control diet group Energy and protein targets as per the time restricted feeding group, but with no time restrictions on consumption. Additionally provided with 50 g whey protein supplement on training days | Both Groups 3 full body resistance sessions/week. Conducted between 3 p.m. and 8 p.m. | Time restricted feeding ↓ 1.2 kg Control diet group ↓ 1.4 kg | Time restricted feeding FM ↓ 1.5 kg LBM NS change (actual values NR) BF% ↓ 1.6% Control diet group FM ↓ 1.4 kg LBM NS change (actual values NR) BF% ↓ 1.5% Analysis based on n = 13 for time restricted feeders and n = 13 for control diet group due to exclusion for low compliance | 4C | 19 | No |
| Modified Alternate Day Fasting Study | ||||||||||
| Oh et al. (2018) [28] | n = 45 Training history unclear, but described as ‘unfamiliar with resistance exercise’ Alternate day fasting + exercise group n = 12 male = 5, female = 7 37.3 ± 7.3 years old BMI 27.5 ± 2.6 kg/m2 BF% 34.2 ± 6.1% Alternate day fasting group n = 13 male = 3, female = 10 32.9 ± 7.3 years old BMI 27.6 ± 2.8 kg/m2 BF% 34.9 ± 4.6% Exercise only group n = 10 male = 7, female = 3 35.7 ± 7.9 years old BMI 28.3 ± 4.1 kg/m2 BF% 31.0 ± 5.0% Normal diet group n = 10 male = 4, female = 6 40.6 ± 10.0 years old BMI 26.3 ± 3.0 kg/m2 BF% 32.2 ± 4.4% | Alternate day fasting + exercise group 2 (10 completers) Alternate day fasting group 4 (9 completers) Exercise only group 2 (8 completers) Normal diet group 2 (8 completers) Sex of drop outs NR | 8 weeks | Alternate day fasting groups 75% Calorie restriction alternating with ad libitum feeding Normal diet/exercise only groups No instruction given | Alternate day fasting + exercise and normal diet + exercise groups 3 training sessions per week consisting of 40 min of resistance training followed by 20 min of aerobic exercise on a treadmill. Resistance training was upper and lower body, 3 different sessions each week. Intensity ranged from 70% 10 RM (15 repetitions) to 100% 10 RM (10 repetitions) and altered each week. Aerobic exercise performed at 60–85% age predicted maximal heart rate | Alternate day fasting + exercise group ↓ 3.3 ± 2.4 kg Alternate day fasting group ↓ 2.4 ± 3.1 kg Exercise only group NS change Normal diet group NS change Data from ITT analysis | Alternate day fasting + exercise FM ↓ 2.7 ± 2.0 kg LBM ↓ 0.4 ± 0.5 kg BF% ↓ 2.5 ± 2.2% Alternate day fasting group FM ↓ 1.6 ± 2.3 kg (NS) LBM ↓ 0.5 ± 0.9 kg (NS) BF% ↓ 1.3 ± 2.4% Exercise only group FM ↓ 1.2 ± 1.9 kg LBM ↓ 0.1 ± 0.9 kg (NS) BF% ↓ 1.1 ± 1.8% (NS) Normal diet group FM ↓ 0.3 ± 1.3 kg (NS) LBM ↓ 0.2 ± 0.7 kg (NS) BF% ↓ 0.1 ± 1.5% (NS) Data from ITT analysis | BIA | 18 | No |
| Ramadan Fasting Studies | ||||||||||
| Trabelsi et al. (2013) [29] | n = 16 Male Resistance trained (3 times/week for 1.6 ± 0.6 and 1.5 ± 0.5 years) Fasted exercise n = 8 25.0 ± 3.0 years old BMI 25.8 ± 4.0 kg/m2 BF% 15.0 ± 2.0% Fed exercise n = 8 25.0 ± 2.0 years old BMI 26.0 ± 1.7 kg/m2 BF% 14.0 ± 1.0% | NR | 4 weeks | Ramadan fasting Average fast 15 h | Both groups 4 resistance sessions/week, 4–6 exercises, 4 sets at 10 RM, split routine, supervised Fasted exercise group Exercise conducted between 4–6 p.m. before breaking fast Fed exercise group Exercise conducted between 9–10 p.m. | NS change in either group | Fasted exercise group LBM ↓ 0.2 kg (NS) BF% ↓ 0.7% (NS) Fed Exercise group LBM ↑ 0.3 kg (NS) BF% ↓ 0.4% (NS) | Skinfolds | 17 | Mixed—exercise conducted between 4–6 p.m. for fasted group, unclear when fast began |
| Trabelsi et al. (2012) [30] | n = 16 Male Recreational bodybuilders (at least 1 year experience) Fasters n = 9 (it is unclear whether this data is duplicated from Trabelsi et al. 2013) 24.0 ± 3.0 years old BMI 26.0 ± 0.7 kg/m2 BF% 14.5 ± 2.0% Non fasters n = 7 26.0 ± 3.0 years old BMI 26.0 ± 1.5 kg/m2 BF% 13.5 ± 1.4% | NR | 4 weeks | Ramadan fasting Average fast 15 h Control group Normal diet | Both groups 4 resistance sessions/week, 4–6 exercises, 4 sets at 10 RM, split routine, supervised | Fasters NS change Non Fasters ↑ 1.9 kg | Fasters FM ↓ 0.6 kg (NS) LBM ↓ 0.1 kg (NS) BF% ↓ 0.7% (NS) Non Fasters FM ↑ 1.2 kg (NS) LBM ↑ 0.7 kg (NS) BF% ↑ 1.1% (NS) | Skinfolds | 16 | Yes—exercise conducted between 4–6 p.m., unclear when fast began |
| Stannard et al. (2008) [31] | n = 8 Male Recreationally active (2–5 sessions/week) 24.1 ± 0.8 years old BMI 24 kg/m2 * BF% 12.9 ± 3.5% | NR | 4 weeks | Ramadan fasting Average fast 14.5 h | 2–5 sessions/week in the ‘weight-training gymnasium’. Type and duration of exercise is unspecified | ↓ 1.3 kg | FM ↓ 0.7 kg LBM ↑ 0.1 kg (NS) BF% ↓ 0.7% (NS) | Underwater weighing | 16 | Unclear |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Keenan, S.; Cooke, M.B.; Belski, R. The Effects of Intermittent Fasting Combined with Resistance Training on Lean Body Mass: A Systematic Review of Human Studies. Nutrients 2020, 12, 2349. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12082349
Keenan S, Cooke MB, Belski R. The Effects of Intermittent Fasting Combined with Resistance Training on Lean Body Mass: A Systematic Review of Human Studies. Nutrients. 2020; 12(8):2349. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12082349
Chicago/Turabian StyleKeenan, Stephen, Matthew B. Cooke, and Regina Belski. 2020. "The Effects of Intermittent Fasting Combined with Resistance Training on Lean Body Mass: A Systematic Review of Human Studies" Nutrients 12, no. 8: 2349. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12082349