Displacing Sedentary Behaviour with Light Intensity Physical Activity Spontaneously Alters Habitual Macronutrient Intake and Enhances Dietary Quality in Older Females

 , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants and Experimental Design
2.2. Anthropometric Assessments
2.3. Assessment of Habitual Dietary Intake
2.4. Recommended Daily Intake and Health-Enhancing Nutrients
2.5. Physical Behaviour Profile
2.6. Energy Balance
2.7. Physical Behaviour Interventions
2.8. Statistical Analysis
3. Results
3.1. Baseline Group Differences
3.2. Habitual Dietary Intake
3.3. Physical Behaviour Profile
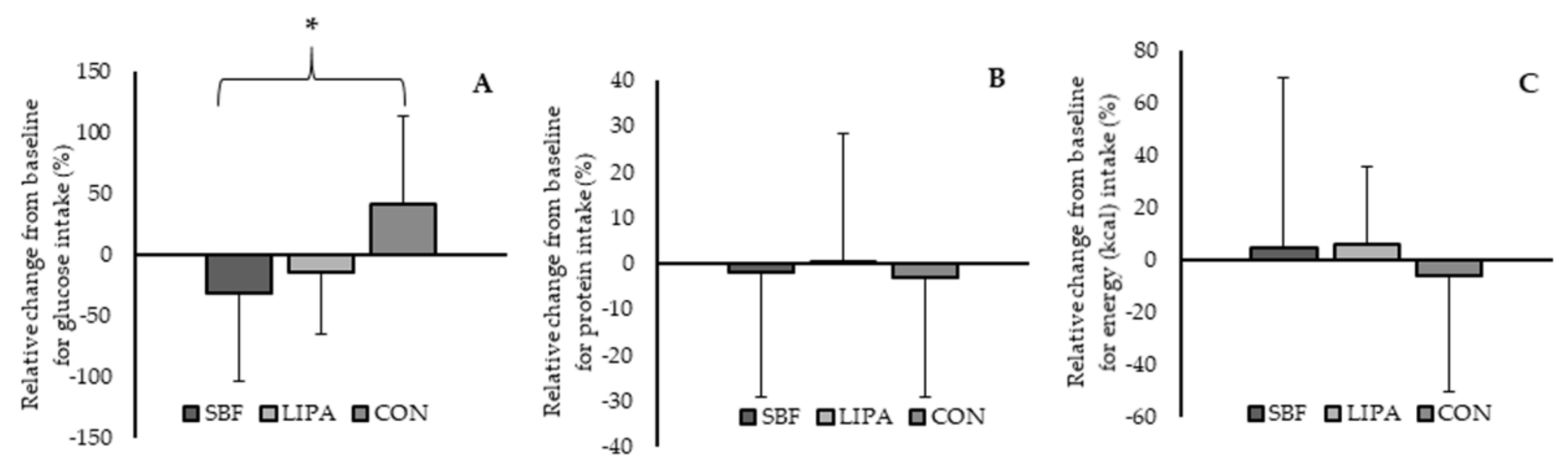
3.4. Carbohydrate Intake as a Factor of Intervention
3.5. Protein Intake as a Factor of Intervention
3.6. Energy Balance as a Factor of Intervention
3.7. Micronutrient Intake as a Factor of Intervention
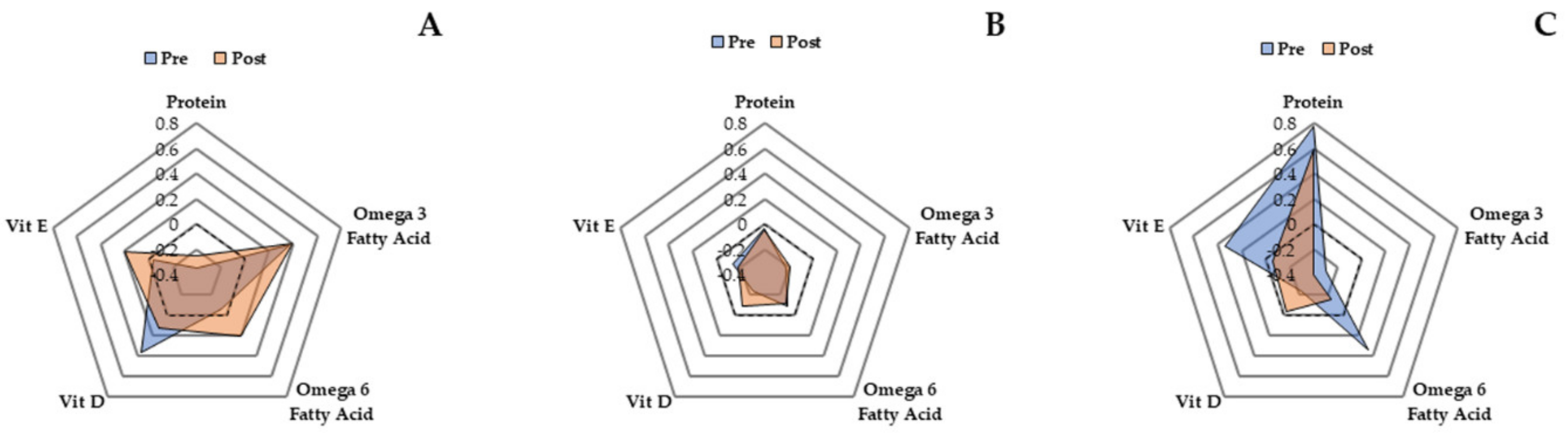
3.8. Dietary Components Promoting Anabolism, as a Factor of the Two Interventions
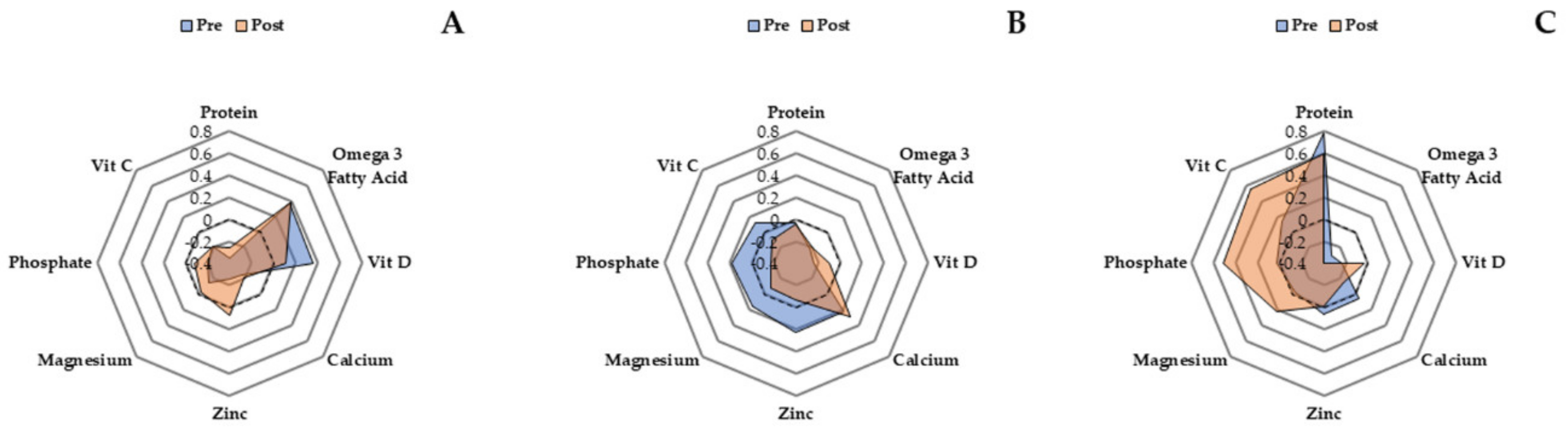
3.9. Dietary Components Promoting Bone Health as a Factor of the Two Interventions
3.10. Effect of Physical Behaviour Classification Change on Habitual Dietary Outcomes
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Global Recommendations on Physical Activity for Health; World Health Organization: Geneva, Switzerland, 2010. [Google Scholar]
- Matthews, C.E.; George, S.M.; Moore, S.C.; Bowles, H.R.; Blair, A.; Park, Y.; Troiano, R.P.; Hollenbeck, A.; Schatzkin, A. Amount of time spent in sedentary behaviors and cause-specific mortality in US adults. Am. J. Clin. Nutr. 2012, 95, 437–445. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ekelund, U.; Tarp, J.; Steene-Johannessen, J.; Hansen, B.H.; Jefferis, B.; Fagerland, M.W.; Whincup, P.; Diaz, K.M.; Hooker, S.P.; Chernofsky, A. Dose-response associations between accelerometry measured physical activity and sedentary time and all cause mortality: systematic review and harmonised meta-analysis. BMJ 2019, 366, l4570. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Rezende, L.F.M.; Rey-López, J.P.; Matsudo, V.K.R.; do Carmo Luiz, O. Sedentary behavior and health outcomes among older adults: a systematic review. Bmc Public Health 2014, 14, 333. [Google Scholar] [CrossRef] [Green Version]
- Ekelund, U.; Steene-Johannessen, J.; Brown, W.J.; Fagerland, M.W.; Owen, N.; Powell, K.E.; Bauman, A.; Lee, I.M. Does physical activity attenuate, or even eliminate, the detrimental association of sitting time with mortality? A harmonised meta-analysis of data from more than 1 million men and women. Lancet 2016, 388, 1302–1310. [Google Scholar] [CrossRef] [Green Version]
- Mansoubi, M.; Pearson, N.; Biddle, S.J.; Clemes, S. The relationship between sedentary behaviour and physical activity in adults: a systematic review. Prev. Med. 2014, 69, 28–35. [Google Scholar] [CrossRef] [PubMed]
- Jefferis, B.J.; Sartini, C.; Ash, S.; Lennon, L.T.; Wannamethee, S.G.; Whincup, P.H. Validity of questionnaire-based assessment of sedentary behaviour and physical activity in a population-based cohort of older men; comparisons with objectively measured physical activity data. Int. J. Behav. Nutr. Phys. Act. 2016, 13, 14. [Google Scholar] [CrossRef] [Green Version]
- Fuezeki, E.; Engeroff, T.; Banzer, W. Health benefits of light-intensity physical activity: a systematic review of accelerometer data of the National Health and Nutrition Examination Survey (NHANES). Sports Med. 2017, 47, 1769–1793. [Google Scholar] [CrossRef]
- Chastin, S.F.; De Craemer, M.; De Cocker, K.; Powell, L.; Van Cauwenberg, J.; Dall, P.; Hamer, M.; Stamatakis, E. How does light-intensity physical activity associate with adult cardiometabolic health and mortality? Systematic review with meta-analysis of experimental and observational studies. Br. J. Sports Med. 2019, 53, 370–376. [Google Scholar] [CrossRef] [Green Version]
- Harvey, J.A.; Chastin, S.F.; Skelton, D.A. Prevalence of sedentary behavior in older adults: a systematic review. Int. J. Environ. Res. Public Health 2013, 10, 6645–6661. [Google Scholar] [CrossRef]
- Wullems, J.A.; Verschueren, S.M.; Degens, H.; Morse, C.I.; Onambélé, G.L. A review of the assessment and prevalence of sedentarism in older adults, its physiology/health impact and non-exercise mobility counter-measures. Biogerontology 2016, 17, 547–565. [Google Scholar] [CrossRef] [Green Version]
- Gennuso, K.P.; Thraen-Borowski, K.M.; Gangnon, R.E.; Colbert, L.H. Patterns of sedentary behavior and physical function in older adults. Aging Clin. Exp. Res. 2016, 28, 943–950. [Google Scholar] [CrossRef] [PubMed]
- Diaz, K.M.; Howard, V.J.; Hutto, B.; Colabianchi, N.; Vena, J.E.; Safford, M.M.; Blair, S.N.; Hooker, S.P. Patterns of sedentary behavior and mortality in US middle-aged and older adults: a national cohort study. Ann. Intern. Med. 2017, 167, 465–475. [Google Scholar] [CrossRef] [PubMed]
- Reid, N.; Healy, G.; Gianoudis, J.; Formica, M.; Gardiner, P.; Eakin, E.; Nowson, C.A.; Daly, R. Association of sitting time and breaks in sitting with muscle mass, strength, function, and inflammation in community-dwelling older adults. Osteoporos. Int. 2018, 29, 1341–1350. [Google Scholar] [CrossRef] [PubMed]
- Da Silva, V.D.; Tribess, S.; Meneguci, J.; Sasaki, J.E.; Garcia-Meneguci, C.A.; Carneiro, J.A.O.; Virtuoso, J.S. Association between frailty and the combination of physical activity level and sedentary behavior in older adults. BMC Public Health 2019, 19, 709. [Google Scholar] [CrossRef] [Green Version]
- Zhu, K.; Devine, A.; Suleska, A.; Tan, C.; Toh, C.; Kerr, D.; Prince, R. Adequacy and change in nutrient and food intakes with aging in a seven-year cohort study in elderly women. J. Nutr. Health Aging 2010, 14, 723–729. [Google Scholar] [CrossRef]
- Wysokiński, A.; Sobów, T.; Kłoszewska, I.; Kostka, T. Mechanisms of the anorexia of aging—A review. Age 2015, 37, 81. [Google Scholar] [CrossRef]
- Levine, J.A.; Lanningham-Foster, L.M.; McCrady, S.K.; Krizan, A.C.; Olson, L.R.; Kane, P.H.; Jensen, M.D.; Clark, M.M. Interindividual variation in posture allocation: possible role in human obesity. Science 2005, 307, 584–586. [Google Scholar] [CrossRef] [Green Version]
- Shaw, K.; Srikanth, V.; Fryer, J.L.; Blizzard, L.; Dwyer, T.; Venn, A. Dual energy X-ray absorptiometry body composition and aging in a population-based older cohort. Int. J. Obes. 2007, 31, 279–284. [Google Scholar] [CrossRef] [Green Version]
- Rønnow Schacht, S.; Vendelbo Lind, M.; Bechshøft, R.L.; Højfeldt, G.; Reitelseder, S.; Jensen, T.; Pernille Jespersen, A.; Sandris Nielsen, D.; Holm, L.; Tetens, I. Investigating risk of suboptimal macro and micronutrient intake and their determinants in older Danish adults with specific focus on protein intake—a cross-sectional study. Nutrients 2019, 11, 795. [Google Scholar] [CrossRef] [Green Version]
- Carrière; Delcourt; Lacroux; Gerber; POLANUT Study Group. Nutrient intake in an elderly population in southern France (POLANUT): Deficiency in some vitamins, minerals and ω-3 PUFA. Int. J. Vitam. Nutr. Res. 2007, 77, 57–65. [Google Scholar]
- Zhuang, P.; Cheng, L.; Wang, J.; Zhang, Y.; Jiao, J. Saturated fatty acid intake is associated with total mortality in a nationwide cohort study. J. Nutr. 2019, 149, 68–77. [Google Scholar] [CrossRef] [PubMed]
- Zhuang, P.; Wang, W.; Wang, J.; Zhang, Y.; Jiao, J. Polyunsaturated fatty acids intake, omega-6/omega-3 ratio and mortality: Findings from two independent nationwide cohorts. Clin. Nutr. 2019, 38, 848–855. [Google Scholar] [CrossRef] [PubMed]
- Witte, K.K.A.; Clark, A.L.; Cleland, J.G.F. Chronic heart failure and micronutrients. J. Am. Coll. Cardiol. 2001, 37, 1765–1774. [Google Scholar] [CrossRef] [Green Version]
- Conzade, R.; Koenig, W.; Heier, M.; Schneider, A.; Grill, E.; Peters, A.; Thorand, B. Prevalence and predictors of subclinical micronutrient deficiency in german older adults: results from the population-based KORA-age study. Nutrients 2017, 9, 1276. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kehoe, L.; Walton, J.; Flynn, A. Nutritional challenges for older adults in Europe: current status and future directions. Proc. Nutr. Soc. 2019, 78, 221–233. [Google Scholar] [CrossRef]
- Blakely, F.; Dunnagan, T.; Haynes, G.; Moore, S.; Pelican, S. Moderate physical activity and its relationship to select measures of a healthy diet. J. Rural Health 2004, 20, 160–165. [Google Scholar] [CrossRef]
- Tucker, M.; Reicks, M. Exercise as a gateway behavior for healthful eating among older adults: an exploratory study. J. Nutr. Educ. Behav. 2002, 34, S14–S19. [Google Scholar] [CrossRef]
- Tomlinson, D.J.; Erskine, R.M.; Morse, C.I.; Onambélé, G.L. Impact of Above-Average Proanabolic Nutrients Is Overridden by High Protein and Energy Intake in the Muscle-Tendon Unit Characteristics of Middle-to Older-Aged Adults. J. Nutr. 2018, 148, 1776–1785. [Google Scholar] [CrossRef]
- Mackay, A.; Mackay, D.; Celis-Morales, C.; Lyall, D.; Gray, S.; Sattar, N.; Gill, J.; Pell, J.; Anderson, J. The association between driving time and unhealthy lifestyles: a cross-sectional, general population study of 386 493 UK Biobank participants. J. Public Health 2019, 41, 527–534. [Google Scholar] [CrossRef]
- Bowman, S.A. PEER REVIEWED: Television-Viewing Characteristics of Adults: Correlations to Eating Practices and Overweight and Health Status. Prev. Chronic Dis. 2006, 3, A38. [Google Scholar]
- Hu, F.B.; Li, T.Y.; Colditz, G.A.; Willett, W.C.; Manson, J.E. Television watching and other sedentary behaviors in relation to risk of obesity and type 2 diabetes mellitus in women. Jama 2003, 289, 1785–1791. [Google Scholar] [CrossRef] [Green Version]
- Saeidifard, F.; Medina-Inojosa, J.R.; Supervia, M.; Olson, T.P.; Somers, V.K.; Erwin, P.J.; Lopez-Jimenez, F. Differences of energy expenditure while sitting versus standing: A systematic review and meta-analysis. Eur. J. Prev. Cardiol. 2018, 25, 522–538. [Google Scholar] [CrossRef] [PubMed]
- Ohlsson, C.; Hägg, D.A.; Hammarhjelm, F.; Dalmau Gasull, A.; Bellman, J.; Windahl, S.H.; Palsdottir, V.; Jansson, J.-O. The gravitostat regulates fat mass in obese male mice while leptin regulates fat mass in lean male mice. Endocrinology 2018, 159, 2676–2682. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jansson, J.-O.; Palsdottir, V.; Hägg, D.A.; Schéle, E.; Dickson, S.L.; Anesten, F.; Bake, T.; Montelius, M.; Bellman, J.; Johansson, M.E. Body weight homeostat that regulates fat mass independently of leptin in rats and mice. Proc. Natl. Acad. Sci. USA 2018, 115, 427–432. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bailey, D.P.; Broom, D.R.; Chrismas, B.C.; Taylor, L.; Flynn, E.; Hough, J. Breaking up prolonged sitting time with walking does not affect appetite or gut hormone concentrations but does induce an energy deficit and suppresses postprandial glycaemia in sedentary adults. Appl. Physiol. Nutr. Metab. 2016, 41, 324–331. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Palsdottir, V.; Windahl, S.H.; Hägg, D.A.; Keantar, H.; Bellman, J.; Buchanan, A.; Vaughan, T.J.; Lindén, D.; Jansson, J.-O.; Ohlsson, C. Interactions between the gravitostat and the fibroblast growth factor system for the regulation of body weight. Endocrinology 2019, 160, 1057–1064. [Google Scholar] [CrossRef]
- Knäuper, B.; Rabiau, M.; Cohen, O.; Patriciu, N. Compensatory health beliefs: scale development and psychometric properties. Psychol. Health 2004, 19, 607–624. [Google Scholar] [CrossRef]
- Schoeller, D.A. Limitations in the assessment of dietary energy intake by self-report. Metabolism 1995, 44, 18–22. [Google Scholar] [CrossRef]
- Basiotis, P.P.; Welsh, S.O.; Cronin, F.J.; Kelsay, J.L.; Mertz, W. Number of days of food intake records required to estimate individual and group nutrient intakes with defined confidence. J. Nutr. 1987, 117, 1638–1641. [Google Scholar] [CrossRef]
- Scientific Advisory Committee on Nutrition. Dietary Reference Values for Energy; The Stationery Office: London, UK, 2012. [Google Scholar]
- DeSalvo, K.B.; Olson, R.; Casavale, K.O. Dietary guidelines for Americans. Jama 2016, 315, 457–458. [Google Scholar] [CrossRef] [Green Version]
- Tomlinson, D.J.; Erskine, R.M.; Morse, C.I.; Onambélé, G.L. Body fat percentage, body mass index, fat mass index and the ageing bone: their singular and combined roles linked to physical activity and diet. Nutrients 2019, 11, 195. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Campbell, W.W.; Leidy, H.J. Dietary protein and resistance training effects on muscle and body composition in older persons. J. Am. Coll. Nutr. 2007, 26, 696S–703S. [Google Scholar] [CrossRef] [PubMed]
- Dhesi, J.K.; Jackson, S.H.D.; Bearne, L.M.; Moniz, C.; Hurley, M.V.; Swift, C.G.; Allain, T.J. Vitamin D supplementation improves neuromuscular function in older people who fall. Age Ageing 2004, 33, 589–595. [Google Scholar] [CrossRef] [Green Version]
- Zhu, K.; Austin, N.; Devine, A.; Bruce, D.; Prince, R.L. A randomized controlled trial of the effects of vitamin D on muscle strength and mobility in older women with vitamin D insufficiency. J. Am. Geriatr. Soc. 2010, 58, 2063–2068. [Google Scholar] [CrossRef] [PubMed]
- Taghiyar, M.; Darvishi, L.; Askari, G.; Feizi, A.; Hariri, M.; Mashhadi, N.S.; Ghiasvand, R. The effect of vitamin C and e supplementation on muscle damage and oxidative stress in female athletes: a clinical trial. Int. J. Prev. Med. 2013, 4, S16. [Google Scholar]
- Jouris, K.B.; McDaniel, J.L.; Weiss, E.P. The effect of omega-3 fatty acid supplementation on the inflammatory response to eccentric strength exercise. J. Sports Sci. Med. 2011, 10, 432. [Google Scholar]
- Castillero, E.; Martín, A.I.; López-Menduiña, M.; Villanúa, M.A.; López-Calderón, A. Eicosapentaenoic acid attenuates arthritis-induced muscle wasting acting on atrogin-1 and on myogenic regulatory factors. Am. J. Physiol. Regul. Integr. Comp. Physiol. 2009, 297, R1322–R1331. [Google Scholar] [CrossRef]
- Holbrook, T.; Barrett-Connor, E.; Wingard, D. Dietary calcium and risk of hip fracture: 14-year prospective population study. Lancet 1988, 332, 1046–1049. [Google Scholar] [CrossRef]
- Castiglioni, S.; Cazzaniga, A.; Albisetti, W.; Maier, J.A.M. Magnesium and osteoporosis: current state of knowledge and future research directions. Nutrients 2013, 5, 3022–3033. [Google Scholar] [CrossRef] [Green Version]
- Penido, M.G.M.G.; Alon, U.S. Phosphate homeostasis and its role in bone health. Pediatric Nephrol. 2012, 27, 2039–2048. [Google Scholar] [CrossRef] [Green Version]
- Holick, M.F. Vitamin D and bone health. J. Nutr. 1996, 126, 1159S–1164S. [Google Scholar] [CrossRef] [PubMed]
- Bonjour, J.-P. Protein intake and bone health. Int. J. Vitam. Nutr. Res. 2011, 81, 134. [Google Scholar] [CrossRef] [PubMed]
- Orchard, T.S.; Pan, X.; Cheek, F.; Ing, S.W.; Jackson, R.D. A systematic review of omega-3 fatty acids and osteoporosis. Br. J. Nutr. 2012, 107, S253–S260. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wullems, J.A.; Verschueren, S.M.; Degens, H.; Morse, C.I.; Onambele, G.L. Performance of thigh-mounted triaxial accelerometer algorithms in objective quantification of sedentary behaviour and physical activity in older adults. PLoS ONE 2017, 12, e0188215. [Google Scholar] [CrossRef] [Green Version]
- Harris, J.A.; Benedict, F.G. A biometric study of human basal metabolism. Proc. Natl. Acad. Sci. United States Am. 1918, 4, 370. [Google Scholar] [CrossRef] [Green Version]
- Siervo, M.; Bertoli, S.; Battezzati, A.; Wells, J.C.; Lara, J.; Ferraris, C.; Tagliabue, A. Accuracy of predictive equations for the measurement of resting energy expenditure in older subjects. Clin. Nutr. 2014, 33, 613–619. [Google Scholar] [CrossRef]
- Turner, J.E.; Markovitch, D.; Betts, J.A.; Thompson, D. Nonprescribed physical activity energy expenditure is maintained with structured exercise and implicates a compensatory increase in energy intake. Am. J. Clin. Nutr. 2010, 92, 1009–1016. [Google Scholar] [CrossRef] [Green Version]
- Schofield, W.N. Predicting basal metabolic rate, new standards and review of previous work. Hum. Nutrition. Clin. Nutr. 1985, 39, 5–41. [Google Scholar]
- Joint, F.A.O. Energy and Protein Requirements: Report of a Joint FAO/WHO/UNU Expert Consultation; Technical Report Series (WHO); World Health Organization: Geneva, Switzerland, 1985. [Google Scholar]
- Ainsworth, B.E.; Haskell, W.L.; Herrmann, S.D.; Meckes, N.; Bassett, D.R., Jr.; Tudor-Locke, C.; Greer, J.L.; Vezina, J.; Whitt-Glover, M.C.; Leon, A.S. 2011 Compendium of Physical Activities: A second update of codes and MET values. Med. Sci. Sports Exerc. 2011, 43, 1575–1581. [Google Scholar] [CrossRef] [Green Version]
- Joo, J.; Williamson, S.A.; Vazquez, A.I.; Fernandez, J.R.; Bray, M.S. The influence of 15-week exercise training on dietary patterns among young adults. Int. J. Obes. 2019, 43, 1681–1690. [Google Scholar] [CrossRef]
- Schulze, M.B.; Manson, J.E.; Ludwig, D.S.; Colditz, G.A.; Stampfer, M.J.; Willett, W.C.; Hu, F.B. Sugar-sweetened beverages, weight gain, and incidence of type 2 diabetes in young and middle-aged women. Jama 2004, 292, 927–934. [Google Scholar] [CrossRef]
- Mackenzie, T.; Brooks, B.; O’Connor, G. Beverage intake, diabetes, and glucose control of adults in America. Ann. Epidemiol. 2006, 16, 688–691. [Google Scholar] [CrossRef] [PubMed]
- Houston, D.K.; Nicklas, B.J.; Ding, J.; Harris, T.B.; Tylavsky, F.A.; Newman, A.B.; Lee, J.S.; Sahyoun, N.R.; Visser, M.; Kritchevsky, S.B. Dietary protein intake is associated with lean mass change in older, community-dwelling adults: the Health, Aging, and Body Composition (Health ABC) Study. Am. J. Clin. Nutr. 2008, 87, 150–155. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aparicio-Ugarriza, R.; Luzardo-Socorro, R.; Palacios, G.; Bibiloni, M.; Argelich, E.; Tur, J.; González-Gross, M. What is the relationship between physical fitness level and macro-and micronutrient intake in Spanish older adults? Eur. J. Nutr. 2019, 58, 1579–1590. [Google Scholar] [CrossRef] [PubMed]
- World Health, O.; United Nations, U. Protein and Amino Acid Requirements in Human Nutrition; World Health Organization: Geneva, Switzerland, 2007; Volume 935. [Google Scholar]
- Morley, J.E.; Argiles, J.M.; Evans, W.J.; Bhasin, S.; Cella, D.; Deutz, N.E.P.; Doehner, W.; Fearon, K.C.H.; Ferrucci, L.; Hellerstein, M.K. Nutritional recommendations for the management of sarcopenia. J. Am. Med Dir. Assoc. 2010, 11, 391–396. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Deutz, N.E.P.; Bauer, J.M.; Barazzoni, R.; Biolo, G.; Boirie, Y.; Bosy-Westphal, A.; Cederholm, T.; Cruz-Jentoft, A.; Krznariç, Z.; Nair, K.S. Protein intake and exercise for optimal muscle function with aging: recommendations from the ESPEN Expert Group. Clin. Nutr. 2014, 33, 929–936. [Google Scholar] [CrossRef] [Green Version]
- Paddon-Jones, D.; Leidy, H. Dietary protein and muscle in older persons. Curr. Opin. Clin. Nutr. Metab. Care 2014, 17, 5. [Google Scholar] [CrossRef] [Green Version]
- Phillips, S.M.; Chevalier, S.; Leidy, H.J. Protein “requirements” beyond the RDA: implications for optimizing health. Appl. Physiol. Nutr. Metab. 2016, 41, 565–572. [Google Scholar] [CrossRef] [Green Version]
- Lerma, N.L.; Keenan, K.G.; Strath, S.J.; Forseth, B.M.; Cho, C.C.; Swartz, A.M. Muscle activation and energy expenditure of sedentary behavior alternatives in young and old adults. Physiol. Meas. 2016, 37, 1686. [Google Scholar] [CrossRef] [Green Version]
- Onambele-Pearson, G.; Wullems, J.; Doody, C.; Ryan, D.; Morse, C.; Degens, H. Influence of Habitual Physical Behavior–Sleeping, Sedentarism, Physical Activity–On Bone Health in Community-Dwelling Older People. Front. Physiol. 2019, 10, 408. [Google Scholar] [CrossRef] [Green Version]
- Hill, T.; Meunier, N.; Andriollo-Sanchez, M.; Ciarapica, D.; Hininger-Favier, I.; Polito, A.; O’Connor, J.M.; Coudray, C.; Cashman, K.D. The relationship between the zinc nutritive status and biochemical markers of bone turnover in older European adults: The ZENITH study. Eur. J. Clin. Nutr. 2005, 59, S73–S78. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Dronkelaar, C.; van Velzen, A.; Abdelrazek, M.; van der Steen, A.; Weijs, P.J.M.; Tieland, M. Minerals and sarcopenia; the role of calcium, iron, magnesium, phosphorus, potassium, selenium, sodium, and zinc on muscle mass, muscle strength, and physical performance in older adults: a systematic review. J. Am. Med. Dir. Assoc. 2018, 19, 6–11. [Google Scholar] [CrossRef] [PubMed]
- Little, P.J.; Bhattacharya, R.; Moreyra, A.E.; Korichneva, I.L. Zinc and cardiovascular disease. Nutrition 2010, 26, 1050–1057. [Google Scholar] [CrossRef] [PubMed]
- Reginster, J.-Y. Trace elements and postmenopausal osteoporosis: a preliminary study of decreased serum manganese. Med. Sci. Res. 1988, 16, 337–338. [Google Scholar]
- Alghadir, A.H.; Gabr, S.A.; Al-Eisa, E.S.; Alghadir, M.H. Correlation between bone mineral density and serum trace elements in response to supervised aerobic training in older adults. Clin. Interv. Aging 2016, 11, 265. [Google Scholar]
- Stelmach-Mardas, M.; Kleiser, C.; Uzhova, I.; Peñalvo, J.L.; La Torre, G.; Palys, W.; Lojko, D.; Nimptsch, K.; Suwalska, A.; Linseisen, J.; et al. Seasonality of food groups and total energy intake: a systematic review and meta-analysis. Eur. J. Clin. Nutr. 2016, 70, 700–708. [Google Scholar] [CrossRef]
- O’Connell, S.E.; Griffiths, P.L.; Clemes, S.A. Seasonal variation in physical activity, sedentary behaviour and sleep in a sample of UK adults. Ann. Hum. Biol. 2014, 41, 1–8. [Google Scholar] [CrossRef]
- Merchant, A.T.; Dehghan, M.; Akhtar-Danesh, N. Seasonal Variation in Leisure-time Physical Activity Among Canadians. Can. J. Public Health 2007, 98, 203–208. [Google Scholar] [CrossRef]
- McArdle, W.D.; Katch, F.I.; Katch, V.L. Essentials of Exercise Physiology; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2006. [Google Scholar]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Group | |||
|---|---|---|---|
| SBF(n = 14) | LIPA (n = 14) | CONTROL (n = 7) | |
| Age (years) | 75 ± 7 | 72 ± 12 | 68 ± 4 |
| Weight (kg) | 69 ± 11 | 66 ± 9 | 67 ± 9 |
| Body Mass Index (kg/m2) | 26.9 ± 3.6 | 25.3 ± 3.6 | 26.9 ± 3.4 |
| Proportion classified as Obese/Overweight (Normal) | 14%/57% (29%) | 14%/43% (43%) | 14%/72% (14%) |
| Polypharmacy(n) | 2 ± 4 | 0 ± 1 | 1 ± 3 |
| Nutritional supplements(n) | 0 ± 1 | 0 ± 1 | 1 ± 1 |
| FRAT (number of positive responses) | 1 ± 1 | 1 ± 1 | 0 ± 1 |
| Proportion who live alone (cohabitate) | 36% (64%) | 43% (57%) | 71% (29%) |
| Sedentary Behaviour (hrs/24 h) | 9.7 ± 2.0 | 9.3 ± 1.5 | 8.9 ± 2.0 |
| LIPA (hrs/24 h) | 2.1 ± 0.7 | 2.2 ± 0.6 | 2.0 ± 1.5 |
| Sedentary Behaviour (% of 24 h time) | 60 ± 7 | 62 ± 7 | 53 ± 13 |
| LIPA (% of 24 h time) | 14 ± 3 | 13 ± 2 | 15 ± 4 |
| LIPA (% of PA time) | 37 ± 5 | 35 ± 4 | 29 ± 7 |
| Weekly MVPA time (≥10 min Bouts) | 77 ± 183 | 51 ± 65 | 51 ± 130 |
| Proportion classified as Sedentary (Ambulatory) | 71% (29%) | 79% (21%) | 43% (57%) |
| Proportion classified as Active (Inactive) | 29% (71%) | 0% (100%) | 14% (86%) |
| Basal Metabolic Rate (kcal) (Harris–Benedict) | 1252 ± 125 | 1230 ± 77 | 1256 ± 95 |
| Metabolic Balance (kcal) (Harris-Benedict) | −98 ± 626 | 72 ± 546 | 243 ± 419 |
| Basal Metabolic Rate (kcal) (Schofield) | 1281 ± 102 | 1253 ± 78 | 1270 ± 79 |
| Metabolic Balance (kcal) (Schofield) | −311 ± 607 | −80 ± 528 | 74 ± 489 |
| Proportion consuming optimal levels of ≥3/5 pro anabolic nutrients | 43% | 29% | 29% |
| Proportion consuming optimal levels of ≥5/8 bone health enhancing nutrients | 36% | 50% | 57% |
| Intervention Outcomes | |||
| Intervention Length (Days) | 57 ± 2 | 56 ± 1 | 54 ± 5 |
| Proportion who begun intervention in Spring/Summer (Autumn/Winter) | 36% (64%) | 36% (64%) | 100% (0%) |
| Proportion who shifted classification from sedentary to ambulatory (stable) | 21% (79%) | 21% (79%) | 29% (71%) |
| SBF (n = 14) | LIPA (n = 14) | CONTROL (n = 7) | ||||
|---|---|---|---|---|---|---|
| Baseline | Week 8 | Baseline | Week 8 | Baseline | Week 8 | |
| Energy (Kcal) | 1371 ± 616 | 1468 ± 699 | 1543 ± 509 | 1602 ± 350 | 1825 ± 679 | 1546 ± 557 |
| Energy (Kj) | 5740 ± 2566 | 6150 ± 2911 | 6479 ± 2118 | 6715 ± 1478 | 7653 ± 2799 | 6483 ± 2351 |
| Protein (g) | 66 ± 11 | 65 ± 20 * | 71 ± 18 | 69 ± 16 * | 84 ± 15 | 80 ± 12 * |
| Relative Protein intake (g/kg) | 1.00 ± 0.30 | 0.98 ± 0.40 | 1.11 ± 0.32 | 1.06 ± 0.23 | 1.29 ± 0.18 | 1.20 ± 0.24 |
| Portions of Fruit consumed (n) | 2 ± 1 | 2 ± 2 | 3 ± 2 | 3 ± 2 | 3 ± 1 | 3 ± 2 |
| Portions of Vegetables consumed (n) | 2 ± 5 | 2 ± 1 | 2 ± 1 | 2 ± 1 | 2 ± 1 | 2 ± 1 |
| Carbohydrate (g) | 144 ± 38 | 144 ± 51 * | 177 ± 48 | 174 ± 45 * | 187 ± 36 | 186 ± 57 * |
| Relative carbohydrate intake (g/kg) | 2.04 ± 1.00 | 2.03 ± 0.97 | 2.85 ± 0.71 | 2.78 ± 0.60 | 2.93 ± 0.67 | 2.56 ± 1.51 |
| Glucose (g) | 13.4 ± 6.4 | 10.5 ± 5.1× | 15.4 ± 5.8 | 13.8 ± 7.2× | 14.3 ± 4.5 | 19.7 ± 7.3× |
| Fructose (g) | 17 ± 8 | 15 ± 7 | 19 ± 7 | 16 ± 9 | 17 ± 5 | 20 ± 7 |
| Maltose (g) | 1.2 ± 0.8 | 1.3 ± 1.0 | 1.7 ± 0.7 | 1.8 ± 0.9 | 2.0 ± 1.2 | 2.0 ± 2.6 |
| Sucrose (g) | 18.5 ± 10.3 | 16.2 ± 6.9 | 23.5 ± 12.5 | 25.1 ± 13.1 | 18.5 ± 11.5 | 16.7 ± 8.3 |
| Galactose (g) | 1.1 ± 1.3 | 0.4 ± 0.6 | 1.2 ± 2.2 | 0.3 ± 0.4 | 0.8 ± 1.0 | 0.9 ± 1.7 |
| Lactose (g) | 12.7 ± 8.4 | 10.2 ± 5.4 | 15.5 ± 8.4 | 13.1 ± 6.7 | 10.7 ± 2.2 | 11.0 ± 5.3 |
| Starch (g) | 66 ± 35 | 72 ± 51 | 70 ± 31 | 79 ± 43 | 80 ± 29 | 87 ± 57 |
| Total Sugars (g) | 71.2 ± 38.4 | 65.6 ± 47.9 | 96.9 ± 47.9 | 75.8 ± 25.6 | 83.4 ± 35.4 | 86.7 ± 44.2 |
| Non-starch Polysaccharides (g) | 15.0 ± 3.0 | 15.2 ± 4.7 | 15.7 ± 6.0 | 15.6 ± 6.7 | 18.4 ± 5.1 | 15.8 ± 4.1 |
| Total Fat (g) | 64 ± 32 | 69 ± 31 | 66 ± 19 | 67 ± 23 | 75 ± 27 | 67 ± 23 |
| Saturated Fatty Acids (g) | 21 ± 22 | 20 ± 13 | 23 ± 19 | 23 ± 10 | 26 ± 8 | 21 ± 17 |
| Mono-Unsaturated Fatty Acids (g) | 21 ± 17 | 20 ± 21 | 21 ± 14 | 20 ± 9 | 22 ± 12 | 20 ± 11 |
| Poly-Unsaturated Fatty Acids (g) | 8 ± 8 | 11 ± 7 | 8 ± 4 | 10 ± 8 | 13 ± 5 | 9 ± 3 |
| Trans Fatty Acids (g) | 0.5 ± 0.6 | 0.6 ± 0.4 | 0.6 ± 0.6 | 0.8 ± 0.5 | 0.7 ± 0.2 | 0.5 ± 1.0 |
| Omega-3 Fatty Acids (g) | 2.6 ± 2.5 | 1.6 ± 3.5 | 1.3 ± 1.4 | 1.9 ± 1.8 | 1.2 ± 1.3 | 0.8 ± 1.2 |
| Omega-6 Fatty Acids (g) | 5.8 ± 5.5 | 7.9 ± 10.4 | 5.6 ± 4.5 | 5.6 ± 4.6 | 7.9 ± 5.4 | 5.3 ± 3.5 |
| Vitamin A (μg) | 908 ± 812 | 989 ± 792 | 836 ± 429 | 1052 ± 1139 | 582 ± 139 | 754 ± 528 |
| Vitamin B1 (mg) | 1.2 ± 0.3 | 1.2 ± 0.9 | 1.5 ± 0.7 | 1.4 ± 0.8 | 1.3 ± 0.3 | 1.2 ± 0.7 |
| Vitamin B2 (mg) | 1.6 ± 0.9 | 1.6 ± 0.8 | 1.6 ± 0.4 | 1.5 ± 0.4 | 1.8 ± 0.7 | 1.4 ± 0.9 |
| Vitamin B3 (mg) | 13.3 ± 12.9 | 13.0 ± 5.1 | 14.0 ± 7.3 | 13.0 ± 15.3 | 17.1 ± 14.0 | 15.1 ± 6.3 |
| Vitamin B6 (mg) | 1.7 ± 0.4 | 1.4 ± 0.5 | 1.8 ± 0.9 | 1.3 ± 0.6 | 1.7 ± 0.8 | 1.7 ± 0.4 |
| Vitamin B9 (μg) | 243 ± 103 | 232 ± 73 | 267 ± 141 | 219 ± 108 | 206 ± 156 | 256 ± 82 |
| Vitamin B12 (μg) | 5.0 ± 3.0 | 4.4 ± 3.6 | 4.1 ± 2.8 | 4.7 ± 4.0 | 4.5 ± 2.5 | 5.0 ± 4.3 |
| Vitamin C (mg) | 101 ± 49 | 95 ± 61 | 116 ± 54 | 100 ± 55 | 117 ± 51 | 139 ± 69 |
| Vitamin D (μg) | 4.9 ± 4.2 | 3.8 ± 5.3 | 3.6 ± 4.3 | 3.6 ± 4.1 | 3.1 ± 2.0 | 4.2 ± 3.8 |
| Vitamin E (mg) | 7.4 ± 4.1 | 7.7 ± 5.8 | 7.3 ± 7.1 | 6.7 ± 4.2 | 10.7 ± 4.2 | 7.4 ± 3.9 |
| Calcium (mg) | 727 ± 295 | 702 ± 251 | 867 ± 350 | 882 ± 466 | 817 ± 194 | 724 ± 249 |
| Chloride (mg) | 2400 ± 1233 | 3033 ± 2506 | 2739 ± 1294 | 2472 ± 873 | 2646 ± 852 | 3105 ± 1109 |
| Copper (mg) | 1.2 ± 0.5 | 1.4 ± 1.0 | 1.4 ± 0.6 | 1.1 ± 0.3 | 1.3 ± 0.5 | 1.5 ± 0.5 |
| Iodine (ug) | 183 ± 168 | 149 ± 98 | 154 ± 67 | 137 ± 47 | 138 ± 70 | 186 ± 89 |
| Iron (mg) | 8.9 ± 2.5 | 9.4 ± 5.7 | 9.9 ± 3.3 | 9.1 ± 3.6 | 16.6 ± 17.5 | 10.3 ± 1.8 |
| Magnesium (mg) | 297 ± 93 | 285 ± 120 | 325 ± 102 | 280 ± 60 | 307 ± 82 | 306 ± 75 |
| Manganese (mg) | 3.3 ± 0.8 | 3.8 ± 2.5 | 4.3 ± 2.7 | 3.6 ± 1.2 | 4.0 ± 0.8 | 4.0 ± 1.4 |
| Phosphorous (mg) | 1159 ± 332 | 1084 ± 337 | 1285 ± 367 | 1055 ± 374 | 1234 ± 182 | 1283 ± 208 |
| Potassium (mg) | 2882 ± 544 | 2551 ± 724 | 3250 ± 786 | 2798 ± 588 | 2819 ± 644 | 3000 ± 455 |
| Selenium (μg) | 55.8 ± 22.9 | 51.7 ± 48.8 | 45.8 ± 21.1 | 43.8 ± 22.3 | 53.3 ± 20.3 | 58.2 ± 22.8 |
| Sodium (mg) | 1459 ± 804 | 1775 ± 1518 | 1833 ± 1030 | 1447 ± 536 | 1672 ± 679 | 1914 ± 720 |
| Zinc (mg) | 6.7 ± 4.8 | 7.9 ± 3.9 | 7.3 ± 4.8 | 6.9 ± 3.6 | 7.9 ± 2.1 | 8.5 ± 2.8 |
| Alcohol (g) | 0 ± 11 | 0 ± 8 | 4 ± 10 | 4 ± 24 | 7 ± 9 | 16 ± 18 |
| Recommended Daily Amount (RDA) | Whole Sample at Baseline (n = 35) | SBF (n = 14) | LIPA (n = 14) | CONTROL (n = 7) | ||||
|---|---|---|---|---|---|---|---|---|
| Group Average Expressed as %RDA | ||||||||
| Proportion Meeting RDA | Pre | Post | Pre | Post | Pre | Post | ||
| Protein (g/kg) | ≥0.8 g/kg/day | 31/35 | 125% | 123% | 139% | 133% | 161% | 150% |
| Carbohydrate (g) | Within 45–65% Daily caloric intake | 10/35 | 93% | 87% | 102% | 96% | 91% | 107% |
| Total Fat (g) | ≤35% Daily caloric intake | 14/35 | 120% | 121% | 110% | 108% | 106% | 111% |
| Saturated Fatty Acids (g) | <11% of Daily caloric intake | 10/35 | 125% | 111% | 122% | 118% | 117% | 111% |
| Trans Fatty Acids (g) | <2% of Daily caloric intake | 35/35 | 16% | 18% | 17% | 22% | 17% | 14% |
| Mono-Unsaturated Fatty Acids (g) | ≥28 g/day | 10/35 | 75% | 71% | 75% | 71% | 79% | 71% |
| Poly-Unsaturated Fatty Acids (g) | ≥14 g/day | 6/35 | 57% | 79% | 57% | 71% | 93% | 64% |
| Omega-3 Fatty Acids (g) | ≥1.6 g/day | 12/35 | 163% | 100% | 81% | 119% | 75% | 50% |
| Omega-6 Fatty Acids (g) | ≥10 g/day | 6/35 | 58% | 79% | 56% | 56% | 79% | 53% |
| Vitamin A (μg) | ≥600 µg/day | 23/35 | 151% | 165% | 139% | 175% | 97% | 126% |
| Vitamin B1 (mg) | ≥0.8 mg/day | 33/35 | 150% | 150% | 188% | 175% | 163% | 150% |
| Vitamin B2 (mg) | ≥1.1 mg/day | 32/35 | 145% | 145% | 145% | 136% | 164% | 127% |
| Vitamin B3 (mg) | ≥12.6 mg/day | 23/35 | 106% | 103% | 111% | 103% | 136% | 120% |
| Vitamin B6 (mg) | ≥1.2 mg/day | 31/35 | 142% | 117% | 150% | 108% | 142% | 142% |
| Vitamin B9 (μg) | ≥200 µg/day | 25/35 | 122% | 116% | 134% | 110% | 103% | 128% |
| Vitamin B12 (μg) | ≥1.5 µg/day | 35/35 | 333% | 293% | 273% | 313% | 300% | 333% |
| Vitamin C (mg) | ≥40 mg/day | 33/35 | 253% | 238% | 290% | 250% | 293% | 348% |
| Vitamin D (μg) | ≥10 µg/day | 3/35 | 49% | 38% | 36% | 36% | 31% | 42% |
| Vitamin E (mg) | ≥3 mg/day | 35/35 | 247% | 257% | 243% | 223% | 357% | 247% |
| Calcium (mg) | ≥700 mg/day | 19/35 | 104% | 100% | 124% | 126% | 117% | 103% |
| Chloride (mg) | ≥2500 mg/day | 15/35 | 96% | 121% | 110% | 99% | 106% | 124% |
| Iodine (ug) | ≥140 µg/day | 16/35 | 131% | 106% | 110% | 98% | 99% | 133% |
| Iron (mg) | ≥8.7 mg/day | 20/35 | 102% | 108% | 114% | 105% | 191% | 118% |
| Magnesium (mg) | ≥270 mg/day | 21/35 | 110% | 106% | 120% | 104% | 114% | 113% |
| Phosphorous (mg) | ≥550 mg/day | 34/35 | 211% | 197% | 234% | 192% | 224% | 233% |
| Potassium (mg) | ≥3500 mg/day | 3/35 | 82% | 73% | 93% | 80% | 81% | 86% |
| Selenium (μg) | ≥60 µg/day | 7/35 | 93% | 86% | 76% | 73% | 89% | 97% |
| Sodium (mg) | <2.4 g/day | 30/35 | 61% | 74% | 76% | 60% | 70% | 80% |
| Zinc (mg) | ≥7 mg/day | 18/35 | 96% | 113% | 104% | 99% | 113% | 121% |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Grant, D.; Tomlinson, D.; Tsintzas, K.; Kolic, P.; Onambele-Pearson, G. Displacing Sedentary Behaviour with Light Intensity Physical Activity Spontaneously Alters Habitual Macronutrient Intake and Enhances Dietary Quality in Older Females. Nutrients 2020, 12, 2431. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12082431
Grant D, Tomlinson D, Tsintzas K, Kolic P, Onambele-Pearson G. Displacing Sedentary Behaviour with Light Intensity Physical Activity Spontaneously Alters Habitual Macronutrient Intake and Enhances Dietary Quality in Older Females. Nutrients. 2020; 12(8):2431. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12082431
Chicago/Turabian StyleGrant, Dale, David Tomlinson, Kostas Tsintzas, Petra Kolic, and Gladys Onambele-Pearson. 2020. "Displacing Sedentary Behaviour with Light Intensity Physical Activity Spontaneously Alters Habitual Macronutrient Intake and Enhances Dietary Quality in Older Females" Nutrients 12, no. 8: 2431. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12082431