
Cognitive Frailty in Thai Community-Dwelling Elderly: Prevalence and Its Association with Malnutrition


 , ,
, , 

Abstract
:1. Introduction
2. Materials and Methods
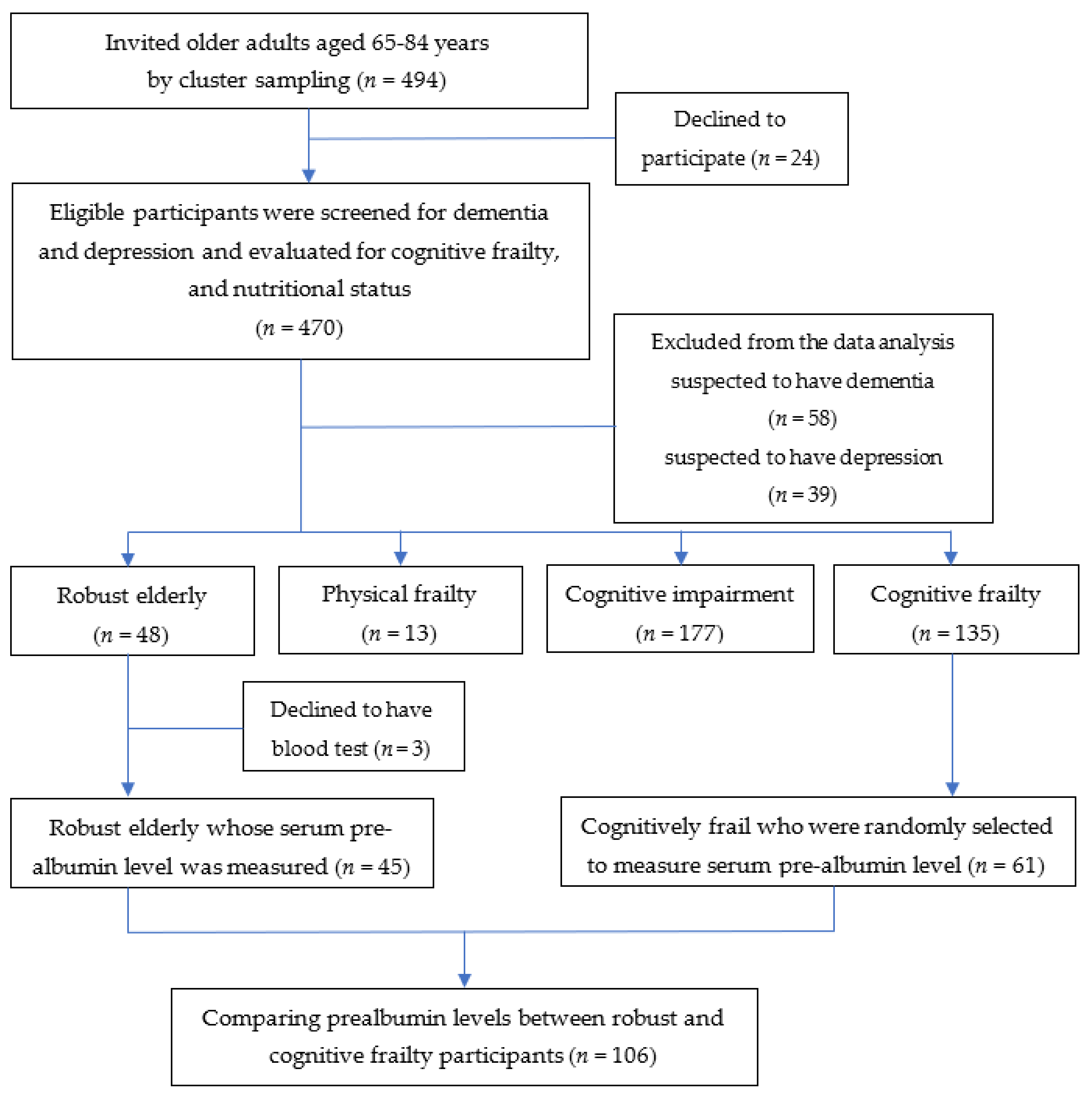
2.1. Study Design and Participants
2.2. Sample Size Calculation
2.3. Questionnaire
2.4. Cognitive Frailty Evaluation
2.5. Nutritional Status Evaluation
2.5.1. Mini Nutritional Assessment Short-Form (MNA-SF)
2.5.2. Serum Prealbumin Level
2.5.3. Triceps Skinfold Thickness
2.5.4. Calf Circumference
2.5.5. Body Mass Index (BMI)
2.6. Statistical Analysis
2.7. Ethical Considerations
3. Results
3.1. Socio-Demographic Information of Robust, Physical Frailty MCI, and Cognitive Frailty in the Elderly
3.2. Nutritional Status of Robust, Physical Frailty MCI, and Cognitive Frailty in the Elderly
3.3. Correlation Coefficient among Nutritional Status Measured by Different Methods
3.4. Association of Malnutrition and Cognitive Frailty
3.5. Factors Associated with Cognitive Frailty
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- United Nations, Department of Economic and Social Affairs, Population Division. World Population Ageing 2019: Highlights. Available online: https://www.un.org/en/development/desa/population/publications/pdf/ageing/WorldPopulationAgeing2019-Highlights.pdf (accessed on 2 October 2021).
- Department of Older Persons. Thailand Aging Population Statistics 2019. Available online: https://www.dop.go.th/th/know/side/1/1/275 (accessed on 2 October 2021).
- Larsson, L.; Degens, H.; Li, M.; Salviati, L.; Lee, Y.I.; Thompson, W.; Kirkland, J.L.; Sandri, M. Sarcopenia: Aging-Related Loss of Muscle Mass and Function. Physiol. Rev. 2019, 99, 427–511. [Google Scholar] [CrossRef] [PubMed]
- Morley, J.E. An Overview of Cognitive Impairment. Clin. Geriatr. Med. 2018, 34, 505–513. [Google Scholar] [CrossRef] [PubMed]
- Rosa, G.; Giannotti, C.; Martella, L.; Massa, F.; Serafini, G.; Pardini, M.; Nobili, F.M.; Monacelli, F. Brain Aging, Cardiovascular Diseases, Mixed Dementia, and Frailty in the Oldest Old: From Brain Phenotype to Clinical Expression. J. Alzheimer’s Dis. 2020, 75, 1083–1103. [Google Scholar] [CrossRef] [PubMed]
- Köhler, F.; Rodríguez-Paredes, M. DNA Methylation in Epidermal Differentiation, Aging, and Cancer. J. Investig. Dermatol. 2020, 140, 38–47. [Google Scholar] [CrossRef] [Green Version]
- Nugent, R.A.; Husain, M.J.; Kostova, D.; Chaloupka, F. Introducing the PLOS special collection of economic cases for NCD prevention and control: A global perspective. PLoS ONE 2020, 15, e0228564. [Google Scholar] [CrossRef]
- Amarya, S.; Singh, K.; Sabharwal, M. Changes during aging and their association with malnutrition. J. Clin. Gerontol. Geriatr. 2015, 6, 78–84. [Google Scholar] [CrossRef] [Green Version]
- Volkert, D. Malnutrition in Older Adults—Urgent Need for Action: A Plea for Improving the Nutritional Situation of Older Adults. Gerontology 2013, 59, 328–333. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Groot, L.; Broek, T.V.D.; van Staveren, W. Energy intake and micronutrient intake in elderly Europeans: Seeking the minimum requirement in the SENECA study. Age Ageing 1999, 28, 469–474. [Google Scholar] [CrossRef] [Green Version]
- Schiffman, S.S. Taste and smell losses in normal aging and disease. JAMA 1997, 278, 1357–1362. [Google Scholar] [CrossRef]
- Azzolino, D.; Passarelli, P.C.; De Angelis, P.; Piccirillo, G.B.; D’Addona, A.; Cesari, M. Poor Oral Health as a Determinant of Malnutrition and Sarcopenia. Nutrients 2019, 11, 2898. [Google Scholar] [CrossRef] [Green Version]
- Khan, A.; Carmona, R.; Traube, M. Dysphagia in the Elderly. Clin. Geriatr. Med. 2014, 30, 43–53. [Google Scholar] [CrossRef]
- Xu, F.; Laguna, L.; Sarkar, A. Aging-related changes in quantity and quality of saliva: Where do we stand in our understanding? J. Texture Stud. 2018, 50, 27–35. [Google Scholar] [CrossRef] [Green Version]
- Schiller, L.R. Maldigestion Versus Malabsorption in the Elderly. Curr. Gastroenterol. Rep. 2020, 22, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Buchman, A.S.; Bennett, D.A. Cognitive frailty. J. Nutr. Health Aging 2013, 17, 738–739. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Geda, Y.E. Mild Cognitive Impairment in Older Adults. Curr. Psychiatry Rep. 2012, 14, 320–327. [Google Scholar] [CrossRef] [PubMed]
- Pinto, T.C.C.; Machado, L.; Bulgacov, T.M.; Rodrigues-Júnior, A.L.; Costa, M.L.G.; Ximenes, R.C.C.; Sougey, E.B. Is the Montreal Cognitive Assessment (MoCA) screening superior to the Mini-Mental State Examination (MMSE) in the detection of mild cognitive impairment (MCI) and Alzheimer’s Disease (AD) in the elderly? Int. Psychogeriatr. 2018, 31, 491–504. [Google Scholar] [CrossRef]
- Fried, L.P.; Tangen, C.M.; Walston, J.; Newman, A.B.; Hirsch, C.; Gottdiener, J.; Seeman, T.; Tracy, R.; Kop, W.J.; Burke, G.; et al. Frailty in Older adults: Evidence for a phenotype. J. Gerontol. Ser. A 2001, 56, M146–M157. [Google Scholar] [CrossRef] [PubMed]
- Shimada, H.; Makizako, H.; Doi, T.; Yoshida, D.; Tsutsumimoto, K.; Anan, Y.; Uemura, K.; Ito, T.; Lee, S.; Park, H.; et al. Combined Prevalence of Frailty and Mild Cognitive Impairment in a Population of Elderly Japanese People. J. Am. Med Dir. Assoc. 2013, 14, 518–524. [Google Scholar] [CrossRef] [PubMed]
- Chye, L.; Wei, K.; Nyunt, M.S.Z.; Gao, Q.; Wee, S.L.; Ng, T.P. Strong Relationship between Malnutrition and Cognitive Frailty in the Singapore Longitudinal Ageing Studies (SLAS-1 and SLAS-2). J. Prev. Alzheimer’s Dis. 2018, 5, 142–148. [Google Scholar] [CrossRef]
- Roppolo, M.; Mulasso, A.; Rabaglietti, E. Cognitive frailty in Italian community-dwelling older adults: Prevalence rate and its association with disability. J. Nutr. Health Aging 2016, 21, 631–636. [Google Scholar] [CrossRef] [PubMed]
- Feng, L.; Nyunt, M.S.Z.; Gao, Q.; Feng, L.; Lee, T.S.; Tsoi, T.; Chong, M.S.; Lim, W.S.; Collinson, S.; Yap, P.; et al. Physical Frailty, Cognitive Impairment, and the Risk of Neurocognitive Disorder in the Singapore Longitudinal Ageing Studies. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2016, 72, 369–375. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Solfrizzi, V.; Scafato, E.; Seripa, D.; Lozupone, M.; Imbimbo, B.; D’Amato, A.; Tortelli, R.; Schilardi, A.; Galluzzo, L.; Gandin, C.; et al. Reversible Cognitive Frailty, Dementia, and All-Cause Mortality. The Italian Longitudinal Study on Aging. J. Am. Med. Dir. Assoc. 2017, 18, 89.e1–89.e8. [Google Scholar] [CrossRef]
- Kim, H.; Awata, S.; Watanabe, Y.; Kojima, N.; Osuka, Y.; Motokawa, K.; Sakuma, N.; Inagaki, H.; Edahiro, A.; Hosoi, E.; et al. Cognitive frailty in community-dwelling older Japanese people: Prevalence and its association with falls. Geriatr. Gerontol. Int. 2019, 19, 647–653. [Google Scholar] [CrossRef]
- Robertson, D.A.; Savva, G.; Kenny, R.A. Frailty and cognitive impairment—A review of the evidence and causal mechanisms. Ageing Res. Rev. 2013, 12, 840–851. [Google Scholar] [CrossRef] [PubMed]
- Panza, F.; Seripa, D.; Solfrizzi, V.; Tortelli, R.; Greco, A.; Pilotto, A.; Logroscino, G. Targeting Cognitive Frailty: Clinical and Neurobiological Roadmap for a Single Complex Phenotype. J. Alzheimer’s Dis. 2015, 47, 793–813. [Google Scholar] [CrossRef] [PubMed]
- Panza, F.; Solfrizzi, V.; Barulli, M.R.; Santamato, A.; Seripa, D.; Pilotto, A.; Logroscino, G. Cognitive Frailty: A Systematic Review of Epidemiological and Neurobiological Evidence of an Age-Related Clinical Condition. Rejuvenation Res. 2015, 18, 389–412. [Google Scholar] [CrossRef]
- Pourhassan, M.; Rommersbach, N.; Lueg, G.; Klimek, C.; Schnatmann, M.; Liermann, D.; Janssen, G.; Wirth, R. The Impact of Malnutrition on Acute Muscle Wasting in Frail Older Hospitalized Patients. Nutrients 2020, 12, 1387. [Google Scholar] [CrossRef] [PubMed]
- Nagano, A.; Wakabayashi, H.; Maeda, K.; Kokura, Y.; Miyazaki, S.; Mori, T.; Fujiwara, D. Respiratory Sarcopenia and Sarcopenic Respiratory Disability: Concepts, Diagnosis, and Treatment. J. Nutr. Health Aging 2021, 25, 507–515. [Google Scholar] [CrossRef] [PubMed]
- Ramsey, K.; Meskers, C.; Trappenburg, M.C.; Verlaan, S.; Reijnierse, E.M.; Whittaker, A.; Maier, A.B. Malnutrition is associated with dynamic physical performance. Aging Clin. Exp. Res. 2019, 32, 1085–1092. [Google Scholar] [CrossRef] [Green Version]
- LeSourd, B.M. Nutrition and immunity in the elderly: Modification of immune responses with nutritional treatments. Am. J. Clin. Nutr. 1997, 66, 478S–484S. [Google Scholar] [CrossRef]
- Agarwal, E.; Miller, M.; Yaxley, A.; Isenring, E. Malnutrition in the elderly: A narrative review. Maturitas 2013, 76, 296–302. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Badosa, E.L.; Tahull, M.B.; Casas, N.V.; Sangrador, G.E.; Méndez, C.F.; Meseguer, I.H.; González Àngels, I.; Urdiales, R.L.; Burguete, F.J.O.; Molas, M.T.; et al. Cribado de la desnutrición hospitalaria en la admisión: La desnutrición aumenta la mortalidad y la duración de la estancia hospitalaria. Nutr. Hosp. 2017, 34, 907–913. [Google Scholar] [CrossRef]
- Nawai, A.; Phongphangam, S.; Leveille, S. Sociodemographic and Health Related Factors Associated with Nutritional Status in thai Older Adults. Innov. Aging 2018, 2, 662–663. [Google Scholar] [CrossRef]
- Cederholm, T.; Bosaeus, I.; Barazzoni, R.; Bauer, J.; Van Gossum, A.; Klek, S.; Muscaritoli, M.; Nyulasi, I.; Ockenga, J.; Schneider, S.; et al. Diagnostic criteria for malnutrition—An ESPEN Consensus Statement. Clin. Nutr. 2015, 34, 335–340. [Google Scholar] [CrossRef]
- Lundin, H.; Sääf, M.; Strender, L.-E.; Mollasaraie, H.A.; Salminen, H. Mini nutritional assessment and 10-year mortality in free-living elderly women: A prospective cohort study with 10-year follow-up. Eur. J. Clin. Nutr. 2012, 66, 1050–1053. [Google Scholar] [CrossRef] [PubMed]
- Lorenzo-López, L.; Maseda, A.; De Labra, C.; Regueiro-Folgueira, L.; Rodríguez-Villamil, J.L.; Millán-Calenti, J.C. Nutritional determinants of frailty in older adults: A systematic review. BMC Geriatr. 2017, 17, 108. [Google Scholar] [CrossRef] [Green Version]
- Rubenstein, L.Z.; Harker, J.O.; Salvà, A.; Guigoz, Y.; Vellas, B. Screening for Undernutrition in Geriatric Practice: Developing the Short-Form Mini-Nutritional Assessment (MNA-SF). J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2001, 56, M366–M372. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kaiser, M.J.; Bauer, J.M.; Ramsch, C.; Uter, W.; Guigoz, Y.; Cederholm, T.; Thomas, D.R.; Anthony, P.; Charlton, K.E.; Maggio, M.; et al. Validation of the Mini Nutritional Assessment short-form (MNA-SF): A practical tool for identification of nutritional status. J. Nutr. Health Aging 2009, 13, 782–788. [Google Scholar] [CrossRef] [PubMed]
- Kawakami, R.; Miyachi, M.; Sawada, S.S.; Torii, S.; Midorikawa, T.; Tanisawa, K.; Ito, T.; Usui, C.; Ishii, K.; Suzuki, K.; et al. Cut-offs for calf circumference as a screening tool for low muscle mass: WASEDA’S Health Study. Geriatr. Gerontol. Int. 2020, 20, 943–950. [Google Scholar] [CrossRef]
- Keller, U. Nutritional Laboratory Markers in Malnutrition. J. Clin. Med. 2019, 8, 775. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sergi, G.; Coin, A.; Enzi, G.; Volpato, S.; Inelmen, E.M.; Buttarello, M.; Peloso, M.; Mulone, S.; Marin, S.; Bonometto, P. Role of visceral proteins in detecting malnutrition in the elderly. Eur. J. Clin. Nutr. 2005, 60, 203–209. [Google Scholar] [CrossRef] [Green Version]
- Ingenbleek, Y. Plasma Transthyretin as A Biomarker of Sarcopenia in Elderly Subjects. Nutrients 2019, 11, 895. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Del Brutto, O.H.; Mera, R.M.; Del Brutto, V.J.; Maestre, G.E.; Gardener, H.; Zambrano, M.; Wright, C.B. Influence of depression, anxiety and stress on cognitive performance in community-dwelling older adults living in rural Ecuador: Results of the Atahualpa Project. Geriatr. Gerontol. Int. 2014, 15, 508–514. [Google Scholar] [CrossRef]
- Wei, K.; Nyunt, M.S.Z.; Gao, Q.; Wee, S.-L.; Ng, T.-P. Frailty and Malnutrition: Related and Distinct Syndrome Prevalence and Association among Community-Dwelling Older Adults: Singapore Longitudinal Ageing Studies. J. Am. Med. Dir. Assoc. 2017, 18, 1019–1028. [Google Scholar] [CrossRef]
- Norazman, C.W.; Adznam, S.N.; Jamaluddin, R. Malnutrition as Key Predictor of Physical Frailty among Malaysian Older Adults. Nutrients 2020, 12, 1713. [Google Scholar] [CrossRef]
- Lang, L.; Clifford, A.; Wei, L.; Zhang, D.; Leung, D.; Augustine, G.; Danat, I.; Zhou, W.; Copeland, J.R.; Anstey, K.; et al. Prevalence and determinants of undetected dementia in the community: A systematic literature review and a meta-analysis. BMJ Open 2017, 7, e011146. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hong, X.; Yan, J.; Xu, L.; Shen, S.; Zeng, X.; Chen, L. Relationship between nutritional status and frailty in hospitalized older patients. Clin. Interv. Aging 2019, 14, 105–111. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tantirittisak, T. (Ed.) Clinical Practice Guidelines: Dementia; Institute of Neurology, Department of Medical Services, Thailand: Bangkok, Thailand, 2014. [Google Scholar]
- Boongird, P. Mental State Examination T10, Dementia Association of Thailand Newsletter. Available online: https://thaidementia.com/news/assets/files/DAT_news_letter_10.pdf (accessed on 2 October 2021).
- Wongpakaran, N.; Van Reekum, R. The Use of GDS-15 in Detecting MDD: A Comparison Between Residents in a Thai Long-Term Care Home and Geriatric Outpatients. J. Clin. Med. Res. 2013, 5, 101–111. [Google Scholar] [CrossRef] [Green Version]
- Yesavage, J.A.; Sheikh, J.I. 9/Geriatric Depression Scale (GDS) recent evidence and development of a shorter version. Clin. Gerontol. 1986, 5, 165–173. [Google Scholar] [CrossRef]
- Julayanont, P.; Tangwongchai, S.; Hemrungrojn, S.; Tunvirachaisakul, C.; Phanthumchinda, K.; Hongsawat, J.; Suwichanarakul, P.; Thanasirorat, S.; Nasreddine, Z.S. The Montreal Cognitive Assessment-Basic: A Screening Tool for Mild Cognitive Impairment in Illiterate and Low-Educated Elderly Adults. J. Am. Geriatr. Soc. 2015, 63, 2550–2554. [Google Scholar] [CrossRef] [PubMed]
- Rattanawiwatpong, P.; Khunphasee, A.; Pongurgsorn, C.; Intarakamhang, P. Validity and Reliability of the Thai Version of Short Format International Physical Activity Questionnaire (IPAQ). J. Thai Rehabil. 2006, 16, 147–160. [Google Scholar]
- Dellière, S.; Cynober, L. Is transthyretin a good marker of nutritional status? Clin. Nutr. 2017, 36, 364–370. [Google Scholar] [CrossRef] [PubMed]
- Addo, O.Y.; Himes, J.H. Reference curves for triceps and subscapular skinfold thicknesses in US children and adolescents. Am. J. Clin. Nutr. 2010, 91, 635–642. [Google Scholar] [CrossRef]
- Kawakami, R.; Murakami, H.; Sanada, K.; Tanaka, N.; Sawada, S.; Tabata, I.; Higuchi, M.; Miyachi, M. Calf circumference as a surrogate marker of muscle mass for diagnosing sarcopenia in Japanese men and women. Geriatr. Gerontol. Int. 2015, 15, 969–976. [Google Scholar] [CrossRef]
- International Obesity Task Force. Asia-Pacific Regional Obesity Guidelines; World Obesity Federation: London, UK, 1999. [Google Scholar]
- Brigola, A.G.; Alexandre, T.D.S.; Inouye, K.; Yassuda, M.S.; Pavarini, S.C.I.; Mioshi, E. Limited formal education is strongly associated with lower cognitive status, functional disability and frailty status in older adults. Dement. Neuropsychol. 2019, 13, 216–224. [Google Scholar] [CrossRef] [PubMed]
- Zahodne, L.B.; Stern, Y.; Manly, J.J. Differing effects of education on cognitive decline in diverse elders with low versus high educational attainment. Neuropsychology 2015, 29, 649–657. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kwan, R.; Leung, A.Y.; Yee, A.; Lau, L.T.; Xu, X.Y.; Dai, D.L.K. Cognitive Frailty and Its Association with Nutrition and Depression in Community-Dwelling Older People. J. Nutr. Health Aging 2019, 23, 943–948. [Google Scholar] [CrossRef] [PubMed]
- Hoogendijk, E.O.; van Hout, H.; Heymans, M.; van der Horst, H.E.; Frijters, D.H.; van Groenou, M.B.; Deeg, D.J.; Huisman, M. Explaining the association between educational level and frailty in older adults: Results from a 13-year longitudinal study in the Netherlands. Ann. Epidemiol. 2014, 24, 538–544.e2. [Google Scholar] [CrossRef]
- Fujiwara, Y.; Shinkai, S.; Kobayashi, E.; Minami, U.; Suzuki, H.; Yoshida, H.; Ishizaki, T.; Kumagai, S.; Watanabe, S.; Furuna, T.; et al. Engagement in paid work as a protective predictor of basic activities of daily living disability in Japanese urban and rural community-dwelling elderly residents: An 8-year prospective study. Geriatr. Gerontol. Int. 2015, 16, 126–134. [Google Scholar] [CrossRef]
- Shirooka, H.; Nishiguchi, S.; Fukutani, N.; Adachi, D.; Tashiro, Y.; Hotta, T.; Morino, S.; Nozaki, Y.; Hirata, H.; Yamaguchi, M.; et al. Association between comprehensive health literacy and frailty level in community-dwelling older adults: A cross-sectional study in Japan. Geriatr. Gerontol. Int. 2016, 17, 804–809. [Google Scholar] [CrossRef]
- Kim, J.W.; Lee, D.Y.; Lee, B.C.; Jung, M.H.; Kim, H.; Choi, Y.S.; Choi, I.-G. Alcohol and Cognition in the Elderly: A Review. Psychiatry Investig. 2012, 9, 8–16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Koch, M.; Fitzpatrick, A.L.; Rapp, S.R.; Nahin, R.L.; Williamson, J.D.; Lopez, O.L.; DeKosky, S.T.; Kuller, L.H.; Mackey, R.H.; Mukamal, K.J.; et al. Alcohol Consumption and Risk of Dementia and Cognitive Decline Among Older Adults with or Without Mild Cognitive Impairment. JAMA Netw. Open 2019, 2, e1910319. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kojima, G.; Liljas, A.; Iliffe, S.; Jivraj, S.; Walters, K. A systematic review and meta-analysis of prospective associations between alcohol consumption and incident frailty. Age Ageing 2018, 47, 26–34. [Google Scholar] [CrossRef] [Green Version]
- Seematter-Bagnoud, L.; Spagnoli, J.; Bula, C.; Santos-Eggimann, B. Alcohol Use and Frailty in Community-Dwelling Older Persons Aged 65 to 70 Years. J. Frailty Aging 2014, 3, 9–14. [Google Scholar] [CrossRef] [PubMed]
- Zuniga, K.; McAuley, E. Considerations in selection of diet assessment methods for examining the effect of nutrition on cognition. J. Nutr. Health Aging 2015, 19, 333–340. [Google Scholar] [CrossRef] [Green Version]
- Xu, L.; Zhang, J.; Shen, S.; Hong, X.; Zeng, X.; Yang, Y.; Liu, Z.; Chen, L.; Chen, X. Association Between Body Composition and Frailty in Elder Inpatients. Clin. Interv. Aging 2020, 15, 313–320. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, L.-Y.; Liu, L.-K.; Hwang, A.-C.; Lin, M.-H.; Peng, L.-N.; Lan, C.-F.; Chang, P.-L. Impact of malnutrition on physical, cognitive function and mortality among older men living in veteran homes by minimum data set: A prospective cohort study in Taiwan. J. Nutr. Health Aging 2016, 20, 41–47. [Google Scholar] [CrossRef] [PubMed]
- Cruz-Jentoft, A.J.; Bahat, G.; Bauer, J.; Boirie, Y.; Bruyère, O.; Cederholm, T.; Cooper, C.; Landi, F.; Rolland, Y.; Sayer, A.A.; et al. Sarcopenia: Revised European consensus on definition and diagnosis. Age Ageing 2019, 48, 16–31. [Google Scholar] [CrossRef] [Green Version]
- Davies, B.; Garcia-Garcia, F.J.; Ara, I.; Artalejo, F.R.; Rodríguez-Mañas, L.; Walter, S. Relationship Between Sarcopenia and Frailty in the Toledo Study of Healthy Aging: A Population Based Cross-Sectional Study. J. Am. Med. Dir. Assoc. 2018, 19, 282–286. [Google Scholar] [CrossRef]
- Hu, F.; Liu, H.; Liu, X.; Jia, S.; Zhao, W.; Zhou, L.; Zhao, Y.; Hou, L.; Xia, X.; Dong, B. Nutritional status mediates the relationship between sarcopenia and cognitive impairment: Findings from the WCHAT study. Aging Clin. Exp. Res. 2021, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Cheong, M.; Chew, S.; Oliver, J.; Baggs, G.; Low, Y.; How, C.; Tan, N.; Huynh, D.; Tey, S. Nutritional Biomarkers and Associated Factors in Community-Dwelling Older Adults: Findings from the SHIELD Study. Nutrients 2020, 12, 3329. [Google Scholar] [CrossRef]
- Hegendörfer, E.; VanAcker, V.; Vaes, B.; Degryse, J.-M. Malnutrition risk and its association with adverse outcomes in a Belgian cohort of community-dwelling adults aged 80 years and over. Acta Clin. Belg. 2021, 76, 351–358. [Google Scholar] [CrossRef] [PubMed]
- Bouillanne, O.; Morineau, G.; Dupont, C.; Coulombel, I.; Vincent, J.-P.; Nicolis, I.; Benazeth, S.; Cynober, L.; Aussel, C. Geriatric Nutritional Risk Index: A new index for evaluating at-risk elderly medical patients. Am. J. Clin. Nutr. 2005, 82, 777–783. [Google Scholar] [CrossRef] [Green Version]
- Perissinotto, E.; Pisent, C.; Sergi, G.; Grigoletto, F. Anthropometric measurements in the elderly: Age and gender differences. Br. J. Nutr. 2002, 87, 177–186. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baumgartner, R.N.; Rhyne, R.L.; Troup, C.; Wayne, S.; Garry, P.J. Appendicular Skeletal Muscle Areas Assessed by Magnetic Resonance Imaging in Older Persons. J. Gerontol. 1992, 47, M67–M72. [Google Scholar] [CrossRef] [PubMed]
- Sánchez-García, S.; García-Peña, C.; Duque-López, M.X.; Juárez-Cedillo, T.; Cortés-Núñez, A.R.; Reyes-Beaman, S. Anthropometric measures and nutritional status in a healthy elderly population. BMC Public Health 2007, 7, 2. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, C.-Y.; Tseng, W.-C.; Yang, Y.-H.; Chen, C.-L.; Lin, L.-L.; Chen, F.-P.; Wong, A.M. Calf Circumference as an Optimal Choice of Four Screening Tools for Sarcopenia Among Ethnic Chinese Older Adults in Assisted Living. Clin. Interv. Aging 2020, 15, 2415–2422. [Google Scholar] [CrossRef]
- Pagotto, V.; Dos Santos, K.F.; Malaquias, S.G.; Bachion, M.M.; Silveira, E.A. Calf circumference: Clinical validation for evaluation of muscle mass in the elderly. Rev. Bras. Enferm. 2018, 71, 322–328. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rivan, N.F.M.; Shahar, S.; Rajab, N.F.; Singh, D.K.A.; Din, N.C.; Mahadzir, H.; Hamid, T. Cognitive frailty among Malaysian older adults: Baseline findings from the LRGS TUA cohort study. Clin. Interv. Aging 2019, 14, 1343–1352. [Google Scholar] [CrossRef] [Green Version]
- Sukkriang, N.; Somrak, K. Correlation Between Mini Nutritional Assessment and Anthropometric Measurements Among Community-Dwelling Elderly Individuals in Rural Southern Thailand. J. Multidiscip. Health 2021, 14, 1509–1520. [Google Scholar] [CrossRef]
- Woldekidan, M.A.; Haile, D.; Shikur, B.; Gebreyesus, S.H. Validity of Mini Nutritional Assessment tool among an elderly population in Yeka sub-city, Addis Ababa, Ethiopia. South Afr. J. Clin. Nutr. 2021, 34, 103–109. [Google Scholar] [CrossRef] [Green Version]
- Bonnefoy, M.; Jauffret, M.; Kostka, T.; Jusot, J. Usefulness of Calf Circumference Measurement in Assessing the Nutritional State of Hospitalized Elderly People. Gerontology 2002, 48, 162–169. [Google Scholar] [CrossRef] [PubMed]
- Syed, Q.; Hendler, K.T.; Koncilja, K. The Impact of Aging and Medical Status on Dysgeusia. Am. J. Med. 2016, 129, 753.e1–753.e6. [Google Scholar] [CrossRef] [Green Version]
- Tuccori, M.; Lapi, F.; Testi, A.; Ruggiero, E.; Moretti, U.; Vannacci, A.; Bonaiuti, R.; Antonioli, L.; Fornai, M.; Giustarini, G.; et al. Drug-Induced Taste and Smell Alterations. Drug Saf. 2011, 34, 849–859. [Google Scholar] [CrossRef] [PubMed]
- Kose, E.; Wakabayashi, H.; Yasuno, N. Polypharmacy and Malnutrition Management of Elderly Perioperative Patients with Cancer: A Systematic Review. Nutrients 2021, 13, 1961. [Google Scholar] [CrossRef]


{kind=link}
| Characteristics (Mean ± SD)/n (%)) | Total (n = 373) | Robust a (n = 48) | Physical Frailty b (n = 13) | MCI c (n = 177) | Cognitive Frailty d (n = 135) | p-Value |
|---|---|---|---|---|---|---|
| Age (years), mean ± SD | 70.45 ± 5.40 | 68.17 ± 3.06 | 69.08 ± 3.64 | 70.15 ± 4.84 | 71.78 ± 6.47 | <0.001 *,ac,ad,bd,cd |
| Gender Male Female | 155 (41.6) 218 (58.4) | 26 (54.2) 22 (45.8) | 3 (23.1) 10 (76.9) | 73 (41.2) 104 (58.8) | 53 (39.3) 82 (60.7) | 0.15 |
| Marital status Married Single/divorced/ Widowed | 238 (63.8) 135 (36.2) | 37 (77.1) 11 (22.9) | 9 (69.2) 4 (30.8) | 108 61.0) 69 (39.0) | 84 (62.2) 51 (37.8) | 0.20 |
| Living alone | 42 (11.3) | 5 (10.4) | 2 (15.4) | 23 (13.0) | 12 (8.9) | 0.67 |
| Educational level No education Grade 1–3 Grade 4–6 High school/Vocational certificate Bachelor’s degree | 8 (2.1) 138 (37.0) 188 (50.4) 24 (6.4) 15 (4.0) | 1 (2.1) 9 (18.8) 18 (37.5) 12 (25.0) 8 (16.7) | 1 (7.7) 6 (46.2) 4 (30.8) 1 (7.7) 1 (7.7) | 4 (2.3) 60 (33.9) 99 (55.9) 9 (5.1) 5 (2.8) | 2 (1.5) 63 (46.7) 67 (49.6) 2 (1.5) 1 (0.7) | <0.001 ** |
| Numbers of underlying diseases | ||||||
| 0 1–2 ≥3 | 107 (28.7) 228 (61.1) 28 (10.2) | 14 (29.2) 28 (58.3) 6 (12.5) | 4 (30.8) 9 (69.2) - | 57 (32.2) 105 (59.3) 15 (8.5) | 32 (23.7) 86 (63.7) 17 (12.6) | 0.512 |
| Underlying diseases, n (%) | ||||||
| No underlying disease Hypertension Type 2 Diabetes mellitus Dyslipidemia Gout Thyroid diseases Coronary heart disease Stroke Chronic kidney disease Osteoarthritis | 103 (27.6) 195 (52.3) 58 (15.6) 59 (15.8) 16 (4.3) 12 (3.2) 12 (3.2) 11 (3.0) 10 (2.7) 8 (2.1) | 14 (29.2) 20 (41.7) 7 (14.6) 10 (20.8) 3 (6.3) 1 (2.1) 1 (2.1) 2 (4.2) - 1 (2.1) | 4 (30.8) 7 (53.9) 2 (15.4) - - - - - - 1 (7.7) | 55 (31.1) 92 (52.0) 21 (11.9) 29 (16.4) 7 (4.0) 7 (4.0) 4 (2.3) 6 (3.4) 5 (2.8) 2 (1.1) | 30 (22.2) 76 (56.3) 28 (20.7) 20 (14.8) 6 (4.4) 4 (3.0) 7 (5.2) 3 (2.2) 5 (3.7) 4 (3.0) | 0.37 0.383 0.201 0.322 0.780 0.809 0.418 0.798 0.525 0.361 |
| Alcohol drinking in previous year | ||||||
| Risky alcohol drinking (>10 standard drinks per week) Non-risky alcohol drinking (≤10 standard drinks per week) No alcohol drinking | 38 (10.2) 20 (5.4) 315 (85.4) | 9 (18.75) 3 (6.25) 36 (75.0) | 1 (7.7) 2 (15.4) 10 (76.9) | 21 (11.9) 12 (6.8) 144 (81.3) | 7 (5.2) 3 (2.2) 125 (92.6) | 0.011 * |
| Current smoking | 25 (6.7) | 3 (6.3) | 0 (0) | 14 (7.9) | 8 (5.9) | 0.68 |
| ADL score, mean ± SD | 19.63 ± 0.83 | 19.83 ± 0.48 | 19.58 ± 0.79 | 19.66 ± 0.80 | 19.53 ± 0.94 | 0.17 |
| Nutritional Status | Total (n = 373) | Robust a (n = 48) | Physical Frailty b (n = 13) | MCI c (n = 177) | Cognitive Frailty d (n = 135) | p-Value |
|---|---|---|---|---|---|---|
| MNA-SF, n (%) At risk of malnutrition Malnourished | 221 (59.2) 31 (8.3) | 30 (62.5) 2 (4.2) | 6 (46.2) 3 (23.1) | 106 (59.9) 8 (4.5) | 79 (58.5) 18 (13.3) | 0.04 * |
| MNA-SF score, mean ± SD | 10.41 ± 1.84 | 10.79 ± 1.51 | 9.69 + 2.18 | 10.68 + 1.62 | 10.02 + 2.10 | <0.01 *,ab,ad,bc,cd |
| Triceps skinfold thickness (cm), mean ± SD | 18.17 ± 8.79 | 19.41 ± 8.14 | 22.86 ± 15.97 | 17.25 ± 7.17 | 18.49 + 9.84 | 0.08 |
| Low calf circumference, n (%) | 194 (52) | 17 (35.4) | 6 (46.2) | 96 (54.2) | 75 (55.6) | 0.09 |
| Calf circumference (cm), mean ± SD | 33.09 ± 4.55 | 34.20 ± 2.95 | 33.47 ± 3.55 | 33.32 ± 5.53 | 32.36 ± 3.48 | 0.08 |
| Underweight by BMI, n (%) | 42 (11.3) | 3 (6.3) | 1 (7.7) | 20 (11.3) | 18 (13.3) | 0.58 |
| Nutritional Status | Total (n = 106) | Robust (n = 45) | Cognitive Frailty (n = 61) | p-Value |
|---|---|---|---|---|
| Low-prealbumin level, n (%) | 95 (89.6) | 39 (86.7) | 56 (91.8) | 0.162 |
| Prealbumin levels (mg/L), median (IQR) | 85.69 (92.90) | 85.8 (89.70) | 85.62 (92.84) | 0.501 |
| Pearson’s Correlation Coefficient | Nutritional Status Evaluation | ||
|---|---|---|---|
| Prealbumin Levels | Triceps Skinfold Thickness | Calf Circumference | |
| MNA-SF | −0.005 | 0.262 ** | 0.304 ** |
| Prealbumin levels | - | 0.036 | 0.045 |
| Triceps skinfold thickness | - | - | 0.212 ** |
| Measurement Methods | Model 1 | p-Value | Model 2 | p-Value | ||
|---|---|---|---|---|---|---|
| Crude OR | 95% CI | Adjusted OR | 95% CI | |||
| MNA-SF category | ||||||
| At risk of malnutrition | 1.23 | 0.76–2.00 | 0.391 | 1.28 | 0.77–2.11 | 0.343 |
| Malnourished | 3.24 | 1.41–7.42 | <0.01 ** | 2.81 | 1.18–6.67 | 0.019 * |
| MNA-SF score | 0.84 | 0.74–0.94 | <0.01 ** | 0.84 | 0.75–0.96 | <0.01 ** |
| Prealbumin levels | 1.00 | 0.99–1.00 | 0.240 | 1.00 | 0.99–1.00 | 0.222 |
| Triceps skinfold thickness | 1.01 | 0.98–1.03 | 0.600 | 1.01 | 0.98–1.04 | 0.268 |
| Calf circumference | 0.92 | 0.86–0.98 * | 0.010 * | 0.93 | 0.86–1.01 | 0.090 |
| Underweight by BMI | 1.37 | 0.71–2.63 | 0.340 | 1.47 | 0.69–3.13 | 0.320 |
| Variables | Adjusted OR | 95% CI | p-Value |
|---|---|---|---|
| Age | 1.06 | 1.02–1.11 | <0.01 ** |
| Female | 0.88 | 0.52–1.47 | 0.358 |
| Educational level above high school | 6.77 | 1.99–23.01 | <0.01 ** |
| Married | 1.12 | 0.65–1.95 | 0.680 |
| Living alone | 0.60 | 0.26–1.37 | 0.228 |
| Number of underlying diseases | 1.17 | 0.94–1.46 | 0.172 |
| Alcohol drinking in previous year (Total of standard drinks per week) | 1.00 | 0.99–1.00 | 0.051 |
| Smoking status | 0.83 | 0.31–2.24 | 0.712 |
| ADL score | 0.78 | 0.59–1.02 | 0.070 |
| MNA-SF | |||
| At risk of malnutrition | 1.28 | 0.77–2.11 | 0.343 |
| Malnourished | 2.81 | 1.18–6.67 | 0.019 * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Seesen, M.; Sirikul, W.; Ruangsuriya, J.; Griffiths, J.; Siviroj, P. Cognitive Frailty in Thai Community-Dwelling Elderly: Prevalence and Its Association with Malnutrition. Nutrients 2021, 13, 4239. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13124239
Seesen M, Sirikul W, Ruangsuriya J, Griffiths J, Siviroj P. Cognitive Frailty in Thai Community-Dwelling Elderly: Prevalence and Its Association with Malnutrition. Nutrients. 2021; 13(12):4239. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13124239
Chicago/Turabian StyleSeesen, Mathuramat, Wachiranun Sirikul, Jetsada Ruangsuriya, Jiranan Griffiths, and Penprapa Siviroj. 2021. "Cognitive Frailty in Thai Community-Dwelling Elderly: Prevalence and Its Association with Malnutrition" Nutrients 13, no. 12: 4239. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13124239