
Associated Factors of Sarcopenia in Community-Dwelling Older Adults: A Systematic Review and Meta-Analysis


Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Eligibility Criteria
2.3. Study Selection
2.4. Data Extraction
2.5. Quality Assessment
2.6. Statistical Analysis
3. Results
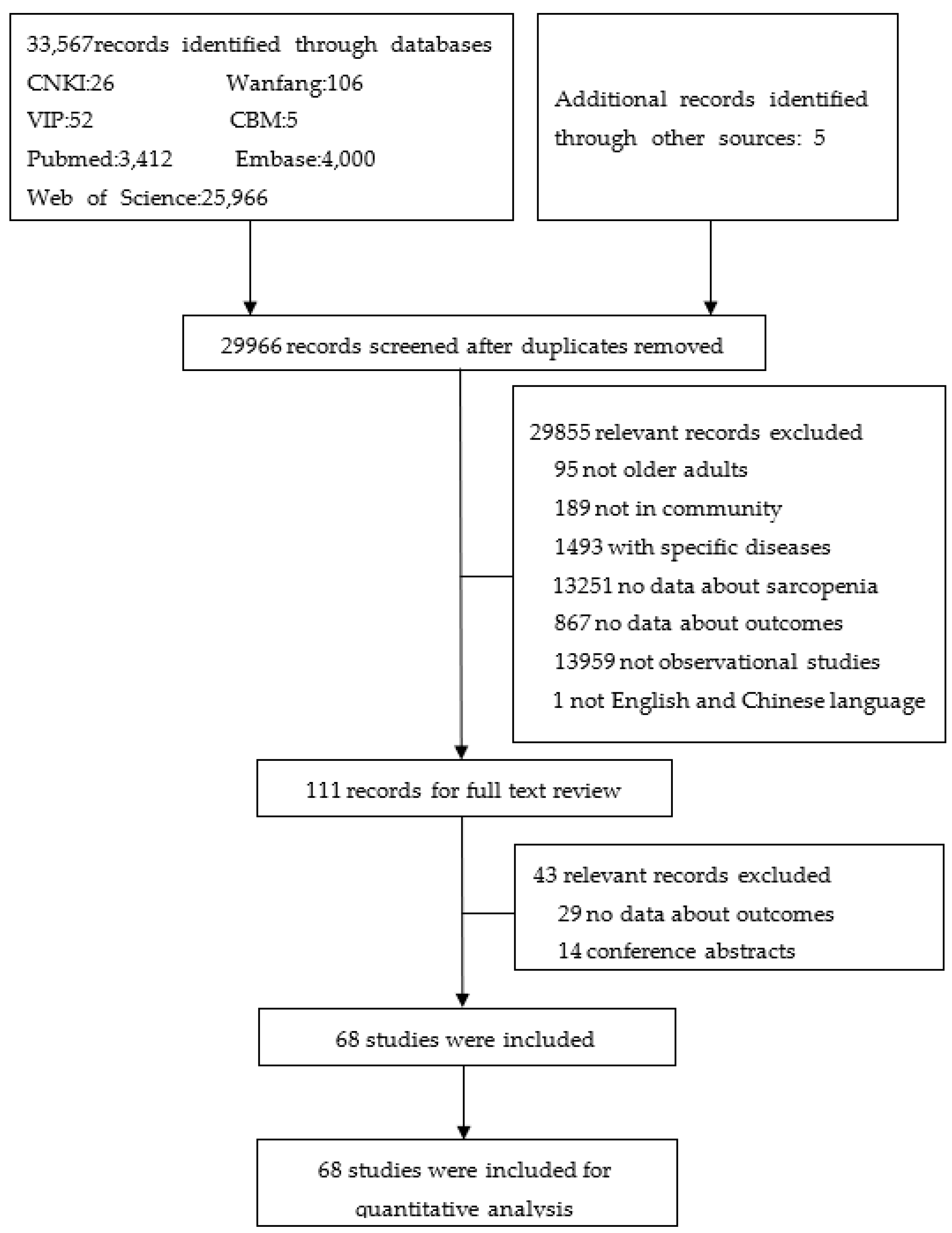
3.1. Search Results
3.2. Characteristics of Included Studies and Participants
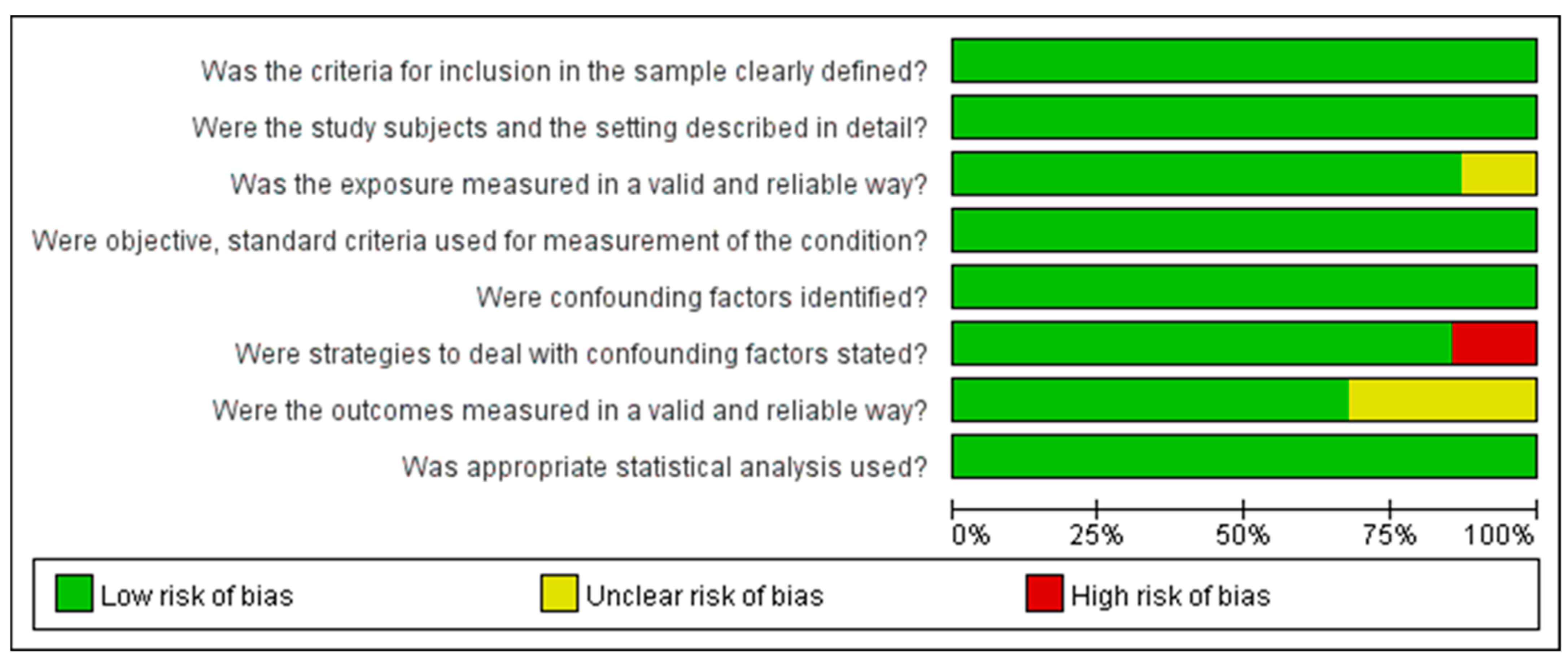
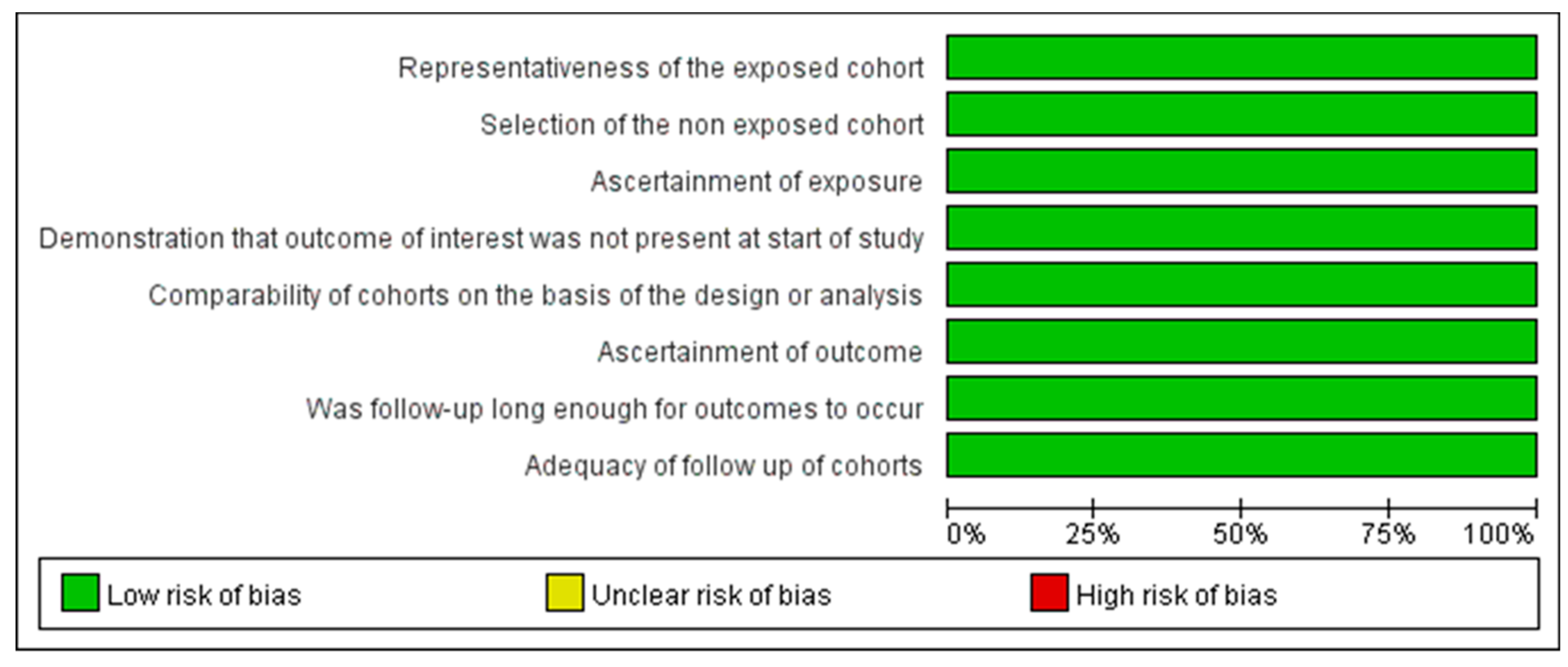
3.3. Quality Assessment of the Included Studies
3.4. Associated Factors of Sarcopenia in Community-Dwelling Older Adults
3.4.1. Sociodemographic Factors
3.4.2. Behavioral Factors
3.4.3. Disease-Related Factors
3.5. Subgroup Analysis
3.6. Publication Bias
4. Discussion
4.1. Sociodemographic Associated Factors of Sarcopenia in Community-Dwelling Older Adults
4.2. Behavioral-Associated Factors of Sarcopenia in Community-Dwelling Older Adults
4.3. Disease-Related Associated Factors of Sarcopenia in Community-Dwelling Older Adults
4.4. Implications of the Review for Future Clinical Practice
4.5. Strengths and Limitations of The Review
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- United Nations Department of Economic and Social Affairs (DESA)/Population Division. World Population Prospects 2019. Available online: https://population.un.org/wpp/Download/Standard/Population/ (accessed on 26 January 2019).
- Malafarina, V.; Uriz-Otano, F.; Iniesta, R.; Gil-Guerrero, L. Sarcopenia in the elderly: Diagnosis, physiopathology and treatment. Maturitas 2012, 71, 109–114. [Google Scholar] [CrossRef] [PubMed]
- Cruz-Jentoft, A.J.; Baeyens, J.P.; Bauer, J.M.; Boirie, Y.; Cederholm, T.; Landi, F.; Martin, F.C.; Michel, J.-P.; Rolland, Y.; Schneider, S.; et al. Sarcopenia: European consensus on definition and diagnosis: Report of the European Working Group on Sarcopenia in Older People. Age Ageing 2010, 39, 412–423. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cruz-Jentoft, A.J.; Bahat, G.; Bauer, J.; Boirie, Y.; Bruyère, O.; Cederholm, T.; Cooper, C.; Landi, F.; Rolland, Y.; Sayer, A. Sarcopenia: Revised European consensus on definition and diagnosis. Age Ageing 2019, 48, 16–31. [Google Scholar] [CrossRef] [Green Version]
- Fielding, R.A.; Vellas, B.; Evans, W.J.; Bhasin, S.; Morley, J.E.; Newman, A.B.; van Kan, G.A.; Andrieu, S.; Bauer, J.; Breuille, D.; et al. Sarcopenia: An Undiagnosed Condition in Older Adults. Current Consensus Definition: Prevalence, Etiology, and Consequences. International Working Group on Sarcopenia. J. Am. Med Dir. Assoc. 2011, 12, 249–256. [Google Scholar] [CrossRef] [Green Version]
- McLean, R.R.; Shardell, M.D.; Alley, D.E.; Cawthon, P.M.; Fragala, M.S.; Harris, T.B.; Kenny, A.M.; Peters, K.W.; Ferrucci, L.; Guralnik, J.M.; et al. Criteria for clinically relevant weakness and low lean mass and their lon-gi-tudinal association with incident mobility impairment and mortality: The foundation for the National Institutes of Health (FNIH) sarcopenia project. J. Gerontol. Biol. Sci. Med. Sci. 2014, 69, 576–583. [Google Scholar] [CrossRef]
- Chen, L.-K.; Liu, L.-K.; Woo, J.; Assantachai, P.; Auyeung, T.-W.; Bahyah, K.S.; Chou, M.-Y.; Hsu, P.-S.; Krairit, O.; Lee, J.S.; et al. Sarcopenia in Asia: Consensus Report of the Asian Working Group for Sarcopenia. J. Am. Med Dir. Assoc. 2014, 15, 95–101. [Google Scholar] [CrossRef] [PubMed]
- Ida, S.; Kaneko, R.; Murata, K. SARC-F for screening of sarcopenia among older adults: A meta-analysis of screening test accuracy. J. Am. Med. Dir. Assoc. 2018, 19, 685–689. [Google Scholar] [CrossRef]
- Mayhew, A.J.; Amog, K.; Phillips, S.; Parise, G.; McNicholas, P.D.; de Souza, R.J.; Thabane, L.; Raina, P. The prevalence of sarcopenia in community-dwelling older adults, an exploration of differences between studies and within definitions: A systematic review and meta-analyses. Age Ageing 2019, 48, 48–56. [Google Scholar] [CrossRef] [Green Version]
- Beaudart, C.; Zaaria, M.; Pasleau, F.; Reginster, J.Y.; Bruyère, O. Health outcomes of sarcopenia: A systematic review and meta-analysis. PLoS ONE 2017, 12, e0169548. [Google Scholar]
- Janssen, I.; Heymsfield, S.B.; Ross, R. Low relative skeletal muscle mass (sarcopenia) in older persons is associated with functional impairment and physical disability. J. Am. Geriatr. Soc. 2002, 50, 889–896. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Janssen, I.; Shepard, D.S.; Katzmarzyk, P.T.; Roubenoff, R. The healthcare costs of sarcopenia in the United States. J. Am. Geriatr. Soc. 2004, 52, 80–85. [Google Scholar] [CrossRef] [PubMed]
- Xia, L.; Zhao, R.; Wan, Q.; Wu, Y.; Zhou, Y.; Wang, Y.; Cui, Y.; Shen, X.; Wu, X. Sarcopenia and adverse health-related outcomes: An umbrella review of meta-analyses of observational studies. Cancer Med. 2020, 9, 7964–7978. [Google Scholar] [CrossRef]
- Zhao, W.T.; Yang, M.; Wu, H.M.; Yang, L.; Zhang, X.M.; Huang, Y. Systematic review and meta-analysis of the association between Sarcopenia and Dysphagia. J. Nutr. Health Aging 2018, 22, 1003–1009. [Google Scholar] [CrossRef] [PubMed]
- Peng, T.C.; Chen, W.L.; Wu, L.W.; Chang, Y.W.; Kao, T.W. Sarcopenia and cognitive impairment: A systematic review and meta-analysis. Clin. Nutr. 2020, 39, 2695–2701. [Google Scholar] [CrossRef]
- Bai, T.; Fang, F.; Li, F.; Ren, Y.; Hu, J.; Cao, J. Sarcopenia is associated with hypertension in older adults: A systematic review and meta-analysis. BMC Geriatr. 2020, 20, 279. [Google Scholar] [CrossRef]
- Veronese, N.; Pizzol, D.; Demurtas, J.; Soysal, P.; Smith, L.; Sieber, C.; Timo, S.; Bourdel-Marchasson, I.; Sinclair, A.; Petrovic, M.; et al. Association between sarcopenia and diabetes: A systematic review and me-ta-analysis of observational studies. Eur. Geriatr. Med. 2019, 10, 685–696. [Google Scholar] [CrossRef] [PubMed]
- Nielsen, B.R.; Abdulla, J.; Andersen, H.E.; Schwarz, P.; Suetta, C. Sarcopenia and osteoporosis in older people: A systematic review and meta-analysis. Eur. Geriatr. Med. 2018, 9, 419–434. [Google Scholar] [CrossRef]
- Wijarnpreecha, K.; Panjawatanan, P.; Thongprayoon, C.; Jaruvongvanich, V.; Ungprasert, P. Sarcopenia and risk of nonalcoholic fatty liver disease: A meta-analysis. Saudi. J. Gastroenterol. 2018, 24, 12–17. [Google Scholar] [CrossRef] [PubMed]
- Chang, K.V.; Hsu, T.H.; Wu, W.T.; Huang, K.C.; Han, D.S. Is sarcopenia associated with depression? A systematic review and meta-analysis of observational studies. Age Ageing 2017, 46, 738–746. [Google Scholar] [CrossRef] [Green Version]
- Marzetti, E.; on behalf of the SPRINTT Consortium; Calvani, R.; Tosato, M.; Cesari, M.; Di Bari, M.; Cherubini, A.; Collamati, A.; D’Angelo, E.; Pahor, M.; et al. Sarcopenia: An overview. Aging Clin. Exp. Res. 2017, 29, 11–17. [Google Scholar] [CrossRef]
- Yang, L.; Yao, X.; Shen, J.; Sun, G.; Sun, Q.; Tian, X.; Li, X.; Li, X.; Ye, L.; Zhang, Z.; et al. Comparison of revised EWGSOP criteria and four other diagnostic criteria of sarcopenia in Chinese community-dwelling elderly residents. Exp. Gerontol. 2019, 130, 110798. [Google Scholar] [CrossRef]
- Su, Y.; Hirayama, K.; Han, T.F.; Izutsu, M.; Yuki, M. Sarcopenia prevalence and risk factors among Japanese community dwelling older adults living in a snow-covered city according to EWGSOP2. J. Clin. Med. 2019, 8, 291. [Google Scholar] [CrossRef] [Green Version]
- Neves, T.; Ferriolli, E.; Lopes, M.; Souza, M.; Fett, C.A.; Fett, W. Prevalence and factors associated with sarcopenia and dynapenia in elderly people. J Frailty Sarcopenia Falls 2018, 3, 194–202. [Google Scholar] [CrossRef] [PubMed]
- Bae, E.J.; Kim, Y.H. Factors affecting sarcopenia in Korean adults by age groups. Osong Public Health Res Perspect. 2017, 8, 169–178. [Google Scholar] [CrossRef]
- Tyrovolas, S.; Koyanagi, A.; Olaya, B.; Ayuso-Mateos, J.L.; Miret, M.; Chatterji, S.; Tobiasz-Adamczyk, B.; Koskinen, S.; Leonardi, M.; Haro, J.M. Factors associated with skeletal muscle mass, sarcopenia, and sarcopenic obesity in older adults: A multi-continent study. J. Cachexia Sarcopenia Muscle 2016, 7, 312–321. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; Moher, D.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; E Brennan, S.; et al. PRISMA 2020 explanation and elaboration: Updated guidance and exemplars for reporting systematic reviews. BMJ 2021, 372, n160. [Google Scholar] [CrossRef] [PubMed]
- Joanna Briggs Institute Critical Appraisal Tools. Available online: http://joannabriggs.org/research/criticalappraisal-tools.html (accessed on 21 August 2021).
- Wells, G.A.; Shea, B.; O’Connell, D.; Peterson, J.; Welch, V.; Losos, M.; Tugwell, P. The Newcastle-Ottawa Scale for Assessing the Quality of Nonrandomised Studies in Meta-Analyses. 2014. Available online: http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp (accessed on 12 June 2021).
- Han, P.; Yu, H.; Ma, Y.; Kang, L.; Fu, L.; Jia, L.; Chen, X.; Yu, X.; Hou, L.; Wang, L.; et al. The increased risk of sarcopenia in patients with cardiovascular risk factors in Suburb-Dwelling older Chinese using the AWGS definition. Sci. Rep. 2017, 7, 9592. [Google Scholar] [CrossRef]
- de Amorim, J.S.C.; da Silva, S.L.A.; Ude Viana, J.; Trelha, C.S. Factors associated with the prevalence of sarcopenia and frailty syndrome in elderly university workers. Arch. Gerontol. Geriatr. 2019, 82, 172–178. [Google Scholar] [CrossRef]
- Santos, V.; Christofaro, D.; Gomes, I.C.; Agostinete, R.R.; Freitas, I.F.; Gobbo, L.A. Factors associated with sarcopenia in subjects aged 80 years and over. Rev. Nutr. 2015, 28, 319–326. [Google Scholar] [CrossRef] [Green Version]
- Gao, L.; Jiang, J.; Yang, M.; Hao, Q.; Luo, L.; Dong, B. Prevalence of sarcopenia and associated factors in Chinese community-dwelling elderly: Comparison between rural and urban areas. J. Am. Med. Dir. Assoc. 2015, 16, 1003.e1–1003.e6. [Google Scholar] [CrossRef]
- Hai, S.; Wang, H.; Cao, L.; Liu, P.; Zhou, J.; Yang, Y.; Dong, B. Association between sarcopenia with lifestyle and family function among community-dwelling Chinese aged 60 years and older. BMC Geriatr. 2017, 17, 187. [Google Scholar] [CrossRef] [PubMed]
- Lim, H.S.; Park, Y.H.; Suh, K.; Yoo, M.H.; Park, H.K.; Kim, H.J.; Lee, J.H.; Byun, D.W. Association between sarcopenia, sarcopenic obesity, and chronic disease in Korean elderly. J. Bone Metab. 2018, 25, 187–193. [Google Scholar] [CrossRef] [PubMed]
- Xu, W.; Chen, T.; Cai, Y.; Hu, Y.; Fan, L.; Wu, C. Sarcopenia in community-dwelling oldest old is associated with disability and poor physical function. J. Nutr. Health Aging 2020, 24, 339–345. [Google Scholar] [CrossRef]
- Meng, N.H.; Li, C.I.; Liu, C.S.; Lin, C.H.; Lin, W.Y.; Chang, C.K.; Li, T.C.; Lin, C.C. Comparison of height- and weight-adjusted sarcopenia in a Taiwanese metropolitan older population. Geriatr. Gerontol. Int. 2015, 15, 45–53. [Google Scholar] [CrossRef] [PubMed]
- Ishii, S.; Tanaka, T.; Shibasaki, K.; Ouchi, Y.; Kikutani, T.; Higashiguchi, T.; Obuchi, S.P.; Ishikawa-Takata, K.; Hirano, H.; Kawai, H.; et al. Development of a simple screening test for sarcopenia in older adults. Geriatr. Gerontol. Int. 2014, 14, 93–101. [Google Scholar] [CrossRef]
- Tseng, T.G.; Lu, C.K.; Hsiao, Y.H.; Pan, S.C.; Tai, C.J.; Lee, M.C. Development of Taiwan risk score for sarcopenia (TRSS) for sarcopenia screening among community-dwelling older adults. Int. J. Environ. Res. Public Health 2020, 17, 2859. [Google Scholar] [CrossRef] [Green Version]
- Kuo, Y.H.; Wang, T.F.; Liu, L.K.; Lee, W.J.; Peng, L.N.; Chen, L.K. Epidemiology of sarcopenia and factors associated with it among community-dwelling older adults in Taiwan. Am. J. Med. Sci. 2019, 357, 124–133. [Google Scholar] [CrossRef]
- Akune, T.; Muraki, S.; Oka, H.; Tanaka, S.; Kawaguchi, H.; Nakamura, K.; Yoshimura, N. Exercise habits during middle age are associated with lower prevalence of sarcopenia: The ROAD study. Osteoporos Int. 2014, 25, 1081–1088. [Google Scholar] [CrossRef]
- Sousa-Santos, A.R.; Afonso, C.; Borges, N.; Santos, A.; Padrão, P.; Moreira, P.; Amaral, T.F. Factors associated with sarcopenia and undernutrition in older adults. Nutr. Diet. 2019, 76, 604–612. [Google Scholar] [CrossRef]
- Samper-Ternent, R.; Reyes-Ortiz, C.; Ottenbacher, K.J.; Cano, C.A. Frailty and sarcopenia in Bogotá: Results from the SABE Bogotá Study. Aging Clin. Exp. Res. 2017, 29, 265–272. [Google Scholar] [CrossRef]
- Kim, H.; Suzuki, T.; Kim, M.; Kojima, N.; Yoshida, Y.; Hirano, H.; Saito, K.; Iwasa, H.; Shimada, H.; Hosoi, E.; et al. Incidence and Predictors of Sarcopenia Onset in Community-Dwelling Elderly Japanese Women: 4-Year Follow-Up Study. J. Am. Med Dir. Assoc. 2014, 16, 85.e1–85.e8. [Google Scholar] [CrossRef] [PubMed]
- Yu, R.; Wong, M.; Leung, J.; Lee, J.; Auyeung, T.W.; Woo, J. Incidence, reversibility, risk factors and the protective effect of high body mass index against sarcopenia in community-dwelling older Chinese adults. Geriatr. Gerontol. Int. 2014, 14, 15–28. [Google Scholar] [CrossRef] [PubMed]
- Han, P.; Zhao, J.; Guo, Q.; Wang, J.; Zhang, W.; Shen, S.; Wang, X.; Dong, R.; Ma, Y.; Kang, L.; et al. Incidence, risk factors, and the protective effect of high body mass index against sarcopenia in suburb-dwelling elderly Chinese populations. J. Nutr. Heal. Aging 2016, 20, 1056–1060. [Google Scholar] [CrossRef] [PubMed]
- Nasimi, N.; Dabbaghmanesh, M.H.; Sohrabi, Z. Nutritional status and body fat mass: Determinants of sarcopenia in community-dwelling older adults. Exp. Gerontol. 2019, 122, 67–73. [Google Scholar] [CrossRef]
- Volpato, S.; Bianchi, L.; Cherubini, A.; Landi, F.; Maggio, M.; Savino, E.; Bandinelli, S.; Ceda, G.P.; Guralnik, J.M.; Zuliani, G.; et al. Prevalence and Clinical Correlates of Sarcopenia in Community-Dwelling Older People: Application of the EWGSOP Definition and Diagnostic Algorithm. Journals Gerontol. Ser. A: Boil. Sci. Med Sci. 2013, 69, 438–446. [Google Scholar] [CrossRef]
- Han, P.; Kang, L.; Guo, Q.; Wang, J.; Zhang, W.; Shen, S.; Wang, X.; Dong, R.; Ma, Y.; Shi, Y.; et al. Prevalence and Factors Associated With Sarcopenia in Suburb-dwelling Older Chinese Using the Asian Working Group for Sarcopenia Definition. Journals Gerontol. Ser. A: Boil. Sci. Med Sci. 2015, 71, 529–535. [Google Scholar] [CrossRef] [Green Version]
- Dodds, R.M.; Granic, A.; Davies, K.; Kirkwood, T.B.; Jagger, C.; Sayer, A.A. Prevalence and incidence of sarcopenia in the very old: Findings from the Newcastle 85+ Study. J. Cachexia Sarcopenia Muscle 2017, 8, 229–237. [Google Scholar] [CrossRef]
- Nakamura, K.; Yoshida, D.; Honda, T.; Hata, J.; Shibata, M.; Hirakawa, Y.; Furuta, Y.; Kishimoto, H.; Ohara, T.; Kitazono, T.; et al. Prevalence and Mortality of Sarcopenia in a Community-dwelling Older Japanese Population: The Hisayama Study. J. Epidemiology 2021, 31, 320–327. [Google Scholar] [CrossRef]
- Kurose, S.; Nishikawa, S.; Nagaoka, T.; Kusaka, M.; Kawamura, J.; Nishioka, Y.; Sato, S.; Tsutsumi, H.; Kimura, Y. Prevalence and risk factors of sarcopenia in community-dwelling older adults visiting regional medical institutions from the Kadoma Sarcopenia Study. Sci. Rep. 2020, 10, 19129. [Google Scholar] [CrossRef]
- Lau, E.M.; Lynn, H.S.; Woo, J.W.; Kwok, T.C.; Melton, L.J. 3rd. Prevalence of and risk factors for sarcopenia in elderly Chinese men and women. J. Gerontol. Biol. Sci. Med. Sci. 2005, 60, 213–216. [Google Scholar] [CrossRef] [Green Version]
- Wang, H.; Hai, S.; Liu, Y.; Liu, X.Y.; Zhou, J.H.; Yang, Y.; Dong, B.R.; Yue, J.R. Prevalence of sarcopenia and associated factors in community-dwelling elderly population in Chengdu China. Sichuan Da Xue Xue Bao Yi Xue Ban 2019, 50, 224–228. (In Chinese) [Google Scholar]
- Tramontano, A.; Veronese, N.; Sergi, G.; Manzato, E.; Rodriguez-Hurtado, D.; Maggi, S.; Trevisan, C.; De Zaiacomo, F.; Gi-antin, V. Prevalence of sarcopenia and associated factors in the healthy older adults of the Peruvian Andes. Arch. Gerontol. Geriatr. 2017, 68, 49–54. [Google Scholar] [CrossRef] [PubMed]
- Figueiredo, C.P.; Domiciano, D.S.; Lopes, J.B.; Caparbo, V.F.; Scazufca, M.; Bonfá, E.; Pereira, R.M. Prevalence of sarcopenia and associated risk factors by two diagnostic criteria in community-dwelling older men: The São Paulo Ageing & Health Study (SPAH). Osteoporos. Int. 2014, 25, 589–596. [Google Scholar]
- Moreira, V.G.; Perez, M.; Lourenço, R.A. Prevalence of sarcopenia and its associated factors: The impact of muscle mass, gait speed, and handgrip strength reference values on reported frequencies. Clinics 2019, 74, e477. [Google Scholar] [CrossRef] [PubMed]
- Erkoyun, E.; Uçku, R. The prevalence of sarcopenia risk and associated factors in patients aged 65-79 years living in a district of Izmir province of Turkey. Turk. J. Phys. Med. Rehabil. 2020, 6, 10–16. [Google Scholar] [CrossRef] [PubMed]
- Momoki, C.; Habu, D.; Ogura, J.; Tada, A.; Hasei, A.; Sakurai, K.; Watanabe, H. Relationships between sarcopenia and household status and locomotive syndrome in a community-dwelling elderly woman in Japan. Geriatr. Gerontol. Int. 2017, 17, 54–60. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Confortin, S.C.; Ono, L.M.; Barbosa, A.R.; d’Orsi, E. Sarcopenia and its association with changes in socioeconomic, behavioral, and health factors: The EpiFloripa Elderly Study. Cad. Saude. Publica 2018, 34, e00164917. [Google Scholar] [PubMed] [Green Version]
- Badrasawi, M.; Jarradat, A.; Khodour, Z.; Lahaleh, R.; Irshaied, A. Sarcopenia prevalence and its correlations with age-related disorders among community-dwelling Palestinian older adults. J. Gerontol. Geriatr. 2020, 68, 126–135. [Google Scholar] [CrossRef]
- Wang, G.; Cai, W.; Shen, X.; Zhang, Q.; Li, C.Y. The application of EWGSOP2 consensus in the screening for sarcopenia in the elderly in Shanghai communities. Chin. J. Clin. Healthc. 2020, 23, 325–330. (In Chinese) [Google Scholar]
- Zhang, Y.; Tan, Y.; Huang, X.; Zhang, Z.; Bai, J.; Zhang, M.; Huang, Y.; Chen, J.; Wang, J.; Bao, Z.; et al. Prevalence of sarcopenia and the associated risk factors in community elderly in Shang-hai. Geriatr. Heal. Care 2018, 24, 608–613. (In Chinese) [Google Scholar]
- Huang, L.; Liu, Y.; Wen, Y.; Liu, K. State and associated factors of sarcopenia in Jinzhou community elderly people. Mod. Prevent. Med. 2017, 44, 4458–4460. (In Chinese) [Google Scholar]
- Mei, J.; Yu, H.; Xia, X. Influencing factors of sarcopenia in community-dwelling elderly of Huangshi. Chin. J. Mod. Med. 2017, 27, 85–89. (In Chinese) [Google Scholar]
- Shafiee, G.; Heshmat, R.; Ostovar, A.; Khatami, F.; Fahimfar, N.; Arzaghi, S.M.; Gharibzadeh, S.; Hanaei, S.; Nabipour, I.; Larijani, B. Comparison of EWGSOP-1and EWGSOP-2 diagnostic criteria on prevalence of and risk factors for sarcopenia among Iranian older people: The Bushehr Elderly Health (BEH) program. J. Diabetes. Metab. Disord. 2020, 19, 727–734. [Google Scholar] [CrossRef]
- Kim, J.E.; Lee, Y.H.; Huh, J.H.; Kang, D.R.; Rhee, Y.; Lim, S.K. Early-stage chronic kidney disease, insulin resistance, and osteoporosis as risk factors of sarcopenia in aged population: The fourth Korea National Health and Nutrition Examination Survey (KNHANES IV), 2008-2009. Osteoporos Int. 2014, 25, 2189–2198. [Google Scholar] [CrossRef]
- Alexandre, T.; Duarte, Y.A.; Santos, J.L.; Wong, R.; Lebrão, M.L. Prevalence and associated factors of sarcopenia among elderly in Brazil: Findings from the SABE study. J. Nutr. Health Aging 2014, 18, 284–290. [Google Scholar] [CrossRef]
- Pérez-Sousa M, Á.; Pozo-Cruz, J.D.; Cano-Gutiérrez, C.A.; Izquierdo, M.; Ramírez-Vélez, R. High prevalence of probable sarcopenia in a representative sample from Colombia: Implications for geriatrics in Latin America. J. Am. Med. Dir. Assoc. 2021, 22, 859–864.e1. [Google Scholar] [CrossRef] [PubMed]
- Dodds, R.M.; Murray, J.C.; Robinson, S.M.; Sayer, A.A. The identification of probable sarcopenia in early old age based on the SARC-F tool and clinical suspicion: Findings from the 1946 British birth cohort. Eur. Geriatr. Med. 2020, 11, 433–441. [Google Scholar] [CrossRef] [Green Version]
- Zhang, Y.; Chen, X.; Hou, L.; Lin, X.; Qin, D.; Wang, H.; Hai, S.; Cao, L.; Dong, B. Prevalence and risk factors governing the loss of muscle function in elderly sarcopenia patients: A longitudinal Study in China with 4 Years of Follow-Up. J. Nutr. Health Aging 2020, 24, 518–524. [Google Scholar] [CrossRef] [PubMed]
- Simsek, H.; Meseri, R.; Sahin, S.; Kilavuz, A.; Bicakli, D.H.; Uyar, M.; Savas, S.; Sarac, F.; Akcicek, F. Prevalence of sarcopenia and related factors in community-dwelling elderly individuals. Saudi Med. J. 2019, 40, 568–574. [Google Scholar] [CrossRef]
- Yuenyongchaiwat, K.; Boonsinsukh, R. Sarcopenia and its relationships with depression, cognition, and physical activity in Thai community-dwelling older adults. Curr. Gerontol. Geriatr. Res. 2020, 2020, 8041489. [Google Scholar]
- Kitamura, A.; Seino, S.; Abe, T.; Nofuji, Y.; Yokoyama, Y.; Amano, H.; Nishi, M.; Taniguchi, Y.; Narita, M.; Fujiwara, Y.; et al. Sarcopenia: Prevalence, associated factors, and the risk of mortality and disability in Japanese older adults. J. Cachexia Sarcopenia Muscle 2021, 12, 30–38. [Google Scholar] [CrossRef]
- Xu, H.Q.; Shi, J.P.; Shen, C.; Liu, Y.; Liu, J.M.; Zheng, X.Y. Sarcopenia-related features and factors associated with low muscle mass, weak muscle strength, and reduced function in Chinese rural residents: A cross-sectional study. Arch. Osteoporos. 2018, 14, 2. [Google Scholar] [CrossRef] [PubMed]
- Wu, C.H.; Chen, K.T.; Hou, M.T.; Chang, Y.F.; Chang, C.S.; Liu, P.Y.; Wu, S.J.; Chiu, C.J.; Jou, I.M.; Chen, C.Y. Prevalence and associated factors of sarcopenia and severe sarcopenia in older Taiwanese living in rural community: The Tianliao old people study 04. Geriatr. Gerontol. Int. 2014, 14, 69–75. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chien, M.Y.; Wang, L.Y.; Chen, H.C. The relationship of sleep duration with obesity and sarcopenia in community-dwelling older adults. Gerontology 2015, 61, 399–406. [Google Scholar] [CrossRef] [PubMed]
- Domiciano, D.S.; Figueiredo, C.P.; Lopes, J.B.; Caparbo, V.F.; Takayama, L.; Menezes, P.R.; Bonfa, E.; Pereira, R.M. Discriminating sarcopenia in community-dwelling older women with high frequency of overweight/obesity: The São Paulo Ageing & Health Study (SPAH). Osteoporos Int. 2013, 24, 595–603. [Google Scholar]
- Hu, X.; Jiang, J.; Wang, H.; Zhang, L.; Dong, B.; Yang, M. Association between sleep duration and sarcopenia among community-dwelling older adults: A cross-sectional study. Medicine 2017, 96, e6268. [Google Scholar] [CrossRef]
- Landi, F.; Liperoti, R.; Russo, A.; Giovannini, S.; Tosato, M.; Barillaro, C.; Capoluongo, E.; Bernabei, R.; Onder, G. Association of anorexia with sarcopenia in a community-dwelling elderly population: Results from the ilSIRENTE study. Eur. J. Nutr. 2013, 52, 1261–1268. [Google Scholar] [CrossRef]
- Tsutsumimoto, K.; Doi, T.; Nakakubo, S.; Kim, M.; Kurita, S.; Ishii, H.; Shimada, H. Association between anorexia of ageing and sarcopenia among Japanese older adults. J. Cachexia Sarcopenia Muscle 2020, 11, 1250–1257. [Google Scholar] [CrossRef] [Green Version]
- Keng, B.; Gao, F.; Teo, L.; Lim, W.S.; Tan, R.S.; Ruan, W.; Ewe, S.H.; Koh, W.P.; Koh, A.S. Associations between skeletal muscle and myocardium in aging: A syndrome of “Cardio-Sarcopenia”? J. Am. Geriatr. Soc. 2019, 67, 2568–2573. [Google Scholar] [CrossRef] [PubMed]
- Souza, A.; Nascimento, D.; Rodrigues, I.; Charone, C.; Lopes, G.L.; Lima, R.S.; Sá, A.A.; Carneiro, T.X.; Moraes, N.S. Association between sarcopenia and diabetes in community dwelling elderly in the Amazon region-Viver Mais Project. Arch. Gerontol. Geriatr. 2019, 83, 121–125. [Google Scholar] [CrossRef]
- Wang, T.; Feng, X.; Zhou, J.; Gong, H.; Xia, S.; Wei, Q.; Hu, X.; Tao, R.; Li, L.; Qian, F.; et al. Type 2 diabetes mellitus is associated with increased risks of sarcopenia and pre-sarcopenia in Chinese elderly. Sci. Rep. 2016, 6, 38937. [Google Scholar] [CrossRef] [Green Version]
- Hsu, Y.H.; Liang, C.K.; Chou, M.Y.; Liao, M.C.; Lin, Y.T.; Chen, L.K.; Lo, Y.K. Association of cognitive impairment, depressive symptoms and sarcopenia among healthy older men in the veteran’s retirement community in southern Taiwan: A cross-sectional study. Geriatr. Gerontol. Int. 2014, 14, 102–108. [Google Scholar] [CrossRef] [Green Version]
- Tzeng, P.L.; Lin, C.Y.; Lai, T.F.; Huang, W.C.; Pien, E.; Hsueh, M.C.; Lin, K.P.; Park, J.H.; Liao, Y. Daily lifestyle behaviors and risks of sarcopenia among older adults. Arch. Public Health 2020, 78, 113. [Google Scholar] [CrossRef]
- Daskalopoulou, C.; Wu, Y.T.; Pan, W.; Giné Vázquez, I.; Prince, M.; Prina, M.; Tyrovolas, S. Factors related with sarcopenia and sarcopenic obesity among low-and middle-income settings: The 10/66 DRG study. Sci. Rep. 2020, 10, 20453. [Google Scholar] [CrossRef] [PubMed]
- Dutra, T.; Pinheiro, P.A.; Carneiro, J.A.O.; Coqueiro, R.D.S.; Fernandes, M.H. Prevalence and factors associated with sarcopenia in elderly women living in the community. Revista Brasileira De Cineantropometria Desempenho Humano 2015, 17, 460–471. [Google Scholar] [CrossRef] [Green Version]
- da Silva, A.P.; Matos, A.; Ribeiro, R.; Gil, Â.; Valente, A.; Bicho, M.; Gorjão-Clara, J. Sarcopenia and osteoporosis in Portuguese centenarians. Eur. J. Clin. Nutr. 2017, 71, 56–63. [Google Scholar] [CrossRef] [PubMed]
- Wu, X.; Li, X.; Xu, M.; Zhang, Z.; He, L.; Li, Y. Sarcopenia prevalence and associated factors among older Chinese population: Findings from the China Health and Retirement Longitudinal Study. PLoS ONE 2021, 16, e0247617. [Google Scholar]
- Andreia, P.; Zaperllon, M.G.; PADAraújo Bertoldo, B.; Santos, S.; Luiz, P.E. Sarcopenia: Prevalence and associated factors among elderly from a Brazilian capital. Fisioterapia Em Movimento 2018, 31, e003102. [Google Scholar]
- Murphy, R.A.; Ip, E.H.; Zhang, Q.; Boudreau, R.M.; Cawthon, P.M.; Newman, A.B.; Tylavsky, F.A.; Visser, M.; Goodpaster, B.H.; Harris, T.B.; et al. Transition to sarcopenia and determinants of transitions in older adults: A popula-tion-based study. J. Gerontol. Biol. Sci. Med. Sci. 2014, 69, 751–758. [Google Scholar] [CrossRef]
- Xie, W.Q.; Xiao, G.L.; Fan, Y.B.; He, M.; Lv, S.; Li, Y.S. Sarcopenic obesity: Research advances in pathogenesis and diagnostic criteria. Aging Clin. Exp. Res. 2021, 33, 247–252. [Google Scholar] [CrossRef] [PubMed]
- Cruz-Jentoft, A.J.; Sayer, A.A. Sarcopenia. Lancet 2019, 393, 2636–2646. [Google Scholar] [CrossRef]
- Cheng, Q.; Zhu, X.; Zhang, X.; Li, H.; Du, Y.; Hong, W.; Xue, S.; Zhu, H. A cross-sectional study of loss of muscle mass corresponding to sarcopenia in healthy Chinese men and women: Reference values, prevalence, and association with bone mass. J. Bone Miner. Metab. 2014, 32, 78–88. [Google Scholar] [CrossRef] [PubMed]
- Chittal, P.; Babu, A.S.; Lavie, C.J. Obesity paradox: Does fat alter outcomes in chronic obstructive pulmonary disease? COPD 2015, 12, 14–18. [Google Scholar] [CrossRef]
- Lavie, C.J.; De Schutter, A.; Parto, P.; Jahangir, E.; Kokkinos, P.; Ortega, F.B.; Arena, R.; Milani, R.V. Obesity and prevalence of cardiovascular diseases and prognosis-the obesity paradox updated. Prog. Cardiovasc. Dis. 2016, 58, 537–547. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ahmadi, S.F.; Zahmatkesh, G.; Streja, E.; Mehrotra, R.; Rhee, C.M.; Kovesdy, C.P.; Gillen, D.L.; Ahmadi, E.; Fonarow, G.C.; Kalantar-Zadeh, K. Association of body mass index with mortality in peritoneal dialysis patients: A systematic review and meta-analysis. Perit. Dial. Int. 2016, 36, 315–325. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shafiee, G.; Keshtkar, A.; Soltani, A.; Ahadi, Z.; Larijani, B.; Heshmat, R. Prevalence of sarcopenia in the world: A systematic review and meta-analysis of general population studies. J. Diabetes Metab. Disord. 2017, 16, 21. [Google Scholar] [CrossRef] [Green Version]
- Steffl, M.; Bohannon, R.W.; Petr, M.; Kohlikova, E.; Holmerova, I. Relation between cigarette smoking and sarcopenia: Meta-analysis. Physiol. Res. 2015, 64, 419–426. [Google Scholar] [CrossRef]
- Pourmotabbed, A.; Ghaedi, E.; Babaei, A.; Mohammadi, H.; Khazaie, H.; Jalili, C.; Symonds, M.E.; Moradi, S.; Miraghajani, M. Sleep duration and sarcopenia risk: A systematic review and dose-response meta-analysis. Sleep Breath. 2020, 24, 1267–1278. [Google Scholar] [CrossRef]
- Steffl, M.; Bohannon, R.W.; Sontakova, L.; Tufano, J.J.; Shiells, K.; Holmerova, I. Relationship between sarcopenia and physical activity in older people: A systematic review and meta-analysis. Clin. Interv. Aging 2017, 12, 835–845. [Google Scholar] [CrossRef] [Green Version]
- Beaudart, C.; the IOF-ESCEO Sarcopenia Working Group; Dawson, A.; Shaw, S.C.; Harvey, N.; Kanis, J.A.; Binkley, N.; Reginster, J.Y.; Chapurlat, R.; Chan, D.C.; et al. Nutrition and physical activity in the prevention and treatment of sarcopenia: Systematic review. Osteoporos. Int. 2017, 28, 1817–1833. [Google Scholar] [CrossRef] [Green Version]
- Steffl, M.; Bohannon, R.W.; Petr, M.; Kohlikova, E.; Holmerova, I. Alcohol consumption as a risk factor for sarcopenia-a meta-analysis. BMC Geriatr. 2016, 16, 99. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sandri, M. Protein breakdown in muscle wasting: Role of autophagy-lysosome and ubiquitin-proteasome. Int. J. Biochem. Cell Biol. 2013, 45, 2121–2129. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, X.; Huang, P.; Dou, Q.; Wang, C.; Zhang, W.; Yang, Y.; Wang, J.; Xie, X.; Zhou, J.; Zeng, Y. Falls among older adults with sarcopenia dwelling in nursing home or community: A meta-analysis. Clin. Nutr. 2020, 39, 33–39. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Luo, D.; Lin, Z.; Li, S.; Liu, S.J. Effect of nutritional supplement combined with exercise intervention on sarcopenia in the elderly: A meta-analysis. Int. J. Nurs. Sci. 2017, 4, 389–401. [Google Scholar] [CrossRef]
- Vlietstra, L.; Hendrickx, W.; Waters, D.L. Exercise interventions in healthy older adults with sarcopenia: A systematic review and meta-analysis. Australas. J. Ageing 2018, 37, 169–183. [Google Scholar] [CrossRef]
- Liao, C.D.; Chen, H.C.; Huang, S.W.; Liou, T.H. The Role of Muscle Mass Gain Following Protein Supplementation Plus Exercise Therapy in Older Adults with Sarcopenia and Frailty Risks: A Systematic Review and Meta-Regression Analysis of Randomized Trials. Nutrients 2019, 11, 1713. [Google Scholar] [CrossRef] [Green Version]
- Yoshimura, Y.; Wakabayashi, H.; Yamada, M.; Kim, H.; Harada, A.; Arai, H. Interventions for Treating Sarcopenia: A Systematic Review and Meta-Analysis of Randomized Controlled Studies. J. Am. Med. Dir. Assoc. 2017, 18, 553.e1–553.e16. [Google Scholar] [CrossRef]
- Wu, P.Y.; Huang, K.S.; Chen, K.M.; Chou, C.P.; Tu, Y.K. Exercise, Nutrition, and combined exercise and nutrition in older adults with sarcopenia: A systematic review and network meta-analysis. Maturitas 2021, 145, 38–48. [Google Scholar] [CrossRef]
- Noubiap, J.J.; Balti, E.V.; Bigna, J.J.; Echouffo-Tcheugui, J.B.; Kengne, A.P. Dyslipidaemia in Africa-comment on a recent systematic review-Authors' reply. Lancet Glob. Health 2019, 7, e308–e309. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Associated Factors | Number of Studies | Heterogeneity | OR (95% CI) | ||
|---|---|---|---|---|---|
| I2 | p | ||||
| Sociodemographic factors | BMI Under weight | 14 | 78.1 | <0.001 | 3.78 (2.55, 5.60) |
| Marital status | 7 | 71.2 | <0.001 | 1.57 (1.08, 2.28) | |
| ADL disability | 7 | 84.7 | <0.001 | 1.49 (1.15, 1.92) | |
| Age (years) | 34 | 80.7 | <0.001 | 1.12 (1.10, 1.13) | |
| Behavioral factors | Sleeping time < 6 h | 2 | 0.0 | 0.473 | 3.32 (1.86, 5.93) |
| Malnutrition/malnutrition risk | 10 | 46.7 | 0.029 | 2.99 (2.40, 3.72) | |
| Sleeping time ≥ 8 h | 2 | 14.7 | 0.279 | 2.30 (1.37, 3.86) | |
| Physical inactivity | 18 | 65.2 | <0.001 | 1.73 (1.48, 2.01) | |
| Living alone | 5 | 36.0 | 0.167 | 1.55 (1.00, 2.40) | |
| Smoking | 29 | 49.5 | <0.001 | 1.20 (1.10, 1.31) | |
| Disease-related factors | Osteopenia/osteoporosis | 6 | 75.2 | <0.001 | 2.73 (1.63, 4.57) |
| Cognitive impairment | 6 | 69.9 | 0.001 | 1.62 (1.05, 2.51) | |
| Anorexia | 2 | 0.0 | 0.425 | 1.50 (1.14, 1.96) | |
| Depression | 11 | 69.4 | <0.001 | 1.46 (1.17, 1.83) | |
| Diabetes | 19 | 56.7 | <0.001 | 1.40 (1.18, 1.66) | |
| Anemia | 2 | 8.3 | 0.351 | 1.39 (1.06, 1.82) | |
| Osteoarthritis | 6 | 32.7 | 0.167 | 1.33 (1.23, 1.44) | |
| Fall | 9 | 0.0 | 0.461 | 1.28 (1.14, 1.44) | |
| Respiratory diseases | 7 | 0.0 | 0.757 | 1.22 (1.09, 1.36) | |
| Heart diseases | 5 | 0.0 | 0.966 | 1.14 (1.00, 1.30) | |
| Not Associated Factors | Number of Studies | Heterogeneity | OR (95% CI) | ||
|---|---|---|---|---|---|
| I2 | p | ||||
| Sociodemographic factors | Male | 11 | 86.4 | <0.001 | 1.50 (0.96, 2.34) |
| Female | 21 | 86.1 | <0.001 | 1.10 (0.80, 1.51) | |
| High level of education | 11 | 60.8 | <0.001 | 0.95 (0.92, 0.98) | |
| BMI Overweight/obesity | 12 | 93.5 | <0.001 | 0.27 (0.17, 0.44) | |
| Behavioral factors | Drinking | 21 | 48.3 | 0.001 | 0.92 (0.84, 1.01) |
| Disease-related factors | Kidney disease | 2 | 78.2 | 0.032 | 2.52 (0.19, 33.30) |
| Stoke | 4 | 81.8 | 0.001 | 1.70 (0.69, 4.17) | |
| Hyperlipidemia | 5 | 29.5 | 0.214 | 1.14 (0.89, 1.47) | |
| Pain | 3 | 12.7 | 0.332 | 1.08 (0.98, 1.20) | |
| Hypertension | 13 | 52.4 | 0.009 | 0.98 (0.84, 1.14) | |
| Cancer | 5 | 0.0 | 0.542 | 0.88 (0.85, 0.92) | |
| Liver disease | 3 | 26.6 | 0.256 | 0.88 (0.85, 0.91) | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gao, Q.; Hu, K.; Yan, C.; Zhao, B.; Mei, F.; Chen, F.; Zhao, L.; Shang, Y.; Ma, Y.; Ma, B. Associated Factors of Sarcopenia in Community-Dwelling Older Adults: A Systematic Review and Meta-Analysis. Nutrients 2021, 13, 4291. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13124291
Gao Q, Hu K, Yan C, Zhao B, Mei F, Chen F, Zhao L, Shang Y, Ma Y, Ma B. Associated Factors of Sarcopenia in Community-Dwelling Older Adults: A Systematic Review and Meta-Analysis. Nutrients. 2021; 13(12):4291. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13124291
Chicago/Turabian StyleGao, Qianqian, Kaiyan Hu, Chunjuan Yan, Bing Zhao, Fan Mei, Fei Chen, Li Zhao, Yi Shang, Yuxia Ma, and Bin Ma. 2021. "Associated Factors of Sarcopenia in Community-Dwelling Older Adults: A Systematic Review and Meta-Analysis" Nutrients 13, no. 12: 4291. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13124291