
Which Probiotic Is the Most Effective for Treating Acute Diarrhea in Children? A Bayesian Network Meta-Analysis of Randomized Controlled Trials



Abstract
:1. Introduction
2. Methods
2.1. Search Strategy
2.2. Study Selection and Data Extraction
2.3. Quality Assessment
2.4. Data Synthesis and Statistical Analysis
3. Results
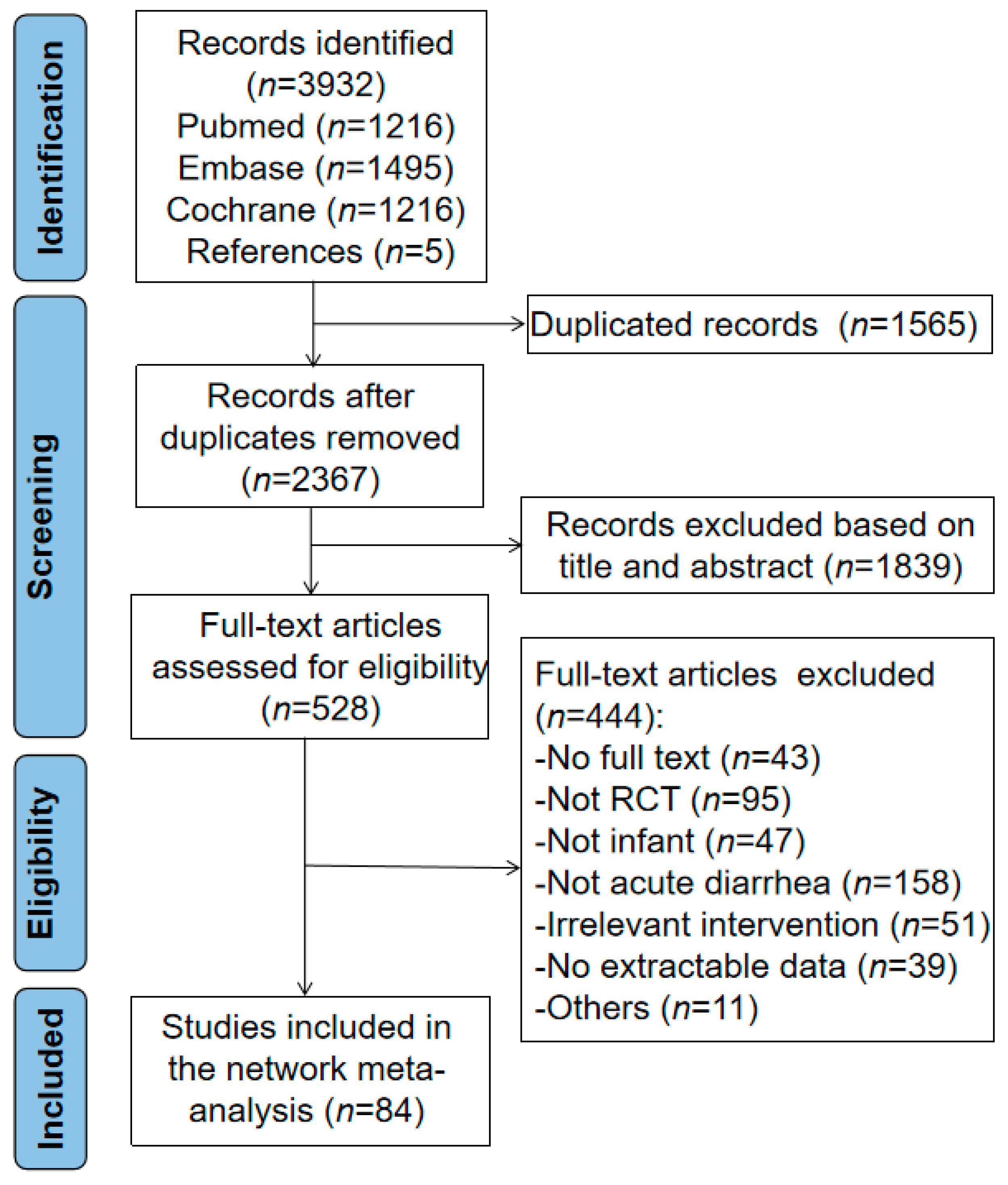
3.1. Characteristics of Included Studies
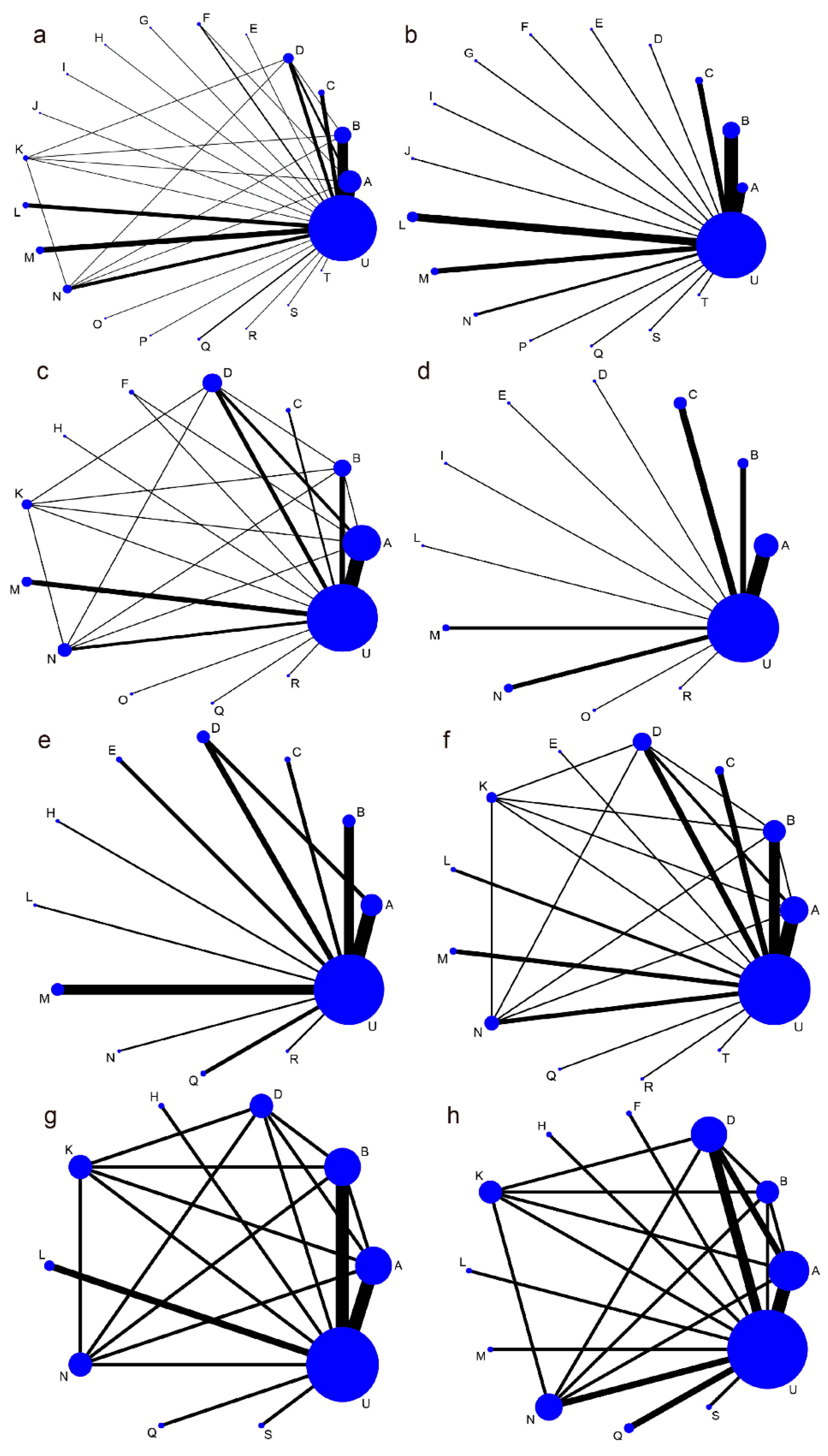
3.2. Network Meta-Analysis Outcomes
3.2.1. Duration of Diarrhea
3.2.2. Diarrhea Lasting ≥2 Days
3.2.3. Duration of Hospitalization
3.2.4. Mean Stool Frequency on Day 2
3.2.5. Duration of Vomiting and Fever
3.3. Risk of Bias Assessment
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Troeger, C.; Colombara, D.V.; Rao, P.C.; Khalil, I.A.; Brown, A.; Brewer, T.G.; Guerrant, R.L.; Houpt, E.R.; Kotloff, K.L.; Misra, K.; et al. Global disability-adjusted life-year estimates of long-term health burden and undernutrition attributable to diarrhoeal diseases in children younger than 5 years. Lancet Glob. Health 2018, 6, e255–e269. [Google Scholar] [CrossRef]
- GBD 2017 Diarrhoeal Disease Collaborators. Quantifying risks and interventions that have affected the burden of diarrhoea among children younger than 5 years: An analysis of the Global Burden of Disease Study 2017. Lancet Infect. Dis. 2020, 20, 37–59. [Google Scholar] [CrossRef]
- World Health Organization. Persistent diarrhoea in children in developing countries: Memorandum from a WHO meeting. Bull. World Health Organ. 1988, 66, 709–717. [Google Scholar]
- Guerrant, R.L.; DeBoer, M.D.; Moore, S.R.; Scharf, R.J.; Lima, A.A. The impoverished gut—A triple burden of diarrhoea, stunting and chronic disease. Nat. Rev. Gastroenterol. Hepatol. 2013, 10, 220–229. [Google Scholar] [CrossRef]
- Li, Y.; Xia, S.; Jiang, X.; Feng, C.; Gong, S.; Ma, J.; Fang, Z.; Yin, J.; Yin, Y. Gut Microbiota and Diarrhea: An Updated Review. Front. Cell. Infect. Microbiol. 2021, 11, 625210. [Google Scholar] [CrossRef]
- Szajewska, H.; Kołodziej, M.; Zalewski, B.M. Systematic review with meta-analysis: Saccharomyces boulardii for treating acute gastroenteritis in children—A 2020 update. Aliment. Pharmacol. Ther. 2020, 51, 678–688. [Google Scholar] [CrossRef]
- Collinson, S.; Deans, A.; Padua-Zamora, A.; Gregorio, G.V.; Li, C.; Dans, L.F.; Allen, S.J. Probiotics for treating acute infectious diarrhoea. Cochrane Database Syst. Rev. 2020, 12. [Google Scholar] [CrossRef]
- Suez, J.; Zmora, N.; Segal, E.; Elinav, E. The pros, cons, and many unknowns of probiotics. Nat. Med. 2019, 25, 716–729. [Google Scholar] [CrossRef]
- Thomas, C.M.; Versalovic, J. Probiotics-host communication: Modulation of signaling pathways in the intestine. Gut Microbes 2010, 1, 148–163. [Google Scholar] [CrossRef]
- Wieers, G.; Belkhir, L.; Enaud, R.; Leclercq, S.; Philippart de Foy, J.M.; Dequenne, I.; de Timary, P.; Cani, P.D. How Probiotics Affect the Microbiota. Front. Cell. Infect. Microbiol. 2019, 9, 454. [Google Scholar] [CrossRef]
- Binder, H.J.; Brown, I.; Ramakrishna, B.S.; Young, G.P. Oral rehydration therapy in the second decade of the twenty-first century. Curr. Gastroenterol. Rep. 2014, 16, 376. [Google Scholar] [CrossRef]
- Islam, T.M.D.T.; Hussain, T.; Rahman, A.; Quaium, S.M.M.A.; Hamid, F. Clinical Efficacy of Bacillus clausii Probiotic in the Management of Acute Diarrhoea in Children. Chattagram Maa-O-Shishu Hosp. Med. Coll. J. 2019, 18, 14–17. [Google Scholar] [CrossRef]
- Depoorter, L.; Vandenplas, Y. Probiotics in Pediatrics. A Review and Practical Guide. Nutrients 2021, 13, 2176. [Google Scholar] [CrossRef]
- Tremblay, A.; Xu, X.; Colee, J.; Tompkins, T.A. Efficacy of a Multi-Strain Probiotic Formulation in Pediatric Populations: A Comprehensive Review of Clinical Studies. Nutrients 2021, 13, 1908. [Google Scholar] [CrossRef]
- Malagón-Rojas, J.N.; Mantziari, A.; Salminen, S.; Szajewska, H. Postbiotics for Preventing and Treating Common Infectious Diseases in Children: A Systematic Review. Nutrients 2020, 12, 389. [Google Scholar] [CrossRef]
- Szajewska, H.; Kołodziej, M.; Gieruszczak-Białek, D.; Skórka, A.; Ruszczyński, M.; Shamir, R. Systematic review with meta-analysis: Lactobacillus rhamnosus GG for treating acute gastroenteritis in children—A 2019 update. Aliment. Pharmacol. Ther. 2019, 49, 1376–1384. [Google Scholar] [CrossRef]
- Ianiro, G.; Rizzatti, G.; Plomer, M.; Lopetuso, L.; Scaldaferri, F.; Franceschi, F.; Cammarota, G.; Gasbarrini, A. Bacillus clausii for the Treatment of Acute Diarrhea in Children: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Nutrients 2018, 10, 1074. [Google Scholar] [CrossRef]
- Szajewska, H.; Guarino, A.; Hojsak, I.; Indrio, F.; Kolacek, S.; Orel, R.; Salvatore, S.; Shamir, R.; van Goudoever, J.B.; Vandenplas, Y.; et al. Use of Probiotics for the Management of Acute Gastroenteritis in Children: An Update. J. Pediatr. Gastroenterol. Nutr. 2020, 71, 261–269. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Group, P. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. BMJ 2009, 339, b2535. [Google Scholar] [CrossRef]
- Hutton, B.; Salanti, G.; Caldwell, D.M.; Chaimani, A.; Schmid, C.H.; Cameron, C.; Ioannidis, J.P.; Straus, S.; Thorlund, K.; Jansen, J.P.; et al. The PRISMA extension statement for reporting of systematic reviews incorporating network meta-analyses of health care interventions: Checklist and explanations. Ann. Intern. Med. 2015, 162, 777–784. [Google Scholar] [CrossRef]
- Higgins, J.P.; Altman, D.G.; Gotzsche, P.C.; Juni, P.; Moher, D.; Oxman, A.D.; Savovic, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A.; et al. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef]
- Puhan, M.A.; Schunemann, H.J.; Murad, M.H.; Li, T.; Brignardello-Petersen, R.; Singh, J.A.; Kessels, A.G.; Guyatt, G.H.; Group, G.W. A GRADE Working Group approach for rating the quality of treatment effect estimates from network meta-analysis. BMJ 2014, 349, g5630. [Google Scholar] [CrossRef]
- Brignardello-Petersen, R.; Bonner, A.; Alexander, P.E.; Siemieniuk, R.A.; Furukawa, T.A.; Rochwerg, B.; Hazlewood, G.S.; Alhazzani, W.; Mustafa, R.A.; Murad, M.H.; et al. Advances in the GRADE approach to rate the certainty in estimates from a network meta-analysis. J. Clin. Epidemiol. 2018, 93, 36–44. [Google Scholar] [CrossRef]
- Salanti, G.; Ades, A.E.; Ioannidis, J.P. Graphical methods and numerical summaries for presenting results from multiple-treatment meta-analysis: An overview and tutorial. J. Clin. Epidemiol. 2011, 64, 163–171. [Google Scholar] [CrossRef]
- Shim, S.R.; Kim, S.J.; Lee, J.; Rucker, G. Network meta-analysis: Application and practice using R software. Epidemiol. Health 2019, 41, e2019013. [Google Scholar] [CrossRef]
- Wan, X.; Wang, W.; Liu, J.; Tong, T. Estimating the sample mean and standard deviation from the sample size, median, range and/or interquartile range. BMC Med. Res. Methodol. 2014, 14, 135. [Google Scholar] [CrossRef]
- Luo, D.; Wan, X.; Liu, J.; Tong, T. Optimally estimating the sample mean from the sample size, median, mid-range, and/or mid-quartile range. Stat. Methods Med. Res. 2018, 27, 1785–1805. [Google Scholar] [CrossRef]
- Shi, J.; Luo, D.; Weng, H.; Zeng, X.T.; Lin, L.; Chu, H.; Tong, T. Optimally estimating the sample standard deviation from the five-number summary. Res. Synth. Methods 2020, 11, 641–654. [Google Scholar] [CrossRef]
- Vaghela, P.; Langade, R.A. Analysis of impact of ors with zinc & probiotics supplements in curing acute diarrhoea. Int. J. Res. Pharm. Sci. 2020, 11, 4054–4060. [Google Scholar] [CrossRef]
- Shin, D.Y.; Yi, D.Y.; Jo, S.; Lee, Y.M.; Kim, J.H.; Kim, W.; Park, M.R.; Yoon, S.M.; Kim, Y.; Yang, S.; et al. Effect of a new Lactobacillus plantarum product, LRCC5310, on clinical symptoms and virus reduction in children with rotaviral enteritis. Medicine 2020, 99, e22192. [Google Scholar] [CrossRef]
- Mourey, F.; Sureja, V.; Kheni, D.; Shah, P.; Parikh, D.; Upadhyay, U.; Satia, M.; Shah, D.; Troise, C.; Decherf, A. A Multicenter, Randomized, Double-Blind, Placebo-Controlled Trial of Saccharomyces boulardii in Infants and Children with Acute Diarrhea. Pediatr. Infect. Dis. J. 2020, 39, e347–e351. [Google Scholar] [CrossRef]
- Kluijfhout, S.; Trieu, T.V.; Vandenplas, Y. Efficacy of the Probiotic Probiotical Confirmed in Acute Gastroenteritis. Pediatr. Gastroenterol. Hepatol. Nutr. 2020, 23, 464–471. [Google Scholar] [CrossRef]
- Chen, K.; Xin, J.; Zhang, G.; Xie, H.; Luo, L.; Yuan, S.; Bu, Y.; Yang, X.; Ge, Y.; Liu, C. A combination of three probiotic strains for treatment of acute diarrhoea in hospitalised children: An open label, randomised controlled trial. Benef. Microbes 2020, 11, 339–346. [Google Scholar] [CrossRef]
- Szymański, H.; Szajewska, H. Lack of Efficacy of Lactobacillus reuteri DSM 17938 for the Treatment of Acute Gastroenteritis: A Randomized Controlled Trial. Pediatr. Infect. Dis. J. 2019, 38, e237–e242. [Google Scholar] [CrossRef]
- Sudha, M.R.; Jayanthi, N.; Pandey, D.C.; Verma, A.K. Bacillus clausii UBBC-07 reduces severity of diarrhoea in children under 5 years of age: A double blind placebo controlled study. Benef. Microbes 2019, 10, 149–154. [Google Scholar] [CrossRef]
- Vidjeadevan, D.; Vinoth, S.; Ramesh, S. Role of Saccharomyces boulardii and Bacillus clausii in reducing the duration of diarrhea: A three-armed randomised controlled trial. Int. J. Contemp. Pediatr. 2018, 5. [Google Scholar] [CrossRef]
- Schnadower, D.; Tarr, P.I.; Casper, T.C.; Gorelick, M.H.; Dean, J.M.; O’Connell, K.J.; Mahajan, P.; Levine, A.C.; Bhatt, S.R.; Roskind, C.G.; et al. Lactobacillus rhamnosus GG versus Placebo for Acute Gastroenteritis in Children. N. Engl. J. Med. 2018, 379, 2002–2014. [Google Scholar] [CrossRef]
- Javeed, A.; Manzoor, S.; Wamiq, S. Effect of oral Saccharomyces boulardii supplementation on the duration of acute watery diarrhea in children. Pak. J. Med. Health Sci. 2018, 12, 212–214. [Google Scholar]
- Hong Chau, T.T.; Minh Chau, N.N.; Hoang Le, N.T.; Chung The, H.; Voong Vinh, P.; Nguyen To, N.T.; Ngoc, N.M.; Tuan, H.M.; Chau Ngoc, T.L.; Kolader, M.E.; et al. A Double-blind, Randomized, Placebo-controlled Trial of Lactobacillus acidophilus for the Treatment of Acute Watery Diarrhea in Vietnamese Children. Pediatr. Infect. Dis. J. 2018, 37, 35–42. [Google Scholar] [CrossRef]
- Freedman, S.B.; Williamson-Urquhart, S.; Farion, K.J.; Gouin, S.; Willan, A.R.; Poonai, N.; Hurley, K.; Sherman, P.M.; Finkelstein, Y.; Lee, B.E.; et al. Multicenter Trial of a Combination Probiotic for Children with Gastroenteritis. N. Engl. J. Med. 2018, 379, 2015–2026. [Google Scholar] [CrossRef]
- Bhat, S.; Shreekrishna, G.N.; Savio, C.D. Efficacy of probiotics in acute diarrhoea in children. Int. J. Contemp. Pediatr. 2018, 5, 1646–1650. [Google Scholar] [CrossRef]
- Sirsat, G.M.; Sankpal, D.M. Role of Saccharomyces boulardii in management of acute diarrhoea of children—A randomized controlled trial. MedPulse Int. J. Pediatr. 2017, 4, 68–72. [Google Scholar]
- Park, M.S.; Kwon, B.; Ku, S.; Ji, G.E. The Efficacy of Bifidobacterium longum BORI and Lactobacillus acidophilus AD031 Probiotic Treatment in Infants with Rotavirus Infection. Nutrients 2017, 9, 887. [Google Scholar] [CrossRef]
- Burki, M.F.K.; Jabeen, F. Efficacy of Saccharomyces boullardii in children with acute diarrhea. Med. Forum Mon. 2017, 28, 112–116. [Google Scholar]
- Yazar, A.S.; Güven, Ş.; Dinleyici, E. Effects of zinc or synbiotic on the duration of diarrhea in children with acute infectious diarrhea. Turk. J. Gastroenterol. 2016, 27, 537–540. [Google Scholar] [CrossRef]
- Sharif, M.R.; Kashani, H.H.; Ardakani, A.T.; Kheirkhah, D.; Tabatabaei, F.; Sharif, A. The Effect of a Yeast Probiotic on Acute Diarrhea in Children. Probiotics Antimicrob. Proteins 2016, 8, 211–214. [Google Scholar] [CrossRef]
- García-Menor, E.; García-Marín, F.; Vecino-López, R.; Horcajo-Martínez, G.; de Ibarrondo Guerrica-Echevarría, M.J.; Gómez-González, P.; Velasco-Ortega, S.; Suárez-Almarza, J.; Nieto-Magro, C. A Multicenter, Prospective, Randomized Controlled Trial to Evaluate the Additional Benefit of a Multistrain Synbiotic (Prodefen®) in the Clinical Management of Acute Viral Diarrhea in Children. Glob. Pediatr. Health 2016, 3. [Google Scholar] [CrossRef]
- Dash, D.K.; Dash, M.; Mohanty, M.D.; Acharya, N. Efficacy of probiotic Saccharomyces boulardii as an adjuvant therapy in acute childhood diarrhoea. J. Nepal Paediatr. Soc. 2016, 36, 250–255. [Google Scholar] [CrossRef]
- Das, S.; Gupta, P.K.; Das, R.R. Efficacy and Safety of Saccharomyces boulardii in Acute Rotavirus Diarrhea: Double Blind Randomized Controlled Trial from a Developing Country. J. Trop. Pediatr. 2016, 62, 464–470. [Google Scholar] [CrossRef]
- Lee, D.K.; Park, J.E.; Kim, M.J.; Seo, J.G.; Lee, J.H.; Ha, N.J. Probiotic bacteria, B. longum and L. acidophilus inhibit infection by rotavirus in vitro and decrease the duration of diarrhea in pediatric patients. Clin. Res. Hepatol. Gastroenterol. 2015, 39, 237–244. [Google Scholar] [CrossRef]
- Hegar, B.; Waspada, I.M.; Gunardi, H.; Vandenplas, Y. A double blind randomized trial showing probiotics to be ineffective in acute diarrhea in Indonesian children. Indian J. Pediatr. 2015, 82, 410–414. [Google Scholar] [CrossRef] [PubMed]
- Freedman, S.B.; Sherman, P.M.; Willan, A.; Johnson, D.; Gouin, S.; Schuh, S. Emergency Department Treatment of Children with Diarrhea who Attend Day Care: A Randomized Multidose Trial of a Lactobacillus helveticus and Lactobacillus rhamnosus Combination Probiotic. Clin. Pediatr. 2015, 54, 1158–1166. [Google Scholar] [CrossRef] [PubMed]
- El-Soud, N.H.A.; Said, R.N.; Mosallam, D.S.; Barakat, N.A.M.; Sabry, M.A. Bifidobacterium lactis in treatment of children with acute diarrhea. A randomized double blind controlled trial. Maced. J. Med. Sci. 2015, 3, 403–407. [Google Scholar] [CrossRef]
- Dinleyici, E.C.; Kara, A.; Dalgic, N.; Kurugol, Z.; Arica, V.; Metin, O.; Temur, E.; Turel, O.; Guven, S.; Yasa, O.; et al. Saccharomyces boulardii CNCM I-745 reduces the duration of diarrhoea, length of emergency care and hospital stay in children with acute diarrhoea. Benef. Microbes 2015, 6, 415–421. [Google Scholar] [CrossRef] [PubMed]
- Dinleyici, E.C.; Dalgic, N.; Guven, S.; Metin, O.; Yasa, O.; Kurugol, Z.; Turel, O.; Tanir, G.; Yazar, A.S.; Arica, V.; et al. Lactobacillus reuteri DSM 17938 shortens acute infectious diarrhea in a pediatric outpatient setting. J. Pediatr. 2015, 91, 392–396. [Google Scholar] [CrossRef] [PubMed]
- Sindhu, K.N.; Sowmyanarayanan, T.V.; Paul, A.; Babji, S.; Ajjampur, S.S.; Priyadarshini, S.; Sarkar, R.; Balasubramanian, K.A.; Wanke, C.A.; Ward, H.D.; et al. Immune response and intestinal permeability in children with acute gastroenteritis treated with Lactobacillus rhamnosus GG: A randomized, double-blind, placebo-controlled trial. Clin. Infect. Dis. 2014, 58, 1107–1115. [Google Scholar] [CrossRef]
- Dinleyici, E.C.; Vandenplas, Y. Lactobacillus reuteri DSM 17938 effectively reduces the duration of acute diarrhoea in hospitalised children. Acta Paediatr. 2014, 103, e300–e305. [Google Scholar] [CrossRef]
- Huang, Y.F.; Liu, P.Y.; Chen, Y.Y.; Nong, B.R.; Huang, I.F.; Hsieh, K.S.; Chen, K.T. Three-combination probiotics therapy in children with salmonella and rotavirus gastroenteritis. J. Clin. Gastroenterol. 2014, 48, 37–42. [Google Scholar] [CrossRef]
- Azim, K.; Sheikh, T.S.; Khan, S.N. Efficacy of probiotics (Saccharomyces bulardii) in acute watery diarrhoea in children. J. Rawalpindi Med. Coll. 2014, 18, 213–215. [Google Scholar]
- Aggarwal, S.; Upadhyay, A.; Shah, D.; Teotia, N.; Agarwal, A.; Jaiswal, V. Lactobacillus GG for treatment of acute childhood diarrhoea: An open labelled, randomized controlled trial. Indian J. Med. Res. 2014, 139, 379–385. [Google Scholar]
- Phavichitr, N.; Puwdee, P.; Tantibhaedhyangkul, R. Cost-benefit analysis of the probiotic treatment of children hospitalized for acute diarrhea in Bangkok, Thailand. Southeast Asian J. Trop. Med. Public Health 2013, 44, 1065–1071. [Google Scholar] [PubMed]
- Dinleyici, E.C.; Dalgic, N.; Guven, S.; Ozen, M.; Kara, A.; Arica, V.; Metin-Timur, O.; Sancar, M.; Kurugol, Z.; Tanir, G.; et al. The effect of a multispecies synbiotic mixture on the duration of diarrhea and length of hospital stay in children with acute diarrhea in Turkey: Single blinded randomized study. Eur. J. Pediatr. 2013, 172, 459–464. [Google Scholar] [CrossRef] [PubMed]
- Burande, M. Comparison of efficacy of Saccharomyces boulardii strain in the treatment of acute diarrhea in children: A prospective, single-blind, randomized controlled clinical trial. J. Pharmacol. Pharmacother. 2013, 4, 205–208. [Google Scholar] [CrossRef] [PubMed]
- Riaz, M.; Alam, S.; Malik, A.; Ali, S.M. Efficacy and safety of Saccharomyces boulardii in acute childhood diarrhea: A double blind randomised controlled trial. Indian J. Pediatr. 2012, 79, 478–482. [Google Scholar] [CrossRef] [PubMed]
- Nixon, A.F.; Cunningham, S.J.; Cohen, H.W.; Crain, E.F. The effect of Lactobacillus GG on acute diarrheal illness in the pediatric emergency department. Pediatr. Emerg. Care 2012, 28, 1048–1051. [Google Scholar] [CrossRef]
- Khan, A.; Javed, T.; Chishti, A.L. Clinical efficacy of use of probiotic “Saccharomyces boulardii” in children with acute watery diarrhea. Pak. Paediatr. J. 2012, 36, 122–127. [Google Scholar]
- Francavilla, R.; Lionetti, E.; Castellaneta, S.; Ciruzzi, F.; Indrio, F.; Masciale, A.; Fontana, C.; La Rosa, M.M.; Cavallo, L.; Francavilla, A. Randomised clinical trial: Lactobacillus reuteri DSM 17938 vs. placebo in children with acute diarrhoea—A double-blind study. Aliment. Pharmacol. Ther. 2012, 36, 363–369. [Google Scholar] [CrossRef]
- Erdoğan, O.; Tanyeri, B.; Torun, E.; Gönüllü, E.; Arslan, H.; Erenberk, U.; Oktem, F. The comparition of the efficacy of two different probiotics in rotavirus gastroenteritis in children. J. Trop. Med. 2012, 2012, 787240. [Google Scholar] [CrossRef]
- Vandenplas, Y.; De Hert, S.G. Randomised clinical trial: The synbiotic food supplement Probiotical vs. placebo for acute gastroenteritis in children. Aliment. Pharmacol. Ther. 2011, 34, 862–867. [Google Scholar] [CrossRef]
- Dutta, P.; Mitra, U.; Dutta, S.; Rajendran, K.; Saha, T.K.; Chatterjee, M.K. Randomised controlled clinical trial of Lactobacillus sporogenes (Bacillus coagulans), used as probiotic in clinical practice, on acute watery diarrhoea in children. Trop. Med. Int. Health 2011, 16, 555–561. [Google Scholar] [CrossRef]
- Dalgic, N.; Sancar, M.; Bayraktar, B.; Pullu, M.; Hasim, O. Probiotic, zinc and lactose-free formula in children with rotavirus diarrhea: Are they effective? Pediatr. Int. 2011, 53, 677–682. [Google Scholar] [CrossRef]
- Corrêa, N.B.; Penna, F.J.; Lima, F.M.; Nicoli, J.R.; Filho, L.A. Treatment of acute diarrhea with Saccharomyces boulardii in infants. J. Pediatr. Gastroenterol. Nutr. 2011, 53, 497–501. [Google Scholar] [CrossRef]
- Ritchie, B.K.; Brewster, D.R.; Tran, C.D.; Davidson, G.P.; McNeil, Y.; Butler, R.N. Efficacy of Lactobacillus GG in aboriginal children with acute diarrhoeal disease: A randomised clinical trial. J. Pediatr. Gastroenterol. Nutr. 2010, 50, 619–624. [Google Scholar] [CrossRef] [PubMed]
- Rerksuppaphol, S.; Rerksuppaphol, L. Lactobacillus acidophilus and Bifidobacterium bifidum stored at ambient temperature are effective in the treatment of acute diarrhoea. Ann. Trop. Paediatr. 2010, 30, 299–304. [Google Scholar] [CrossRef]
- Grandy, G.; Medina, M.; Soria, R.; Terán, C.G.; Araya, M. Probiotics in the treatment of acute rotavirus diarrhoea. A randomized, double-blind, controlled trial using two different probiotic preparations in Bolivian children. BMC Infect. Dis. 2010, 10, 253. [Google Scholar] [CrossRef]
- Chen, C.C.; Kong, M.S.; Lai, M.W.; Chao, H.C.; Chang, K.W.; Chen, S.Y.; Huang, Y.C.; Chiu, C.H.; Li, W.C.; Lin, P.Y.; et al. Probiotics have clinical, microbiologic, and immunologic efficacy in acute infectious diarrhea. Pediatr. Infect. Dis. J. 2010, 29, 135–138. [Google Scholar] [CrossRef] [PubMed]
- Misra, S.; Sabui, T.K.; Pal, N.K. A randomized controlled trial to evaluate the efficacy of Lactobacillus GG in infantile diarrhea. J. Pediatr. 2009, 155, 129–132. [Google Scholar] [CrossRef]
- Teran, C.G.; Teran-Escalera, C.N.; Villarroel, P. Nitazoxanide vs. probiotics for the treatment of acute rotavirus diarrhea in children: A randomized, single-blind, controlled trial in Bolivian children. Int. J. Infect. Dis. 2009, 13, 518–523. [Google Scholar] [CrossRef] [PubMed]
- Kianifar, H.R.; Farid, R.; Ahanchian, H.; Jabbari, F.; Moghiman, T.; Sistanian, A. Probiotics in the treatment of acute diarrhea in young children. Iran. J. Med. Sci. 2009, 34, 204–207. [Google Scholar]
- Basu, S.; Paul, D.K.; Ganguly, S.; Chatterjee, M.; Chandra, P.K. Efficacy of high-dose Lactobacillus rhamnosus GG in controlling acute watery diarrhea in Indian children: A randomized controlled trial. J. Clin. Gastroenterol. 2009, 43, 208–213. [Google Scholar] [CrossRef]
- Rafeey, M.; Ostadrahimi, A.; Boniadi, M.; Ghorashi, Z.; Alizadeh, M.M.; Hadafey, V. Lactobacillus acidophilus yogurt and supplement in children with acute diarrhea: A clinical trial. Res. J. Med. Sci. 2008, 2, 13–18. [Google Scholar]
- Narayanappa, D. Randomized double blinded controlled trial to evaluate the efficacy and safety of Bifilac in patients with acute viral diarrhea. Indian J. Pediatr. 2008, 75, 709–713. [Google Scholar] [CrossRef]
- Mao, M.; Yu, T.; Xiong, Y.; Wang, Z.; Liu, H.; Gotteland, M.; Brunser, O. Effect of a lactose-free milk formula supplemented with bifidobacteria and streptococci on the recovery from acute diarrhoea. Asia Pac. J. Clin. Nutr. 2008, 17, 30–34. [Google Scholar]
- Villarruel, G.; Rubio, D.M.; Lopez, F.; Cintioni, J.; Gurevech, R.; Romero, G.; Vandenplas, Y. Saccharomyces boulardii in acute childhood diarrhoea: A randomized, placebo-controlled study. Acta Paediatr. 2007, 96, 538–541. [Google Scholar] [CrossRef] [PubMed]
- Ozkan, T.B.; Sahin, E.; Erdemir, G.; Budak, F. Effect of Saccharomyces boulardii in children with acute gastroenteritis and its relationship to the immune response. J. Int. Med. Res. 2007, 35, 201–212. [Google Scholar] [CrossRef]
- Canani, R.B.; Cirillo, P.; Terrin, G.; Cesarano, L.; Spagnuolo, M.I.; De Vincenzo, A.; Albano, F.; Passariello, A.; De Marco, G.; Manguso, F.; et al. Probiotics for treatment of acute diarrhoea in children: Randomised clinical trial of five different preparations. BMJ 2007, 335, 340. [Google Scholar] [CrossRef] [PubMed]
- Henker, J.; Blokhin, B.M.; Bolbot, Y.K.; Maydannik, V.G.; Wolff, C.; Schulze, L. The probiotic E. coli line Nissle 1917 (EcN) stops acute diarrhoea in infants and small children. Results of a confirming study. Z. Gastroenterol. 2006, 44, 863. [Google Scholar]
- Basu, S.; Chatterjee, M.; Ganguly, S.; Chandra, P.K. Efficacy of Lactobacillus rhamnosus GG in acute watery diarrhoea of Indian children: A randomised controlled trial. J. Paediatr. Child Health 2007, 43, 837–842. [Google Scholar] [CrossRef] [PubMed]
- Vivatvakin, B.; Kowitdamrong, E. Randomized control trial of live Lactobacillus acidophilus plus Bifidobacterium infantis in treatment of infantile acute watery diarrhea. J. Med. Assoc. Thail. 2006, 89 (Suppl. 3), S126–S133. [Google Scholar]
- Szymański, H.; Pejcz, J.; Jawień, M.; Chmielarczyk, A.; Strus, M.; Heczko, P.B. Treatment of acute infectious diarrhoea in infants and children with a mixture of three Lactobacillus rhamnosus strains—A randomized, double-blind, placebo-controlled trial. Aliment. Pharmacol. Ther. 2006, 23, 247–253. [Google Scholar] [CrossRef]
- Billoo, A.G.; Memon, M.A.; Khaskheli, S.A.; Murtaza, G.; Iqbal, K.; Saeed Shekhani, M.; Siddiqi, A.Q. Role of a probiotic (Saccharomyces boulardii) in management and prevention of diarrhoea. World J. Gastroenterol. 2006, 12, 4557–4560. [Google Scholar] [CrossRef]
- Sarker, S.A.; Sultana, S.; Fuchs, G.J.; Alam, N.H.; Azim, T.; Brüssow, H.; Hammarström, L. Lactobacillus paracasei strain ST11 has no effect on rotavirus but ameliorates the outcome of nonrotavirus diarrhea in children from Bangladesh. Pediatrics 2005, 116, e221–e228. [Google Scholar] [CrossRef] [PubMed]
- Kurugöl, Z.; Koturoğlu, G. Effects of Saccharomyces boulardii in children with acute diarrhoea. Acta Paediatr. 2005, 94, 44–47. [Google Scholar] [CrossRef] [PubMed]
- Kowalska-Duplaga, K.; Fyderek, K.; Szajewska, H.; Janiak, R. Efficacy of Trilac® in the treatment of acute diarrhoea in infants and young children—A multicentre, randomized, double-blind placebo-controlled study. Pediatr. Wspolczesna 2004, 6, 295–299. [Google Scholar]
- Costa-Ribeiro, H.; Ribeiro, T.C.; Mattos, A.P.; Valois, S.S.; Neri, D.A.; Almeida, P.; Cerqueira, C.M.; Ramos, E.; Young, R.J.; Vanderhoof, J.A. Limitations of probiotic therapy in acute, severe dehydrating diarrhea. J. Pediatr. Gastroenterol. Nutr. 2003, 36, 112–115. [Google Scholar] [CrossRef] [PubMed]
- Rosenfeldt, V.; Michaelsen, K.F.; Jakobsen, M.; Larsen, C.N.; Møller, P.L.; Tvede, M.; Weyrehter, H.; Valerius, N.H.; Paerregaard, A. Effect of probiotic Lactobacillus strains on acute diarrhea in a cohort of nonhospitalized children attending day-care centers. Pediatr. Infect. Dis. J. 2002, 21, 417–419. [Google Scholar] [CrossRef]
- Rosenfeldt, V.; Michaelsen, K.F.; Jakobsen, M.; Larsen, C.N.; Møller, P.L.; Pedersen, P.; Tvede, M.; Weyrehter, H.; Valerius, N.H.; Paerregaard, A. Effect of probiotic Lactobacillus strains in young children hospitalized with acute diarrhea. Pediatr. Infect. Dis. J. 2002, 21, 411–416. [Google Scholar] [CrossRef]
- Hafeez, A.; Tariq, P.; Ali, S.; Kundi, Z.U.; Khan, A.; Hassan, M. The efficacy of Saccharomyces boulardii in the treatment of acute watery diarrhea in children: A multicentre randomized controlled trial. J. Coll. Physicians Surg. Pak. 2002, 12, 432–434. [Google Scholar]
- Urganci, N.; Polat, T.; Uysalol, M.; Cetinkaya, F. Evaluation of the efficacy of Saccharomyces boulardii in children with acute diarrhoea. Arch. Gastroenterohepatol. 2001, 20, 81–83. [Google Scholar]
- Lee, M.C.; Lin, L.H.; Hung, K.L.; Wu, H.Y. Oral bacterial therapy promotes recovery from acute diarrhea in children. Acta Paediatr. Taiwanica 2001, 42, 301–305. [Google Scholar]
- Boudraa, G.; Benbouabdellah, M.; Hachelaf, W.; Boisset, M.; Desjeux, J.F.; Touhami, M. Effect of feeding yogurt versus milk in children with acute diarrhea and carbohydrate malabsorption. J. Pediatr. Gastroenterol. Nutr. 2001, 33, 307–313. [Google Scholar] [CrossRef] [PubMed]
- Guandalini, S.; Pensabene, L.; Zikri, M.A.; Dias, J.A.; Casali, L.G.; Hoekstra, H.; Kolacek, S.; Massar, K.; Micetic-Turk, D.; Papadopoulou, A.; et al. Lactobacillus GG administered in oral rehydration solution to children with acute diarrhea: A multicenter European trial. J. Pediatr. Gastroenterol. Nutr. 2000, 30, 54–60. [Google Scholar] [CrossRef]
- Hernandez, C.L.; Pineda, E.E.; Jimenez, M.I.R.; Lucena, M.S. Clinical therapeutic affect of Saccharomyces boulardii on children with acute diarrhea. Rev. Enferm. Infecc. Pediatr. 1998, 11, 87–89. [Google Scholar]
- Shornikova, A.V.; Isolauri, E.; Burkanova, L.; Lukovnikova, S.; Vesikari, T. A trial in the Karelian Republic of oral rehydration and Lactobacillus GG for treatment of acute diarrhoea. Acta Paediatr. 1997, 86, 460–465. [Google Scholar] [CrossRef] [PubMed]
- Shornikova, A.V.; Casas, I.A.; Mykkänen, H.; Salo, E.; Vesikari, T. Bacteriotherapy with Lactobacillus reuteri in rotavirus gastroenteritis. Pediatr. Infect. Dis. J. 1997, 16, 1103–1107. [Google Scholar] [CrossRef] [PubMed]
- Shornikova, A.V.; Casas, I.A.; Isolauri, E.; Mykkänen, H.; Vesikari, T. Lactobacillus reuteri as a therapeutic agent in acute diarrhea in young children. J. Pediatr. Gastroenterol. Nutr. 1997, 24, 399–404. [Google Scholar] [CrossRef] [PubMed]
- Guarino, A.; Canani, R.B.; Spagnuolo, M.I.; Albano, F.; Di Benedetto, L. Oral bacterial therapy reduces the duration of symptoms and of viral excretion in children with mild diarrhea. J. Pediatr. Gastroenterol. Nutr. 1997, 25, 516–519. [Google Scholar] [CrossRef]
- Pant, A.R.; Graham, S.M.; Allen, S.J.; Harikul, S.; Sabchareon, A.; Cuevas, L.; Hart, C.A. Lactobacillus GG and acute diarrhoea in young children in the tropics. J. Trop. Pediatr. 1996, 42, 162–165. [Google Scholar] [CrossRef]
- Isolauri, E.; Kaila, M.; Mykkänen, H.; Ling, W.H.; Salminen, S. Oral bacteriotherapy for viral gastroenteritis. Dig. Dis. Sci. 1994, 39, 2595–2600. [Google Scholar] [CrossRef]
- Cetina-Sauri, G.; Sierra Basto, G. Evaluation of Saccharomyces boulardii for the treatment of acute diarrhea in pediatric patients. Ann. Pediatr. 1994, 41, 397–400. [Google Scholar]
- Baral, R.; Nonvignon, J.; Debellut, F.; Agyemang, S.A.; Clark, A.; Pecenka, C. Cost of illness for childhood diarrhea in low- and middle-income countries: A systematic review of evidence and modelled estimates. BMC Public Health 2020, 20, 619. [Google Scholar] [CrossRef] [PubMed]
- Patro-Gołąb, B.; Szajewska, H. Systematic Review with Meta-Analysis: Lactobacillus reuteri DSM 17938 for Treating Acute Gastroenteritis in Children. An Update. Nutrients 2019, 11, 2762. [Google Scholar] [CrossRef] [PubMed]
- Rannikko, J.; Holmberg, V.; Karppelin, M.; Arvola, P.; Huttunen, R.; Mattila, E.; Kerttula, N.; Puhto, T.; Tamm, U.; Koivula, I.; et al. Fungemia and Other Fungal Infections Associated with Use of Saccharomyces boulardii Probiotic Supplements. Emerg. Infect. Dis. 2021, 27, 2090–2096. [Google Scholar] [CrossRef] [PubMed]
- Uusitupa, H.M.; Rasinkangas, P.; Lehtinen, M.J.; Makela, S.M.; Airaksinen, K.; Anglenius, H.; Ouwehand, A.C.; Maukonen, J. Bifidobacterium animalis subsp. lactis 420 for Metabolic Health: Review of the Research. Nutrients 2020, 12, 892. [Google Scholar] [CrossRef]
- Derrien, M.; van Hylckama Vlieg, J.E. Fate, activity, and impact of ingested bacteria within the human gut microbiota. Trends Microbiol. 2015, 23, 354–366. [Google Scholar] [CrossRef]
- Morgan, R.L.; Preidis, G.A.; Kashyap, P.C.; Weizman, A.V.; Sadeghirad, B.; McMaster Probiotic, P.; Synbiotic Work, G. Probiotics Reduce Mortality and Morbidity in Preterm, Low-Birth-Weight Infants: A Systematic Review and Network Meta-analysis of Randomized Trials. Gastroenterology 2020, 159, 467–480. [Google Scholar] [CrossRef]
- Van den Akker, C.H.P.; van Goudoever, J.B.; Szajewska, H.; Embleton, N.D.; Hojsak, I.; Reid, D.; Shamir, R. Probiotics for Preterm Infants: A Strain-Specific Systematic Review and Network Meta-analysis. J. Pediatr. Gastroenterol. Nutr. 2018, 67, 103–122. [Google Scholar] [CrossRef]
- Tan-Lim, C.S.C.; Esteban-Ipac, N.A.R.; Mantaring, J.B.V., 3rd; Chan Shih Yen, E.; Recto, M.S.T.; Sison, O.T.; Alejandria, M.M. Comparative effectiveness of probiotic strains for the treatment of pediatric atopic dermatitis: A systematic review and network meta-analysis. Pediatr. Allergy Immunol. 2021, 32, 124–136. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Intervention | Duration of Diarrhea (MD, 95%CI) | Duration of Diarrhea (Control = Placebo) (MD, 95%CI) | Duration of Diarrhea (Control = No Treatment) (MD, 95%CI) | Diarrhea Lasting ≥ 2 Days (OR, 95%CI) | Duration of Hospitalization (MD, 95%CI) | Mean stool Frequency on Day 2 (MD, 95%CI) | Duration of Vomiting (MD, 95%CI) | Duration of Fever (MD, 95%CI) |
|---|---|---|---|---|---|---|---|---|
| S. boulardii | −0.98 c (−1.29, −0.68) | −1.25 b (−1.59, −0.91) | −0.95 c (−1.33, −0.58) | 0.22 b (0.11, 0.41) | −0.88 c (−1.58, −0.18) | −0.66 b (−1.1, −0.23) | −0.07 b (−0.31, 0.19) | −0.18 c (−0.53, 0.16) |
| LGG | −0.78 c (−1.12, −0.44) | −0.23 b (−0.51, 0.02) | −1.57 c (−2.13, −1.01) | 0.56 c (0.21, 1.4) | −1.21 c (−2.09, −0.33) | −0.66 b (−1.2, −0.14) | −0.16 a (−0.42, 0.09) | −0.56 b (−1.2, 0.11) |
| L. reuteri | −0.91 b (−1.5, −0.32) | −0.84 b (−1.39, −0.29) | −0.98 c (−1.92, −0.04) | 0.23 b (0.090, 0.60) | −0.69 c (−2.02, 0.65) | −1.5 b (−2.3, −0.61) | - | - |
| Bacillus clausii | −0.26 c (−0.78, 0.26) | −0.26 b (−0.96, 0.44) | −0.31 c (−0.90, 0.28) | 0.32 c (0.020, 4.2) | −0.35 c (−1.36, 0.65) | −0.40 a (−0.98, 0.18) | −0.12 b (−0.61, 0.38) | −0.1 b (−0.5, 0.33) |
| L. acidophilus | 0.03 c (−1.27, 1.32) | 0.03 b (−0.74, 0.8) | - | 0.84 c (0.11, 6.2) | −0.28 c (−1.6, 1.04) | 0.0018 c (−1.9, 1.9) | - | - |
| B. lactis | −2.13 c (−3.06, −1.22) | −0.98 b (−1.82, −0.14) | −3.17 c (−4.47, −1.87) | - | - | - | −0.52 c (−1.3, 0.27) | |
| L. sporogenes | −0.1 b (−1.36, 1.17) | −0.1 b (−0.82, 0.62) | - | - | - | - | - | - |
| L. plantarum | −1.23 c (−2.52, 0.06) | - | −1.23 c (−2.55, 0.08) | - | 0.23 c (−1.69, 2.15) | - | −0.08 c (−0.84, 0.68) | −0.23 c (−2.13, 1.64) |
| ECN 1917 | −1.44 d (−2.70, −0.17) | −1.44 d (−2.16, −0.72) | - | 0.50 d (0.062, 4.0) | - | - | - | - |
| L. paracasei | −0.16 b (−1.48, 1.16) | −0.16 b (−0.98, 0.65) | - | - | - | - | - | - |
| E. faecium | 0.16 b (−0.88, 1.20) | - | −0.01 b (−1.09, 1.06) | - | - | −0.22 b (−1.3, 0.80) | −0.12 b (−0.6, 0.36) | 0.08 b (−0.68, 0.86) |
| L. spp. | −0.31 a (−0.93, 0.31) | −0.23 a (−0.67, 0.18) | - | 1.0 b (0.14, 7.3) | −1.1 c (−3.06, 0.86) | −0.22 c (−1.1, 0.70) | −0.24 b (−0.79, 0.31) | −0.2 c (−1.29, 0.89) |
| L. spp. + B. spp. | −0.86 c (−1.33, −0.4) | −0.79 c (−1.22, −0.38) | −0.97 c (−1.57, −0.37) | 0.20 c (0.052, 0.77) | −0.65 c (−1.5, 0.19) | −0.78 d (−1.6, −0.021) | - | −0.66 c (−1.7, 0.39) |
| L. spp. + B. spp. + S. spp. | −1.17 b (−1.75, −0.59) | −1.19 b (−1.81, −0.58) | −1.26 d (−1.99, −0.51) | 0.35 c (0.11, 1.0) | −0.74 c (−2.69, 1.22) | −0.77 b (−1.5, −0.014) | −0.26 b (−0.75, 0.23) | −0.12 b (−0.71, 0.47) |
| L. spp. + S. spp. | −0.73 c (−2.07, 0.61) | - | −0.73 c (−2.1, 0.64) | 0.26 d (0.031, 2.2) | - | - | - | - |
| B. spp. + S. spp. | −0.04 c (−1.28, 1.20) | −0.04 c (−0.71, 0.63) | - | - | - | - | - | - |
| Bacillus spp. + E. spp. + C. spp. | −1.1 c (−2.02, −0.18) | −1.1 b (−1.84, −0.35) | −1.1 c (−2.44, 0.24) | - | −0.46 c (−1.8, 0.91) | −1.6 b (−2.9, −0.44) | −0.63 b (−1.15, −0.11) | −0.12 b (−0.65, 0.44) |
| L. spp. + B. spp. + E. spp. | −1.53 c (−2.82, −0.24) | - | −1.53 c (−2.85, −0.21) | 0.16 d (0.019, 1.4) | −0.83 c (−2.73, 1.07) | −1.3 c (−2.6, 0.073) | - | - |
| L. spp. + B. spp. + Pediococcus spp. | −1.1 c (−2.66, 0.47) | −1.1 c (−2.27, 0.08) | - | - | - | - | −1.20 c (−2.51, 0.11) | −0.5 c (−1.97, 0.97) |
| L. spp. + Bacillus spp. + S. spp. + C. spp. | −1.1 c (−2.49, 0.29) | −1.1 c (−2.03, −0.17) | - | - | - | −0.85 c (−2.5, 0.77) | - | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Li, Z.; Zhu, G.; Li, C.; Lai, H.; Liu, X.; Zhang, L. Which Probiotic Is the Most Effective for Treating Acute Diarrhea in Children? A Bayesian Network Meta-Analysis of Randomized Controlled Trials. Nutrients 2021, 13, 4319. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13124319
Li Z, Zhu G, Li C, Lai H, Liu X, Zhang L. Which Probiotic Is the Most Effective for Treating Acute Diarrhea in Children? A Bayesian Network Meta-Analysis of Randomized Controlled Trials. Nutrients. 2021; 13(12):4319. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13124319
Chicago/Turabian StyleLi, Zengbin, Guixian Zhu, Chao Li, Hao Lai, Xin Liu, and Lei Zhang. 2021. "Which Probiotic Is the Most Effective for Treating Acute Diarrhea in Children? A Bayesian Network Meta-Analysis of Randomized Controlled Trials" Nutrients 13, no. 12: 4319. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13124319