
The Beneficial Effects of Astaxanthin on Glucose Metabolism and Modified Low-Density Lipoprotein in Healthy Volunteers and Subjects with Prediabetes

Abstract
:1. Introduction
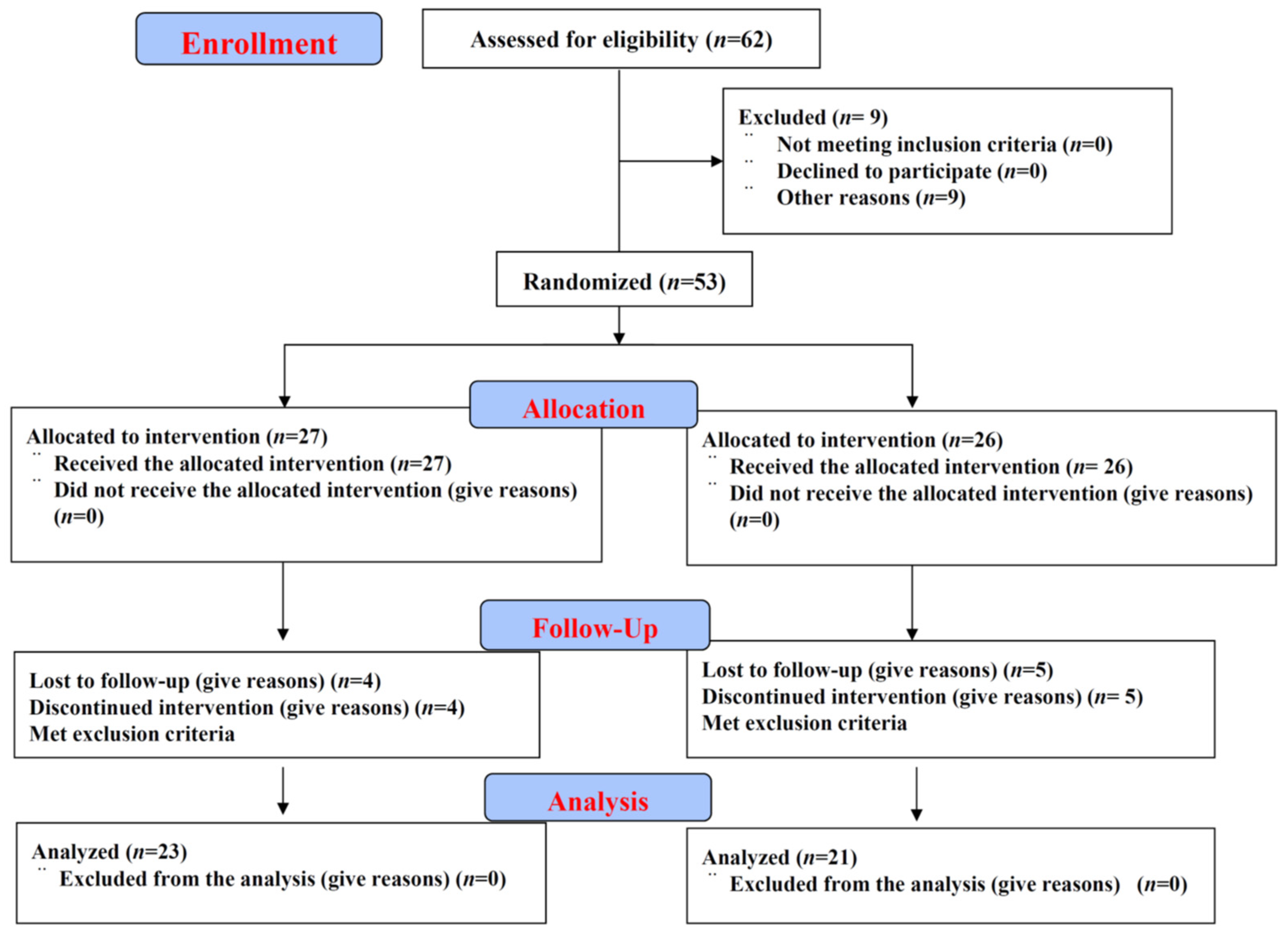
2. Participants and Methods
2.1. Study Population
2.2. Study Protocol
2.3. Sample Processing and Data Collection
2.4. Statistical Analysis
3. Results
3.1. Baseline Anthropometric and Demographic Characteristics of the Participants
3.2. Changes in the Plasma ASTX Concentration
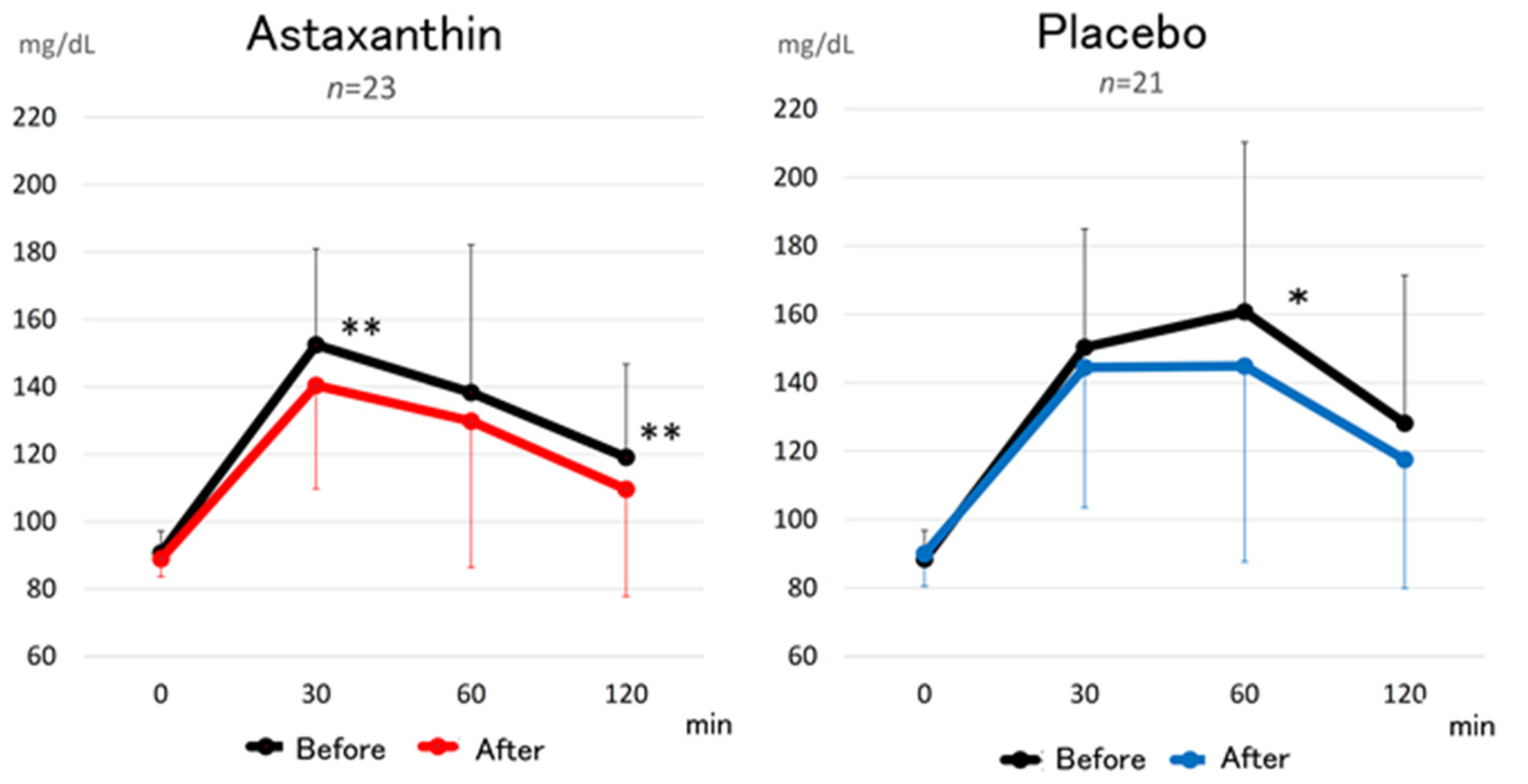
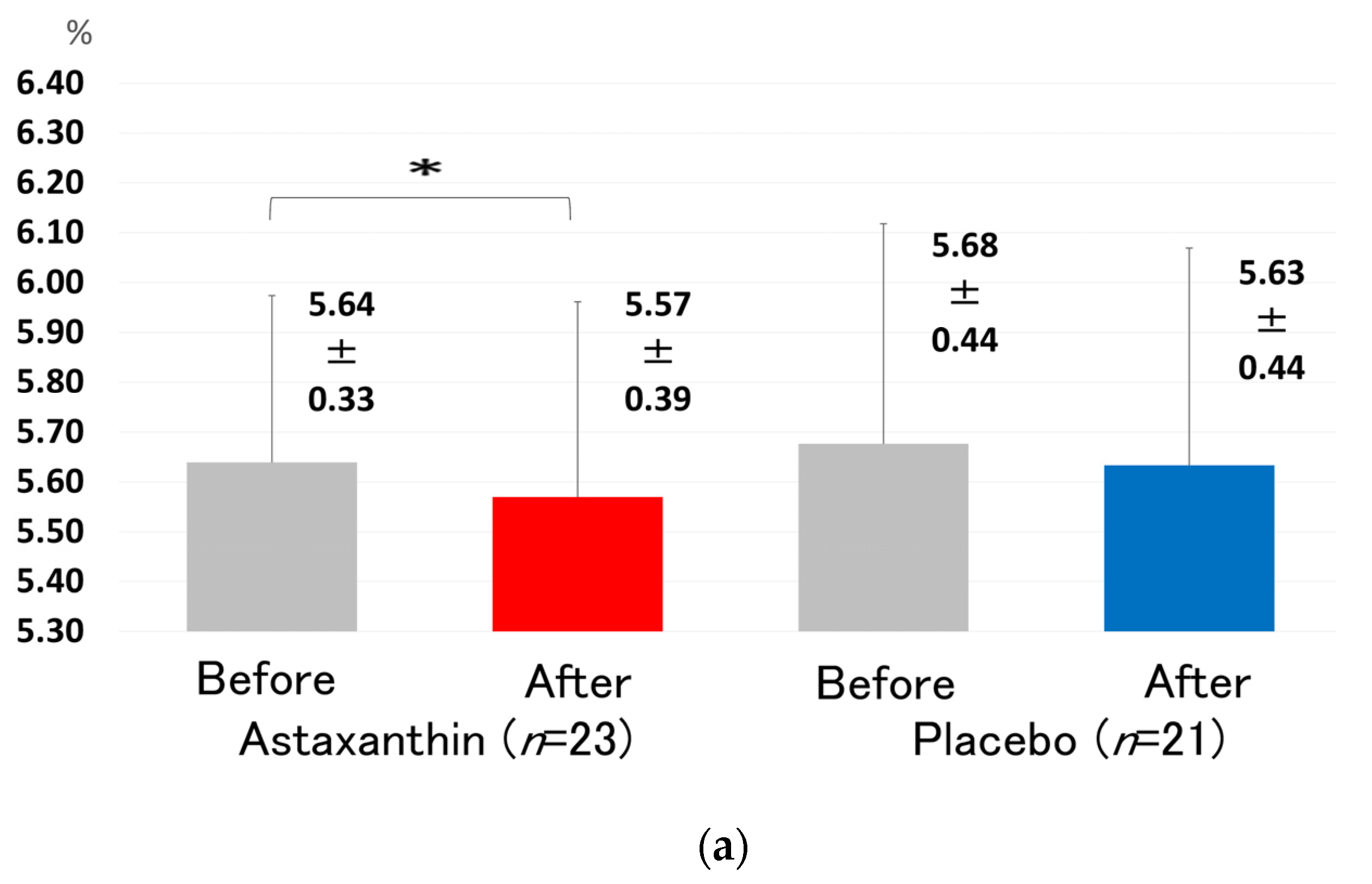
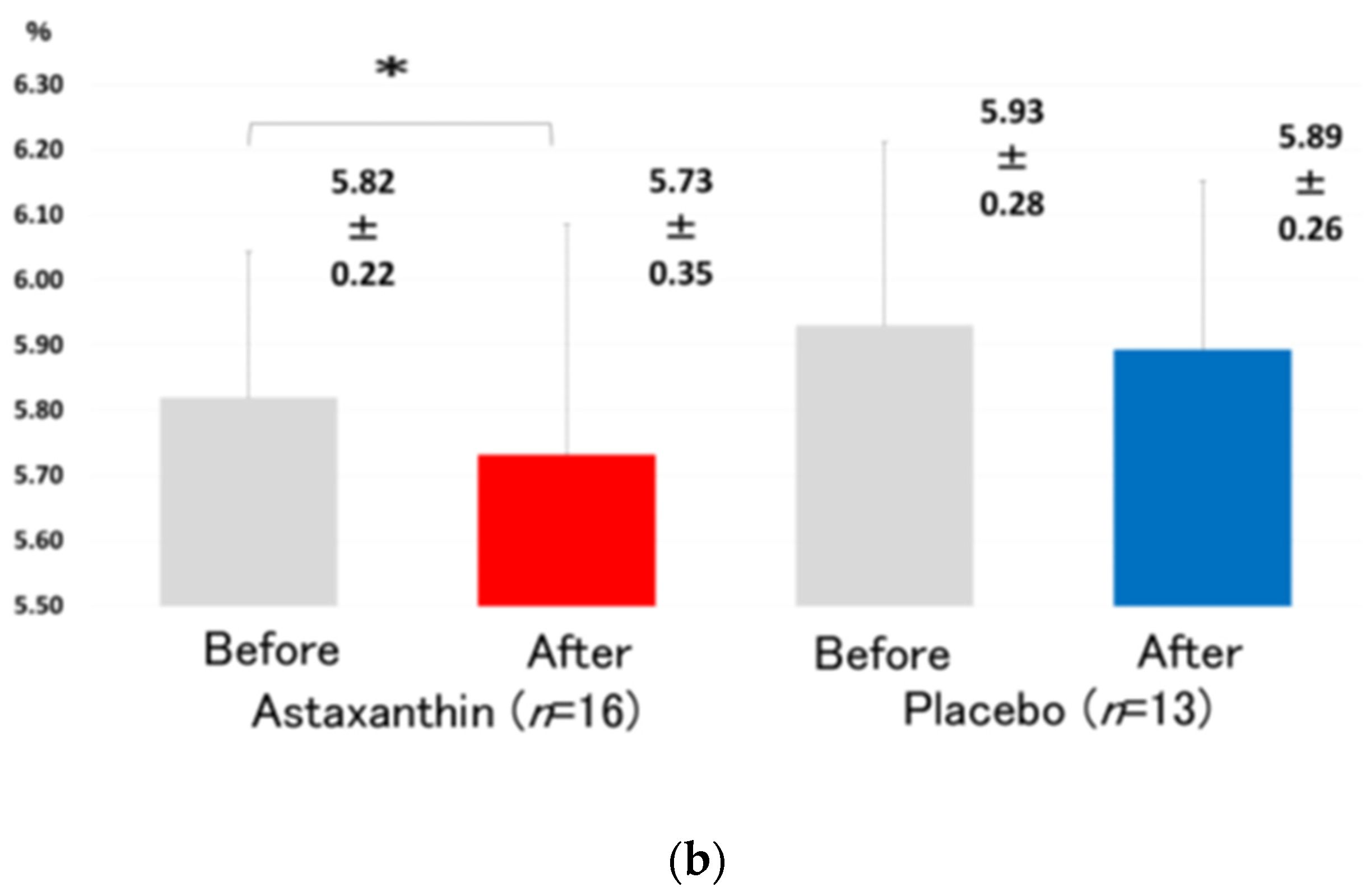
3.3. Changes in the Glucose Metabolic Parameters
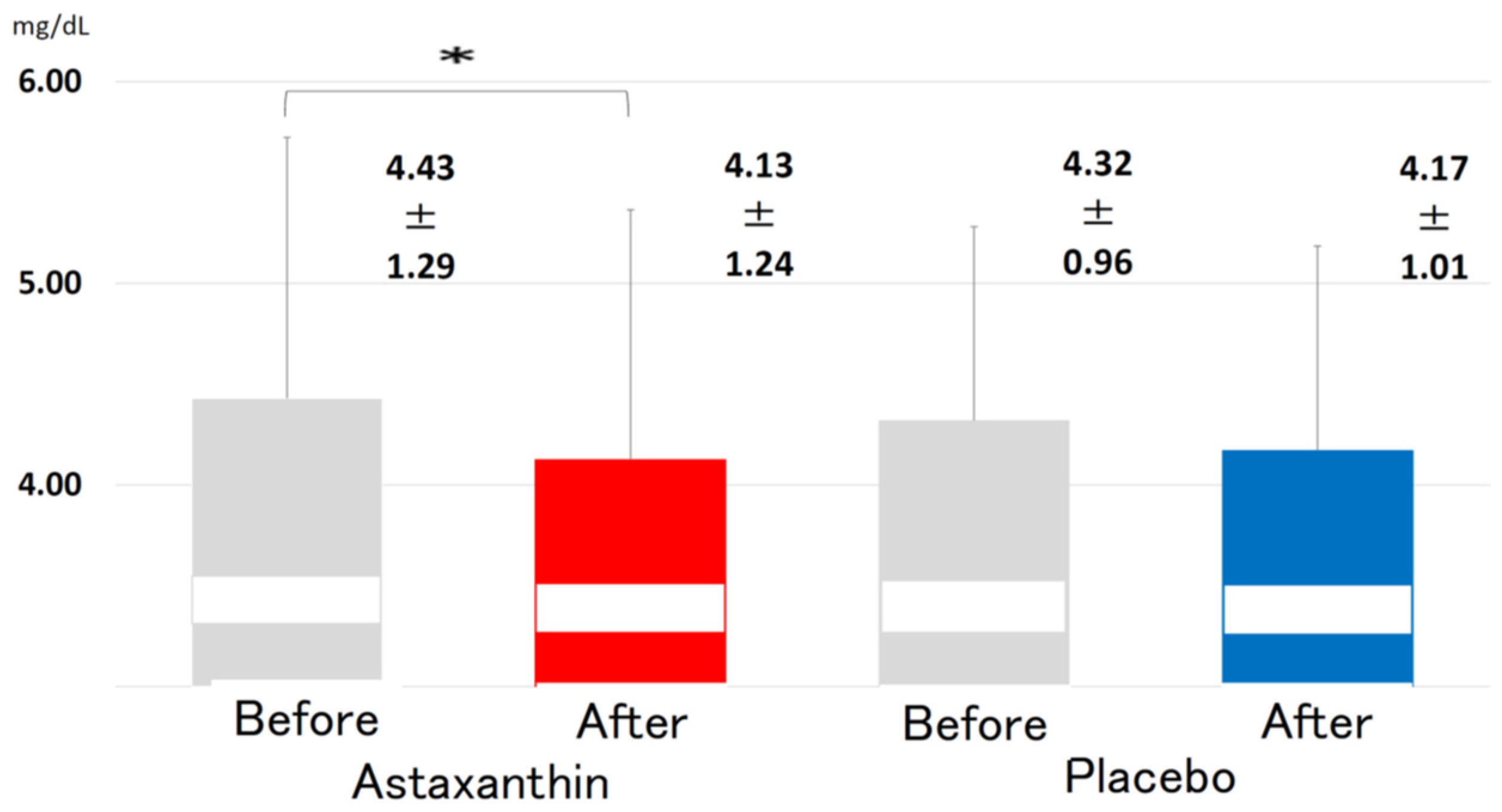
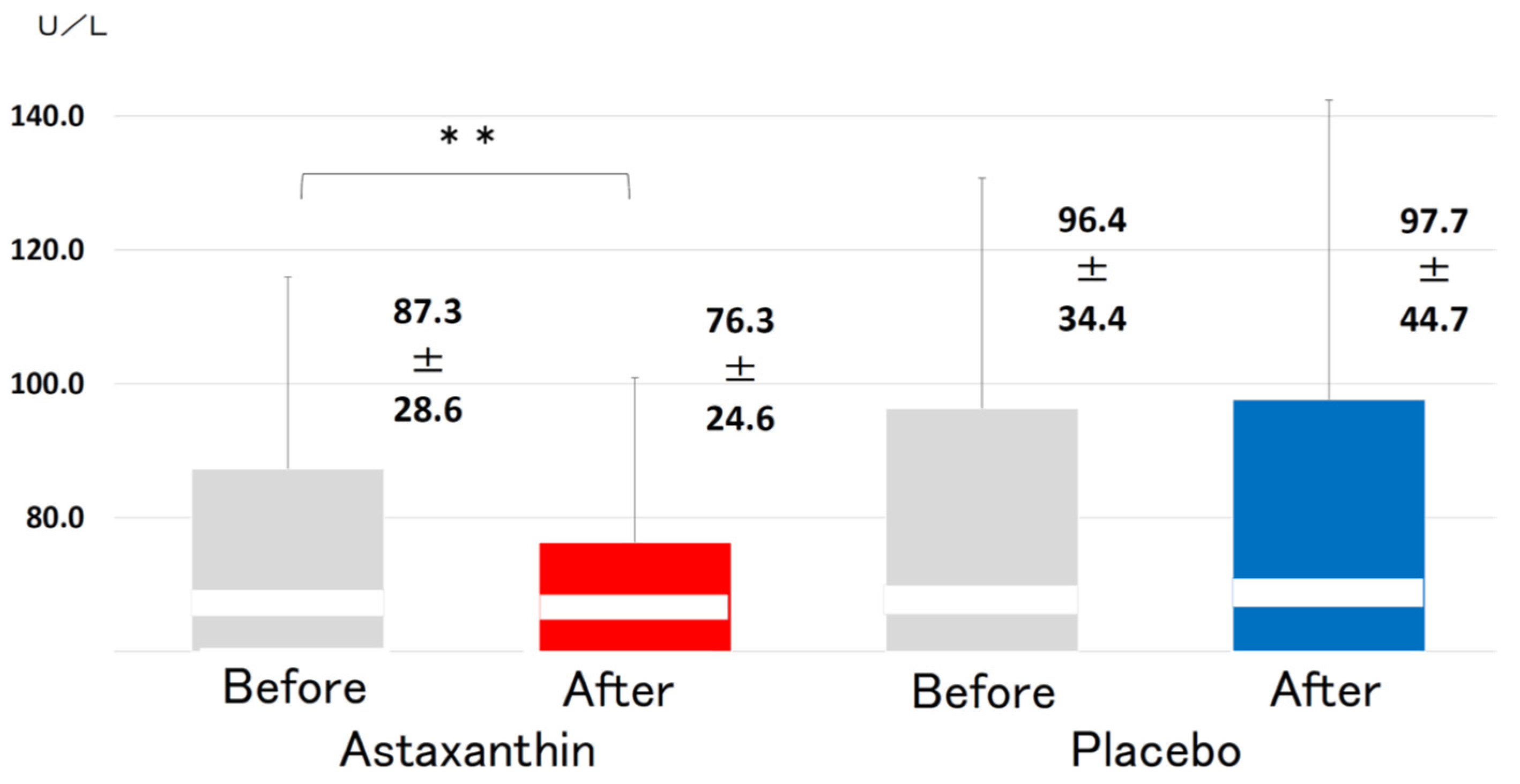
3.4. Changes in the Lipid Parameters
3.5. Changes in Other Parameters
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| ASTX | Astaxanthin |
| BIA | Bioelectrical impedance analysis |
| MDA-LDL | Malondialdehyde-modified low-density lipoprotein |
| VFA | Visceral fat area |
| 75 g | OGTT 75 g oral glucose tolerance test |
| TC | Total cholesterol |
| TG | Triglyceride |
| HDL-C | High-density lipoprotein-cholesterol |
References
- Baena-Díez, J.M.; Peñafiel, J.; Subirana, I.; Ramos, R.; Elosua, R.; Marín-Ibañez, A.; Guembe, M.J.; Rigo, F.; Tormo-Díaz, M.J.; Moreno-Iribas, C.; et al. Risk of cause specific death in individuals with diabetes: A competing risks analysis. Diabetes Care 2016, 39, 1987–1995. [Google Scholar] [CrossRef] [Green Version]
- Blas, E.; Kuru, A. Diabetes: Equity and social determinants. In Equity, Social Determinants and Public Health Programmes; World Health Organization: Geneva, Switzerland, 2010. [Google Scholar]
- Cho, N.H.; Shaw, J.E.; Karuranga, S.; Huang, Y.; da Rocha Fernandes, J.D.; Ohlrogge, A.W.; Malanda, B. IDF Diabetes Atlas: Global estimates of diabetes prevalence for 2017 and projections for 2045. Diabetes Res. Clin Pract. 2018, 138, 271–281. [Google Scholar] [CrossRef] [PubMed]
- Hurrle, S.; Hsu, W.H. The etiology of oxidative stress in insulin resistance. Biomed. J. 2017, 40, 257–262. [Google Scholar] [CrossRef]
- Higuera-Ciapara, I.; Felix-Valenzuela, L.; Goycoolea, F.M. Astaxanthin: A review of its chemistry and applications. Crit. Rev. Food Sci. Nutr. 2006, 46, 185–196. [Google Scholar] [CrossRef]
- Miki, W. Biological functions and activities of animal carotenoids. Pure Appl. Chem. 1991, 63, 141–146. [Google Scholar] [CrossRef]
- Nishida, Y.; Yamashita, E.; Miki, W. Quenching Activities of Common Hydrophilic and Lipophilic Antioxidants against Singlet Oxygen Using Chemiluminescence Detection System. Carotenoid Sci. 2007, 11, 16–20. [Google Scholar]
- Kurashige, M.; Okimasu, E.; Inoue, M.; Utsumi, K. Inhibition of oxidative injury of biological membranes by astaxanthin. Physiol. Chem. Phys. Med NMR 1990, 22, 27–38. [Google Scholar] [PubMed]
- Guerin, M.; Huntley, M.E.; Olaizola, M. Haematococcus astaxanthin: Applications for human health and nutrition. Trends Biotechnol. 2003, 21, 210–216. [Google Scholar] [CrossRef]
- Hama, S.; Uenishi, S.; Yamada, A.; Ohgita, T.; Tsuchiya, H.; Yamashita, E.; Kogure, K. Scavenging of hydroxyl radicals in aqueous solution by astaxanthin encapsulated in liposomes. Biol. Pharm. Bull. 2012, 35, 2238–2242. [Google Scholar] [CrossRef] [Green Version]
- Kidd, P. Astaxanthin, cell membrane nutrient with diverse clinical benefits and anti-aging potential. Altern. Med. Rev. 2011, 16, 355–364. [Google Scholar]
- Kimura, M.; Iida, M.; Yamauchi, H.; Suzuki, M.; Shibasaki, T.; Saito, Y.; Saito, H. Astaxanthin supplementation effects on adipocyte size and lipid profile in OLETF rats with hyperphagia and visceral fat accumulation. J. Funct. Foods 2014, 11, 114–120. [Google Scholar] [CrossRef]
- Bhuvaneswari, S.; Anuradha, C.V. Astaxanthin prevents loss of insulin signaling and improves glucose metabolism in liver of insulin resistant mice. Can. J. Physiol. Pharmacol. 2012, 90, 1544–1552. [Google Scholar] [CrossRef] [PubMed]
- Yoshida, H.; Yanai, H.; Ito, K.; Tomono, Y.; Koikeda, T.; Tsukahara, H.; Tada, N. Administration of natural astaxanthin increases serum HDL-cholesterol and adiponectin in subjects with mild hyperlipidemia. Atherosclerosis 2010, 209, 520–523. [Google Scholar] [CrossRef]
- Monroy-Ruiz, J.; Sevilla, M.-Á.; Carrón, R.; Montero, M.-J. Astaxanthin-enriched-diet reduces blood pressure and improves cardiovascular parameters in spontaneously hypertensive rats. Pharmacol. Res. 2011, 63, 44–50. [Google Scholar] [CrossRef]
- Yang, Y.; Seo, J.M.; Nguyen, A.; Pham, T.X.; Park, H.J.; Park, Y.; Kim, B.; Bruno, R.S.; Lee, J. Astaxanthin-rich extract from the green alga Haematococcus pluvialis lowers plasma lipid concentrations and enhances antioxidant defense in apolipoprotein E knockout mice. J. Nutr. 2011, 141, 1611–1617. [Google Scholar] [CrossRef] [Green Version]
- Satoh, A.; Tsuji, S.; Okada, Y.; Murakami, N.; Urami, M.; Nakagawa, K.; Ishikura, M.; Katagiri, M.; Koga, Y.; Shirasawa, T. Preliminary Clinical Evaluation of Toxicity and Efficacy of A New Astaxanthin-rich Haematococcus pluvialis Extract. J. Clin. Biochem. Nutr. 2009, 44, 280–284. [Google Scholar] [CrossRef] [Green Version]
- Ambati, R.R.; Phang, S.-M.; Ravi, S.; Aswathanarayana, R.G. Astaxanthin: Sources, extraction, stability, biological activities and its commercial applications—A review. Mar. Drugs 2014, 12, 128–152. [Google Scholar] [CrossRef]
- Bonetti, P.O.; Barsness, G.W.; Keelan, P.C.; Schnell, T.I.; Pumper, G.M.; Kuvin, J.T.; Schnall, R.P.; Holmes, D.R.; Higano, S.T.; Lerman, A. Enhanced external counter-pulsation improves endothelial function in patients with symptomatic coronary artery disease. J. Am. Coll. Cardiol. 2003, 41, 1761–1768. [Google Scholar] [CrossRef] [Green Version]
- Hamburg, N.M.; Benjamin, E.J. Assessment of Endothelial Function Using Digital Pulse Amplitude Tonometry. Trends Cardiovasc. Med. 2009, 19, 6–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ursoniu, S.; Sahebkar, A.; Serban, M.-C.; Banach, M. Lipid profile and glucose changes after supplementation with astaxanthin: A systematic review and meta-analysis of randomized controlled trials. Arch. Med. Sci. 2015, 11, 253–266. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Uchiyama, K.; Naito, Y.; Hasegawa, G.; Nakamura, N.; Takahashi, J.; Yoshikawa, T. Astaxanthin protects beta-cells against glucose toxicity in diabetic db/db mice. Redox Rep. 2002, 7, 290–293. [Google Scholar] [CrossRef] [PubMed]
- Ishiki, M.; Nishida, Y.; Ishibashi, H.; Wada, T.; Fujisaka, S.; Takikawa, A.; Urakaze, M.; Sasaoka, T.; Usui, I.; Tobe, K. Impact of divergent effects of astaxanthin on insulin signaling in L6 cells. Endocrinology 2013, 154, 2600–2612. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mashhadi, N.S.; Zakerkish, M.; Mohammadiasl, J.; Zarei, M.; Mohammadshahi, M.; Haghighizadeh, M.H. Astaxanthin improves glucose metabolism and reduces blood pressure in patients with type 2 diabetes mellitus. Asia Pac. J. Clin. Nutr. 2018, 27, 341–346. [Google Scholar]
- Iwamoto, T.; Hosoda, K.; Hirano, R.; Kurata, H.; Matsumoto, A.; Miki, W.; Kamiyama, M.; Itakura, H.; Yamamoto, S.; Kondo, K. Inhibition of Low-Density Lipoprotein Oxidation by Astaxanthin. J. Atheroscler. Thromb. 2000, 7, 216–222. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, X.J.; Tian, D.C.; Wang, F.W.; Zhang, M.-H.; Fan, C.-D.; Chen, W.; Wang, M.-H.; Fu, X.-Y.; Ma, J.-K. ASTX inhibits homocysteine-induced endothelial cell dysfunction via the regulation of the reactive oxygen species-dependent VEGF-VEGFR2-FAK signaling pathway. Mol. Med. Rep. 2019, 19, 4753–4760. [Google Scholar]
- Zhao, Z.-W.; Cai, W.; Lin, Y.-L.; Lin, Q.-F.; Jiang, Q.; Lin, Z.; Chen, L.-L. Ameliorative effect of astaxanthin on endothelial dysfunction in streptozotocin-induced diabetes in male rats. Drug Res. 2011, 61, 239–246. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Astaxanthin n = 23 (Male: 8 Female: 15) | Placebo n = 21 (Male: 7 Female: 14) | ||
|---|---|---|---|
| Age (years) | 46.2 ± 13.7 | 48.2 ± 12.0 | n.s. |
| BMI | 21.0 ± 2.0 | 23.9 ± 5.4 | n.s. |
| Systolic BP (mmHg) | 110.1 ± 18.9 | 117.9 ± 15.6 | n.s. |
| Diastolic BP (mmHg) | 68.3 ± 13.8 | 71.8 ± 9.6 | n.s. |
| Pulse Rate | 71.1 ± 7.7 | 72.6 ± 9.6 | n.s. |
| Waist Circumference (cm) | 77.1 ± 7.4 | 85.3 ± 12.6 | * |
| Subjects with prediabetes (n) (HbA1c 5.6~6.4) | 16 | 13 |
| Astaxanthin (n = 23) | Placebo (n = 21) | |||||||
|---|---|---|---|---|---|---|---|---|
| Before | After | Before | After | |||||
| Mean | SD | Mean | SD | Mean | SD | Mean | SD | |
| TC (mg/dL) | 199.4 | 25.8 | 200.3 | 30.4 | 213.9 | 44.5 | 214.5 | 40.3 |
| TG (mg/dL) | 84.9 | 39.0 | 90.3 | 53.7 | 95.3 | 51.8 | 108.8 | 77.5 |
| HDL-C (mg/dL) | 64.0 | 14.3 | 64.7 | 15.3 | 59.4 | 12.3 | 57.0 | 11.3 |
| LDL-C (mg/dL) (Friedewalde) | 118.5 | 22.1 | 117.5 | 24.2 | 135.5 | 37.4 | 135.8 | 36.4 |
| non HDL-C (mg/dL) | 135.5 | 23.7 | 135.6 | 26.6 | 154.4 | 42.8 | 157.5 | 41.7 |
| MDA-LDL (U/L) | 87.3 | 28.6 | 76.3 ** | 24.6 | 96.4 | 34.4 | 97.7 | 44.7 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Urakaze, M.; Kobashi, C.; Satou, Y.; Shigeta, K.; Toshima, M.; Takagi, M.; Takahashi, J.; Nishida, H. The Beneficial Effects of Astaxanthin on Glucose Metabolism and Modified Low-Density Lipoprotein in Healthy Volunteers and Subjects with Prediabetes. Nutrients 2021, 13, 4381. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13124381
Urakaze M, Kobashi C, Satou Y, Shigeta K, Toshima M, Takagi M, Takahashi J, Nishida H. The Beneficial Effects of Astaxanthin on Glucose Metabolism and Modified Low-Density Lipoprotein in Healthy Volunteers and Subjects with Prediabetes. Nutrients. 2021; 13(12):4381. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13124381
Chicago/Turabian StyleUrakaze, Masaharu, Chikaaki Kobashi, Yukihiro Satou, Kouichi Shigeta, Masahiro Toshima, Masatoshi Takagi, Jiro Takahashi, and Hiroshi Nishida. 2021. "The Beneficial Effects of Astaxanthin on Glucose Metabolism and Modified Low-Density Lipoprotein in Healthy Volunteers and Subjects with Prediabetes" Nutrients 13, no. 12: 4381. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13124381