Associations of Dietary Intake on Biological Markers of Inflammation in Children and Adolescents: A Systematic Review

 , , , ,
, , , ,
Abstract
:1. Introduction
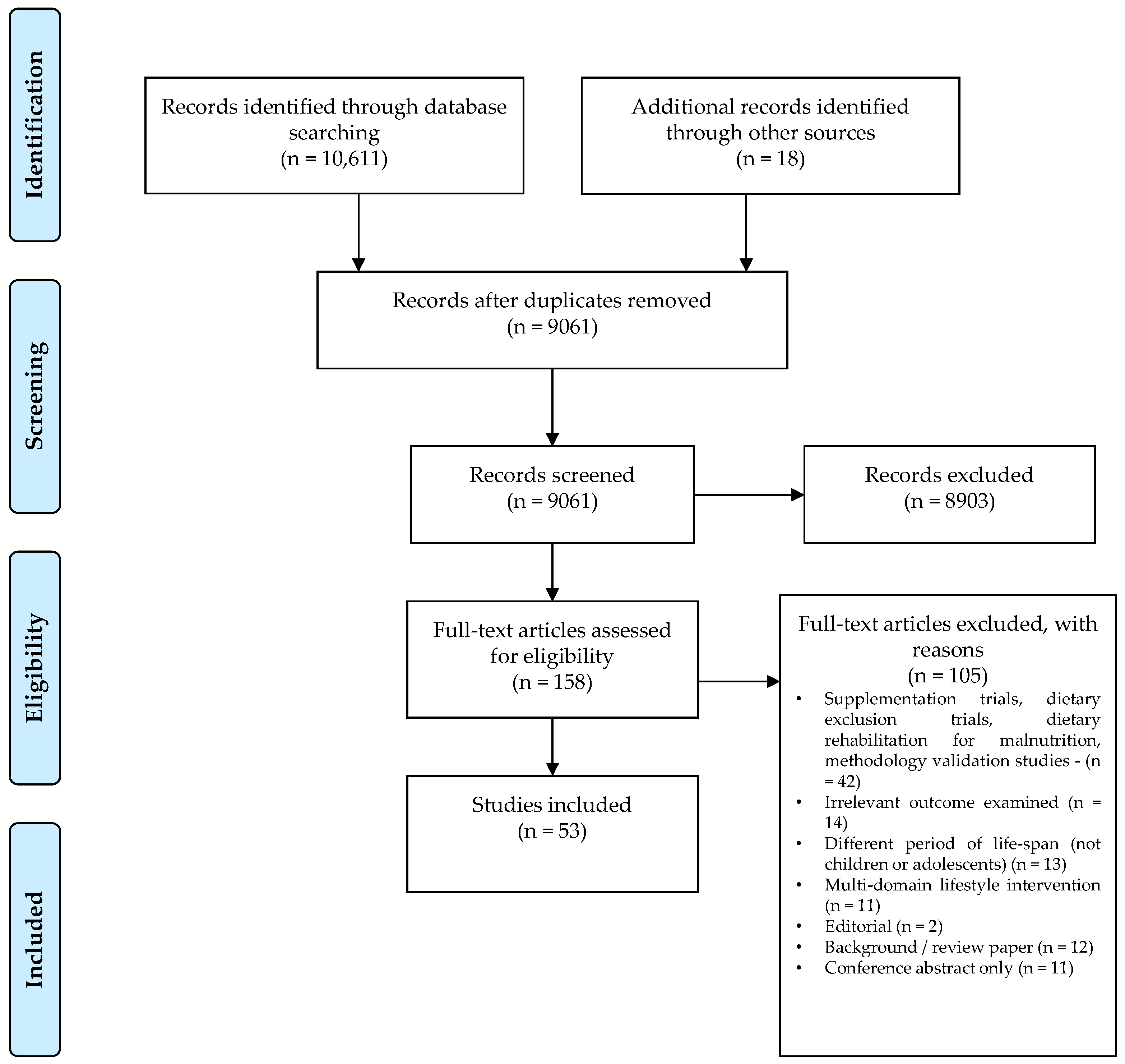
2. Materials and Methods
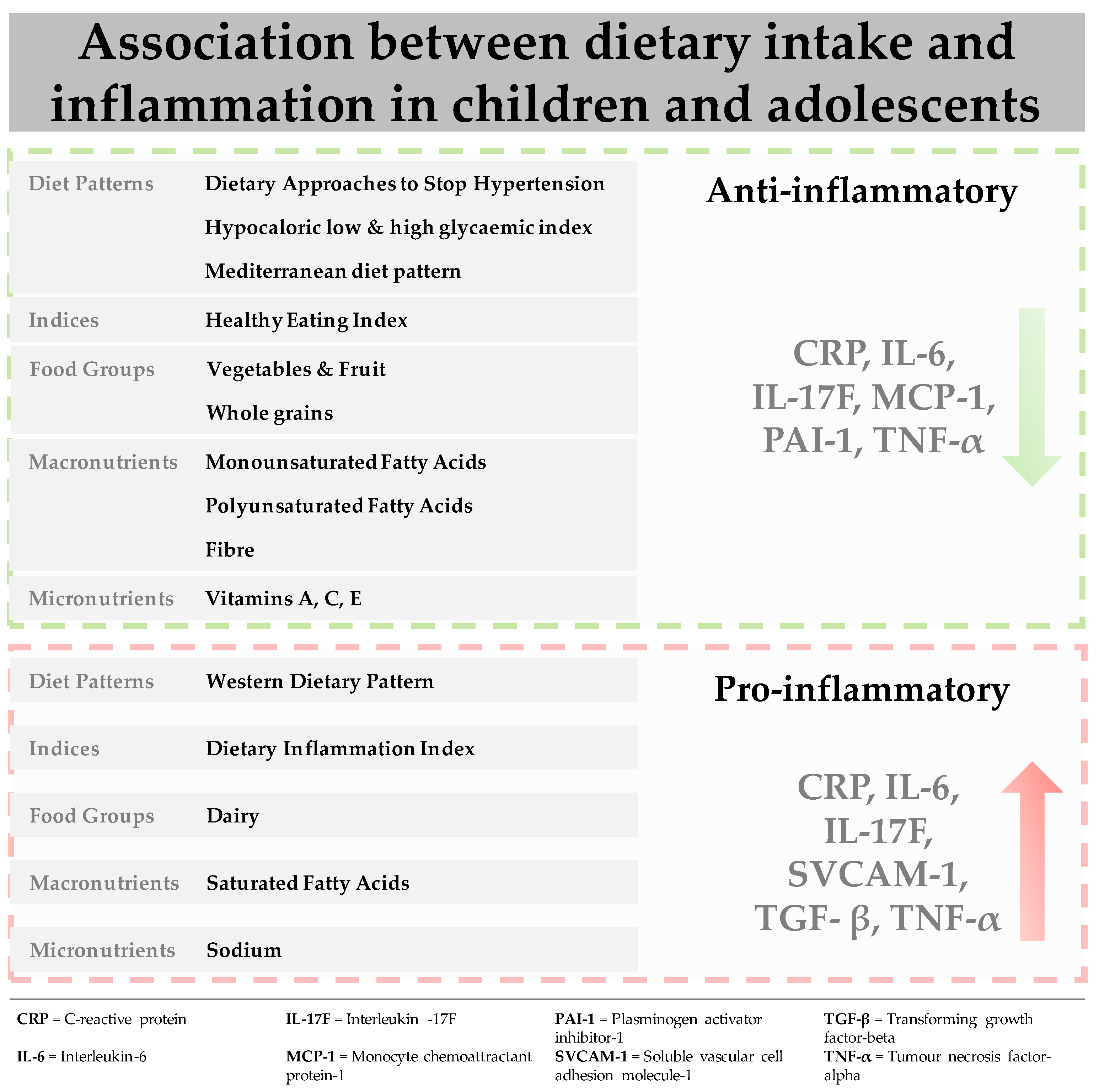
3. Results
3.1. Dietary Patterns
3.1.1. DASH Dietary Pattern
3.1.2. Low and High Glycaemic Index Dietary Pattern
3.1.3. Mediterranean Dietary Pattern
3.1.4. Western Dietary Pattern (WDP)
3.2. Indices
3.2.1. Dietary Inflammatory Index (DII)
3.2.2. Healthy Eating Index (HEI)
3.2.3. Diet Quality Index (DQI)
3.3. Food Groups
3.3.1. Vegetables and Fruits
3.3.2. Dairy
3.3.3. Meat, Seafood and Eggs
3.3.4. Whole and Refined Grains
3.3.5. Added Sugar and Sugar Sweetened Beverages (SSB)
3.4. Macronutrients
3.4.1. Fats
3.4.2. Fibre
3.5. Micronutrients
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Calder, P.C.; Ahluwalia, N.; Brouns, F.; Buetler, T.; Clement, K.; Cunningham, K.; Esposito, K.; Jö Nsson, L.S.; Kolb, H.; Lansink, M.; et al. Dietary factors and low-grade inflammation in relation to overweight and obesity commissioned by the ILSI Europe Metabolic Syndrome and Diabetes Task Force. Br. J. Nutr. 2011, 106, S1–S78. [Google Scholar] [CrossRef]
- Minihane, A.M.; Vinoy, S.; McArdle, H.J.; Kremer, B.H.A.; Sterkman, L.; Vafeiadou, K.; Benedetti, M.M.; Williams, C.M.; Calder, P.C.; Russell, W.R.; et al. Low-grade inflammation, diet composition and health: Current research evidence and its translation. Br. J. Nutr. 2015, 114, 999–1012. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Giacobbe, J.; Benoiton, B.; Zunszain, P.; Pariante, C.M.; Borsini, A. The Anti-Inflammatory Role of Omega-3 Polyunsaturated Fatty Acids Metabolites in Pre-Clinical Models of Psychiatric, Neurodegenerative, and Neurological Disorders. Front. Psychiatry 2020, 11. [Google Scholar] [CrossRef]
- Kiecolt-Glaser, J.K.; Derry, H.M.; Fagundes, C.P. Inflammation: Depression Fans the Flames and Feasts on the Heat. Am. J. Psychiatry 2015, 172, 1075–1091. [Google Scholar] [CrossRef]
- Zunszain, P.A.; Hepgul, N.; Pariante, C.M. Inflammation and Depression. Behavioral Neurobiology of Depression and its Treatment. Springer: Berlin, Germany, 2012; pp. 135–151. [Google Scholar]
- Sawyer, K.M.; Zunszain, P.A.; Dazzan, P.; Pariante, C.M. Intergenerational transmission of depression: Clinical observations and molecular mechanisms. Mol. Psychiatry 2019, 24, 1157–1177. [Google Scholar] [CrossRef] [Green Version]
- Cattaneo, A.; The Neuroimmunology of Mood Disorders and Alzheimer’s Disease (NIMA) Consortium; Ferrari, C.; Turner, L.; Mariani, N.; Enache, D.; Hastings, C.; Kose, M.; Lombardo, G.; McLaughlin, A.P.; et al. Whole-blood expression of inflammasome- and glucocorticoid-related mRNAs correctly separates treatment-resistant depressed patients from drug-free and responsive patients in the BIODEP study. Transl. Psychiatry 2020, 10, 1–14. [Google Scholar] [CrossRef]
- Osimo, E.F.; Cardinal, R.N.; Jones, P.B.; Khandaker, G.M. Prevalence and correlates of low-grade systemic inflammation in adult psychiatric inpatients: An electronic health record-based study. Psychoneuroendocrinology 2018, 91, 226–234. [Google Scholar] [CrossRef]
- Barbaresko, J.; Koch, M.; Schulze, M.B.; Nöthlings, U. Dietary pattern analysis and biomarkers of low-grade inflammation: A systematic literature review. Nutr. Rev. 2013, 71, 511–527. [Google Scholar] [CrossRef]
- Furman, D.; Campisi, J.; Verdin, E.; Carrera-Bastos, P.; Targ, S.; Franceschi, C.; Ferrucci, L.; Gilroy, D.W.; Fasano, A.; Miller, G.W.; et al. Chronic inflammation in the etiology of disease across the life span. Nat. Med. 2019, 25, 1822–1832. [Google Scholar] [CrossRef]
- Stein, D.J.; Benjet, C.; Gureje, O.; Lund, C.; Scott, K.M.; Poznyak, V.; Van Ommeren, M. Integrating mental health with other non-communicable diseases. BMJ 2019, 364, l295. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bennett, J.M.; Reeves, G.; Billman, G.E.; Sturmberg, J.P. Inflammation–Nature’s way to efficiently respond to all types of challenges: Implications for understanding and managing “the epidemic” of chronic diseases. Front. Med. 2018, 5, 316. [Google Scholar] [CrossRef] [Green Version]
- Singh, J.; Merrill, E.D.; Sandesara, P.B.; Schoeneberg, L.; Dai, H.; Raghuveer, G. Vitamin D, low-grade inflammation and cardio-vascular risk in young children: A pilot study. Pediatr. Cardiol. 2015, 36, 1338–1343. [Google Scholar] [CrossRef]
- Amaral, G.A.; Alves, J.D.; Honorio-França, A.C.; Fagundes, D.L.; Araujo, G.G.; Lobato, N.S.; Lima, V.V.; Giachini, F.R. Interleukin 1-beta is Linked to Chronic Low-Grade Inflammation and Cardiovascular Risk Factors in Overweight Adolescents. Endocr. Metab. Immune Disord. Drug Targets 2020, 20, 887–894. [Google Scholar] [CrossRef]
- Al-Hamad, D.; Raman, V. Metabolic syndrome in children and adolescents. Transl. Pediatr. 2017, 6, 397–407. [Google Scholar] [CrossRef] [Green Version]
- Reinehr, T. Inflammatory markers in children and adolescents with type 2 diabetes mellitus. Clin. Chim. Acta 2019, 496, 100–107. [Google Scholar] [CrossRef]
- Stroescu, R.F.; Mărginean, O.; Bizerea, T.; Gafencu, M.; Voicu, A.; Doroș, G. Adiponectin, leptin and high sensitivity C-reactive protein values in obese children—Important markers for metabolic syndrome? J. Pediatr. Endocrinol. Metab. 2019, 32, 27–31. [Google Scholar] [CrossRef] [PubMed]
- Marx, W.; Lane, M.; Hockey, M.; Aslam, H.; Berk, M.; Walder, K.; Borsini, A.; Firth, J.; Pariante, C.M.; Berding, K.; et al. Diet and depression: Exploring the biological mechanisms of action. Mol. Psychiatry 2020, 2020, 1–17. [Google Scholar] [CrossRef]
- Berk, M.; Williams, L.J.; Jacka, F.N.; O’Neil, A.; Pasco, J.A.; Moylan, S.; Allen, N.B.; Stuart, A.L.; Hayley, A.C.; Byrne, M.L.; et al. So depression is an inflammatory disease, but where does the inflammation come from? BMC Med. 2013, 11, 200. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grosso, G.; Mistretta, A.; Frigiola, A.; Gruttadauria, S.; Biondi, A.; Basile, F.; Vitaglione, P.; D’Orazio, N.; Galvano, F. Mediterranean Diet and Cardiovascular Risk Factors: A Systematic Review. Crit. Rev. Food Sci. Nutr. 2013, 54, 593–610. [Google Scholar] [CrossRef]
- Silveira, B.K.S.; Oliveira, T.M.S.; Andrade, P.A.; Hermsdorff, H.H.M.; Rosa, C.d.O.B.; Franceschini, S.d.C.C. Dietary Pattern and Macro-nutrients Profile on the Variation of Inflammatory Biomarkers: Scientific Update. Cardiol. Res. Pract. 2018, 1–18. [Google Scholar]
- Sun, C.-H.; Li, Y.; Zhang, Y.; Zhou, X.-L.; Wang, F. The effect of vitamin–mineral supplementation on CRP and IL-6: A systemic review and meta-analysis of randomised controlled trials. Nutr. Metab. Cardiovasc. Dis. 2011, 21, 576–583. [Google Scholar] [CrossRef]
- Esposito, K.; Marfella, R.; Ciotola, M.; Di Palo, C.; Giugliano, F.; Giugliano, G.; D’Armiento, M.; D’Andrea, F.; Giugliano, D. Effect of a Mediterranean-style diet on endothelial dysfunction and markers of vascular inflammation in the metabolic syndrome: A randomized trial. J. Am. Med Assoc. 2004, 292, 1440–1446. [Google Scholar] [CrossRef] [Green Version]
- Giugliano, D.; Ceriello, A.; Esposito, K. The effects of diet on inflammation: Emphasis on the metabolic syndrome. J. Am. Coll. Cardiol. 2006, 48, 677–685. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kohlboeck, G.; Sausenthaler, S.; Standl, M.; Koletzko, S.; Bauer, C.P.; Von Berg, A.; Berdel, D.; Krämer, U.; Schaaf, B.; Lehmann, I.; et al. Food Intake, Diet Quality and Behavioral Problems in Children: Results from the GINI-plus/LISA-plus Studies. Ann. Nutr. Metab. 2012, 60, 247–256. [Google Scholar] [CrossRef] [Green Version]
- Jacka, F.N.; Kremer, P.J.; Berk, M.; De Silva-Sanigorski, A.M.; Moodie, M.; Leslie, E.R.; Pasco, J.A.; Swinburn, B.A. A Prospective Study of Diet Quality and Mental Health in Adolescents. PLoS ONE 2011, 6, e24805. [Google Scholar] [CrossRef] [PubMed]
- Jacka, F.N.; Kremer, P.; Leslie, E.; Berk, M.; Patton, G.; Toumbourou, J.W.; Williams, J.W. Associations Between Diet Quality and Depressed Mood in Adolescents: Results from the Australian Healthy Neighbourhoods Study. Aust. N. Z. J. Psychiatry 2010, 44, 435–442. [Google Scholar] [CrossRef]
- Van der Velde, L.A.; Nguyen, A.N.; Schoufour, J.D.; Geelen, A.; Jaddoe, V.W.; Franco, O.H.; Voortman, T. Diet quality in childhood: The Generation R Study. Eur. J. Nutr. 2019, 58, 1259–1269. [Google Scholar] [CrossRef] [Green Version]
- Lassale, C.; Batty, G.D.; Baghdadli, A.; Jacka, F.; Sánchez-Villegas, A.; Kivimäki, M.; Akbaraly, T. Healthy dietary indices and risk of depressive outcomes: A systematic review and meta-analysis of observational studies. Mol. Psychiatry 2019, 24, 965–986. [Google Scholar] [CrossRef] [Green Version]
- Saugo, E.; Lasalvia, A.; Bonetto, C.; Cristofalo, D.; Poli, S.; Bissoli, S.; Bertani, M.; Lazzarotto, L.; Gardellin, F.; Ceccato, E.; et al. Dietary habits and physical activity in first-episode psychosis patients treated in community services. Effect on early anthropometric and cardio-metabolic alterations. Schizophr. Res. 2020, 216, 374–381. [Google Scholar] [CrossRef]
- Hilger-Kolb, J.; Bosle, C.; Motoc, I.; Hoffmann, K. Associations between dietary factors and obesity-related biomarkers in healthy children and adolescents—A systematic review. Nutr. J. 2017, 16, 1–12. [Google Scholar] [CrossRef] [Green Version]
- Suhett, L.G.; Hermsdorff, H.H.M.; Cota, B.C.; Ribeiro, S.A.V.; Shivappa, N.; Hebert, J.R.; Franceschini, S.; De Novaes, J.F. Dietary inflammatory potential, cardiometabolic risk and inflammation in children and adolescents: A systematic review. Crit. Rev. Food Sci. Nutr. 2021, 61, 407–416. [Google Scholar] [CrossRef]
- Rocha, N.P.; Milagres, L.C.; Longo, G.Z.; Ribeiro, A.Q.; Novaes, J.F.d. Association between dietary pattern and cardiometabolic risk in children and adolescents: A systematic review. J. Pediatr. 2017, 93, 214–222. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. Int. J. Surg. 2010, 8, 336–341. [Google Scholar] [CrossRef] [Green Version]
- Von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P. The Strengthening the Reporting of Observa-tional Studies in Epidemiology (STROBE) statement: Guidelines for reporting observational studies. Ann. Intern Med. 2007, 147, 573–577. [Google Scholar] [CrossRef] [Green Version]
- Higgins, J.P.; Green, S. Cochrane Handbook for Systematic Reviews of Interventions; John Wiley & Sons: Hoboken, NJ, USA, 2011. [Google Scholar]
- Oddy, W.H.; Allen, K.L.; Trapp, G.S.; Ambrosini, G.L.; Black, L.J.; Huang, R.-C.; Rzehak, P.; Runions, K.C.; Pan, F.; Beilin, L.J.; et al. Dietary patterns, body mass index and inflammation: Pathways to depression and mental health problems in adolescents. Brain Behav. Immun. 2018, 69, 428–439. [Google Scholar] [CrossRef] [Green Version]
- Sen, S.; Rifas-Shiman, S.L.; Shivappa, N.; Wirth, M.D.; Hebert, J.R.; Gold, D.R.; Gillman, M.W.; Oken, E. Associations of prenatal and early life dietary inflammatory potential with childhood adiposity and cardiometabolic risk in Project Viva. Pediatr. Obes. 2017, 13, 292–300. [Google Scholar] [CrossRef]
- Del Mar Bibiloni, M.; Maffeis, C.; Llompart, I.; Pons, A.; Tur, J.A. Dietary factors associated with subclinical inflammation among girls. Eur. J. Clin. Nutr. 2013, 67, 1264–1270. [Google Scholar] [CrossRef]
- Liese, A.D.; Ma, X.; Ma, X.; Mittleman, M.A.; Catherine, P.; Standiford, D.A.; Lawrence, J.M.; Pihoker, C.; Marcovina, S.M.; Mayer-Davis, E.J.; et al. Dietary quality and markers of inflammation: No association in youth with type 1 diabetes. J. Diabetes Its Complicat. 2018, 32, 179–184. [Google Scholar] [CrossRef] [PubMed]
- Saneei, P.; Hashemipour, M.; Kelishadi, R.; Esmaillzadeh, A. The Dietary Approaches to Stop Hypertension (DASH) Diet Affects Inflammation in Childhood Metabolic Syndrome: A Randomized Cross-Over Clinical Trial. Ann. Nutr. Metab. 2014, 64, 20–27. [Google Scholar] [CrossRef] [PubMed]
- Damsgaard, C.T.; Papadaki, A.; Jensen, S.M.; Ritz, C.; Dalskov, S.-M.; Hlavaty, P.; Saris, W.; Martínez, J.A.; Handjieva-Darlenska, T.; Andersen, M.R.; et al. Higher Protein Diets Consumed Ad Libitum Improve Cardiovascular Risk Markers in Children of Overweight Parents from Eight European Countries. J. Nutr. 2013, 143, 810–817. [Google Scholar] [CrossRef] [Green Version]
- Iannuzzi, A.; Licenziati, M.R.; Vacca, M.; De Marco, D.; Cinquegrana, G.; Laccetti, M.; Bresciani, A.; Covetti, G.; Iannuzzo, G.; Rubba, P.; et al. Comparison of two diets of varying glycemic index on carotid subclinical atherosclerosis in obese children. Hear. Vessel. 2009, 24, 419–424. [Google Scholar] [CrossRef]
- Parillo, M.; Licenziati, M.R.; Vacca, M.; De Marco, D.; Iannuzzi, A. Metabolic changes after a hypocaloric, low-glycemic-index diet in obese children. J. Endocrinol. Investig. 2011, 35, 629–633. [Google Scholar]
- Rouhani, M.H.; Kelishadi, R.; Hashemipour, M.; Esmaillzadeh, A.; Surkan, P.J.; Keshavarz, A.; Azadbakht, L. The Impact of a Low Glycemic Index Diet on Inflammatory Markers and Serum Adiponectin Concentration in Adolescent Overweight and Obese Girls: A Randomized Clinical Trial. Horm. Metab. Res. 2016, 48, 251–256. [Google Scholar] [CrossRef] [PubMed]
- Agostinis-Sobrinho, C.; Ramírez-Vélez, R.; García-Hermoso, A.; Rosário, R.; Moreira, C.; Lopes, L.; Martinkenas, A.; Mota, J.; Santos, R. The combined association of adherence to Mediterranean diet, muscular and cardiorespiratory fitness on low-grade inflammation in adolescents: A pooled analysis. Eur. J. Nutr. 2018, 58, 2649–2656. [Google Scholar] [CrossRef] [PubMed]
- Arouca, A.; Michels, N.; Moreno, L.A.; González-Gil, E.M.; Marcos, A.; Gómez, S.; Díaz, L.E.; Widhalm, K.; Molnár, D.; Manios, Y. Asso-ciations between a Mediterranean diet pattern and inflammatory biomarkers in European adolescents. Eur. J. Nutr. 2018, 57, 1747–1760. [Google Scholar] [CrossRef]
- De Carvalho, K.M.B.; Ronca, D.B.; Michels, N.; Huybrechts, I.; Cuenca-García, M.; Marcos, A.; Molnar, D.; Dallongeville, J.; Manios, Y.; Schaan, B.; et al. Does the Mediterranean Diet Protect against Stress-Induced Inflammatory Activation in European Adolescents? The HELENA Study. Nutrients 2018, 10, 1770. [Google Scholar] [CrossRef] [Green Version]
- Douros, K.; Thanopoulou, M.-I.; Boutopoulou, B.; Papadopoulou, A.; Papadimitriou, A.; Fretzayas, A.; Priftis, K.N. Adherence to the Mediterranean diet and inflammatory markers in children with asthma. Allergol. Immunopathol. 2019, 47, 209–213. [Google Scholar] [CrossRef]
- Karampola, M.; Argiriou, A.; Hitoglou-Makedou, A. Study on dietary constituents, hs-CRP serum levels and investigation of correlation between them in excess weight adolescents. Hippokratia 2019, 23, 3. [Google Scholar]
- Lazarou, C.; Panagiotakos, D.; Chrysohoou, C.; Andronikou, C.; Matalas, A.-L. C-Reactive protein levels are associated with adiposity and a high inflammatory foods index in mountainous Cypriot children. Clin. Nutr. 2010, 29, 779–783. [Google Scholar] [CrossRef]
- Sureda, A.; Bibiloni, M.D.M.; Julibert, A.; Bouzas, C.; Argelich, E.; Llompart, I.; Pons, A.; Tur, J.A. Adherence to the Mediterranean Diet and Inflammatory Markers. Nutrients 2018, 10, 62. [Google Scholar] [CrossRef] [Green Version]
- Çağiran Yilmaz, F.; Çağiran, D.; Özçelik, A.Ö. Adolescent Obesity and Its Association with Diet Quality and Cardiovascular Risk Factors. Ecol. Food Nutr. 2019, 58, 207–218. [Google Scholar] [CrossRef] [PubMed]
- Khayyatzadeh, S.S.; Bagherniya, M.; Fazeli, M.; Khorasanchi, Z.; Bidokhti, M.S.; Ahmadinejad, M.; Khoshmohabbat, S.; Arabpour, M.; Afkhamizadeh, M.; Ferns, G.A.; et al. A Western dietary pattern is associated with elevated level of high sensitive C-reactive protein among adolescent girls. Eur. J. Clin. Investig. 2018, 48, e12897. [Google Scholar] [CrossRef] [PubMed]
- Almeida-De-Souza, J.; Santos, R.; Barros, R.; Abreu, S.; Moreira, C.; Lopes, L.; Mota, J.; Moreira, P. Dietary inflammatory index and inflammatory biomarkers in adolescents from LabMed physical activity study. Eur. J. Clin. Nutr. 2017, 72, 710–719. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Coheley, L.M.; Shivappa, N.; Hebert, J.R.; Lewis, R.D. Dietary inflammatory index® and cortical bone outcomes in healthy ado-lescent children. Osteoporos. Int. 2019, 30, 1645–1654. [Google Scholar] [CrossRef] [PubMed]
- Seremet Kurklu, N.; Karatas Torun, N.; Ozen Kucukcetin, I.; Akyol, A. Is there a relationship between the dietary inflammatory index and metabolic syndrome among adolescents? J. Pediatr. Endocrinol. Metab. JPEM 2020, 33, 495–502. [Google Scholar] [CrossRef]
- Shivappa, N.; Hebert, J.R.; Marcos, A.; Diaz, L.-E.; Gomez, S.; Nova, E.; Michels, N.; Arouca, A.; González-Gil, E.; Frederic, G.; et al. As-sociation between dietary inflammatory index and inflammatory markers in the HELENA study. Mol. Nutr. Food Res. 2017, 61. [Google Scholar]
- Navarro, P.; De Dios, O.; Jois, A.; Gavela-Pérez, T.; Gorgojo, L.; Martín-Moreno, J.M.; Soriano-Guillén, L.; Garcés, C. Vegetable and Fruit Intakes Are Associated with hs-CRP Levels in Pre-Pubertal Girls. Nutrients 2017, 9, 224. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sanjeevi, N.; Lipsky, L.M.; Nansel, T.R. Cardiovascular Biomarkers in Association with Dietary Intake in a Longitudinal Study of Youth with Type 1 Diabetes. Nutrients 2018, 10, 1552. [Google Scholar] [CrossRef] [Green Version]
- Chan, S.; Ping-Delfos, W.L.; Beilin, L.J.; Oddy, W.H.; Burrows, S.; Mori, T.A. Use of the Dietary Guideline Index to assess cardi-ometabolic risk in adolescents. Br. J. Nutr. 2015, 113, 1741–1752. [Google Scholar] [CrossRef] [Green Version]
- Vyncke, K.E.; Huybrechts, I.; Dallongeville, J.; Mouratidou, T.; Van Winckel, M.A.; García, M.L.C.; Ottevaere, C.; González-Gross, M.; Moreno, L.A.; Kafatos, A.G.; et al. Intake and serum profile of fatty acids are weakly correlated with global dietary quality in European adolescents. Nutrients 2013, 29, 411–419.e3. [Google Scholar] [CrossRef] [Green Version]
- Gonzalez-Gil, E.M.; Santabárbara, J.; Russo, P.; Ahrens, W.; Claessens, M.; Lissner, L.; Börnhorst, C.; Krogh, V.; Iacoviello, L.; Molnar, D.; et al. Food intake and inflammation in European children: The IDEFICS study. Eur. J. Nutr. 2015, 55, 2459–2468. [Google Scholar] [CrossRef] [PubMed]
- Qureshi, M.M.; Singer, M.R.; Moore, L.L. A cross-sectional study of food group intake and C-reactive protein among children. Nutr. Metab. 2009, 6, 40. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hagin, S.; Lobato, D.J.; Sands, B.E.; Korzenik, J.R.; Merrick, M.; Shah, S.A.; Bancroft, B.; Bright, R.; Law, M.; Moniz, H.; et al. Dietary be-haviors in newly diagnosed youth with inflammatory bowel disease. Child Health Care. 2017, 46, 408–420. [Google Scholar] [CrossRef]
- Holt, E.M.; Steffen, L.M.; Moran, A.; Basu, S.; Steinberger, J.; Ross, J.A.; Hong, C.-P.; Sinaiko, A.R. Fruit and Vegetable Consumption and Its Relation to Markers of Inflammation and Oxidative Stress in Adolescents. J. Am. Diet. Assoc. 2009, 109, 414–421. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Han, Y.-Y.; Forno, E.; Brehm, J.M.; Acostaperez, E.; Álvarez, M.; Colón-Semidey, A.; Rivera-Soto, W.; Campos, H.; Litonjua, A.A.; Alcorn, J.F.; et al. Diet, interleukin-17, and childhood asthma in Puerto Ricans. Ann. Allergy Asthma Immunol. 2015, 115, 288–293.e1. [Google Scholar] [CrossRef] [Green Version]
- Aslam, H.; Jacka, F.N.; Marx, W.; Karatzi, K.; Mavrogianni, C.; Karaglani, E.; Mohebbi, M.; Pasco, J.A.; O’Neil, A.; Berk, M.; et al. The Associations between Dairy Product Consumption and Biomarkers of Inflammation, Adipocytokines, and Oxidative Stress in Children: A Cross-Sectional Study. Nutrients 2020, 12, 3055. [Google Scholar] [CrossRef]
- Cabral, M.; Araújo, J.; Lopes, C.; Ramos, E. Food intake and high-sensitivity C-reactive protein levels in adolescents. Nutr. Metab. Cardiovasc. Dis. 2018, 28, 1067–1074. [Google Scholar] [CrossRef]
- Aeberli, I.; Molinari, L.; Spinas, G.; Lehmann, R.; L’Allemand, D.; Zimmermann, M.B. Dietary intakes of fat and antioxidant vitamins are predictors of subclinical inflammation in overweight Swiss children. Am. J. Clin. Nutr. 2006, 84, 748–755. [Google Scholar] [CrossRef] [Green Version]
- Hajihashemi, P.; Azadbakht, L.; Hashemipor, M.; Kelishadi, R.; Esmaillzadeh, A. Whole-grain intake favorably affects markers of systemic inflammation in obese children: A randomized controlled crossover clinical trial. Mol. Nutr. Food Res. 2014, 58, 1301–1308. [Google Scholar] [CrossRef]
- Hur, I.Y.; Reicks, M. Relationship between Whole-Grain Intake, Chronic Disease Risk Indicators, and Weight Status among Adolescents in the National Health and Nutrition Examination Survey, 1999–2004. J. Acad. Nutr. Diet. 2012, 112, 46–55. [Google Scholar] [CrossRef]
- Jin, R.; Welsh, J.A.; Le, N.-A.; Holzberg, J.; Sharma, P.; Martin, D.R.; Vos, M.B. Dietary fructose reduction improves markers of cardi-ovascular disease risk in Hispanic-American adolescents with NAFLD. Nutrients 2014, 6, 3187–3201. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kosova, E.C.; Auinger, P.; Bremer, A.A. The Relationships between Sugar-Sweetened Beverage Intake and Cardiometabolic Markers in Young Children. J. Acad. Nutr. Diet. 2013, 113, 219–227. [Google Scholar] [CrossRef] [Green Version]
- Prihaningtyas, R.; Widjaja, N.; Irawan, R.; Hanindita, M.; Hidajat, B. Dietary Intakes and High Sensivity crp (hsCRP) in Adolescents with Obesity. Carpathian J. Food Sci. Technol. 2019, 11, 83–88. [Google Scholar]
- Thomas, N.-E.; Baker, J.S.; Graham, M.R.; Cooper, S.-M.; Davies, B. C-reactive protein in schoolchildren and its relation to adiposity, physical activity, aerobic fitness and habitual diet. Br. J. Sports Med. 2008, 42, 357–360. [Google Scholar] [CrossRef]
- Harris, C.; Filipiak-Pittroff, B.; Berdel, D.; Bauer, C.-P.; Schikowski, T.; Koletzko, S.; Heinrich, J.; Schulz, H.; Standl, M. Dietary saturated fat and low-grade inflammation modified by accelerometer-measured physical activity in adolescence: Results from the GINIplus and LISA birth cohorts. BMC Public Health 2019, 19, 1–11. [Google Scholar] [CrossRef]
- Arya, S.; Isharwal, S.; Misra, A.; Pandey, R.M.; Rastogi, K.; Vikram, N.; Dhingra, V.; Chatterjee, A.; Sharma, R.; Luthra, K. C-reactive protein and dietary nutrients in urban Asian Indian adolescents and young adults. Nutrition 2006, 22, 865–871. [Google Scholar] [CrossRef]
- Oldewage-Theron, W.; Kruger, R. The association between diet quality and subclinical inflammation among children aged 6–18 years in the Eastern Cape, South Africa. Public Health Nutr. 2016, 20, 102–111. [Google Scholar] [CrossRef] [Green Version]
- Au, L.E.; Economos, C.D.; Goodman, E.; Houser, R.F.; Must, A.; Chomitz, V.R.; Morgan, E.H.; Sacheck, J.M. Dietary Intake and Cardi-ometabolic Risk in Ethnically Diverse Urban Schoolchildren. J. Acad. Nutr. Diet. 2012, 112, 1815–1821. [Google Scholar] [CrossRef] [Green Version]
- Machado, A.M.; De Paula, H.; Cardoso, L.D.; Costa, N.M.B. Effects of brown and golden flaxseed on the lipid profile, glycemia, inflammatory biomarkers, blood pressure and body composition in overweight adolescents. Nutrients 2015, 31, 90–96. [Google Scholar] [CrossRef] [Green Version]
- Jaacks, L.M.; Crandell, J.; Liese, A.D.; Lamichhane, A.P.; Bell, R.A.; Dabelea, D.; D’Agostino, R.B.; Dolan, L.M.; Marcovina, S.; Reynolds, K.; et al. No association of dietary fiber intake with inflammation or arterial stiffness in youth with type 1 diabetes. J. Diabetes Its Complicat. 2014, 28, 305–310. [Google Scholar] [CrossRef] [Green Version]
- Lin, Y.; Huybrechts, I.; Vereecken, C.; Mouratidou, T.; Valtueña, J.; Kersting, M.; González-Gross, M.; Bolca, S.; Wärnberg, J.; Cuenca-García, M.; et al. Dietary fiber intake and its association with indicators of adiposity and serum biomarkers in European adolescents: The HELENA study. Eur. J. Nutr. 2014, 54, 771–782. [Google Scholar] [CrossRef] [PubMed]
- Swann, O.G.; Breslin, M.; Kilpatrick, M.; O’Sullivan, T.A.; Mori, T.A.; Beilin, L.J.; Oddy, W.H. Dietary fibre intake and its association with inflammatory markers in adolescents. Br. J. Nutr. 2021, 125, 329–336. [Google Scholar] [CrossRef]
- Parikh, S.; Pollock, N.K.; Bhagatwala, J.; Guo, D.-H.; Gutin, B.; Zhu, H.; Dong, Y. Adolescent Fiber Consumption Is Associated with Visceral Fat and Inflammatory Markers. J. Clin. Endocrinol. Metab. 2012, 97, E1451–E1457. [Google Scholar] [CrossRef] [Green Version]
- Miller, S.J.; Batra, A.K.; Shearrer, G.E.; House, B.T.; Cook, L.T.; Pont, S.J.; Goran, M.I.; Davis, J.N. Dietary fibre linked to decreased in-flammation in overweight minority youth. Pediatr. Obes. 2016, 11, 33–39. [Google Scholar] [CrossRef]
- Zhu, H.; Pollock, N.K.; Kotak, I.; Gutin, B.; Wang, X.; Bhagatwala, J.; Parikh, S.; Harshfield, G.A.; Dong, Y. Dietary Sodium, Adiposity, and Inflammation in Healthy Adolescents. Pediatrics 2014, 133, e635–e642. [Google Scholar] [CrossRef] [Green Version]
- King, D.E.; Mainous, A.G., 3rd; Geesey, M.E.; Ellis, T. Magnesium intake and serum C-reactive protein levels in children. Magnes Res. 2007, 20, 32–36. [Google Scholar]
- De Sousa, A.F.; de Andrade Mesquita, L.S.; Cruz, K.J.C.; de Oliveira, A.R.S.; Morais, J.B.S.; Severo, J.S.; Beserra, J.B.; do Nascimento Nogueira, N.; do Nascimento Marreiro, D. No Relation Between Zinc Status and Inflammatory Biomarkers in Adolescent Judokas. Int. J. Vitam. Nutr. Res. 2019. [Google Scholar]
- Zhang, R.; Chen, J.; Zheng, H.; Li, Y.; Huang, H.; Liang, Z.; Jiang, H.; Sun, J. Effects of medium chain triglycerides on body fat dis-tribution and adipocytokine levels in children with acute lymphoblastic leukemia under chemotherapy. Medicine 2019, 98, e16811. [Google Scholar] [CrossRef]
- Moeller, S.M.; Reedy, J.; Millen, A.E.; Dixon, L.B.; Newby, P.; Tucker, K.L.; Krebs-Smith, S.M.; Guenther, P.M. Dietary Patterns: Challenges and Opportunities in Dietary Patterns Research. J. Am. Diet. Assoc. 2007, 107, 1233–1239. [Google Scholar] [CrossRef] [PubMed]
- Casas, R.; Sacanella, E.; Estruch, R. The immune protective effect of the Mediterranean diet against chronic low-grade inflam-matory diseases. Endocr. Metab. Immune Disord.-Drug Targets 2014, 14, 245–254. [Google Scholar] [CrossRef] [Green Version]
- Dai, J.; Miller, A.H.; Bremner, J.D.; Goldberg, J.; Jones, L.; Shallenberger, L.; Buckham, R.; Murrah, N.V.; Veledar, E.; Wilson, P.W. Ad-herence to the Mediterranean diet is inversely associated with circulating interleukin-6 among middle-aged men: A twin study. Circulation 2008, 117, 169. [Google Scholar] [CrossRef] [Green Version]
- Davis, R.; Day, A.S.; Barrett, J.; VanLint, A.; Andrews, J.M.; Costello, S.P.; Bryant, R.V. Habitual dietary fibre and prebiotic intake is inadequate in patients with inflammatory bowel disease: Findings from a multicentre cross-sectional study. J. Hum. Nutr. Diet. 2020. [Google Scholar] [CrossRef] [PubMed]
- Chang, J.P.-C.; Su, K.-P.; Mondelli, V.; Satyanarayanan, S.K.; Yang, H.-T.; Chiang, Y.-J.; Chen, H.-T.; Pariante, C.M. High-dose eicosa-pentaenoic acid (EPA) improves attention and vigilance in children and adolescents with attention deficit hyperactivity disorder (ADHD) and low endogenous EPA levels. Transl. Psychiatry 2019, 9, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Chang, J.P.-C.; Su, K.-P.; Mondelli, V.; Pariante, C.M. Omega-3 polyunsaturated fatty acids in youths with attention deficit hyper-activity disorder: A systematic review and meta-analysis of clinical trials and biological studies. Neuropsychopharmacology 2018, 43, 534–545. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Borsini, A.; Alboni, S.; Horowitz, M.A.; Tojo, L.M.; Cannazza, G.; Su, K.-P.; Pariante, C.M.; Zunszain, P.A. Rescue of IL-1β-induced reduction of human neurogenesis by omega-3 fatty acids and antidepressants. Brain Behav. Immun. 2017, 65, 230–238. [Google Scholar] [CrossRef] [Green Version]
- Fogarty, A.; Lewis, S.A.; McKeever, T.M.; Britton, J.R. Is higher sodium intake associated with elevated systemic inflammation? A population-based study. Am. J. Clin. Nutr. 2009, 89, 1901–1904. [Google Scholar] [CrossRef]
- Sacks, F.M.; Svetkey, L.P.; Vollmer, W.M.; Appel, L.J.; Bray, G.A.; Harsha, D.; Obarzanek, E.; Conlin, P.R.; Miller, E.R.; Simons-Morton, D.G.; et al. Effects on Blood Pressure of Reduced Dietary Sodium and the Dietary Approaches to Stop Hypertension (DASH) Diet. N. Engl. J. Med. 2001, 344, 3–10. [Google Scholar] [CrossRef]
- Schultz, H.; Ying, G.-S.; Dunaief, J.L.; Dunaief, D.M. Rising Plasma Beta-Carotene Is Associated With Diminishing C-Reactive Protein in Patients Consuming a Dark Green Leafy Vegetable–Rich, Low Inflammatory Foods Everyday (LIFE) Diet. Am. J. Lifestyle Med. 2019, 2019. [Google Scholar] [CrossRef]
- Li, T.; Qiu, Y.; Yang, H.S.; Li, M.Y.; Zhuang, X.J.; Zhang, S.H.; Feng, R.; Chen, B.L.; He, Y.; Zeng, Z.R.; et al. Systematic review and meta-analysis: Association of a pre-illness Western dietary pattern with the risk of developing inflammatory bowel disease. J. Dig. Dis. 2020, 21, 362–371. [Google Scholar] [CrossRef]
- Okręglicka, K. Health effects of changes in the structure of dietary macronutrients intake in western societies. Rocz. Państwowego Zakładu Hig. 2015, 66, 97–105. [Google Scholar]
- Zimmermann, M.B.; Aeberli, I. Dietary determinants of subclinical inflammation, dyslipidemia and components of the metabolic syndrome in overweight children: A review. Int. J. Obes. 2008, 32, S11–S18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Navarro, S.L.; Kantor, E.D.; Song, X.; Milne, G.L.; Lampe, J.W.; Kratz, M.; White, E. Factors Associated with Multiple Biomarkers of Systemic Inflammation. Cancer Epidemiol. Biomark. Prev. 2016, 25, 521–531. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cunningham-Rundles, S.; McNeeley, D.F.; Moon, A. Mechanisms of nutrient modulation of the immune response. J. Allergy Clin. Immunol. 2005, 115, 1119–1128. [Google Scholar] [CrossRef]
- Zolin, S.J.; Vodovotz, Y.; Forsythe, R.M.; Rosengart, M.R.; Namas, R.; Brown, J.B.; Peitzman, A.P.; Billiar, T.R.; Sperry, J.L. The Early Evolving Sex Hormone Enviorment is Associated with Significant Outcome and Inflamatory Response Differences Post-injury. J. Trauma Acute Care Surg 2015, 78, 451. [Google Scholar] [CrossRef] [Green Version]
- Da Silva, C.T.B.; de Abreu Costa, M.; Kapczinski, F.; de Aguiar, B.W.; Salum, G.A.; Manfro, G.G. Inflammation and internalizing dis-orders in adolescents. Prog. Neuropsychopharmacol. Biol. Psychiatry. 2017, 77, 133–137. [Google Scholar] [CrossRef]
- Whitacre, C.C. Sex differences in autoimmune disease. Nat. Immunol. 2001, 2, 777–780. [Google Scholar] [CrossRef] [PubMed]
- Ortona, E.; Pierdominici, M.; Maselli, A.; Veroni, C.; Aloisi, F.; Shoenfeld, Y. Sex-based differences in autoimmune diseases. Ann. Ist. Super. Sanità 2016, 52, 205–212. [Google Scholar]
- Ağirbaşli, M.; Agaoglu, N.B.; Orak, N.; Caglioz, H.; Ocek, T.; Poci, N.; Salaj, A.; Maya, S. Sex hormones and metabolic syndrome in children and adolescents. Metabolism 2009, 58, 1256–1262. [Google Scholar] [CrossRef]
- Reilly, S.M.; Saltiel, A.R. Adapting to obesity with adipose tissue inflammation. Nat. Rev. Endocrinol. 2017, 13, 633–643. [Google Scholar] [CrossRef]
- Monteiro, R.; Azevedo, I. Chronic Inflammation in Obesity and the Metabolic Syndrome. Mediat. Inflamm. 2010, 2010, 1–10. [Google Scholar] [CrossRef]
- Livingstone, M.B.E.; Robson, P.J. Measurement of dietary intake in children. Proc. Nutr. Soc. 2000, 59, 279–293. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Foster, E.; Adamson, A.J. Challenges involved in measuring intake in early life: Focus on methods. Proc. Nutr. Soc. 2014, 73, 201–209. [Google Scholar] [CrossRef]
- Magarey, A.; Watson, J.; Golley, R.K.; Burrows, T.; Sutherland, R.; Mcnaughton, S.A.; Denney-Wilson, E.; Campbell, K.; Collins, C. As-sessing dietary intake in children and adolescents: Considerations and recommendations for obesity research. Int. J. Pediatr. Obes. 2011, 6, 2–11. [Google Scholar] [CrossRef]
- Cowan, S.F.; Leeming, E.R.; Sinclair, A.; Dordevic, A.L.; Truby, H.; Gibson, S.J. Effect of whole foods and dietary patterns on markers of subclinical inflammation in weight-stable overweight and obese adults: A systematic review. Nutr. Rev. 2019, 78, 19–38. [Google Scholar] [CrossRef]
- Potischman, N. Biologic and Methodologic Issues for Nutritional Biomarkers. J. Nutr. 2003, 133, 875S–880S. [Google Scholar] [CrossRef] [Green Version]
- Cunha, A.L.P.d.; Costa, A.C.C.d.; Vasconcelos, Z.; Carmo, M.d.G.T.D.O.; Chaves, C.R.M.d.M. Fatty acid profile in erythrocytes associated with serum cytokines in pediatric cystic fibrosis patients. Rev. Nutr. 2018, 31, 455–466. [Google Scholar] [CrossRef]
- Klein-Platat, C.; Drai, J.; Oujaa, M.; Schlienger, J.-L.; Simon, C. Plasma fatty acid composition is associated with the metabolic syndrome and low-grade inflammation in overweight adolescents. Am. J. Clin. Nutr. 2005, 82, 1178–1184. [Google Scholar] [CrossRef] [Green Version]
- Berger, M.E.; Smesny, S.; Kim, S.-W.; Davey, C.G.; Rice, S.; Sarnyai, Z.; Schlögelhofer, M.; Schäfer, M.R.; Berk, M.; McGorry, P.D.; et al. Omega-6 to omega-3 polyunsaturated fatty acid ratio and subsequent mood disorders in young people with at-risk mental states: A 7-year longitudinal study. Transl. Psychiatry 2017, 7, e1220. [Google Scholar] [CrossRef]
- Dragsted, L.O.; Gao, Q.; Scalbert, A.; Vergères, G.; Kolehmainen, M.; Manach, C.; Brennan, L.; Afman, L.A.; Wishart, D.S.; Andres-Lacueva, C.; et al. Validation of biomarkers of food intake—Critical assessment of candidate biomarkers. Genes Nutr. 2018, 13, 1–14. [Google Scholar] [CrossRef] [Green Version]
- Tworoger, S.S.; Hankinson, S.E. Use of biomarkers in epidemiologic studies: Minimizing the influence of measurement error in the study design and analysis. Cancer Causes Control. 2006, 17, 889–899. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Author and Country (* also in Table 2) | Sample Characteristics | Pathology (Present or Outcome) | Dietary Pattern or Index (Intervention Period if Applicable) | Components of Dietary Pattern or Indices | Biological Markers of Inflammation | Main Findings ↑ Increase/Positive Association ↓ Decrease/Negative or Inverse Association ↔ No Association |
|---|---|---|---|---|---|---|
| Experimental | ||||||
| Damsgaard et al. (2012) (Europe) [42] | n = 253 13.2 (10.6–16.2) female 12.8 (10.3–15.2) male 51% female | Parents were overweight/obese Present | Randomized to 1 of 5 diet patterns: 1. High Protein Diet Pattern 2. Low Protein Diet Pattern 3. HGI Diet Pattern 4. LGI Diet Pattern 5. Control (6 months) | High protein/low protein High GI/low GI | hs-CRP | Patterns—high protein, low protein, high GI, low GI, control: ↔ No associations |
| Iannuzzi et al. (2009) (Italy) [43] | n = 26 7–13 years 54% female | Obese Present | Hypocaloric HGI Diet Pattern Hypocaloric LGI Diet Pattern | HGI: Energy intake 30% < required for weight maintenance, 25–30% fat, 15–20% protein, 50–60% carbohydrate, high glycaemic index. LGI: same as HGI diet but mean daily estimated index was 60 | CRP | HGI intake: CRP ↓ LGI intake: CRP ↓ |
| Parillo et al. (2012) (Italy) [44] | n = 22 8–13 years 54% female | Obese Present | Hypocaloric HGI Diet Pattern Hypocaloric LGI Diet Pattern | HGI: Energy intake < 30% less than reqd. for weight maintenance, 25–30% fat, 15–20% protein, 50–60% carbohydrate, fibre intake 0.5 g/kg and high glycaemic index of 90. LGI: Same as for HGI diet, but mean daily estimated glycaemic index was 60. | hs-CRP | HGI intake: CRP ↓ LGI intake: CRP ↓ |
| Rouhani et al. (2016) (Iran) [45] | n = 50 Exp-25, 13.28 ± 0.16 Cont-25, 13.93 ± 0.24 100% female | Overweight/obese Present | LGI Diet Pattern HND (10 weeks) | LGI: carbohydrate containing foods from a list of LGI grains, fruits, vegetables, dairy and high glycaemic foods to be avoided (moderately calorie restricted) HND: based on healthy eating guidelines | CRP, Il-6 | LGI intake: IL-6 and CRP ↓, HND intake: Il-6 ↓ All other ↔ |
| Saneei et al. (2014) (Iran) [41] | n = 60 (30 exp. 30 cont.) 14.2 ± 0.7 100% female | Metabolic syndrome Present | Randomized to: DASH Dietary Pattern Typical Iranian Diet (cross-over trial: 6-wk cycle, 4 wk wash-out) | DASH Diet Typical Iranian Diet | CRP, IL-2, IL-6, TNF-α, | DASH, compared to typical Iranian diet: CRP ↓ All other ↔ |
| Observational | ||||||
| Agostinis-Sobrinho et al. (2018) (Columbia and Portugal) [46] | n = 1462 13.5 ± 2.1 43% female | NA | MDP | Kidmed (16 questions, maximum score 12): Group 1—optimal adherence (≥8, optimal MedDiet); and Group 2 and 3—Low adherence (4–7, improvement needed (adjust intake to Med) or ≤3, very low diet quality) | hs-CRP | Optimal adherence to MDP + High MF/High CRF: hs-CRP ↓ Optimal adherence to MDP + Low MF/Low CRF: hs-CRP ↑ Low adherence to MedDiet + Low MF/Low CRF: hs-CRP ↑ |
| Almeida-de-Souza et al. (2015) (Portugal) [55] | n = 329 15.00 (13.0–16.0) 56% female | NA | DII | DII score was calculated considering 31 food parameters, expressed as tertiles: Tertile 1—low (<−1.34) Tertile 2—medium (−1.34 to 1.41) Tertile 3—high (>1.41) | CRP, IL-6 | DII: 0.57 ± 0.92–2.07 3rd Tertile compared to 1st: Il-6 ↑ CRP ↔ |
| Arouca et al. (2017) * (Europe) [47] | n = 464 14.79 ± 1.24 53% female | NA | MDP | MDP: MD score (0–9 points, higher scores indicating greater adherence) Positive components: (1) high ratio of monounsaturated to saturated dietary lipids (mainly olive oil), (2) vegetables, (3) fruits and nuts, (4) fish (5) cereals (6) of pulses Negative components: (7) meat and meat products (8) milk and dairy products, and (9) any consumption of alcohol (deducted in this study) | CRP, IL-1, IL-2, IL-4, IL-5, IL-6, Il-10, sVCAM-1, sICAM-1, sE-selectin, TNF-α, TGFβ-1 | MDS (mean 4.23 ± 1.49 boys, 4.19 ± 1.43 girls): CRP, TGFβ-1 ↑ (boys), sVCAM-1 ↓ (all) All other ↔ |
| Carvalho et al. (2018) (Multi-country) [48] | n = 242 14.4 ± 1.1 56.61% female | NA | MDP | MDP: modified MD score (0–8 points, higher scores indicating greater adherence) Positive components: (1) high ratio of monounsaturated to saturated dietary lipids (mainly olive oil), (2) vegetables, (3) fruits and nuts, (4) fish (5) cereals (6) of pulses Negative components: (7) meat and meat products (8) milk and dairy products | CRP, IL-1, IL-2, IL-4, IL-6, TNF-α, | MDS: 4.2 ± 1.5 High adherence vs. low adherence: IL-1, IL-2, IL-6, TNF-α ↓ (unadjusted) |
| Chan et al. (2015) (Australia) [61] | n = 1419 14 years, 49% female n = 843 17 years 53.5% female | NA | DGI-CA | Modified DGI-CA: score 0–100 points, scores closer to 100 represent maximum compliance, item 10. alcohol excluded Eleven indicators (1) wide variety of foods, (2) serves of vegetables, legumes, fruit (3) serves of breads and cereals (4) lean meat/fish/poultry (5) milk/yoghurt/cheese (6) plenty of water (7) limited SFA/moderate total fat (8) low salt foods (9) prevent weight gain (10) | hs-CRP | DGI-CA 14-yrs 47.1 ± 10.2; and DGI-CA17-yrs 47.7 ± 11.0: ↔ No associations reported |
| Coheley et al. (2019) (USA) [56] | n = 323 11.38 ± 1.23 57% female | NA | DII | DII calculated from 27 food parameters available (of 45 recognised in the DII score) from the 3 day food diary, expressed as levels of inflammatory potential: [<−1.34]—low [−1.34 to 1.41]—medium [>1.41]—and high | IL-6, MCP-1, TNF-α | DII: score 0.59 ± 1.36 (pro-inflammatory): ↔ No associations reported |
| del Mar Bibiloni (2013) * (Spain) [39] | n = 219 14.9 ± 1.3 100% female | NA | WDP MDP | WDP—yoghurt and cheese, dairy desserts, red meats, poultry, sausages, eggs, bread, cereals, pasta, rice dishes, pizza, fruit juices, canned fruits, nuts, soft drinks, high-fat foods, other oils and fats, sweets and chocolates MDP—yoghurt and cheese, red meat, poultry, fish and seafood, eggs, legumes, pasta, fresh fruit, fruit juices, vegetables, potatoes, tubercles and olive oil Participants were categorised across tertiles of the two patterns | hs-CRP, IL-6, PAI-1, TNF-α | WDP score: Il-6 ↑, ↔ All other MDP score: ↔ No associations reported |
| Douros et al. (2018) (Greece) [49] | n = 70 Exp-44, 8.9 ± 2.4, 41% female Cont-26, 8.6 ± 2.1, 35% female | Asthma Present | MDP | Kidmed (16 questions, maximum score 12): Optimal adherence: ≥8, optimal MedDiet Average adherence: 4–7 Low adherence: ≤3 | IL-4, IL-17, IL-33 | KidMed (mean 5.70 ± 1.94): Asthmatic only: IL-4, Il-17 ↓ Il-33 ↑ Control: ↔ No associations reported |
| Karampola et al. (2019) * (Greece) [50] | n = 142: Exp-71 (28 overweight/43 obese) Cont-71 13.4 ± 1.46 46% female | Overweight/obese Present | MDP | KidMed (16 questions, maximum score 12): Group 1—optimal adherence (≥8, optimal MedDiet); Group 2 and 3—Low adherence (4–7, improvement needed (adjust intake to Med) or ≤3, very low diet quality) | hs-CRP | KidMed—obese—5, overweight—7, controls—6: ↔ No associations reported |
| Khayyatzadeh et al. (2018) (Iran) [54] | n = 670 14.5 ± 1.5 100% female | NA | WDP | WDP: high in refined grains, snacks, red meats, poultry, fish, organ meat, pizza, fruit juices, industrial juice and compote, mayonnaise, nuts, sugars, soft drinks, sweets and desserts, coffee and pickle | hs-CRP | WDP (higher adherence): hs-CRP ↑ |
| Kurklu et al. (2019) (Turkey) [57] | n = 343 10–16 years 63% female | Metabolic syndrome Outcome | DII | DII calculated from 31 food parameters available (of 45 recognised in the DII score) from the 3 day food diary, expressed as levels of inflammatory potential: Quartile 1 = 1.04–3.19 Quartile 2 = 3.19–3.80 Quartile 3 = 3.81–4.31 Quartile 4 = 4.32–5.11 | CRP, IL-6, TNF-α | DII (range: 1.04–5.11, average 3.6 ± 0.82): 4th quartile compared to 1st quartile: Il-6 ↑ ↔ All other |
| Lazarou et al. (2010) (Greece) [51] | n = 83 9.2 ± 1.7 50% female | Obesity Present | MDP DII | KidMed (16 questions, maximum score 12): 0–3: Poor quality 4–12: at least average quality Inflammatory Foods Index: composed of nine foods/food groups | hs-CRP | KidMeD: CRP < 0.10 mg/dL: 33% poor quality, 67% at least average quality CRP > 0.10 mg/dL: 31% poor quality, 69% at least average quality MDP: ↔ No associations reported DII (high score): hs-CRP ↑ |
| Liese et al. (2017) (USA) [40] | n = 2520 14.2 ± 3.0 50% female | Type-1 Diabetes Present | DASH dietary pattern HEI-2010 MDP-modified KidMed TAC | Dietary indices were used to evaluate diet quality in this study; DASH, HEI2010, KidMed and TAC All indices were coded based on food item, food group and nutrient data | CRP, IL-6 | DASH (43; possible range 0–80): ↔ No associations reported HEI-2010 (55; possible range 0–100): ↔ No associations reported Modified KidMed (3.7; possible range 3–12): ↔ No associations reported Total Antioxidant Capacity (TAC): ↔ No associations reported |
| Navarro (2017) * (Spain) [59] | n = 571 6.8 years 53% female | NA | HEI | HEI Pattern 1: fibre, fruit, fruit and vegetable, and vitamin A and E intakes Pattern 2: fat intake, particularly monounsaturated and polyunsaturated intakes | hs-CRP | HEI (higher score 62.8 ± 10.3 females): hs-CRP ↓ (females only, 3rd tertile hs-CRP) Pattern 1: hs-CRP ↓ (female only) Pattern 2: ↔ No associations reported |
| Oddy et al. (2018) (Australia) [37] | n = 843 14 years 51% female 3-year follow-up | Depression Outcome | WDP (compared to HDP) | WDP: take-away and processed foods, red and processed meats, full-fat dairy, fried potatoes, refined grains, confectionary, soft drink, crisps, sauces and dressings HDP: wholegrains, fruit, vegetables, legumes and fish | hs-CRP | WDP adherence (14-yrs): hs-CRP (17-years) ↑ HDP adherence (14-yrs): hs-CRP (17-yrs) ↓ |
| Sanjeevi et al. (2018) * (USA) [60] | n = 136 12.7 ± 2.6 % female not reported | Type-1 Diabetes Present | HEI: representing adherence to Dietary Guidelines of Americans 2015 (diet quality) (Secondary analysis of a trial that aimed to increase intake of whole plant foods in experimental group—18-month behavioural intervention trial) | Index: HEI-2015 comprised of twelve component scores summed to obtain total score 0–100. Higher score indicates higher adherence to DGA 2015 | CRP | HEI (46.05 ± 11.70): ↔ No associations reported |
| Sen et al. (2017) (USA) [38] | n = 922 3.1 years and 7.7 years % female not reported | NA | DII | DII derived from FFQ and expressed as quartiles, low to high. | hs-CRP | DII (highest quartiles—early childhood): hs-CRP, (mid childhood) ↔ No associations reported |
| Shivappa et al. (2016) (Europe) [58] | n = 532 12.5–17.5 55% female | NA | DII | DII derived from 25 food parameters (of 45 recognised in the DII score) and expressed levels of inflammatory potential: Tertile 1—low inflammation Tertile 2—medium inflammation Tertile 3—high inflammation | CRP, IL-1, IL-2, IL-6, IL-4, IL-10, IFN-y, sICAM, sVCAM, TNF-α | DII (Tertile 3): IL-1, IL-2, IFN-y, TNF-α, sVCAM ↑ ↔ All other |
| Sureda et al. (2018) (Spain) [52] | n = 364 12–17 years 60% female | NA | MDP | MDP: MD score (0–9 points, higher scores indicating greater adherence) Energy-adjusted, daily consumption values of: legumes, cereals and roots (including bread and potatoes), fruit (including nuts), vegetables, fish, meat (and meat products) and milk (and milk products). Alcohol considered null. Summed then converted to the relative percentage of adherence: Above median value (≥50%) Under median value (<50%) | hs-CRP, PAI-1, TNF-α | Females—41% above median (average adherence): Med Diet Score: hs-CRP ↓, ↔ All other Males—46% above median (average adherence): Med Diet Score: ↔ No associations reported |
| Vyncke et al. (2013) (Europe) [62] | n = 1804 (biomarker sub-sample 552) 14.7 ± 1.2 53% female | NA | DQI-A | DQI-A score 0–100 points, scores closer to 100 represent maximum compliance derived from intake of: (1) water, (2) bread and cereals, (3) grains and potatoes, (4) vegetables, (5) fruit, (6) milk products, (7) cheese, (8) meat, fish, eggs, and substitutes, (9) fats and oils | hs-CRP, IL-1, IL-6, IFN-y, TNF-α | DQI-A (range 11.1 to 82.5, median 55.0): ↔ No associations reported |
| Yilmaz et al. (2019) (Turkey) [53] | n = 95 10–18 years 56% female | Obesity (Present) Cardiovascular Risk Factors (Outcome) | MDP | KidMed (16 questions, maximum score 12): Optimal adherence: ≥8, optimal MedDiet Average adherence: 4–7 Low adherence: ≤3 | hs-CRP | Med Diet Quality (low adherence—60% of participants): ↔ No associations reported |
| Author and Country (* also in Table 1) | Sample Characteristics | Pathology (Present or Outcome) | Dietary Intake (Intervention Period If Applicable) | Components Examined | Biological Markers of Inflammation | Main Findings ↑ Increase/Positive Association ↓ Decrease/Negative or Inverse Association ↔ No Association |
|---|---|---|---|---|---|---|
| Experimental—Food Groups and Nutrients | ||||||
| Hajihashemi et al. (2014) (Iran) [71] | n = 44 (22 exp. 22 cont.) 8–15 years 100% female | Overweight/obese Present | Randomized to: Whole-grain diet Control (cross-over trial—6-week cycle, 2 week run-in, 4 week wash-out) | Food group: whole-grains | hs-CRP, sICAM, sVCAM, SAA | Wholegrains v control: hs-CRP, sICAM, SAA ↓ ↔ All other |
| Jin et al. (2014) (USA) [73] | n = 21 Exp. 9, 14.2 ± 0.88, 33% female Cont, 12, 13.0 ± 0.71, 67% female | Non-alcohol fatty liver disease marker (hepatic fat >8%) | Randomized to: Glucose Group Fructose Group (4 weeks) | Food group —sugar sweetened beverages containing 33 g of sugar in either fructose or glucose form | hs-CRP, PAI-1 | Post 4 weeks: Glucose: hs-CRP ↓ ↔ All other |
| Machado et al. (2014) (Brazil) [81] | n = 75 Exp 1–25, 52% female Exp 2–25, 48% female Cont. 25, 56% female 13.7 ± 2.1 | Overweight Present | Randomized to: Brown Flax Seed (BF) Golden Flax Seed (GF) Control (11 weeks) | Macronutrients: Fibre from provided foods containing brown, golden or no flax seed: coconut cookies, cereal bars, cake, kibbeh, basked stuffed pastries, butter cookies | CRP, interleukin (IL), IL-1B, IL-6, IL-10, INF-y, TNF-α | BF, GF, Cont: TNF-α ↑ All other: ↔ |
| Food Groups—Observational | ||||||
| Arouca et al. (2017) * (Europe) [47] | n = 464 14.79 ± 1.24 53% female | NA | Food Groups Nutrients | Food groups (MedDiet constituents): vegetables, fruits, nuts, pulses, cereals and roots, dairy, fish, meat Macronutrient: MUFA, | CRP, IL-1, IL-2, IL-4, IL-5, IL-6, IL-10, sVCAM-1, sICAM-1, sE-selectin, TNF-α, TGFβ | Dietary Intake: Vegetables and fruit: IL-10 ↑ (all, females), CRP ↑ (males), IL-4 ↓ (all, females), TNF-α ↓ (females) Pulses: IL-5 ↑ (males), IL-6 ↑ (all, males), IL-2 (females) Cereals (refined grains): IL-6, IL-10 ↓ (all) MUFA/SFA: IL-6 (all, females), sVCAM-1 (males), TGFβ-1 (females) ↑ sVCAM-1 (females)↓ Dairy: IL-1 (all, females), IL-5 (all, males), IL-6 (all, males, females), IL-10 (females), TGFβ-1 (females) ↑ Meat: IL-2 (females), IL-10 (all, females) ↑ ↔ All other |
| Aslam et al. (2020) (Greece) [68] | n = 1338 11.5 ± 0.7 51% female | NA | Food Groups | Food group: Dairy products | hs-CRP, IL-6 | ↔ No associations reported |
| Cabral et al. (2018) (Portugal) [69] | n = 991 13 years 54% female | NA | Food groups | Food groups: vegetables, fruits, starchy, refined grains, whole-grains, dairy, seafood, meat, soft-drink, fast-food, sweets and pastry | hs-CRP | Vegetables/legumes (higher intake): hs-CRP ↓ (obese only) |
| Gonzales-gil (2015) (Europe) [63] | n = 6403 2519 aged 2–6 years 48% female 3884 aged 6–10 years 51% female | NA | Food Groups | Food groups: vegetables, fruits, refined grains, whole-grains, milk, dairy (yoghurt and cheese), fish, meat, egg, drinks, processed foods/snack foods, added sugar—spreads/jam/honey | hs-CRP | Vegetable (increased intake): hs-CRP (males and females) ↓ Refined grains (increased intake): hs-CRP (females) ↑ SSB (increased intake): hs-CRP (females) ↑ ↔ All other |
| Hagin et al. (2017) (USA) [65] | n = 86 12.6 years mean 43% female | Inflammatory Bowel Disease (69% with Crohns Disease) Present | Food Groups | Food groups: vegetables, fruits, snacks (including potato chips, candy, cookies, etc) | CRP | Vegetable intake: CRP ↓ ↔ All other |
| Han et al. (2015) (Puerto Rico) [67] | n = 678 10.5 ± 2.7 47% female | Asthma Present | Food Groups | Food groups: vegetables, fruits, whole-grains, dairy, meat, fats/oils, sweets/soda/snacks | IL-1B, IL-4, IL-6, IL-10, IL-17A, IL-17F, IL-21, IL-22, IL-23, IL-25, IL-31, IL-33, INF-y, TNF-α | Vegetables: IL-17F ↓ Whole-grains: IL-17F ↓ Dairy: IL-17F ↑ Sweets/Soda/Snacks: IL-17F ↑ ↔ All other |
| Holt et al. (2009) (USA) [66] | n = 285 14.9 ± 1.23 46% female | NA | Food Groups Nutrients | Food Groups: vegetables, fruits, fruit juice, french-fried potatoes, legumes Micronutrients: vitamin C, beta-carotene | hs-CRP, IL-6, TNF-α | Total vegetable and fruit: TNF-α, IL-6, ↓ Vegetable: TNF-α ↓ Fruit: hs-CRP ↓ Vitamin C: hs-CRP, IL-6 ↓ Beta-Carotene: IL-6 and TNF-α ↓ ↔ All other |
| Hur et al. (2012) (USA) [72] | n = 4928 15.5 ± 0.1 49% female | NA | Food Groups Nutrients | Food groups: whole-grains | CRP | Whole-grain: CRP ↓ (females) |
| Kosova et al. (2012) (USA) [74] | n = 4880 3–11 years 49% female | NA | Food groups | Food groups: Sugar sweetened beverage intake | CRP | SSB (high intake): CRP ↑ (males) |
| Navarro (2017) * (Spain) [59] | n = 571 6.8 years 53% female | NA | Food Groups Nutrients | Food groups: vegetables, fruits Macronutrients: fat, carbohydrate, protein, fibre Micronutrients: Vitamins: A, E | hs-CRP | High dietary intake: Fruit and Vegetable: hs-CRP ↓ (female) SFA, vitamins A, E: hs-CRP ↑ (female only) Fibre: hs-CRP ↓ (female only) ↔ All other |
| Qureshi et al. (2009) (USA) [64] | n = 4110 11.6 ± 3.3 50% female | NA | Food Groups Nutrients | Food groups: vegetables, fruits, whole-grains, refined grains, dairy, meat/other proteins including eggs Macronutrients: fat, carbohydrate, protein, fibre | hs-CRP | Vegetables, refined grain (low intake): hs-CRP ↑ ↔ All other |
| Sanjeevi et al. (2018) * (USA) [60] | n = 136 12.7 ± 2.6 % female not reported | Type-1 Diabetes Present | Food Groups Nutrients (Secondary analysis of a trial that aimed to increase intake of whole plant foods in experimental group) | Food groups: vegetables, fruits, whole-grains, dairy, meat, eggs, seafood, nuts and seeds, refined grains, sodium, added sugars Macronutrients: fat (SFA) | CRP | ↔ No associations reported |
| Nutrients—Observational | ||||||
| Aeberli et al. (2006) (Switzerland) [70] | n = 79 10.1 ± 2.1 46.83% female | Overweight/obese Present | Nutrients Food Groups | Macronutrients: fats (SFA, PUFA, MUFA, total fat), protein Food Groups: meat intake | hs-CRP, IL-6 | Fat (Total fat, % energy as fat): hs-CRP ↑ ↔ All other |
| Arya et al. (2005) (India) [78] | n = 359 18 ± 2.3 13% female | NA | Nutrients | Macronutrients: fat, carbohydrate, protein, fibre | CRP | SFA (high intake): CRP ↑ ↔ All other |
| Au et al. (2012) (USA) [80] | n = 148 10–12 years % female unknown | Cardiometabolic Risk Outcome | Nutrients | Macronutrients: Fat (SFA, MUFA, PUFA), carbohydrate | hs-CRP, IL-6 | ↔ No associations reported |
| de Sousa et al. (2017) (Brazil) [89] | n = 52 14–19 years 100% male | NA | Nutrients | Micronutrients: Dietary zinc | IL-1B, IL-6, TNF-α | ↔ No associations reported |
| del Mar Bibiloni (2013) * (Spain) [39] | n = 219 14.9 ± 1.3 100% female | NA | Nutrients | Macronutrients: fat (SFA, PUFA—linoleic acid, MUFA—oleic acid) Micronutrients: beta-carotene, vitamins A, C, E, manganese, selenium, magnesium | hs-CRP, IL-6, PAI-1, TNF-α, | Dietary intake of: PUFA (linoleic acid): PAI-1 ↓ MUFA (oleic acid), vitamin E: Il-6 ↓ Magnesium: Il-6 ↑ ↔ All other |
| Harris et al. (2019) (Germany) [77] | n = 824 15.2 ± 0.3 53% female | NA | Nutrients | Macronutrients: Fat (SFA) | hs-CRP | SFA: hs-CRP ↓ (males only) |
| Jaacks et al. (2014) (USA) [82] | n = 1405 47.9 ± 43.2 50% female | Type-1 Diabetes Present | Nutrients | Macronutrients: Dietary Fibre | Il-6, CRP | ↔ No associations reported |
| Karampola et al. (2019) * (Greece) [50] | n = 142 13.4 ± 1.46 % female not stated | Overweight/obese Present | Nutrients Food Groups | Macronutrients: fat, carbohydrates, protein, fibre Food groups: added sugars | hs-CRP | ↔ No associations reported |
| King et al. (2016) (USA) [88] | n = 5007 6–17 years 47% female | NA | Nutrients | Micronutrients: magnesium | CRP | Magnesium (low intake): CRP ↑ |
| Lin et al. (2014) (Europe) [83] | n = 1804 14.7 ± 1.2 53% female | NA | Nutrients | Macronutrients: fibre—total fibre, energy-adjusted fibre, water in/soluble fibre | CRP | ↔ No associations reported |
| Miller et al. (2017) (USA) [86] | n = 142 15.3 ± 0.1 66.43% female | Overweight/obese Present | Nutrients | Macronutrients: dietary fibre derived from dietary intake information: fat, carbohydrate, added sugars, protein, vegetable, fruit, wholegrains, legumes, refined grains, SSB, snack foods (sweet) | IL-6, IL-8, monocyte chemoattractant protein-1 (MCP1), PAI-1, TNF-α | Total fibre: PAI-1 ↓ Insoluble fibre: PAI-1, MCP-1 ↑ ↔ All other |
| Oldewage-Theron et al. (2016) (South Africa) [79] | n = 232 6–18 years 51.29% female | NA | Nutrients | Macronutrients: fat (PUFA, MUFA, SFA, TFA, linoleic acid) Micronutrients: iron, zinc, magnesium, vitamin C, E | hs-CRP | ↔ No associations reported |
| Parikh et al. (2012) (USA) [85] | n = 559 14–18 years 49% female | NA | Nutrients | Macronutrients: fibre | hs-CRP, | Fibre: hs-CRP (both genders) ↓ ↔ All other |
| Prihaningtyas et al. (2019) (Indonesia) [75] | n = 59 13–16 years 46% female | Obesity Present | Nutrients | Macronutrients: fat, carbohydrate, protein | hs-CRP | ↔ No associations reported |
| Swann et al. (2020) (Australia) [84] | n = 621 17-years 53% | N/A | Nutrients | Macronutrient: fibre | hs-CRP | ↔ No associations reported |
| Thomas et al. (2007) (UK) [76] | n = 164 12–13 years 54% female | NA | Nutrients | Macronutrients: fat (SFA) | hs-CRP | ↔ No associations reported |
| Zhu et al. (2014) (USA) [87] | n = 766 14–18 years 50% female | NA | Nutrients | Micronutrients: dietary sodium | hs-CRP, ICAM-1, TNF-α | Sodium intake: TNF-α ↑ ↔ All other |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bujtor, M.; Turner, A.I.; Torres, S.J.; Esteban-Gonzalo, L.; Pariante, C.M.; Borsini, A. Associations of Dietary Intake on Biological Markers of Inflammation in Children and Adolescents: A Systematic Review. Nutrients 2021, 13, 356. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13020356
Bujtor M, Turner AI, Torres SJ, Esteban-Gonzalo L, Pariante CM, Borsini A. Associations of Dietary Intake on Biological Markers of Inflammation in Children and Adolescents: A Systematic Review. Nutrients. 2021; 13(2):356. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13020356
Chicago/Turabian StyleBujtor, Melissa, Anne I. Turner, Susan J. Torres, Laura Esteban-Gonzalo, Carmine M. Pariante, and Alessandra Borsini. 2021. "Associations of Dietary Intake on Biological Markers of Inflammation in Children and Adolescents: A Systematic Review" Nutrients 13, no. 2: 356. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13020356