
Three-Year Follow-Up of the POIBA Intervention on Childhood Obesity: A Quasi-Experimental Study

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
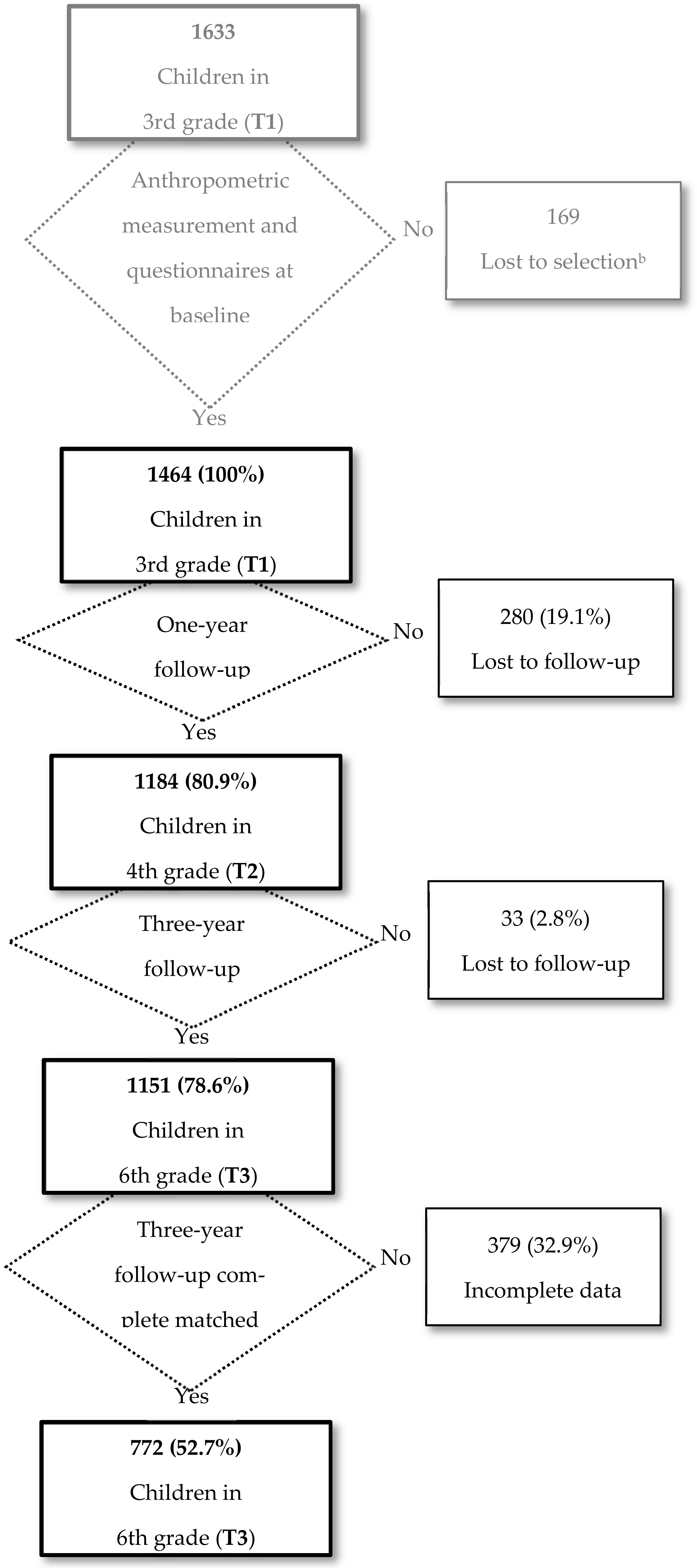
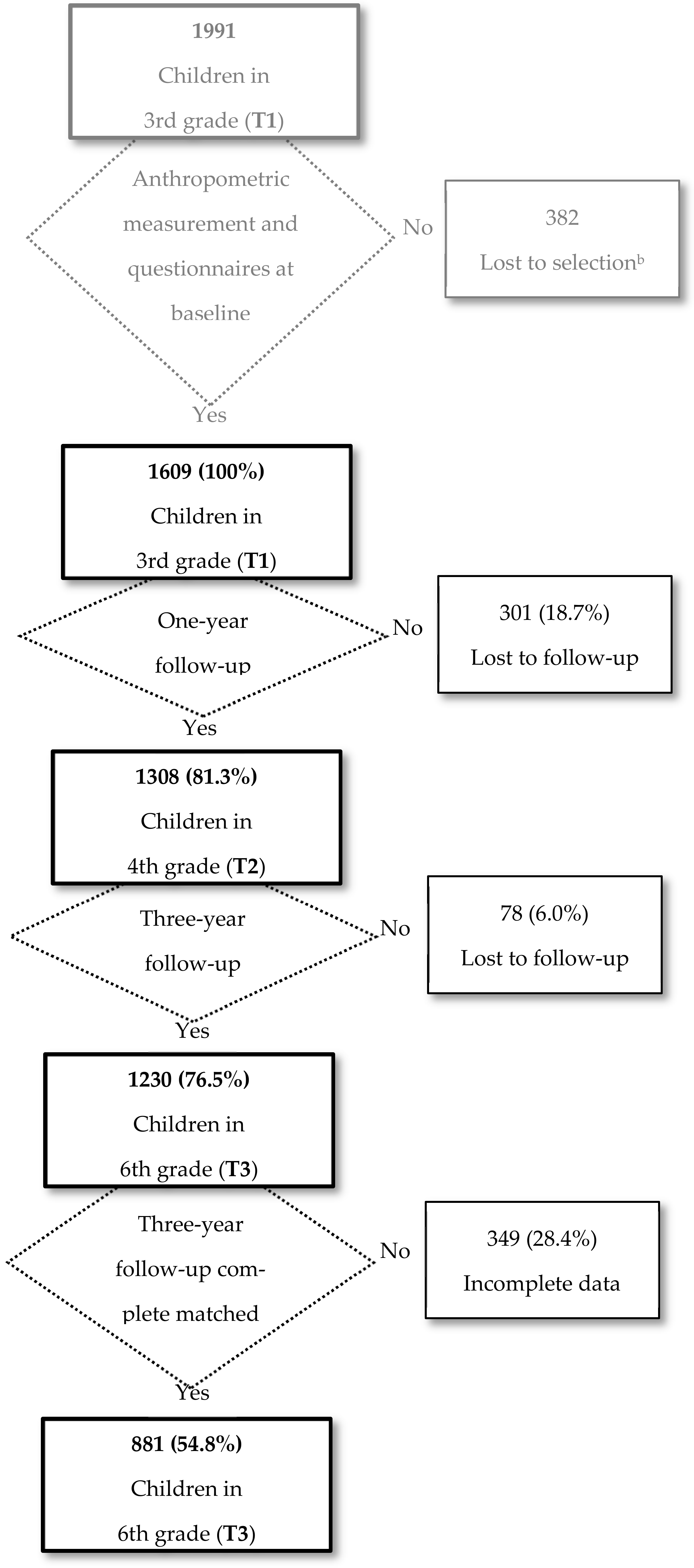
2.2. Study Population
Intervention
- Classroom component
- ”Our digestion”. The contents of the session were based on knowing the phases of the digestion process, assessing the importance of chewing food properly, and respecting the necessary rest after each meal to promote the digestion process. The activity worked included a worksheet to complete and a group discussion.
- “Food groups”. The aims of this session were to know the five food groups (fruit and vegetables; starchy food; dairy; protein (meat, fish, eggs and nuts); oils, fats, and sweets) and to identify the origin of each food (animal, vegetable and mineral). Two activities were proposed: the completion of a worksheet to delve into the different food groups and bringing from home products and packaging of the different food groups.
- “Nutrients and their functions”. The objectives were to know what nutrients are, identify where nutrients are found, learn to classify foods according to the main functions of nutrients, and learn some dietary recommendations. Two activities were carried out: discussing the contents of a worksheet in the group class and working on some videos focused on nutrients. The main contents of the activities focused on nutrients as essential substances for life; the classification of nutrients, according to their main function, into builders, energy and regulators, and the importance of a varied and balanced diet to obtain the nutrients necessaries for life.
- “Food pyramid”. The main aims were to know the concept of portion and how the portions are distributed, identify the food groups that form the food pyramid and their frequency of consumption, develop favorable attitudes and basic skills to incorporate the recommended foods into the diet and reduce those of sporadic consumption. The activity consisted of building a big pyramid in the classroom using the products and packaging provided by children and displaying it in a visible place in the classroom.
- “The best breakfast”. The aims were to identify the three food groups that should be included in a healthy breakfast (dairy, carbohydrates and fruit), realize that breakfast at home and at school are complementary and practice how to make a healthy and desirable breakfast. The activity consisted of preparing a healthy breakfast in small groups with food that children brought from home.
- “Remember the food pyramid”. The main objectives were to review the basic contents of the food groups and their situation in the food pyramid, understand the concept of portion, promote a favorable attitude towards a balanced diet and recognize the nutritional needs of our body. The activity consisted of rebuilding a food pyramid and working on the concept of portion based on the food groups in the pyramid.
- “A balanced diet”. The objectives were to identify correct and improvable aspects of a weekly menu, develop skills to identify if the frequencies of food groups in a diet are correct, and make proposals for a balanced diet at family dinners. The activity consisted of the assessment in small groups of a balanced weekly menu, making sure that each food group appears in the appropriate quantities and frequencies.
- Physical activity component
- Family component
2.3. Data Collection
- Baseline measurement (T1): Between April and June 2011, in the third year of primary school (8–9 years old).
- One-year follow-up measurement (T2): Between April and June 2012, in the fourth grade of primary school (9–10 years old).
- Three-year follow-up measurement (T3): Between April and June 2014, in the sixth grade of primary school (11–12 years old).
2.3.1. Anthropometric Measurements
2.3.2. Information on Behaviors, Knowledge, and Attitudes
2.4. Variables
2.4.1. Outcome Variables
Primary Outcome
Intermediate Outcome
- Food frequency: Healthy foods (water, fruits and vegetables, and meat) were measured according to the number of weekly or daily servings. Unhealthy foods (sweets and fried potatoes) were measured according to higher occasional or casual consumption [36].
- Food behavior: Having a proper breakfast, including carbohydrates, dairy, and fruits [36] (yes/no); having dinner in front of the TV (yes/no); eating at school (yes/no); not eating alone, meaning having breakfast, lunch or dinner with someone at home (yes/no); frequenting fast-food restaurants (yes/no).
- Physical activity: Out-of-school physical activity (yes/no); engaging in leisure-time physical activity (<2 days/week, ≥2 days/week) [37].
- Daily use of screens: On weekdays and on weekends (<2 h/day, ≥2 h/day) [38].
- Global Nutrition score: More than one change in the nine variables of food frequency and food behavior.
- Global Activity score: More than one change in the four variables of physical activity and daily screen use.
- Global score: More than one change in the thirteen variables of the global nutrition score and global activity score.
2.4.2. Independent Variables
2.4.3. Process Evaluation Variables
2.5. Ethics
2.6. Statistical Analysis
3. Results
4. Discussion
Limitations and Strengths
5. Conclusions
5.1. Implications for Public Health
5.2. Recommendations for Future Studies
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Amini, M.; Djazayery, A.; Majdzadeh, R.; Taghdisi, M.H.; Jazayeri, S. Effect of school-based interventions to control childhood obesity: A review of reviews. Int. J. Prev. Med. 2015. [Google Scholar] [CrossRef]
- World Health Organization (WHO). Overweight and Obesity. Available online: https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight (accessed on 4 November 2019).
- World Health Organization (WHO). Prevalence of Obesity among Children and Adolescents. OECD Analysis on WHO Global Health Observatory Data. Available online: https://www.who.int/data/gho/data/themes/topics/topic-details/GHO/ncd-risk-factors (accessed on 17 January 2021).
- Moens, E.; Braet, C.; Bosmans, G.; Rosseel, Y. Unfavourable family characteristics and their associations with childhood obesity: A cross-sectional study. Eur. Eat. Disord. Rev. 2009, 17, 315–323. [Google Scholar] [CrossRef] [PubMed]
- Sanders, R.H.; Han, A.; Baker, J.S.; Cobley, S. Childhood obesity and its physical and psychological co-morbidities: A systematic review of Australian children and adolescents. Eur. J. Pediatr. 2015, 174, 715–746. [Google Scholar] [CrossRef] [PubMed]
- Román, B.; Serra-Majem, L.; Ribas-Barba, L.; Pérez-Rodrigo, C. Actividad física en la población infantil y juvenil española en el tiempo libre. Estudio enKid (1998–2000). Apunt. Med. Esport 2006, 151, 86–94. [Google Scholar]
- De Jong, E.; Visscher, T.L.S.; Hirasing, R.A.; Heymans, M.W.; Seidell, J.C.; Renders, C.M. Association between TV viewing, computer use and overweight, determinants and competing activities of screen time in 4- to 13-year-old children. Int. J. Obes. 2013, 37, 47–53. [Google Scholar] [CrossRef] [Green Version]
- Bentham, J.; Di Cesare, M.; Bilano, V.; Bixby, H.; Zhou, B.; Stevens, G.A.; Abdeen, Z.A.; Hamid, Z.A.; Abu-Rmeileh, N.M.; Acosta-Cazares, B.; et al. Worldwide trends in body-mass index, underweight, overweight, and obesity from 1975 to 2016: A pooled analysis of 2416 population-based measurement studies in 128·9 million children, adolescents, and adults. Lancet 2017, 390, 2627–2642. [Google Scholar]
- Story, M.; Kaphingst, K.M.; French, S. The role of schools in obesity prevention. Futur. Child. 2006, 16, 109–142. [Google Scholar] [CrossRef]
- Branscum, P.; Sharma, M. After-school based obesity prevention interventions: A comprehensive review of the literature. Int. J. Environ. Res. Public Health. 2012, 9, 1438–1457. [Google Scholar] [CrossRef] [Green Version]
- Hoelscher, D.M.; Kirk, S.; Ritchie, L.; Cunningham-Sabo, L. Position of the Academy of Nutrition and Dietetics: Interventions for the prevention and treatment of pediatric overweight and obesity. J. Acad. Nutr. Diet. 2013, 113, 1375–1394. [Google Scholar] [CrossRef]
- Goldthorpe, J.; Epton, T.; Keyworth, C.; Calam, R.; Armitage, C.J. Are primary/elementary school-based interventions effective in preventing/ameliorating excess weight gain? A systematic review of systematic reviews. Obes. Rev. 2020. [Google Scholar] [CrossRef]
- Lambrinou, C.P.; Androutsos, O.; Karaglani, E.; Cardon, G.; Huys, N.; Wikström, K.; Kivelä, J.; Ko, W.; Karuranga, E.; Tsochev, K.; et al. Effective strategies for childhood obesity prevention via school based, family involved interventions: A critical review for the development of the Feel4Diabetes-study school based component. BMC Endocr. Disord. 2020. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.; Kang, B.; Lee, E.Y.; Yang, H.K.; Kim, H.S.; Lim, S.Y.; Lee, J.H.; Lee, S.S.; Suh, B.K.; Yoon, K.H. Effect of an obesity prevention program focused on motivating environments in childhood: A school-based prospective study. Int. J. Obes. 2017, 41, 1027–1034. [Google Scholar] [CrossRef] [PubMed]
- Saint-Maurice, P.F.; Bai, Y.; Welk, G.J.; Bandelli, L.N.; Allums-Featherston, K.; Candelaria, N. Impact of NFL PLAY 60 programming on elementary school children’s body mass index and aerobic capacity: The NFL PLAY 60 fitnessgram partnership project. J. Sch. Health 2017, 87, 873–881. [Google Scholar] [CrossRef] [PubMed]
- Liu, Z.; Xu, H.M.; Wen, L.M.; Peng, Y.Z.; Lin, L.Z.; Zhou, S.; Li, W.H.; Wang, H.J. A systematic review and meta-analysis of the overall effects of school-based obesity prevention interventions and effect differences by intervention components. Int. J. Behav. Nutr. Phys. Act 2019. [Google Scholar] [CrossRef] [PubMed]
- Mei, H.; Xiong, Y.; Xie, S.; Guo, S.; Li, Y.; Guo, B.; Zhang, J. The impact of long-term school-based physical activity interventions on body mass index of primary school children—A meta-analysis of randomized controlled trials. BMC Public Health 2016. [Google Scholar] [CrossRef] [Green Version]
- Martin, A.; Booth, J.N.; Laird, Y.; Sproule, J.; Reilly, J.J.; Saunders, D.H. Physical activity, diet and other behavioural interventions for improving cognition and school achievement in children and adolescents with obesity or overweight. Cochrane Database Syst. Rev. 2018. [Google Scholar] [CrossRef] [Green Version]
- Eagle, T.F.; Gurm, R.; Smith, C.A.; Corriveau, N.; Durussell-Weston, J.; Palma-Davis, L.; Aaronson, S.; Goldberg, C.; Kline-Rogers, E.; Cotts, T.; et al. A middle school intervention to improve health behaviors and reduce cardiac risk factors. Am. J. Med. 2013, 126, 903–908. [Google Scholar] [CrossRef]
- Rahelić, V.; Głąbska, D.; Guzek, D.; Pavić, E.; Samarin, I.R.; Bogdanić, A.; Špehar Uroić, A.; Rojnić Putarek, N.; Krnić, N. Role of parents in body mass reduction in children with obesity—Adherence and success of 1-year participation in an intervention program. Medicina 2020, 56, 168. [Google Scholar] [CrossRef] [Green Version]
- Kalantari, N.; Mohammadi, N.K.; Rafieifar, S.; Eini-Zinab, H.; Aminifard, A.; Malmir, H.; Ashoori, N.; Abdi, S.; Gholamalizadeh, M.; Doaei, S. Indicator for success of obesity reduction programs in adolescents: Body composition or body mass index? evaluating a school-based health promotion project after 12 weeks of intervention. Int. J. Prev. Med. 2017, 8, 128–132. [Google Scholar]
- Recasens, M.A.; Xicola-Coromina, E.; Manresa, J.M.; Ullmo, P.A.; Jensen, B.B.; Franco, R.; Suarez, A.; Nadal, A.; Vila, M.; Recasens, I.; et al. Impact of school-based nutrition and physical activity intervention on body mass index eight years after cessation of randomized controlled trial (AVall study). Clin. Nutr. 2019, 38, 2592–2598. [Google Scholar] [CrossRef]
- Lohman, T.G.; Hingle, M.; Going, S.B. Body composition in children. Pediatr. Exerc. Sci. 2013, 25, 573–590. [Google Scholar] [CrossRef] [PubMed]
- Nooyens, A.C.J.; Koppes, L.L.J.; Visscher, T.L.S.; Twisk, J.W.R.; Kemper, H.C.G.; Schuit, A.J.; van Mechelen, W.; Seidell, J.C. Adolescent skinfold thickness is a better predictor of high body fatness in adults than is body mass index: The Amsterdam Growth and Health Longitudinal Study. Am. J. Clin. Nutr. 2007, 85, 1533–1539. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, Y.; Lau, B.D.; Bleich, S.; Cheskin, L.; Boult, C.; Segal, J.B.; Wang, Y. Executive summary. In Future Research Needs for Childhood Obesity Prevention Programs: Identification of Future Research Needs From Comparative Effectiveness Review No. 115; Agency for Healthcare Research and Quality: Rockville, MD, USA, 2013. [Google Scholar]
- Plachta-Danielzik, S.; Landsberg, B.; Lange, D.; Seiberl, J.; Müller, M.J. Eight-year follow-up of school-based intervention on childhood overweight—The Kiel obesity prevention study. Obes. Facts. 2011, 4, 35–43. [Google Scholar] [CrossRef] [PubMed]
- Sánchez-Martínez, F.; Juárez, O.; Serral, G.; Valmayor, S.; Puigpinós, R.; Pasarín, M.I.; Díez, É.; Ariza, C. A childhood obesity prevention programme in Barcelona (POIBA project): Study protocol of the intervention. J. Public Health Res. 2018, 7, 14–21. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ariza, C.; Sánchez-Martínez, F.; Serral, G.; Valmayor, S.; Juárez, O.; Pasarín, M.I.; Castell, C.; Rajmil, L.; López, M.J. The Incidence of obesity, assessed as adiposity, is reduced after 1 year in primary schoolchildren by the POIBA intervention. J. Nutr. 2019, 149, 258–269. [Google Scholar] [CrossRef]
- Agència de Salut Pública de Barcelona (ASPB). Creixem Sans. Available online: https://www.aspb.cat/documents/creixem-sans/ (accessed on 23 January 2021).
- Agència de Salut Pública de Barcelona (ASPB). Creixem més Sans. Available online: https://www.aspb.cat/documents/creixem-mes-sans/ (accessed on 23 January 2021).
- Arechavala, T.; Ariza, C.; Valmayor, S.; Serral, G.; Moncada, A.; Rajmil, L.; Schiaffino, A.; Sánchez-Martínez, F. Validation of ‘POIBA-how do we eat?’ questionnaire in 9–10 years old schoolchildren. Food Nutr. Res. 2017. [Google Scholar] [CrossRef] [Green Version]
- Agència de Salut Pública de Barcelona. POIBA Project. POIBA—How Do We Move? Available online: www.aspb.cat/documents/poiba-como-nos-movemos/ (accessed on 30 November 2020).
- Fryar, C.D.; Gu, Q.; Ogden, C.L. Anthropometric Reference Data for Children and Adults: United States 2007–2010; National Center for Biotechnology Information: Bethesda, MD, USA, 2012. [Google Scholar]
- De Onis, M.; Onyango, A.W.; Borghi, E.; Siyam, A.; Nishida, C.; Siekmann, J. Development of a WHO growth reference for school-aged children and adolescents. Bull. World Health Organ. 2007, 85, 660–667. [Google Scholar] [CrossRef]
- World Health Organization (WHO). Child Growth Standards. Available online: www.who.int/toolkits/child-growth-standards/standards/weight-for-age (accessed on 30 November 2020).
- Grupo Colaborativo de la Sociedad Española de Nutrición Comunitaria (SENC); Aranceta Bartrina, J.; Arija Val, V.; Maíz Aldalur, E.; Martínez de la Victoria Muñoz, E.; Ortega Anta, R.M.; Pérez-Rodrigo, C.; Quiles Izquierdo, J.; Rodríguez Martín, A.; Román Viñas, B.; et al. Dietary guidelines for the Spanish population (SENC, December 2016), The new graphic icon of healthy nutrition. Nutr. Hosp. 2016, 33, 1–48. [Google Scholar]
- Physical Activity Guidelines Advisory Committee. Physical Activity Guidelines Advisory Committee Report; Department of Health and Human Services: Washington, DC, USA, 2008.
- Bar-On, M.E.; Broughton, D.D.; Buttross, S.; Corrigan, S.; Gedissman, A.; González De Rivas, M.R.; Rich, M.; Shifrin, D.L.; Brody, M.; Wilcox, B.; et al. Children, adolescents, and television. Pediatrics 2001, 107, 423–426. [Google Scholar]
- Currie, C.; Molcho, M.; Boyce, W.; Holstein, B.; Torsheim, T.; Richter, M. Researching health inequalities in adolescents: The development of the Health Behaviour in School-Aged Children (HBSC) Family Affluence Scale. Soc. Sci. Med. 2008, 66, 1429–1436. [Google Scholar] [CrossRef]
- Gabinet Tècnic de Programació Ajuntament de Barcelona. Distribució territorial de la renda familiar a Barcelona (2008). Barc. Econ. 2009, 87, 79–87. [Google Scholar]
- El Harake, M.D.; Kharroubi, S.; Hamadeh, S.K.; Jomaa, L. Impact of a pilot school-based nutrition intervention on dietary knowledge, attitudes, behavior and nutritional status of syrian refugee children in the Bekaa, Lebanon. Nutrients 2018, 10, 913. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bleich, S.N.; Vercammen, K.A.; Zatz, L.Y.; Frelier, J.M.; Ebbeling, C.B.; Peeters, A. Interventions to prevent global childhood overweight and obesity: A systematic review. Lancet Diabetes Endocrinol. 2018, 6, 332–346. [Google Scholar] [CrossRef]
- Shaya, F.T.; Flores, D.; Gbarayor, C.M.; Wang, J. School-based obesity interventions: A literature review. J. Sch. Health. 2008, 78, 189–196. [Google Scholar] [CrossRef] [PubMed]
- Paradis, G.; Lévesque, L.; Macaulay, A.C.; Cargo, M.; McComber, A.; Kirby, R.; Receveur, O.; Kishchuk, N.; Potvin, L. Impact of a diabetes prevention program on body size, physical activity, and diet among Kanien’kehá:ka (Mohawk) children 6 to 11 years old: 8-Year results from the Kahnawake Schools Diabetes Prevention Project. Pediatrics 2005, 115, 333–339. [Google Scholar] [CrossRef]
- Dusenbury, L.; Brannigan, R.; Hansen, W.B.; Walsh, J.; Falco, M. Quality of implementation: Developing measures crucial to understanding the diffusion of preventive interventions. Health Educ. Res. 2005, 20, 308–313. [Google Scholar] [CrossRef]
- Ariza, C.; Pérez, A.; Sánchez-Martínez, F.; Diéguez, M.; Espelt, A.; Pasarín, M.I.; Suelves, J.M.; De la Torre, R.; Nebot, M. Evaluation of the effectiveness of a school-based cannabis prevention program. Drug Alcohol Depend. 2013, 132, 257–264. [Google Scholar] [CrossRef]
- Sallis, J.F.; McKenzie, T.L.; Conway, T.L.; Elder, J.P.; Prochaska, J.J.; Brown, M.; Zive, M.M.; Marshall, S.J.; Alcaraz, J.E. Environmental interventions for eating and physical activity: A randomized controlled trial in middle schools. Am. J. Prev. Med. 2003, 24, 209–217. [Google Scholar] [CrossRef]
- Wang, Y.; Cai, L.; Wu, Y.; Wilson, R.F.; Weston, C.; Fawole, O.; Bleich, S.N.; Cheskin, L.J.; Showell, N.N.; Lau, B.D.; et al. What childhood obesity prevention programmes work? A systematic review and meta-analysis. Obes. Rev. 2015, 16, 547–565. [Google Scholar] [CrossRef]
- Llargués, E.; Recasens, A.; Franco, R.; Nadal, A.; Vila, M.; Pérez, M.J.; Recasens, I.; Salvador, G.; Serra, J.; Roure, E.; et al. Evaluación a medio plazo de una intervención educativa en hábitos alimentarios y de actividad física en escolares: Estudio Avall 2. Endocrinol. Nutr. 2012, 59, 288–295. [Google Scholar]
- De Assis, M.A.A.; Kupek, E.; Guimarães, D.; Calvo, M.C.M.; de Andrade, D.F.; Bellisle, F. Test-retest reliability and external validity of the previous day food questionnaire for 7-10-year-old school children. Appetite 2008, 51, 187–193. [Google Scholar] [CrossRef] [PubMed]
- Weber, J.L.; Lytle, L.; Gittelsohn, J.; Cunningham-Sabo, L.; Heller, K.; Anliker, J.A.; Stevens, J.; Hurley, J.; Ring, K. Validity of self-reported dietary intake at school meals by American Indian children: The pathways study. J. Am. Diet. Assoc. 2004, 104, 746–752. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Intervention (n = 1151) | Comparison (n = 1230) | Total p (a) vs. (d) | Complete Cases p (b) vs. (e) | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Total (a) | Complete Cases e (b) (n = 772) | Incomplete Cases f (c) (n = 379) | p | Total (d) | Complete Cases e (e) (n = 881) | Incomplete Cases f (f) (n = 349) | p | |||||||||
| n | % | n | % | n | % | n | % | n | % | n | % | |||||
| Sex | 0.498 | 0.714 | 0.159 | 0.306 | ||||||||||||
| Male | 591 | 51.3 | 391 | 50.6 | 200 | 52.8 | 596 | 48.5 | 424 | 48.1 | 172 | 49.3 | ||||
| Female | 560 | 48.7 | 381 | 49.4 | 179 | 47.2 | 634 | 51.5 | 457 | 51.9 | 177 | 50.7 | ||||
| SESb(FAScIndex) | 0.287 | 0.108 | 0.158 | 0.285 | ||||||||||||
| High | 702 | 61.0 | 479 | 62.0 | 223 | 58.8 | 741 | 60.2 | 543 | 61.6 | 198 | 56.7 | ||||
| Middle | 310 | 26.9 | 207 | 26.8 | 103 | 27.2 | 366 | 29.8 | 259 | 29.4 | 107 | 30.7 | ||||
| Low | 137 | 11.9 | 84 | 10.9 | 53 | 14.0 | 123 | 10.0 | 79 | 9.0 | 44 | 12.6 | ||||
| Missing | 2 | 0.2 | 2 | 0.3 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | ||||
| Country of origin | 0.023 | 0.490 | 0.883 | 0.556 | ||||||||||||
| Natives | 795 | 69.1 | 550 | 71.2 | 245 | 64.6 | 853 | 69.3 | 616 | 69.9 | 237 | 67.9 | ||||
| Immigrants | 356 | 30.9 | 222 | 28.8 | 134 | 35.4 | 377 | 30.7 | 265 | 30.1 | 112 | 32.1 | ||||
| Family structure | 0.240 | 0.835 | 0.321 | 0.574 | ||||||||||||
| Two-parent home | 955 | 83.0 | 650 | 84.1 | 305 | 80.5 | 1,036 | 84.2 | 745 | 84.5 | 291 | 83.3 | ||||
| Single-parent home | 180 | 15.6 | 111 | 14.4 | 69 | 18.2 | 186 | 15.1 | 130 | 14.8 | 56 | 16.1 | ||||
| Other | 14 | 1.2 | 9 | 1.2 | 5 | 1.3 | 8 | 0.7 | 6 | 0.7 | 2 | 0.6 | ||||
| Missing | 2 | 0.2 | 2 | 0.3 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | ||||
| Type of school | <0.001 | 0.742 | 0.192 | 0.003 | ||||||||||||
| Private/Subsidized | 652 | 56.6 | 471 | 61.0 | 181 | 47.8 | 664 | 54.0 | 473 | 53.7 | 191 | 54.7 | ||||
| Public | 499 | 43.4 | 301 | 39.0 | 198 | 52.2 | 566 | 46.0 | 408 | 46.3 | 158 | 45.3 | ||||
| SES (GDHIdIndex) | <0.001 | <0.001 | <0.001 | <0.001 | ||||||||||||
| Disadvantaged SES | 561 | 48.7 | 417 | 54.0 | 144 | 38.0 | 496 | 40.3 | 299 | 33.9 | 197 | 56.4 | ||||
| Advantaged SES | 590 | 51.3 | 355 | 46.0 | 235 | 62.0 | 734 | 59.7 | 582 | 66.1 | 152 | 43.6 | ||||
| Intervention (n = 1151) | Comparison (n = 1230) | Total p (a) vs. (d) | Complete Cases p (b) vs. (e) | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Total (a) | Complete Casesd (b) (n = 772) | Incomplete Casese (c) (n = 379) | p | Total (d) | Complete Casesd (e) (n = 881) | Incomplete Casese (f) (n = 349) | p | |||||||||
| n | % | n | % | n | % | n | % | n | % | n | % | |||||
| BMIb | 0.047 | 0.399 | 0.167 | 0.157 | ||||||||||||
| Normal weight (<1 SD) | 708 | 61.5 | 494 | 64.0 | 214 | 56.4 | 761 | 61.8 | 552 | 62.6 | 209 | 59.9 | ||||
| Overweight (1 SD) | 273 | 23.7 | 172 | 22.3 | 101 | 26.7 | 317 | 25.8 | 227 | 25.8 | 90 | 25.8 | ||||
| Obesity (2 SD) | 170 | 14.8 | 106 | 13.7 | 64 | 16.9 | 152 | 12.4 | 102 | 11.6 | 50 | 14.3 | ||||
| Dinner in front of TV | 0.593 | 0.004 | 0.634 | 0.377 | ||||||||||||
| No | 594 | 51.6 | 394 | 51.0 | 200 | 52.8 | 621 | 50.5 | 467 | 53.0 | 154 | 44.1 | ||||
| Yes | 550 | 47.8 | 373 | 48.3 | 177 | 46.7 | 598 | 48.6 | 405 | 46.0 | 193 | 55.3 | ||||
| Missing | 7 | 0.6 | 5 | 0.7 | 2 | 0.5 | 11 | 0.9 | 9 | 1.0 | 2 | 0.6 | ||||
| Eating at school | 0.073 | 0.001 | 0.127 | 0.001 | ||||||||||||
| Yes | 901 | 78.3 | 591 | 76.5 | 310 | 81.8 | 985 | 80.1 | 725 | 82.3 | 260 | 74.5 | ||||
| No | 234 | 20.3 | 168 | 21.8 | 66 | 17.4 | 218 | 17.7 | 136 | 15.4 | 82 | 23.5 | ||||
| Missing | 16 | 1.4 | 13 | 1.7 | 3 | 0.8 | 27 | 2.2 | 20 | 2.3 | 7 | 2.0 | ||||
| Proper breakfastc | 0.113 | 0.181 | 0.198 | 0.936 | ||||||||||||
| Yes | 447 | 38.8 | 312 | 40.4 | 135 | 35.6 | 508 | 41.3 | 353 | 40.1 | 155 | 44.4 | ||||
| No | 697 | 60.6 | 455 | 58.9 | 242 | 63.9 | 711 | 57.8 | 519 | 58.9 | 192 | 55.0 | ||||
| Missing | 7 | 0.6 | 5 | 0.7 | 2 | 0.5 | 11 | 0.9 | 9 | 1.0 | 2 | 0.6 | ||||
| Frequenting fast-food restaurants | 0.911 | 0.046 | 0.037 | 0.286 | ||||||||||||
| No | 162 | 14.1 | 109 | 14.1 | 53 | 14.0 | 137 | 11.1 | 108 | 12.3 | 29 | 8.3 | ||||
| Yes | 977 | 84.9 | 653 | 84.6 | 324 | 85.5 | 1070 | 87.0 | 756 | 85.8 | 314 | 90.0 | ||||
| Missing | 12 | 1.0 | 10 | 1.3 | 2 | 0.5 | 23 | 1.9 | 17 | 1.9 | 6 | 1.7 | ||||
| Eating alone | 0.264 | 0.997 | 0.379 | 0.236 | ||||||||||||
| No | 1005 | 87.3 | 668 | 86.5 | 337 | 88.9 | 1085 | 88.2 | 776 | 88.1 | 309 | 88.5 | ||||
| Yes | 139 | 12.1 | 99 | 12.8 | 40 | 10.6 | 134 | 10.9 | 96 | 10.9 | 38 | 10.9 | ||||
| Missing | 7 | 0.6 | 5 | 0.7 | 2 | 0.5 | 11 | 0.9 | 9 | 1.0 | 2 | 0.6 | ||||
| Out-of-school physical activity | 0.126 | <0.001 | <0.001 | <0.001 | ||||||||||||
| Yes | 804 | 69.9 | 548 | 71.0 | 256 | 67.6 | 941 | 76.5 | 699 | 79.3 | 242 | 69.4 | ||||
| No | 334 | 29.0 | 212 | 27.5 | 122 | 32.1 | 271 | 22.0 | 170 | 19.3 | 101 | 28.9 | ||||
| Missing | 13 | 1.1 | 12 | 1.5 | 1 | 0.3 | 18 | 1.5 | 12 | 1.4 | 6 | 1.7 | ||||
| Leisure time physical activity | 0.247 | 0.196 | 0.753 | 0.809 | ||||||||||||
| Yes (≥2 h/week) | 740 | 64.3 | 485 | 62.8 | 255 | 67.2 | 782 | 63.5 | 551 | 62.5 | 231 | 66.2 | ||||
| No (<2 h/week) | 396 | 34.4 | 273 | 35.4 | 123 | 32.5 | 430 | 35.0 | 318 | 36.1 | 112 | 32.1 | ||||
| Missing | 15 | 1.3 | 14 | 1.8 | 1 | 0.3 | 18 | 1.5 | 12 | 1.4 | 6 | 1.7 | ||||
| Screen time on weekdays (Monday–Thursday) | 0.636 | 0.003 | 0.074 | 0.005 | ||||||||||||
| <2 h/day | 653 | 56.7 | 432 | 56.0 | 221 | 58.3 | 740 | 60.2 | 554 | 62.8 | 186 | 53.3 | ||||
| ≥2 h/day | 483 | 42.0 | 326 | 42.2 | 157 | 41.4 | 471 | 38.3 | 315 | 35.8 | 156 | 44.7 | ||||
| Missing | 15 | 1.3 | 14 | 1.8 | 1 | 0.3 | 19 | 1.5 | 12 | 1.4 | 7 | 2.0 | ||||
| Screen time on weekends | 0.112 | <0.001 | 0.023 | 0.012 | ||||||||||||
| (Friday–Sunday) | ||||||||||||||||
| <2 h/day | 464 | 40.3 | 322 | 41.7 | 142 | 37.5 | 551 | 44.8 | 423 | 48.0 | 128 | 36.7 | ||||
| ≥2 h/day | 672 | 58.4 | 436 | 56.5 | 236 | 62.2 | 660 | 53.7 | 446 | 50.6 | 214 | 61.3 | ||||
| Missing | 15 | 1.3 | 14 | 1.8 | 1 | 0.3 | 19 | 1.5 | 12 | 1.4 | 7 | 2.0 | ||||
| One-Year Follow-Up | Three-Year Follow-Up | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Sample n | Baseline % | Follow-Up % | Unadjusted Change e | Adjusted Differences f (95% CI) | p | Sample n | Baseline % | Follow-Up % | Unadjusted Change e | Adjusted Differences f (95% CI) | p | ||
| Food frequencyb (% eating the right number of servings) | |||||||||||||
| Water (4–8 glasses/day) | 0.467 | 0.767 | |||||||||||
| Comparison | 1308 | 79.2 | 82.7 | 3.5 | 1 | 881 | 79.8 | 81.8 | 2.0 | 1 | |||
| Intervention | 1182 | 76.8 | 84.0 | 7.2 | 1.05 (0.92–1.19) | 769 | 78.8 | 82.7 | 3.9 | 1.02 (0.88–1.20) | |||
| Fruits and Vegetables (≥5 pieces/day) | 0.455 | 0.852 | |||||||||||
| Comparison | 1291 | 29.1 | 26.0 | −3.1 | 1 | 869 | 28.7 | 18.0 | −10.7 | 1 | |||
| Intervention | 1175 | 29.3 | 28.4 | −0.9 | 1.08 (0.87–1.35) | 763 | 30.5 | 18.6 | −11.9 | 0.97 (0.72–1.31) | |||
| Meat (3-4 times/week) | 0.481 | 0.291 | |||||||||||
| Comparison | 1289 | 58.4 | 62.7 | 4.3 | 1 | 868 | 57.0 | 54.3 | −2.8 | 1 | |||
| Intervention | 1174 | 57.8 | 65.3 | 7.5 | 1.05 (0.91–1.22) | 763 | 59.5 | 62.4 | 2.9 | 1.10 (0.92–1.32) | |||
| Occasional sweets (1 time/month) | 0.278 | 0.392 | |||||||||||
| Comparison | 1284 | 54.8 | 61.1 | 6.3 | 1 | 864 | 56.1 | 57.8 | 1.6 | 1 | |||
| Intervention | 1173 | 52.3 | 63.4 | 11.1 | 1.09 (0.93–1.26) | 762 | 51.1 | 57.0 | 5.9 | 1.08 (0.90–1.31) | |||
| Occasionally fried potatoes (1 time/month) | 0.349 | 0.512 | |||||||||||
| Comparison | 1286 | 44.3 | 54.2 | 9.9 | 1 | 866 | 45.5 | 61.4 | 15.9 | 1 | |||
| Intervention | 1173 | 40.8 | 54.0 | 13.2 | 1.08 (0.92–1.28) | 761 | 41.1 | 59.3 | 18.1 | 1.07 (0.87–1.30) | |||
| Food behaviorb (% showing healthy behavior) | |||||||||||||
| Proper breakfast (carbohydrates, dairy and fruits) | 0.330 | 0.650 | |||||||||||
| Comparison | 1295 | 41.5 | 41.3 | −0.2 | 1 | 872 | 40.5 | 36.1 | −4.4 | 1 | |||
| Intervention | 1177 | 39.4 | 42.8 | 3.4 | 1.09 (0.91–1.30) | 766 | 40.7 | 38.3 | −2.5 | 1.05 (0.84–1.32) | |||
| Dinner in front of TV (without screens) | 0.637 | 0.995 | |||||||||||
| Comparison | 1295 | 51.7 | 53.0 | 1.3 | 1 | 872 | 53.6 | 50.1 | −3.5 | 1 | |||
| Intervention | 1177 | 51.7 | 54.9 | 3.2 | 1.04 (0.89–1.21) | 766 | 51.3 | 48.0 | −3.3 | 1.00 (0.82–1.22) | |||
| Eating at school (1 healthy meal/day) | 0.625 | 0.631 | |||||||||||
| Comparison | 1308 | 82.0 | 78.1 | −3.9 | 1 | 881 | 84.3 | 73.3 | −11.0 | 1 | |||
| Intervention | 1181 | 80.5 | 74.3 | −6.2 | 0.97 (0.85–1.10) | 769 | 78.7 | 65.8 | −12.9 | 0.96 (0.82–1.13) | |||
| Not eating alone (better accompanied) | 0.521 | 0.867 | |||||||||||
| Comparison | 1295 | 89.3 | 85.2 | −4.1 | 1 | 872 | 89.0 | 82.6 | −6.4 | 1 | |||
| Intervention | 1177 | 87.8 | 87.1 | −0.7 | 1.04 (0.92–1.17) | 766 | 87.1 | 79.8 | −7.3 | 0.99 (0.85–1.15) | |||
| Global Nutrition Score (% showing > 1 of 9 previous changes) | 0.013 | 0.188 | |||||||||||
| Comparison | 1308 | 40.6 | 881 | 41.1 | |||||||||
| Intervention | 1184 | 45.5 | 772 | 44.3 | |||||||||
| Physical activity c (% practicing physical activity) | |||||||||||||
| Practicing out-of-school physical activity | 0.197 | 0.364 | |||||||||||
| Comparison | 1283 | 77.6 | 79.0 | 1.4 | 1 | 864 | 80.4 | 78.2 | −2.2 | 1 | |||
| Intervention | 1167 | 70.6 | 78.2 | 7.6 | 1.09 (0.96–1.24) | 740 | 71.8 | 75.1 | 3.3 | 1.08 (0.92–1.27) | |||
| Engaging in physical activity in leisure time (≥2 days/week) | 0.409 | 0.689 | |||||||||||
| Comparison | 1281 | 64.3 | 65.7 | 1.4 | 1 | 864 | 63.4 | 72.0 | 8.6 | 1 | |||
| Intervention | 1165 | 65.2 | 70.6 | 5.4 | 1.06 (0.92–1.22) | 733 | 63.7 | 69.9 | 6.1 | 0.97 (0.81–1.15) | |||
| Daily use of screens d (% using <2 h/day) | |||||||||||||
| On Weekdays | 0.290 | 0.089 | |||||||||||
| Comparison | 1279 | 61.1 | 62.9 | 1.8 | 1 | 862 | 63.9 | 56.2 | −7.8 | 1 | |||
| Intervention | 1164 | 57.4 | 63.9 | 6.5 | 1.08 (0.93–1.25) | 728 | 56.7 | 58.4 | 1.7 | 1.17 (0.97–1.41) | |||
| On Weekends | 0.379 | 0.215 | |||||||||||
| Comparison | 1279 | 45.5 | 45.8 | 0.3 | 1 | 863 | 49.0 | 31.6 | −17.4 | 1 | |||
| Intervention | 1164 | 40.7 | 44.2 | 3.5 | 1.08 (0.91–1.28) | 728 | 42.2 | 31.5 | −10.7 | 1.16 (0.91–1.46) | |||
| Global Activity Score (% showing > 1 of 4 previous changes) | 0.009 | 0.012 | |||||||||||
| Comparison | 1308 | 15.4 | 881 | 11.9 | |||||||||
| Intervention | 1184 | 19.3 | 772 | 16.2 | |||||||||
| Global Score (% showing >1 of 13 previous changes) | 0.002 | 0.025 | |||||||||||
| Comparison | 1308 | 59.3 | 881 | 58.5 | |||||||||
| Intervention | 1184 | 65.3 | 772 | 63.9 | |||||||||
| CIR b of Obesity | Difference CIR | Ratio of Incidences d | p | OR (95% CI) e | Effect Size (d Cohen’s) | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Boys | Girls | Total | ||||||||||
| nc | % | nc | % | p | nc | % | ||||||
| Global (1653) | 20/652 | 3.1 | 38/693 | 5.5 | 0.029 | 58/1345 | 4.3 | - | - | - | - | - |
| Comparison group (881) | 10/332 | 3.0 | 18/371 | 4.9 | 0.213 | 28/703 | 4.0 | - | - | - | - | - |
| Intervention group (772) | 10/320 | 3.1 | 20/322 | 6.2 | 0.064 | 30/642 | 4.7 | −0.7 | −17.3 | 0.858 | 0.95 (0.55–1.65) | 0.03 |
| Not acceptable | 7/135 | 5.2 | 10/139 | 7.2 | 0.491 | 17/274 | 6.2 | −2.2 | −55.8 | 0.904 | 1.04 (0.54–2.00) | 0.02 |
| Acceptable intervention group f | 3/115 | 2.6 | 8/126 | 6.4 | 0.165 | 11/241 | 4.6 | −0.6 | −14.6 | 0.745 | 0.89 (0.42–1.85) | 0.07 |
| Qualified intervention group g | 0/70 | 0.0 | 2/57 | 3.5 | 0.114 | 2/127 | 1.6 | 2.4 | 60.5 | 0.107 | 0.30 (0.07–1.30) | 0.67 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sánchez-Martínez, F.; Brugueras, S.; Serral, G.; Valmayor, S.; Juárez, O.; López, M.J.; Ariza, C.; on behalf of the POIBA Project Evaluation Group. Three-Year Follow-Up of the POIBA Intervention on Childhood Obesity: A Quasi-Experimental Study. Nutrients 2021, 13, 453. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13020453
Sánchez-Martínez F, Brugueras S, Serral G, Valmayor S, Juárez O, López MJ, Ariza C, on behalf of the POIBA Project Evaluation Group. Three-Year Follow-Up of the POIBA Intervention on Childhood Obesity: A Quasi-Experimental Study. Nutrients. 2021; 13(2):453. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13020453
Chicago/Turabian StyleSánchez-Martínez, Francesca, Silvia Brugueras, Gemma Serral, Sara Valmayor, Olga Juárez, María José López, Carles Ariza, and on behalf of the POIBA Project Evaluation Group. 2021. "Three-Year Follow-Up of the POIBA Intervention on Childhood Obesity: A Quasi-Experimental Study" Nutrients 13, no. 2: 453. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13020453