
Dairy Consumption and Incidence of Breast Cancer in the ‘Seguimiento Universidad de Navarra’ (SUN) Project

 ,
,  , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
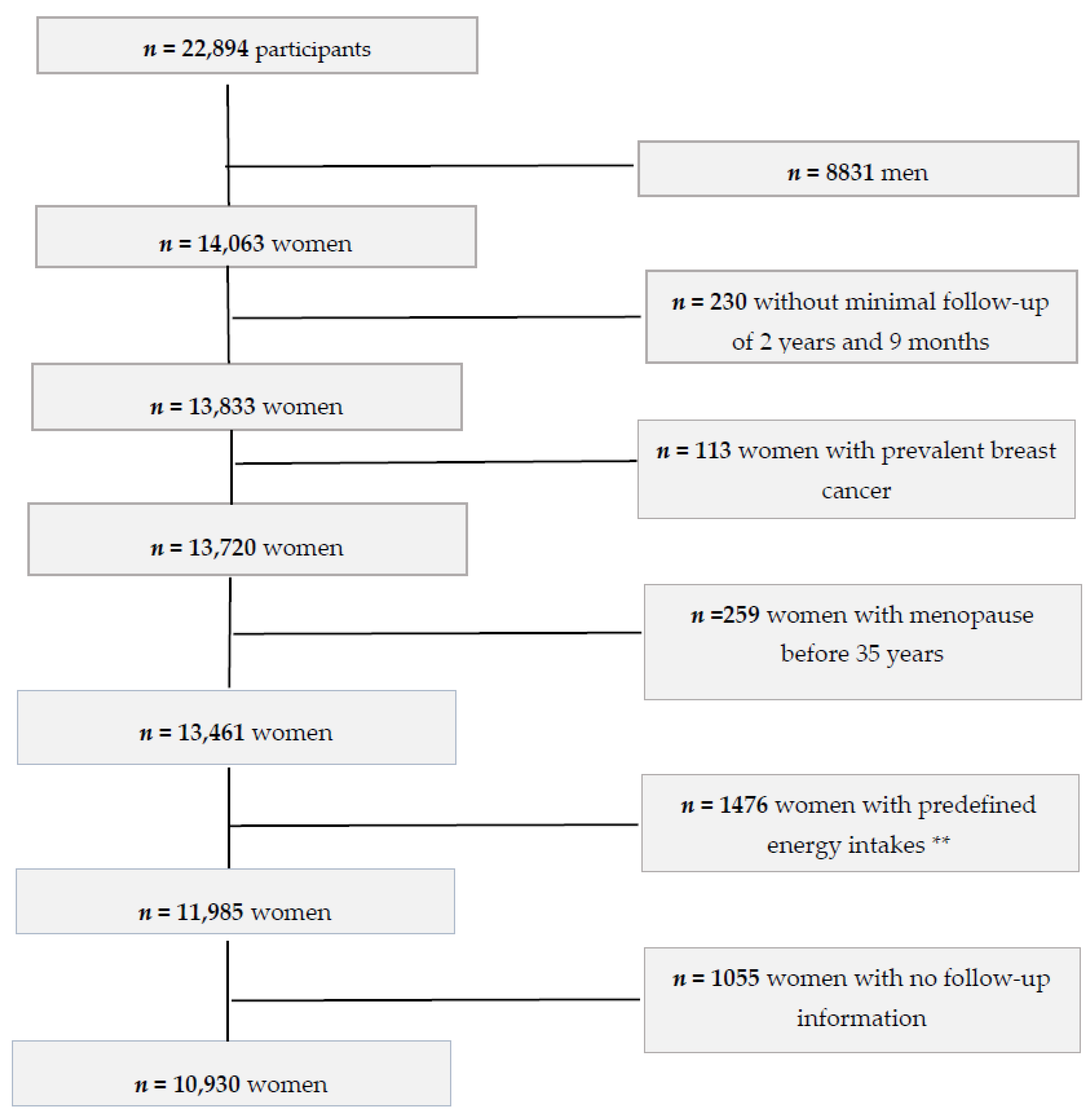
2.1. Study Sample
2.2. Assessment of Dairy Consumption
2.3. Breast Cancer Ascertainment
2.4. Evaluation of Covariates
2.5. Statistical Analysis
3. Results
4. Discussion
4.1. Evidence from Previous Epidemiological Studies
4.2. Biological Mechanisms
4.3. Limitations and Strengths
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization; GLOBOCAN. Cancer Fact Sheets: Breast Cancer. 2018. Available online: http://gco.iarc.fr/today/fact-sheets-cancers (accessed on 12 April 2020).
- Bennett, I.C.; Gattas, M.; Teh, B.T. The genetic basis of breast cancer and its clinical implications. ANZ J. Surg. 1999, 69, 95–105. [Google Scholar] [CrossRef]
- Chan, D.S.M.; Abar, L.; Cariolou, M.; Nanu, N.; Greenwood, D.C.; Bandera, E.V.; McTiernan, A.; Norat, T. World Cancer Research Fund International: Continuous Update Project—Systematic literature review and meta-analysis of observational cohort studies on physical activity, sedentary behavior, adiposity, and weight change and breast cancer risk. Cancer Causes Control. 2019, 30, 1183–1200. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Anderson, K.N.; Schwab, R.B.; Martinez, M.E. Reproductive risk factors and breast cancer subtypes: A review of the literature. Breast Cancer Res. Treat. 2014, 144, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Neuhouser, M.L.; Aragaki, A.K.; Prentice, R.L.; Manson, J.E.; Chlebowski, R.; Carty, C.L.; Ochs-Balcom, H.M.; Thomson, C.A.; Caan, B.J.; Tinker, L.F.; et al. Overweight, Obesity, and Postmenopausal Invasive Breast Cancer Risk: A Secondary Analysis of the Women’s Health Initiative Randomized Clinical Trials. JAMA Oncol. 2015, 1, 611–621. [Google Scholar] [CrossRef]
- Amadou, A.; Ferrari, P.; Muwonge, R.; Moskal, A.; Biessy, C.; Romieu, I.; Hainaut, P. Overweight, obesity and risk of premenopausal breast cancer according to ethnicity: A systematic review and dose-response meta-analysis. Obes. Rev. 2013, 14, 665–678. [Google Scholar] [CrossRef]
- Laudisio, D.; Muscogiuri, G.; Barrea, L.; Savastano, S.; Colao, A. Obesity and breast cancer in premenopausal women: Current evidence and future perspectives. Eur. J. Obstet. Gynecol. Reprod. Biol. 2018, 230, 217–221. [Google Scholar] [CrossRef]
- McPherson, K.; Steel, C.M.; Dixon, J.M. ABC of breast diseases: Breast cancer—Epidemiology, risk factors, and genetics. BMJ 2000, 321, 624–628. [Google Scholar] [CrossRef] [Green Version]
- Moorman, P.G.; Terry, P.D. Consumption of dairy products and the risk of breast cancer: A review of the literature. Am. J. Clin. Nutr. 2004, 80, 5–14. [Google Scholar] [CrossRef] [Green Version]
- Dong, J.-Y.; Zhang, L.; He, K.; Qin, L.-Q. Dairy consumption and risk of breast cancer: A meta-analysis of prospective cohort studies. Breast Cancer Res. Treat. 2011, 127, 23–31. [Google Scholar] [CrossRef]
- Zang, J.; Shen, M.; Du, S.; Chen, T.; Zou, S. The Association between Dairy Intake and Breast Cancer in Western and Asian Populations: A Systematic Review and Meta-Analysis. J. Breast Cancer 2015, 18, 313–322. [Google Scholar] [CrossRef] [Green Version]
- Karkeni, E.; Morin, S.O.; Tayeh, B.B.; Goubard, A.; Josselin, E.; Castellano, R.; Fauriat, C.; Guittard, G.; Olive, D.; Nunès, J.A. Vitamin D Controls Tumor Growth and CD8+ T Cell Infiltration in Breast Cancer. Front. Immunol. 2019, 10, 1307. [Google Scholar] [CrossRef] [Green Version]
- Hossain, S.; Beydoun, M.A.; Beydoun, H.A.; Chen, X.; Zonderman, A.B.; Wood, R.J. Vitamin D and breast cancer: A systematic review and meta-analysis of observational studies. Clin. Nutr. ESPEN 2019, 30, 170–184. [Google Scholar] [CrossRef] [PubMed]
- Song, D.; Deng, Y.; Liu, K.; Zhou, L.; Li, N.; Zheng, Y.; Hao, Q.; Yang, S.; Wu, Y.; Zhai, Z.; et al. Vitamin D intake, blood vitamin D levels, and the risk of breast cancer: A dose-response meta-analysis of observational studies. Aging 2019, 11, 12708–12732. [Google Scholar] [CrossRef] [PubMed]
- Hidayat, K.; Chen, G.C.; Zhang, R.; Du, X.; Zou, S.Y.; Shi, B.M.; Qin, L.Q. Calcium intake and breast cancer risk: Meta-analysis of pro-spective cohort studies. Br. J. Nutr. 2016, 116, 158–166. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kelley, N.S.; Hubbard, N.E.; Erickson, K.L. Conjugated Linoleic Acid Isomers and Cancer. J. Nutr. 2007, 137, 2599–2607. [Google Scholar] [CrossRef] [Green Version]
- Cao, Y.; Hou, L.; Wang, W. Dietary total fat and fatty acids intake, serum fatty acids and risk of breast cancer: A meta-analysis of prospective cohort studies. Int. J. Cancer 2016, 138, 1894–1904. [Google Scholar] [CrossRef]
- Thiébaut, A.C.M.; Kipnis, V.; Chang, S.-C.; Subar, A.F.; Thompson, F.E.; Rosenberg, P.S.; Hollenbeck, A.R.; Leitzmann, M.; Schatzkin, A. Dietary Fat and Postmenopausal Invasive Breast Cancer in the National Institutes of Health-AARP Diet and Health Study Cohort. J. Natl. Cancer Inst. 2007, 99, 451–462. [Google Scholar] [CrossRef]
- Sieri, S.; Krogh, V.; Ferrari, P.; Berrino, F.; Pala, V.; Thiébaut, A.C.M.; Tjønneland, A.; Olsen, A.; Overvad, K.; Jakobsen, M.U.; et al. Dietary fat and breast cancer risk in the European Prospective Investigation into Cancer and Nutrition. Am. J. Clin. Nutr. 2008, 88, 1304–1312. [Google Scholar]
- Murphy, N.; Knuppel, A.; Papadimitriou, N.; Martin, R.; Tsilidis, K.; Smith-Byrne, K.; Fensom, G.; Perez-Cornago, A.; Travis, R.; Key, T.; et al. Insulin-like growth factor-1, insulin-like growth factor-binding protein-3, and breast cancer risk: Observational and Mendelian randomization analyses with ∼430 000 women. Ann. Oncol. 2020, 31, 641–649. [Google Scholar] [CrossRef] [Green Version]
- Zhang, K.; Dai, H.; Liang, W.; Zhang, L.; Deng, Z. Fermented dairy foods intake and risk of cancer. Int. J. Cancer 2019, 144, 2099–2108. [Google Scholar] [CrossRef] [PubMed]
- Marcondes, L.; Franco, O.; Ruiter, R.; Ikram, M.; Mulder, M.; Stricker, B.; Kiefte-de Jong, J. Animal foods and post-menopausal breast cancer risk: A prospective cohort study. Br. J. Nutr. 2019, 122, 583–591. [Google Scholar] [CrossRef]
- Godos, J.; Tieri, M.; Ghelfi, F.; Titta, L.; Marventano, S.; Lafranconi, A.; Gambera, A.; Alonzo, E.; Sciacca, S.; Buscemi, S.; et al. Dairy foods and health: An umbrella review of observational studies. Int. J. Food Sci. Nutr. 2019, 71, 138–151. [Google Scholar] [CrossRef]
- Nilsson, L.M.; Winkvist, A.; Esberg, A.; Jansson, J.-H.; Wennberg, P.; Van Guelpen, B.; Johansson, I. Dairy Products and Cancer Risk in a Northern Sweden Population. Nutr. Cancer 2019, 72, 409–420. [Google Scholar] [CrossRef] [Green Version]
- Genkinger, J.M.; Makambi, K.H.; Palmer, J.R.; Rosenberg, L.; Adams-Campbell, L.L. Consumption of dairy and meat in relation to breast cancer risk in the Black Women’s Health Study. Cancer Causes Control. 2013, 24, 675–684. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fraser, E.G.; Jaceldo-Siegl, K.; Orlich, M.; Mashchak, A.; Sirirat, R.; Knutsen, S. Dairy, soy, and risk of breast cancer: Those confounded milks. Int. J. Epidemiol. 2020, 49, 1526–1537. [Google Scholar] [CrossRef]
- Han, Y.; Zong, X.; Li, Y.; Colditz, G.A.; Toriola, A.T. Milk intake and mammographic density in premenopausal women. Breast Cancer Res. Treat. 2018, 174, 249–255. [Google Scholar] [CrossRef]
- Farvid, M.S.; Eliassen, A.H.; Cho, E.; Chen, W.Y.; Willett, W.C. Dairy Consumption in Adolescence and Early Adulthood and Risk of Breast Cancer. Cancer Epidemiol. Biomark. Prev. 2018, 27, 575–584. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kaluza, J.; Komatsu, S.; Lauriola, M.; Harris, H.R.; Bergkvist, L.; Michaëlsson, K.; Wolk, A. Long-term consumption of non-fermented and fermented dairy products and risk of breast cancer by estrogen receptor status—Population-based prospective cohort study. Clin. Nutr. 2020, 0261. [Google Scholar] [CrossRef]
- Toledo, E.; Salas-Salvadó, J.; Donat-Vargas, C.; Buil-Cosiales, P.; Estruch, R.; Ros, E.; Corella, D.; Fitó, M.; Hu, F.B.; Arós, F.; et al. Mediterranean Diet and Invasive Breast Cancer Risk Among Women at High Cardiovascular Risk in the PREDIMED Trial: A Randomized Clinical Trial. JAMA Intern Med. 2015, 175, 1752–1760. [Google Scholar] [CrossRef]
- Morze, J.; Danielewicz, A.; Przybyłowicz, K.; Zeng, H.; Hoffmann, G.; Schwingshackl, L. An updated systematic review and me-ta-analysis on adherence to mediterranean diet and risk of cancer. Eur. J. Nutr. 2020, 8. [Google Scholar]
- Carlos, S.; De La Fuente-Arrillaga, C.; Bes-Rastrollo, M.; Razquin, C.; Rico-Campà, A.; Martínez-González, M.A.; Ruiz-Canela, M. Mediterranean Diet and Health Outcomes in the SUN Cohort. Nutrients 2018, 10, 439. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Willett, W.C. (Ed.) Issues in analysis and presentation of dietary data. In Nutritional Epidemiology, 3rd ed.; Oxford University Press: New York, NY, USA, 2013; p. 305. [Google Scholar]
- Martin-Moreno, J.M.; Boyle, P.; Gorgojo, L.; Maisonneuve, P.; Fernandez-Rodriguez, J.C.; Salvini, S.; Willett, W.C. Development and Validation of a Food Frequency Questionnaire in Spain. Int. J. Epidemiol. 1993, 22, 512–519. [Google Scholar] [CrossRef]
- Fernandez-Ballarth, J.D.; Pinol, J.L.; Zazpe, I.; Corella, D.; Carrasco, P.; Toledo, E.; Perez-Bauer, M.; Martinez-Gonzalez, M.; Salas-Salvado, J.; Martin-Moreno, J.M. Relative validity of a semi-quantitative food-frequency questionnaire in an elderly Mediterranean population of Spain. Br. J. Nutr. 2010, 103, 1808–1816. [Google Scholar] [CrossRef] [Green Version]
- Bes-Rastrollo, M.; Pérez Valdivieso, J.R.; Sánchez-Villegas, A.; Alonso, A.M.G.M.; Martínez-González, M.A. Validación del peso e índice de masa corporal au-to-declarados de los participantes de una cohorte de graduados universitarios. Rev. Esp. Obes. 2005, 3, 352–358. [Google Scholar]
- Martínez-González, M.A.; López-Fontana, C.; Varo, J.J.; Sánchez-Villegas, A.; Martinez, J.A. Validation of the Spanish version of the physical activity questionnaire used in the Nurses’ Health Study and the Health Professionals’ Follow-up Study. Public Health Nutr. 2005, 8, 920–927. [Google Scholar] [CrossRef]
- Shivappa, N.; Sandin, S.; Löf, M.; Hébert, J.R.; Adami, H.O.; Weiderpass, E. Prospective study of dietary inflammatory index and risk of cancer in Swedish women. Br. J. Cancer. 2015, 113, 1099–1103. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schröder, H.; Fitó, M.; Estruch, R.; Martínez-González, M.A.; Corella, D.; Salas-Salvadó, J.; Lamuela-Raventós, R.M.; Ros, E.; Salaverría, I.; Fiol, M.; et al. A Short Screener Is Valid for Assessing Mediterranean Diet Adherence among Older Spanish Men and Women. J. Nutr. 2011, 141, 1140–1145. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martínez-Gonzalez, M.A.; Fernandez-Jarne, E.; Serrano-Martínez, M.; Wright, M.; Gomez-Gracia, E. Development of a short dietary intake questionnaire for the quantitative estimation of adherence to a cardioprotective Mediterranean diet. Eur. J. Clin. Nutr. 2004, 58, 1550e2. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martínez-Gonzalez, M.A.; García-Arellano, A.; Toledo, E.; Salas-Salvado, J.; Buil- Cosiales, P.; Corella, D.; Covas, M.I.; Schroder, H.; Aros, F.; Gomez-Gracia, E.; et al. A 14-item mediter-ranean diet assessment tool and obesity indexes among high-risk subjects: The PREDIMED trial. PLoS ONE 2012, 7, e43134. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pala, V.; Krogh, V.; Berrino, F.; Sieri, S.; Grioni, S.; Tjønneland, A.; Olsen, A.; Jakobsen, M.U.; Overvad, K.; Clavel-Chapelon, F.; et al. Meat, eggs, dairy products, and risk of breast cancer in the European Prospective Investigation into Cancer and Nutrition (EPIC) cohort. Am. J. Clin. Nutr. 2009, 90, 602–612. [Google Scholar] [CrossRef]
- Kesse-Guyot, E.; Bertrais, S.; Duperray, B.; Arnault, N.; Bar-Hen, A.; Galan, P.; Hercberg, S. Dairy Products, Calcium and the Risk of Breast Cancer: Results of the French SU.VI.MAX Prospective Study. Ann. Nutr. Metab. 2007, 51, 139–145. [Google Scholar] [CrossRef]
- Brinkman, M.; Baglietto, L.; Krishnan, K.; English, D.R.; Severi, G.; Morris, H.A.; Hopper, J.L.; Giles, G.G. Consumption of animal products, their nutrient components and postmeno-pausal circulating steroid hormone concentrations. Eur. J. Clin. Nutr. 2010, 64, 176–183. [Google Scholar] [CrossRef] [PubMed]
- McCullough, M.L.; Rodríguez, C.; Diver, W.R.; Feigelson, H.S.; Stevens, V.L.; Thun, M.J.; Calle, E.E. Dairy, Calcium, and Vitamin D Intake and Postmenopausal Breast Cancer Risk in the Cancer Prevention Study II Nutrition Cohort. Cancer Epidemiol. Biomark. Prev. 2005, 14, 2898–2904. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sellem, L.; Srour, B.; Guéraud, F.; Pierre, F.; Kesse-Guyot, E.; Fiolet, T.; Lavalette, C.; Egnell, M.; Latino-Martel, P.; Fassier, P.; et al. Saturated, mono- and polyunsaturated fatty acid intake and cancer risk: Results from the French prospective cohort NutriNet-Santé. Eur. J. Nutr. 2019, 58, 1515–1527. [Google Scholar] [CrossRef]
- Sieri, S.; Chiodini, P.; Agnoli, C.; Pala, V.; Berrino, F.; Trichopoulou, A.; Benetou, V.; Vasilopoulou, E.; Sánchez, M.J.; Chirlaque, M.D.; et al. Dietary fat intake and development of specific breast cancer subtypes. J. Natl. Cancer Inst. 2014, 106, dju068. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moschos, S.J.; Mantzoros, C.S. The Role of the IGF System in Cancer: From Basic to Clinical Studies and Clinical Applications. Oncology 2002, 63, 317–332. [Google Scholar] [CrossRef]
- Yu, H.; Rohan, T. Role of the Insulin-Like Growth Factor Family in Cancer Development and Progression. JNCI J. Natl. Cancer Inst. 2000, 92, 1472–1489. [Google Scholar] [CrossRef]
- Sergeev, I. Calcium as a mediator of 1,25-dihydroxyvitamin D3-induced apoptosis. J. Steroid Biochem. Mol. Biol. 2004, 89, 419–425. [Google Scholar] [CrossRef] [PubMed]
- Tavera-Mendoza, L.E.; Westerling, T.; Libby, E.; Marusyk, A.; Cato, L.; Cassani, R.; Cameron, L.A.; Ficarro, S.B.; Marto, J.A.; Klawitter, J.; et al. Vitamin D receptor regulates autophagy in the normal mammary gland and in luminal breast cancer cells. Proc. Natl. Acad. Sci. USA 2017, 114, E2186–E2194. [Google Scholar] [CrossRef] [Green Version]
- Bocca, C.; Bozzo, F.; Cannito, S.; Colombatto, S.; Miglietta, A. CLA reduces breast cancer cell growth and invasion through ERalpha and PI3K/Akt pathways. Chem. Biol. Interact. 2010, 5, 183, 187–193. [Google Scholar]
- Guo, J.; Givens, D.I.; Astrup, A.; Bakker, S.J.L.; Goossens, G.H.; Kratz, M.; Marette, A.; Pijl, H.; Soedamah-Muthu, S.S. The Impact of Dairy Products in the Development of Type 2 Diabetes: Where Does the Evidence Stand in 2019? Adv. Nutr. 2019, 10, 1066–1075. [Google Scholar] [CrossRef] [Green Version]
- Eussen, S.J.P.M.; Van Dongen, M.C.J.M.; Wijckmans, N.; Biggelaar, L.D.; Elferink, S.J.W.H.O.; Singh-Povel, C.M.; Schram, M.T.; Sep, S.J.S.; Van Der Kallen, C.J.; Koster, A.; et al. Consumption of dairy foods in relation to impaired glucose metabolism and type 2 diabetes mellitus: The Maastricht Study. Br. J. Nutr. 2016, 115, 1453–1461. [Google Scholar] [CrossRef] [Green Version]
- Eketunde, A.O. Diabetes as a Risk Factor for Breast Cancer. Cureus 2020, 12, e8010. [Google Scholar] [CrossRef]
- Boyle, P.; Boniol, M.; Koechlin, A.; Robertson, C.R.; Valentini, F.; Coppens, K.; Fairley, L.L.; Zheng, T.; Zhang, Y.; Pasterk, M.; et al. Diabetes and breast cancer risk: A meta-analysis. Br. J. Cancer 2012, 107, 1608–1617. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ryu, T.Y.; Park, J.; Scherer, P.E. Hyperglycemia as a Risk Factor for Cancer Progression. Diabetes Metab. J. 2014, 38, 330–336. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Africander, D.; Storbeck, K.-H. Steroid metabolism in breast cancer: Where are we and what are we missing? Mol. Cell. Endocrinol. 2018, 466, 86–97. [Google Scholar] [CrossRef] [PubMed]
- Galceran, J.; Ameijide, A.; Carulla, M.; Mateos, A.; Quirós, J.R.; Rojas, D.; Alemán, A.; Torrella, A.; Chico, M.; Vicente, M.; et al. Cancer incidence in Spain. Clin. Transl. Oncol. 2017, 19, 799–825. [Google Scholar] [CrossRef]
- Willet, W.C. (Ed.) Reproducibility and Validity of Food Frequency Questionnaires. In Nutritional Epidemiology, 3rd ed.; Oxford University Press: New York, NY, USA, 2013; p. 96. [Google Scholar]



{kind=link}
{kind=link}
| Quartiles of Energy Adjusted Dairy Product Consumption | ||||
|---|---|---|---|---|
| Q1 | Q2 | Q3 | Q4 | |
| N | 2733 | 2732 | 2733 | 2732 |
| Median energy-adjusted dairy product consumption (servings/day) | 1.5 | 2.5 | 3.3 | 4.7 |
| Median energy-adjusted dairy product consumption range (servings/day) | ≤2 | 2–3 | 3–4 | ≥4 |
| Median energy-adjusted whole-fat dairy product consumption (servings/day) | 0.4 | 1.0 | 1.6 | 2.8 |
| Median energy-adjusted low-fat dairy product consumption (servings/day) | 0.7 | 0.9 | 1.7 | 3.2 |
| Median energy-adjusted fermented dairy product consumption (servings/day) | 0.5 | 1.0 | 1.5 | 2.6 |
| Median total milk consumption (servings/day) | 0.7 | 1 | 1.3 | 2.5 |
| Median total yogurt consumption (servings/day) | 0.1 | 0.4 | 0.6 | 1 |
| Median total cheese consumption (servings/day) | 0.2 | 0.5 | 0.6 | 0.9 |
| Time of university education (years), mean (SD) | 4.8 (1.3) | 4.9 (1.3) | 4.9 (1.3) | 4.8 (1.4) |
| Age (years), mean (SD) | 35.6 (10.8) | 34.9 (10.5) | 35.0 (10.3) | 35.4 (10.7) |
| Height (cm), mean (SD) | 163.6 (6.1) | 163.7 (6.0) | 163.5 (6.0) | 163.6 (6.1) |
| Body max index (kg/m2), mean (SD) | 22.0 (3.1) | 22. 2 (3.1) | 22.3 (3.0) | 22.4 (3.0) |
| Physical activity (METs-h/week), mean (SD) | 17.7 (19.6) | 17.8 (18.5) | 19.2 (19.3) | 20.4 (21.1) |
| Total energy intake (kcal/day), mean (SD) | 2392 (588) | 2221 (561) | 2256 (562) | 2314 (566) |
| Alcohol intake (g/day), mean (SD) | 4.9 (7.0) | 4.2 (5.8) | 3.7 (5.4) | 3.3 (5.1) |
| Hours/day television watching, mean (SD) | 1.7 (1.3) | 1.6 (1.2) | 1.6 (1.2) | 1.6 (1.2) |
| Sugar-sweetened beverage consumption (%) | ||||
| Never or seldom | 58.5 | 60.2 | 63.3 | 68.3 |
| ≥1 servings/week | 41.5 | 39.8 | 36.7 | 31.6 |
| Age at menarche (%) | ||||
| Early | 1.1 | 1.0 | 1.1 | 1.3 |
| 10–11 years | 17.6 | 19.8 | 18.7 | 20.5 |
| 12–13 years | 55.7 | 54.9 | 55.3 | 53.5 |
| ≥14 years | 25.5 | 25.1 | 24.8 | 24.6 |
| Obstetric history (%) | ||||
| Age <25 years and nulliparous | 18.0 | 18.1 | 17.4 | 17.5 |
| Age ≥25 years and nulliparous | 49.3 | 50.7 | 48.6 | 47.6 |
| First pregnancy before 25 years | 4.5 | 4.1 | 4.8 | 5.1 |
| First pregnancy between 25 and 30 years of age | 14.1 | 13.6 | 15.2 | 14.7 |
| First pregnancy being 30 years old or older | 13.9 | 13.2 | 13.8 | 14.9 |
| Oral contraceptive use (%) | ||||
| No | 97.6 | 97.1 | 97.7 | 97.7 |
| Yes | 2.3 | 2.8 | 2.3 | 2.3 |
| Menopausal status at recruitment (%) | ||||
| Premenopausal (%) | 91.9 | 92.6 | 92.6 | 91.5 |
| Postmenopausal (%) | 8.0 | 7.4 | 7.4 | 8.5 |
| Age at menopause (%) a | ||||
| <50 | 4.1 | 3.8 | 4.1 | 4.5 |
| ≥50 | 3.9 | 3.6 | 3.3 | 3.9 |
| Family history of breast cancer (%) b | ||||
| None | 89.3 | 89.9 | 89.3 | 88.9 |
| Before 45 years | 1.7 | 1.7 | 2.0 | 1.8 |
| After 45 years | 8.9 | 8.4 | 8.6 | 9.3 |
| Hormone replacement therapy (%) c | ||||
| No | 95.9 | 95.9 | 95.2 | 94.1 |
| Yes | 4.1 | 4.1 | 4.8 | 5.9 |
| Time of hormone replacement therapy (years) mean (SD) c | 0.1 (0.9) | 0.1 (0.8) | 0.1 (0.8) | 0.2 (1.1) |
| Breastfeeding (months), mean (SD) | 2.3 (4.9) | 2.2 (4.7) | 2.4 (5.0) | 2.4 (5.1) |
| Smoking status (%) | ||||
| Never | 47.8 | 52.4 | 54.3 | 52.1 |
| Current | 26.5 | 22.7 | 20.7 | 20.8 |
| Former | 25.7 | 25.9 | 24.9 | 27.1 |
| Lifetime tobacco exposure (pack-years), mean (SD) | 4.7 (7.5) | 4.0 (6.9) | 3.9 (6.9) | 4.3 (7.4) |
| Energy-adjusted calcium intake from non-dairy product (mg/day), mean (SD) | 1514 (1774.8) | 1383 (1428.6) | 1394 (1328.2) | 1409(1583.4) |
| Energy-adjusted vitamin D intake from non-dairy product (mg/day), mean (SD) | 6.1(5.1) | 6 (4) | 6 (4.2) | 6 (4.1) |
| Energy-adjusted saturated fat intake from non-dairy product (mg/day), mean (SD) | 23.8 (6.4) | 22.4 (5.2) | 21.3 (5) | 18.9 (5.2) |
| Coffee consumption (servings/day), (%) | ||||
| <1 | 39.7 | 36.0 | 34.0 | 31.6 |
| ≥1 | 60.3 | 63.9 | 65.9 | 68.3 |
| Adherence to Mediterranean diet, mean (SD) d | 3.5 (1.6) | 3.3 (1.6) | 3.4 (1.6) | 3.5 (1.6) |
| Total Dairy Product Consumption | |||||
| Q1 (Ref.) | Q2 | Q3 | Q4 | p for trend | |
| N | 2733 | 2732 | 2733 | 2732 | |
| Median total dairy product consumption | 1.6 | 2.5 | 3.4 | 4.8 | |
| Incident cases | 41 | 23 | 19 | 36 | |
| Person-years of follow-up | 30,609 | 30,506 | 31,368 | 30,811 | |
| Incidence rate/10,000 person-years | 13.39 | 7.53 | 6.05 | 11.68 | |
| Age-adjusted HR (95% CI) | 1.00 (Ref.) | 0.59 (0.35–0.99) | 0.45 (0.26–0.78) | 0.89(0.57–1.39) | 0.665 |
| Multivariable adjusted model 1 | 1.00 (Ref.) | 0.64 (0.37–1.09) | 0.53 (0.28–1.00) | 1.19 (0.61–2.31) | 0.496 |
| Multivariable adjusted model 2 | 1.00 (Ref.) | 0.63 (0.37–1.09) | 0.52 (0.28–0.97) * | 1.17 (0.60–2.30) | 0.523 |
| Repeated measurements | 1.00 (Ref.) | 0.49 (0.28–0.84) ** | 0.49 (0.29–0.84) ** | 0.84 (0.52–1.35) | 0.623 |
| Whole-Fat Dairy Product Consumption | |||||
| Q1 (Ref.) | Q2 | Q3 | Q4 | p for trend | |
| N | 2733 | 2732 | 2733 | 2732 | |
| Median whole-fat dairy product consumption | 0.6 | 1.19 | 1.18 | 3.1 | |
| Incident cases | 29 | 32 | 28 | 30 | |
| Person-years of follow-up | 29,397 | 29,672 | 31,367 | 32,859 | |
| Incidence rate/10,000 person-years | 9.86 | 10.78 | 8.92 | 9.12 | |
| Age-adjusted HR (95% CI) | 1.00 (Ref.) | 1.19 (0.71–1.97) | 1.01 (0.60–1.72) | 1.09 (0.65–1.83) | 0.886 |
| Multivariable adjusted model 1 | 1.00 (Ref.) | 1.27 (0.75–2.15) | 1.08 (0.62–1.88) | 1.11 (0.63–1.95) | 0.912 |
| Multivariable adjusted model 2 | 1.00 (Ref.) | 1.27 (0.75–2.15) | 1.07 (0.61–1.88) | 1.10 (0.66–1.95) | 0.915 |
| Repeated measurements | 1.00 (Ref.) | 1.27 (0.76–2.14) | 1.09 (0.63–1.87) | 1.05 (0.61–1.79) | 0.830 |
| Low-Fat Dairy Product Consumption | |||||
| Q1 (Ref.) | Q2 | Q3 | Q4 | p for trend | |
| N | 2,733 | 2732 | 2,733 | 2732 | |
| Median low-fat dairy product consumption | 0.67 | 0.68 | 1.5 | 3 | |
| Incident cases | 44 | 23 | 24 | 28 | |
| Person-years of follow-up | 33,043 | 30,357 | 29,727 | 29,727 | |
| Incidence rate/10,000 person-years | 13.31 | 7.57 | 8.07 | 9.28 | |
| Age-adjusted HR (95% CI) | 1.00 (Ref.) | 0.57 (0.34–0.95) | 0.58 (0.35–0.96) | 0.63 (0.39–1.03) | 0.113 |
| Multivariable adjusted model 1 | 1.00 (Ref.) | 0.65 (0.39–1.08) | 0.69 (0.40–1.17) | 0.80 (0.44–1.44) | 0.440 |
| Multivariable adjusted model 2 | 1.00 (Ref.) | 0.65 (0.39–1.09) | 0.69 (0.40–1.17) | 0.79 (0.44–1.44) | 0.422 |
| Repeated measurements | 1.00 (Ref.) | 0.58 (0.35–0.95) * | 0.55 (0.32–0.92) * | 0.65 (0.39–1.06) | 0.136 |
| Fermented Dairy Product Consumption | |||||
| Q1 (Ref.) | Q2 | Q3 | Q4 | p for trend | |
| N | 2733 | 2732 | 2733 | 2732 | |
| Median fermented dairy product consumption | 0.5 | 1.04 | 1.6 | 2.6 | |
| Incident cases | 30 | 29 | 33 | 27 | |
| Person-years of follow-up | 31,229 | 30,973 | 30,896 | 30,196 | |
| Incidence rate/10,000 person-years | 9.60 | 9.36 | 10.68 | 8.94 | |
| Age-adjusted HR (95% CI) | 1.00 (Ref.) | 0.99 (0.59–1.65) | 1.08 (0.66–1.78) | 0.91 (0.54–1.53) | 0.746 |
| Multivariable adjusted model 1 | 1.00 (Ref.) | 1.16 (0.68–1.96) | 1.32 (0.77–2.24) | 1.23 (0.68–2.23) | 0.522 |
| Multivariable adjusted model 2 | 1.00 (Ref.) | 1.16 (0.68–1.96) | 1.32 (0.77–2.24) | 1.23 (0.68–2.23) | 0.515 |
| Repeated measurements | 1.00 (Ref.) | 1.09 (0.65–1.85) | 1.06 (0.63–1.79) | 0.99 (0.57–1.72) | 0.841 |
| Total Dairy Product Consumption | |||||
| Q1 (Ref.) | Q2 | Q3 | Q4 | p for trend | |
| N | 2493 | 2493 | 2493 | 2492 | |
| Mean whole-fat dairy product consumption | 1.8 | 2.7 | 3.6 | 4.9 | |
| Incident cases | 20 | 16 | 9 | 22 | |
| Person-years of follow-up | 23,954 | 24,344 | 25,245 | 24,389 | |
| Incidence rate/10,000 person-years | 8.34 | 6.57 | 3.56 | 9.02 | |
| Age-adjusted HR (95% CI) | 1.00 (Ref.) | 0.84 (0.43–1.62) | 0.42 (0.19–0.92) | 1.08 (0.58–1.98) | 0.933 |
| Multivariable adjusted model 1 | 1.00 (Ref.) | 0.88 (0.43–1.77) | 0.50 (0.20–1.27) | 1.37 (0.53–3.51) | 0.447 |
| Multivariable adjusted model 2 | 1.00 (Ref.) | 0.88 (0.43–1.78) | 0.51 (0.20–1.28) | 1.36 (0.53–3.53) | 0.456 |
| Repeated measurements | 1.00 (Ref.) | 0.75 (0.37–1.50) | 0.51 (0.24–1.10) | 1.00 (0.52–1.91) | 0.991 |
| Whole-Fat Dairy Product Consumption | |||||
| Q1 (Ref.) | Q2 | Q3 | Q4 | p for trend | |
| N | 2493 | 2493 | 2493 | 2492 | |
| Mean whole-fat dairy product consumption | 0.6 | 1.2 | 1.8 | 3 | |
| Incident cases | 16 | 14 | 17 | 20 | |
| Person-years of follow-up | 21,544 | 23,533 | 25,522 | 27,332 | |
| Incidence rate/10,000 person-years | 7.42 | 5.94 | 6.66 | 7.31 | |
| Age-adjusted HR (95% CI) | 1.00 (Ref.) | 0.76 (0.37–1.57) | 0.94 (0.47–1.85) | 1.08 (0.56–2.08) | 0.603 |
| Multivariable adjusted model 1 | 1.00 (Ref.) | 0.82 (0.39–1.73) | 0.94 (0.45–1.94) | 1.10 (0.53–2.30) | 0.416 |
| Multivariable adjusted model 2 | 1.00 (Ref.) | 0.82 (0.39–1.73) | 0.94 (0.45–1.94) | 1.11 (0.53–2.31) | 0.423 |
| Repeated measurements | 1.00 (Ref.) | 0.90 (0.43–1.89) | 0.98 (0.49–1.98) | 1.13 (0.57–2.25) | 0.647 |
| Low-Fat Dairy Product Consumption | |||||
| Q1 (Ref.) | Q2 | Q3 | Q4 | p for trend | |
| N | 2493 | 2493 | 2493 | 2492 | |
| Median low-fat dairy product consumption | 0.1 | 1 | 1.7 | 3 | |
| Incident cases | 29 | 9 | 13 | 16 | |
| Person-years of follow-up | 26,719 | 24,414 | 23,747 | 23,052 | |
| Incidence rate/10,000 person-years | 10.85 | 3.68 | 5.47 | 6.94 | |
| Age-adjusted HR (95% CI) | 1.00 (Ref.) | 0.40 (0.19–0.83) | 0.49 (0.25–0.95) | 0.60 (0.32–1.12) | 0.159 |
| Multivariable adjusted model 1 | 1.00 (Ref.) | 0.36 (0.17–0.78) | 0.49 (0.23–0.99) | 0.61 (0.28–1.33) | 0.209 |
| Multivariable adjusted model 2 | 1.00 (Ref.) | 0.36 (0.17–0.78) * | 0.49 (0.23–0.99) * | 0.61 (0.28–1.33) | 0.207 |
| Repeated measurements | 1.00 (Ref.) | 0.26 (0.11–0.59) ** | 0.48 (0.25–0.92) * | 0.55 (0.28–1.07) | 0.198 |
| Fermented Dairy Product Consumption | |||||
| Q1 (Ref.) | Q2 | Q3 | Q4 | p for trend | |
| N | 2493 | 2493 | 2493 | 2492 | |
| Median fermented dairy product | 0.6 | 1 | 1.7 | 2.7 | |
| Incident cases | 16 | 13 | 23 | 15 | |
| Person-years of follow-up | 24,455 | 25,100 | 24,333 | 24,044 | |
| Incidence rate/10,000 person-years | 6.54 | 5.17 | 9.45 | 6.23 | |
| Age-adjusted HR (95% CI) | 1.00 (Ref.) | 0.80 (0.38–1.67) | 1.37 (0.72–2.60) | 0.90 (0.44–1.82) | 0.995 |
| Multivariable adjusted model 1 | 1.00 (Ref.) | 0.86 (0.40–1.88) | 1.56 (0.78–3.13) | 1.13 (0.51–2.53) | 0.555 |
| Multivariable adjusted model 2 | 1.00 (Ref.) | 0.87 (0.41–1.83) | 1.56 (0.78–3.13) | 1.13 (0.51–2.53) | 0.552 |
| Repeated measurements | 1.00 (Ref.) | 0.88 (0.41–1.86) | 1.41 (0.71–2.80) | 0.89 (0.43–1.88) | 0.970 |
| Total Dairy Product Consumption | |||||
| Q1 (Ref.) | Q2 | Q3 | Q4 | p for trend | |
| N | 825 | 825 | 825 | 824 | |
| Median dairy product | 1.7 | 2.6 | 3.6 | 5 | |
| Incident cases | 15 | 10 | 7 | 11 | |
| Person-years of follow-up | 5938 | 5252 | 5403 | 5891 | |
| Incidence rate/10,000 person-years | 30.31 | 13.32 | 12.95 | 18.67 | |
| Age-adjusted HR (95% CI) | 1.00 (Ref.) | 0.38 (0.15–0.91) | 0.37 (0.15–0.89) | 0.58 (0.27–1.24) | 0.178 |
| Multivariable adjusted model 1 | 1.00 (Ref.) | 0.37 (0.16–0.86) | 0.34 (0.13–0.89) | 0.59 (0.20–1.75) | 0.484 |
| Multivariable adjusted model 2 | 1.00 (Ref.) | 0.36 (0.15–0.88) * | 0.33 (0.13–0.88) * | 0.57 (0.19–1.74) | 0.462 |
| Repeated measurements | 1.00 (Ref.) | 0.28 (0.10–0.76) * | 0.42 (0.18–0.96) * | 0.59 (0.26–1.34) | 0.283 |
| Whole-Fat Dairy Product Consumption | |||||
| Q1 (Ref.) | Q2 | Q3 | Q4 | p for trend | |
| N | 825 | 825 | 825 | 824 | |
| Median whole-fat dairy | 0.5 | 1 | 1.6 | 2.9 | |
| Incident cases | 10 | 15 | 9 | 9 | |
| Person-years of follow-up | 7164 | 5578 | 5078 | 4664 | |
| Incidence rate/10,000 person-years | 16.74 | 23.30 | 19.69 | 17.15 | |
| Age-adjusted HR (95% CI) | 1.00 (Ref.) | 1.55 (0.69–3.46) | 0.94 (0.38–2.33) | 0.98 (0.39–2.44) | 0.666 |
| Multivariable adjusted model 1 | 1.00 (Ref.) | 1.62 (0.70–3.75) | 1.20 (0.47–3.06) | 0.87 (0.31–2.37) | 0.394 |
| Multivariable adjusted model 2 | 1.00 (Ref.) | 1.60 (0.69–3.72) | 1.18 (0.46–3.02) | 0.85 (0.31–2.34) | 0.371 |
| Repeated measurements | 1.00 (Ref.) | 1.49 (0.69–3.21) | 1.20 (0.47–3.07) | 0.70 (0.27–1.84) | 0.338 |
| Low-Fat Dairy Product Consumption | |||||
| Q1 (Ref.) | Q2 | Q3 | Q4 | p for trend | |
| N | 825 | 825 | 825 | 824 | |
| Median low-fat dairy | 0.1 | 1 | 2 | 3.4 | |
| Incident cases | 13 | 11 | 11 | 8 | |
| Person-years of follow-up | 5396 | 5175 | 5367 | 6546 | |
| Incidence rate/10,000 person-years | 24.09 | 21.25 | 16.76 | 15.27 | |
| Age-adjusted HR (95% CI) | 1.00 (Ref.) | 0.85 (0.39–1.88) | 0.62 (0.26–1.47) | 0.58 (0.24–1.39) | 0.186 |
| Multivariable adjusted model 1 | 1.00 (Ref.) | 1.12 (0.48–2.56) | 1.01 (0.40–2.53) | 1.13 (0.40–3.17) | 0.848 |
| Multivariable adjusted model 2 | 1.00 (Ref.) | 1.13 (0.49–2.59) | 1.01 (0.40–2.54) | 1.12 (0.40–3.15) | 0.830 |
| Repeated measurements | 1.00 (Ref.) | 1.19 (0.51–2.78) | 0.60 (0.22–1.66) | 0.83 (0.36–1.93) | 0.443 |
| Fermented Dairy Product Consumption | |||||
| Q1 (Ref.) | Q2 | Q3 | Q4 | p for trend | |
| N | 825 | 825 | 825 | 824 | |
| Median fermented dairy | 0.6 | 1 | 1.7 | 2.8 | |
| Incident cases | 12 | 12 | 9 | 10 | |
| Person-years of follow-up | 5980 | 5152 | 5745 | 5607 | |
| Incidence rate/10,000 person-years | 20.06 | 23.28 | 15.66 | 17.83 | |
| Age-adjusted HR (95% CI) | 1.00 (Ref.) | 0.95 (0.42–2.12) | 0.70 (0.29–1.66) | 0.81 (0.34–1.88) | 0.555 |
| Multivariable adjusted model 1 | 1.00 (Ref.) | 1.34 (0.38–3.10) | 0.96 (0.38–2.44) | 1.24 (0.47–3.25) | 0.855 |
| Multivariable adjusted model 2 | 1.00 (Ref.) | 1.33 (0.58–3.09) | 0.96 (0.38–2.44) | 1.24 (0.46–3.26) | 0.848 |
| Repeated measurements | 1.00 (Ref.) | 1.20 (0.53–2.76) | 0.64 (0.25–1.62) | 1.07 (0.43–2.63) | 0.856 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Aguilera-Buenosvinos, I.; Fernandez-Lazaro, C.I.; Romanos-Nanclares, A.; Gea, A.; Sánchez-Bayona, R.; Martín-Moreno, J.M.; Martínez-González, M.Á.; Toledo, E. Dairy Consumption and Incidence of Breast Cancer in the ‘Seguimiento Universidad de Navarra’ (SUN) Project. Nutrients 2021, 13, 687. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13020687
Aguilera-Buenosvinos I, Fernandez-Lazaro CI, Romanos-Nanclares A, Gea A, Sánchez-Bayona R, Martín-Moreno JM, Martínez-González MÁ, Toledo E. Dairy Consumption and Incidence of Breast Cancer in the ‘Seguimiento Universidad de Navarra’ (SUN) Project. Nutrients. 2021; 13(2):687. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13020687
Chicago/Turabian StyleAguilera-Buenosvinos, Inmaculada, Cesar Ignacio Fernandez-Lazaro, Andrea Romanos-Nanclares, Alfredo Gea, Rodrigo Sánchez-Bayona, Jose M. Martín-Moreno, Miguel Ángel Martínez-González, and Estefanía Toledo. 2021. "Dairy Consumption and Incidence of Breast Cancer in the ‘Seguimiento Universidad de Navarra’ (SUN) Project" Nutrients 13, no. 2: 687. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13020687