
Effect of a Low-Glycemic Load Diet Intervention on Maternal and Pregnancy Outcomes in Obese Pregnant Women

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
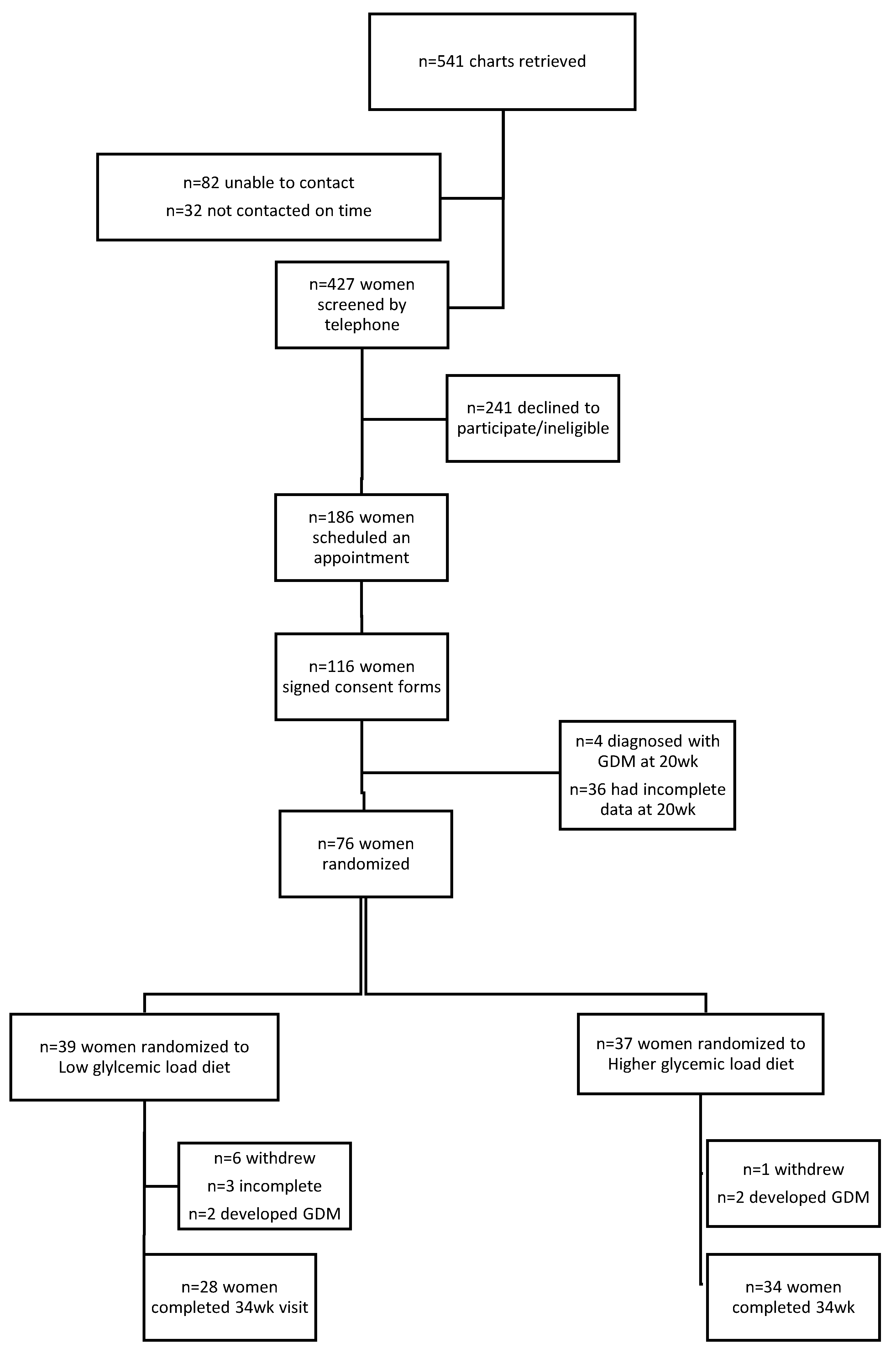
2.1. Study Design and Population
2.2. Dietary Intervention
2.3. Outcome Measurements
2.3.1. Maternal Anthropometrics and Body Composition:
2.3.2. Oral Glucose Tolerance Test, Blood Sampling, and Analysis
2.3.3. Pregnancy Outcomes
2.3.4. Data from the Control Cohort
2.4. Statistical Analyses
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Stotland, N.E.; Hopkins, L.M.; Caughey, A.B. Gestational Weight Gain, Macrosomia, and Risk of Cesarean Birth in Nondiabetic Nulliparas. Obstet. Gynecol. 2004, 104, 671–677. [Google Scholar] [CrossRef]
- Jain, N.J.; Denk, C.E.; Kruse, L.K.; Dandolu, V. Maternal Obesity: Can Pregnancy Weight Gain Modify Risk of Selected Adverse Pregnancy Outcomes? Am. J. Perinatol. 2007, 24, 291–298. [Google Scholar] [CrossRef]
- Potti, S.; Sliwinski, C.S.; Jain, N.J.; Dandolu, V. Obstetric Outcomes in Normal Weight and Obese Women in Relation to Gestational Weight Gain: Comparison between Institute of Medicine Guidelines and Cedergren Criteria. Am. J. Perinatol. 2009, 27, 415–420. [Google Scholar] [CrossRef]
- Kc, K.; Shakya, S.; Zhang, H. Gestational Diabetes Mellitus and Macrosomia: A Literature Review. Ann. Nutr. Metab. 2015, 66, 14–20. [Google Scholar] [CrossRef]
- Poston, L.; Caleyachetty, R.; Cnattingius, S.; Corvalán, C.; Uauy, R.; Herring, S.; Gillman, M.W. Preconceptional and maternal obesity: Epidemiology and health consequences. Lancet Diabetes Endocrinol. 2016, 4, 1025–1036. [Google Scholar] [CrossRef]
- Driscoll, A.K.; Gregory, E.C. Increases in prepregnancy obesity: United States, 2016–2019. In NCHS Data Brief; National Center for Health Statistics: Hyattsville, MD, USA, 2020. [Google Scholar]
- Snowden, J.M.; Mission, J.F.; Marshall, N.E.; Quigley, B.; Main, E.; Gilbert, W.M.; Chung, J.H.; Caughey, A.B. The Impact of maternal obesity and race/ethnicity on perinatal outcomes: Independent and joint effects. Obesity 2016, 24, 1590–1598. [Google Scholar] [CrossRef]
- Buchanan, T.A.; Xiang, A.H. Gestational diabetes mellitus. J. Clin. Investig. 2005, 115, 485–491. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Homko, C.J.; Sivan, E.; Reece, E.A.; Boden, G. Fuel Metabolism During Pregnancy. Semin. Reprod. Med. 1999, 17, 119–125. [Google Scholar] [CrossRef]
- Zeng, Z.; Liu, F.; Li, S. Metabolic Adaptations in Pregnancy: A Review. Ann. Nutr. Metab. 2017, 70, 59–65. [Google Scholar] [CrossRef] [PubMed]
- Catalano, P.M.; Shankar, K. Obesity and pregnancy: Mechanisms of short term and long term adverse consequences for mother and child. BMJ 2017, 356, j1. [Google Scholar] [CrossRef] [PubMed]
- Augustin, L.; Kendall, C.; Jenkins, D.; Willett, W.; Astrup, A.; Barclay, A.; Björck, I.; Brand-Miller, J.; Brighenti, F.; Buyken, A.; et al. Glycemic index, glycemic load and glycemic response: An International Scientific Consensus Summit from the International Carbohydrate Quality Consortium (ICQC). Nutr. Metab. Cardiovasc. Dis. 2015, 25, 795–815. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barclay, A.W.; Petocz, P.; McMillan-Price, J.; Flood, V.M.; Prvan, T.; Mitchell, P.; Brand-Miller, J.C. Glycemic index, glycemic load, and chronic disease risk—A meta-analysis of observational studies. Am. J. Clin. Nutr. 2008, 87, 627–637. [Google Scholar] [CrossRef]
- Livesey, G.; Taylor, R.; Livesey, H.; Liu, S. Is there a dose-response relation of dietary glycemic load to risk of type 2 diabetes? Meta-analysis of prospective cohort studies. Am. J. Clin. Nutr. 2013, 97, 584–596. [Google Scholar] [CrossRef] [Green Version]
- Livesey, G.; Taylor, R.; Livesey, H.F.; Buyken, A.E.; Jenkins, D.J.A.; Augustin, L.S.A.; Sievenpiper, J.L.; Barclay, A.W.; Liu, S.; Wolever, T.M.S.; et al. Dietary Glycemic Index and Load and the Risk of Type 2 Diabetes: A Systematic Review and Updated Meta-Analyses of Prospective Cohort Studies. Nutrients 2019, 11, 1280. [Google Scholar] [CrossRef] [Green Version]
- Livesey, G.; Taylor, R.; Livesey, H.F.; Buyken, A.E.; Jenkins, D.J.A.; Augustin, L.S.A.; Sievenpiper, J.L.; Barclay, A.W.; Liu, S.; Wolever, T.M.S.; et al. Dietary Glycemic Index and Load and the Risk of Type 2 Diabetes: Assessment of Causal Relations. Nutrients 2019, 11, 1436. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, R.; Han, S.; Chen, G.-C.; Li, Z.-N.; Silva-Zolezzi, I.; Parés, G.V.; Wang, Y.; Qin, L.-Q. Effects of low-glycemic-index diets in pregnancy on maternal and newborn outcomes in pregnant women: A meta-analysis of randomized controlled trials. Eur. J. Nutr. 2016, 57, 167–177. [Google Scholar] [CrossRef] [PubMed]
- Bronstein, M.N.; Mak, R.P.; King, J.C. The thermic effect of food in normal-weight and overweight pregnant women. Br. J. Nutr. 1995, 74, 261–275. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maslova, E.; Hansen, S.; Grunnet, L.G.; Strøm, M.; Bjerregaard, A.A.; Hjort, L.; Kampmann, F.B.; Madsen, C.M.; Thuesen, A.C.B.; Bech, B.H.; et al. Maternal glycemic index and glycemic load in pregnancy and offspring metabolic health in childhood and adolescence—A cohort study of 68,471 mother–Offspring dyads from the Danish National Birth Cohort. Eur. J. Clin. Nutr. 2019, 73, 1049–1062. [Google Scholar] [CrossRef]
- Knudsen, V.K.; Heitmann, B.L.; Halldorsson, T.I.; Sørensen, T.I.A.; Olsen, S.F. Maternal dietary glycaemic load during pregnancy and gestational weight gain, birth weight and postpartum weight retention: A study within the Danish National Birth Cohort. Br. J. Nutr. 2013, 109, 1471–1478. [Google Scholar] [CrossRef] [Green Version]
- Van Raaij, J.M.; Peek, M.E.; Vermaat-Miedema, S.H.; Schonk, C.M.; Hautvast, J.G. New equations for estimating body fat mass in pregnancy from body density or total body water. Am. J. Clin. Nutr. 1988, 48, 24–29. [Google Scholar] [CrossRef]
- Matthews, D.R.; Hosker, J.P.; Rudenski, A.S.; Naylor, B.A.; Treacher, D.F.; Turner, R.C. Homeostasis model assessment: Insulin resistance and beta-cell function from fasting plasma glucose and insulin concentrations in man. Diabetologia 1985, 28, 412–419. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Matsuda, M.; DeFronzo, R.A. Insulin sensitivity indices obtained from oral glucose tolerance testing: Comparison with the euglycemic insulin clamp. Diabetes Care 1999, 22, 1462–1470. [Google Scholar] [CrossRef]
- McAuley, K.A.; Williams, S.M.; Mann, J.I.; Walker, R.J.; Lewis-Barned, N.J.; Temple, L.A.; Duncan, A.W. Diagnosing Insulin Resistance in the General Population. Diabetes Care 2001, 24, 460–464. [Google Scholar] [CrossRef] [Green Version]
- Biondi-Zoccai, G.; Romagnoli, E.; Agostoni, P.; Capodanno, D.; Castagno, D.; D’Ascenzo, F.; Sangiorgi, G.; Modena, M.G. Are propensity scores really superior to standard multivariable analysis? Contemp. Clin. Trials 2011, 32, 731–740. [Google Scholar] [CrossRef] [Green Version]
- Shah, B.R.; Laupacis, A.; Hux, J.E.; Austin, P.C. Propensity score methods gave similar results to traditional regression modeling in observational studies: A systematic review. J. Clin. Epidemiol. 2005, 58, 550–559. [Google Scholar] [CrossRef] [PubMed]
- American College of Obstetricians and Gynecologists. ACOG Committee opinion no. 548: Weight gain during pregnancy. Obstet. Gynecol. 2013, 121, 210–212. [Google Scholar] [CrossRef] [PubMed]
- Louie, J.C.Y.; Markovic, T.P.; Perera, N.; Foote, D.; Petocz, P.; Ross, G.P.; Brand-Miller, J.C. A Randomized Controlled Trial Investigating the Effects of a Low-Glycemic Index Diet on Pregnancy Outcomes in Gestational Diabetes Mellitus. Diabetes Care 2011, 34, 2341–2346. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Markovic, T.P.; Muirhead, R.; Overs, S.; Ross, G.P.; Louie, J.C.Y.; Kizirian, N.; Denyer, G.; Petocz, P.; Hyett, J.; Brand-Miller, J.C. Randomized Controlled Trial Investigating the Effects of a Low–Glycemic Index Diet on Pregnancy Outcomes in Women at High Risk of Gestational Diabetes Mellitus: The GI Baby 3 Study. Diabetes Care 2015, 39, 31–38. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rhodes, E.T.; Pawlak, D.B.; Takoudes, T.C.; Ebbeling, C.B.; A Feldman, H.; Lovesky, M.M.; A Cooke, E.; Leidig, M.M.; Ludwig, D.S. Effects of a low–glycemic load diet in overweight and obese pregnant women: A pilot randomized controlled trial. Am. J. Clin. Nutr. 2010, 92, 1306–1315. [Google Scholar] [CrossRef] [Green Version]
- Food and Nutrition Service; U.S. Department of Agriculture. Special Supplemental Nutrition Program for Women, Infants, and Children (WIC). Available online: https://wwwfnsusdagov/wic (accessed on 17 November 2020).
- Clapp, J.F., 3rd. Effect of dietary carbohydrate on the glucose and insulin response to mixed caloric intake and exercise in both nonpregnant and pregnant women. Diabetes Care 1998, 21 (Suppl. 2), B107-12. [Google Scholar]
- Walsh, J.M.; Mahony, R.M.; Culliton, M.; Foley, M.E.; McAuliffe, F.M. Impact of a Low Glycemic Index Diet in Pregnancy on Markers of Maternal and Fetal Metabolism and Inflammation. Reprod. Sci. 2014, 21, 1378–1381. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Low-GL Group (n = 28) | Higher GL Group (n = 34) | p for Difference 1 | |||
|---|---|---|---|---|---|
| n | Mean (SD)/Median (25th, 75h Percentile) | n | Mean (SD)/Median (25th, 75h Percentile) | ||
| Age, years | 28 | 29.3 (5.20) | 34 | 28.3 (6.00) | 0.5 |
| BMI study baseline, kg/m2 | 28 | 33.1 (6.26) | 34 | 32.2 (4.13) | 0.5 |
| Gravida | 28 | 2 (1.5,4) | 34 | 3 (2,4) | 0.7 |
| Parity | 21 | 2 (1,2) | 29 | 1 (1,2) | 0.2 |
| Ethnicity n (%) | 28 | 34 | 0.2 | ||
| Hispanic | 22 (78.6%) | 22 (64.7%) | |||
| African American | 3 (10.7%) | 8 (23.5%) | |||
| Caucasian | 0 (0%) | 3 (8.8%) | |||
| Asian | 0 (0%) | 0 (0%) | |||
| Hawaiian/Pacific Islanders | 1 (3.6%) | 0 (0%) | |||
| Mixed ethnicity | 2 (7.1%) | 1 (2.9%) | |||
| Family history of diabetes, n (%) | 28 | 16 (57.1%) | 34 | 15 (44.1%) | 0.4 |
| Low-GL Group (n = 28) Mean (SD) | Higher GL Group (n = 34) Mean (SD) | p for Difference 2 | |
|---|---|---|---|
| Energy, kcal | 1460 (208) | 1817 (361) | <0.0001 |
| Carbohydrate, en% 3 | 53.3 (6.14) | 55.1 (6.42) | 0.3 |
| Fat, en% 3 | 27.2 (6.08) | 26.3 (5.90) | 0.5 |
| Protein, en% 3 | 19.2 (2.66) | 18.5 (3.52) | 0.4 |
| Total sugars, g | 88.8 (21.0) | 113.0 (34.7) | 0.002 |
| Total dietary fiber, g | 23.6 (8.05) | 22.4 (6.43) | 0.5 |
| Soluble fiber, g | 6.70 (2.50) | 6.46 (2.22) | 0.7 |
| Insoluble fiber, g | 16.9 (6.05) | 15.9 (4.87) | 0.5 |
| Total whole grain, g | 2.25 (1.36) | 2.48 (1.83) | 0.6 |
| Dietary GI | 53.5 (3.58) | 55.7 (3.04) | 0.01 |
| Dietary GL (g) | 95.1 (15.9) | 130.9 (31.8) | <0.0001 |
| GL, (g/1000 kcal) | 65.4 (8.14) | 72.1 (10.8) | 0.009 |
| Low-GL Group | Higher-GL Group | Mean between-Group Difference (95% CI) 1 | p | |||
|---|---|---|---|---|---|---|
| n | Mean (SD)/Median (25th, 75h Percentile) | n | Mean (SD)/Median (25th, 75h Percentile) | |||
| Maternal metabolic parameters | ||||||
| Fasting glucose (mg/dL) | ||||||
| gw 20 | 27 | 79.4 (5.50) | 33 | 81.1 (5.50) | 1.67 (−4.53; 1.19) | 0.2 |
| gw 28 | 25 | 81.1 (7.89) | 34 | 82.7 (6.66) | −1.66 (−5.46; 2.14) | 0.4 |
| gw 34 | 25 | 81.2 (7.29) | 34 | 82.5 (8.15) | −1.31 (−5.42; 2.81) | 0.5 |
| mean change | 25 | 1.90 (−2.10; 5.80) | 33 | 1.2 (−4.0; 3.8) | 0.44 (−3.37; 4.24) | 0.5 |
| Glucose 3h-iAUC (mg/dL/min) | ||||||
| gw 20 | 27 | 5904 (4101; 8358) | 33 | 6551 (4899; 8712) | −376 (−1792; 1040) | 0.6 |
| gw 28 | 25 | 7239 (6201; 8984) | 32 | 6394 (5022; 8533) | 752 (−418; 1923) | 0.3 |
| gw 34 | 25 | 7161 (5703; 9933) | 33 | 8051 (6002; 10266) | −148 (−1685; 1389) | 0.8 |
| mean change | 25 | 2037 (647; 3108) | 32 | 1232 (−467; 2552) | 482 (−1152; 2120) | 0.6 |
| Fasting Insulin (μU/mL) | ||||||
| gw 20 | 27 | 14.6 (8.1; 20.2) | 33 | 13.1 (8.3; 18.5) | 1.64 (−2.37; 5.66) | 0.5 |
| gw 28 | 25 | 18.2 (12.1; 22.2) | 34 | 14.5 (10.0; 20.3) | 2.83 (−2.26; 7.92) | 0.16 |
| gw 34 | 25 | 20.6 (14.5; 25.1) | 34 | 16.0 (12.5; 23.6) | 0.91 (−6.12; 7.94) | 0.3 |
| mean change | 25 | 4.4 (1.4; 11.3) | 33 | 4.4 (0.2; 6.2) | −0.48 (−6.14; 5.18) | 0.7 |
| Insulin 3h-iAUC (μU/mL/min) | ||||||
| gw 20 | 27 | 10421 (6846; 19130) | 33 | 10925 (8523; 13941) | −545 (−6187; 5096) | 0.8 |
| gw 28 | 25 | 15972 (8865; 19245) | 33 | 10269 (8910; 13994) | 3893 (−357; 8143) | 0.07 |
| gw 34 | 25 | 17828 (12360; 26306) | 33 | 14178 (10829; 18116) | 5346 (−4105; 14796) | 0.3 |
| mean change | 25 | 6137 (677; 13281) | 32 | 4167 (933; 6097) | 705 (−569; 14266) | 0.1 |
| HOMA-IR2 | ||||||
| gw 20 | 27 | 2.98 (1.49; 3.96) | 34 | 2.61 (1.42; 3.71) | 0.36 (−0.53; 1.25) | 0.5 |
| gw 28 | 28 | 3.18 (2.07; 4.54) | 34 | 2.92 (1.93; 4.66) | 0.08 (−1.11; 1.26) | 0.8 |
| gw 34 | 28 | 3.63 (2.32; 5.05) | 34 | 3.27 (2.50; 4.85) | −0.37 (−2.02; 1.28) | 1.0 |
| mean change | 27 | 0.73 (−0.17; 2.34) | 34 | 1.09 (0.16; 1.60) | −0.59 (−2.00; 0.82) | 0.6 |
| Matsuda Index3 | ||||||
| gw 20 | 27 | 2.82 (2.04; 5.49) | 33 | 3.22 (2.40; 4.33) | 0.24 (−0.83; 1.31) | 0.9 |
| gw 28 | 25 | 2.17 (1.80; 3.54) | 33 | 2.84 (2.22; 3.85) | −0.34 (−1.11; 0.43) | 0.07 |
| gw 34 | 25 | 1.78 (1.54; 2.97) | 33 | 1.75 (2.30; 2.97) | 0.20 (−0.81; 0.41) | 0.3 |
| mean change | 25 | −1.33 (−2.95; −0.43) | 32 | −1.02 (−1.37; −0.42) | −0.64 (−1.49; 0.21) | 0.3 |
| McAuley-Index4 | ||||||
| gw 20 | 27 | 1.49 (0.39) | 33 | 1.57 (0.34) | −0.08 (−0.27; 0.11) | 0.4 |
| gw 28 | 25 | 1.32 (0.40) | 34 | 1.40 (0.24) | −0.08 (−0.25; 0.08) | 0.3 |
| gw 34 | 25 | 1.22 (0.30) | 34 | 1.28 (0.25) | −0.06 (−0.20; 0.09) | 0.4 |
| mean change | 25 | −0.28 (−0.42; −0.13) | 33 | −0.24 (−0.41; −0.12) | 0.02 (−0.10; 0.15) | 0.9 |
| Maternal anthropometric parameters | ||||||
| Gestational weight gain (between gw 20 and gw34) (kg) | ||||||
| 26 | 5.65 (3.10; 7.50) | 33 | 5.67 (3.60; 8.55) | −1.10 (−2.89; 0.68) | 0.4 | |
| Excess gestational weight gain, n (%) 5 | ||||||
| 26 | 18 (69.2%) | 33 | 24 (72.7%) | - | 0.8 | |
| Maternal fat mass (%) | ||||||
| gw 20 | 28 | 39.57 (6.62) | 34 | 40.04 (5.12) | −0.47 (−3.45; 2.51) | 0.8 |
| gw 28 | 27 | 39.57 (5.76) | 33 | 39.26 (4.97) | 0.31 (−2.46; 3.08) | 0.8 |
| gw 34 | 26 | 38.88 (6.75) | 33 | 38.55 (4.54) | 0.33 (−2.62; 3.28) | 0.8 |
| mean change | 26 | −1.70 (−2.71; 0.53) | 33 | −1.26 (−2.84; 0.80) | 0.27 (−1.09; 1.63) | 0.7 |
| Pregnancy outcomes | ||||||
| Gender (female) | ||||||
| 28 | 15 (53.6%) | 33 | 17 (51.5%) | - | 0.9 | |
| Gestational age (week) | ||||||
| 28 | 38.7 (1.65) | 33 | 39.1 (1.43) | −0.39 (−1.18; 0.40) | 0.3 | |
| Birth weight (g) | ||||||
| 28 | 3383 (430) | 33 | 3370 (458) | 12.97 (−216; 242) | 0.9 | |
| Birth Length (cm) | ||||||
| 28 | 50.65 (2.14) | 32 | 51.30 (1.96) | −0.66 (−1.72; 0.41) | 0.2 | |
| Head circumference (cm) | ||||||
| 22 | 34.7 (1.30) | 26 | 34.3 (1.88) | 0.45 (−0.51; 1.40) | 0.3 | |
| Appropriate for gestational age, n (%) | ||||||
| 28 | 17 (60.7%) | 33 | 27 (81.8%) | - | 0.2 | |
| Cesarean section, n (%) | ||||||
| 28 | 5 (17.9%) | 30 | 8 (26.7%) | - | 0.4 | |
| Pregnancy complications, n (%) | ||||||
| 26 | 4 (15.4%) | 27 | 5 (18.5%) | - | 0.5 | |
| ß | 95% CI | p | |
|---|---|---|---|
| Maternal metabolic measurements | |||
| Fasting glucose (mg/dL) | 0.6867 | −0.6236; 1.9970 | 0.3 |
| Glucose 3h-iAUC | 155.64 | −401.37; 712.65 | 0.6 |
| Fasting Insulin (μU/mL) 1 | −0.00539 | −0.1161; 0.1053 | 0.9 |
| Insulin 3h-iAUC 1 | 391.99 | −2111.96; 2895.93 | 0.8 |
| HOMA-IR 1 | 0.002501 | −0.1183; 0.1233 | 0.9 |
| Matsuda Index × | −0.01184 | −0.1292; 0.1055 | 0.8 |
| McAuley-Index | 0.02113 | −0.04718; 0.08943 | 0.5 |
| Maternal anthropometric measurements | |||
| Weight (kg) 1 | 0.01105 | −0.01075; 0.03285 | 0.4 |
| Fat mass (%) 2 | −0.7322 | −1.6551; 0.1924 | 0.2 |
| Study Participants (n = 47) | Routine Group (n = 47) | p for Difference 1 | |
|---|---|---|---|
| Mean (SD)/Median (25th, 75h Percentile) | Mean (SD)/Median (25th, 75h Percentile) | ||
| Gestational weight gain (between gw 20 and gw34), kg | 5.69 (3.30, 7.80) | 6.55 (4.50, 9.00) | 0.2 |
| Gestational weight gain (between gw 20 and gw34), kg/week | 0.41 (0.24, 0.56) | 0.47 (0.32, 0.64) | 0.2 |
| Excess gestational weight gain 2, n (%) | 31 (66.0%) | 41 (87.2%) | 0.046 |
| Gestational age, weeks | 39.0 (1.40) | 39.2 (1.66) | 0.5 |
| Birthweight, g | 3390 (440) | 3374 (523) | 0.4 |
| Macrosomia, n (%) | 0 (0%) | 7 (14.9%) | 0.006 |
| LGA, n (%) | 1 (2.1%) | 6 (12.8%) | 0.01 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Goletzke, J.; De Haene, J.; Stotland, N.E.; Murphy, E.J.; Perez-Rodriguez, M.; King, J.C. Effect of a Low-Glycemic Load Diet Intervention on Maternal and Pregnancy Outcomes in Obese Pregnant Women. Nutrients 2021, 13, 748. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13030748
Goletzke J, De Haene J, Stotland NE, Murphy EJ, Perez-Rodriguez M, King JC. Effect of a Low-Glycemic Load Diet Intervention on Maternal and Pregnancy Outcomes in Obese Pregnant Women. Nutrients. 2021; 13(3):748. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13030748
Chicago/Turabian StyleGoletzke, Janina, Jessica De Haene, Naomi E. Stotland, Elizabeth J. Murphy, Marcela Perez-Rodriguez, and Janet C. King. 2021. "Effect of a Low-Glycemic Load Diet Intervention on Maternal and Pregnancy Outcomes in Obese Pregnant Women" Nutrients 13, no. 3: 748. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13030748