
Psychological Resilience, Experimentally Manipulated Social Status, and Dietary Intake among Adolescents

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Protocol
2.3. Materials
2.3.1. Anthropometrics
2.3.2. Food Security
2.3.3. Socioeconomic Status and Subjective Social Status
2.3.4. Psychological Resilience: Connor Davidson Resilience Scale (CD-RISC)
2.3.5. Physical Activity Energy Expenditure
2.3.6. Resting Metabolic Heartrate
2.3.7. Dietary Intake
2.4. Statistical Analysis
3. Results

{kind=link}
| Characteristic | All (n = 132) | Manipulated High SS Group | Manipulated Low SS Group | ||
|---|---|---|---|---|---|
| Resilience < 73 (n = 26) | Resilience ≥ 73 (n = 38) | Resilience < 73 (n = 29) | Resilience ≥ 73 (n = 39) | ||
| Age (mean, SD) | 19.1 ± 1.3 | 19.2 ± 1.3 | 19.1 ± 1.2 | 19.2 ± 1.0 | 19.0 ± 1.5 |
| Female (n, %) | 80 (60.6%) | 17 (65.4%) | 22 (57.9%) | 16 (55.2%) | 25 (64.1%) |
| BMI (mean, SD) | 24.4 ± 4.1 | 25.6 ± 4.6 | 23.7 ± 4.3 | 24.3 ± 3.5 | 24.5 ± 4.0 |
| Community SSS (n, % low) | 37 (28.0%) | 6 (23.1%) | 9 (23.7%) | 9 (31.0%) | 13 (33.3%) |
| Food Security (n, % secure) | 98 (74.2%) | 20 (76.9%) | 30 (78.9%) | 19 (65.5%) | 29 (74.4%) |
| Resilience | 72.2 ± 10.5 | 60.9 ± 7.0 | 79.3 ± 4.9 | 63.5 ± 6.8 | 79.2 ± 6.8 |
| Variable | SFA | Sodium | Sugar | Total Energy Intake | % Energy Needs Consumed | |
|---|---|---|---|---|---|---|
| Female | b ± SE | −4.76 ± 0.73 | −785.39 ± 124.47 | −20.41 ± 5.37 | −453.15 ± 63.88 | −13.23 ± 3.42 |
| p | <0.001 * | <0.001 * | 0.001 * | <0.001 * | 0.053 * | |
| BMI | b ± SE | 0.05 ± 0.06 | 4.12 ± 10.28 | −0.20 ± 0.44 | 0.50 ± 5.28 | −0.68 ± 0.28 |
| p | 0.118 | 0.431 | 0.934 | 0.387 | 0.072 | |
| Low community SSS | b ± SE | 0.33 ± 0.56 | 101.54 ± 94.83 | 1.42 ± 4.09 | 31.59 ± 48.67 | 2.70 ± 2.60 |
| p | 0.311 | 0.186 | 0.318 | 0.173 | 0.109 | |
| Food Secure | b ± SE | −0.92 ± 0.57 | −80.15 ± 97.34 | −10.29 ± 4.20 | −119.41 ± 49.96 | −4.63 ± 2.67 |
| p | 0.229 | 0.583 | 0.039* | 0.052 | 0.174 | |
| Resilience | b ± SE | −0.06 ± 0.03 | −4.3 0 ± 5.58 | −0.37 ± 0.24 | −7.17 ± 2.87 | −0.39 ± 0.15 |
| p | 0.961 | 0.6353 | 0.365 | 0.845 | 0.739 | |
| Low manipulated SS | b ± SE | −2.97 ± 0.77 | −343.32 ± 131.30 | −10.06 ± 5.67 | −243.97 ± 67.39 | −9.83 ± 3.60 |
| p | 0.136 | 0.486 | 0.242 | 0.265 | 0.460 | |
| Female X Low SS | b ± SE | 3.69 ± 1.00 | 470.19 ± 169.85 | 9.46 ± 7.33 | 322.12 ± 87.18 | 13.31 ± 4.66 |
| p | <0.001 * | 0.007 * | 0.242 | <0.001 * | 0.007 * | |
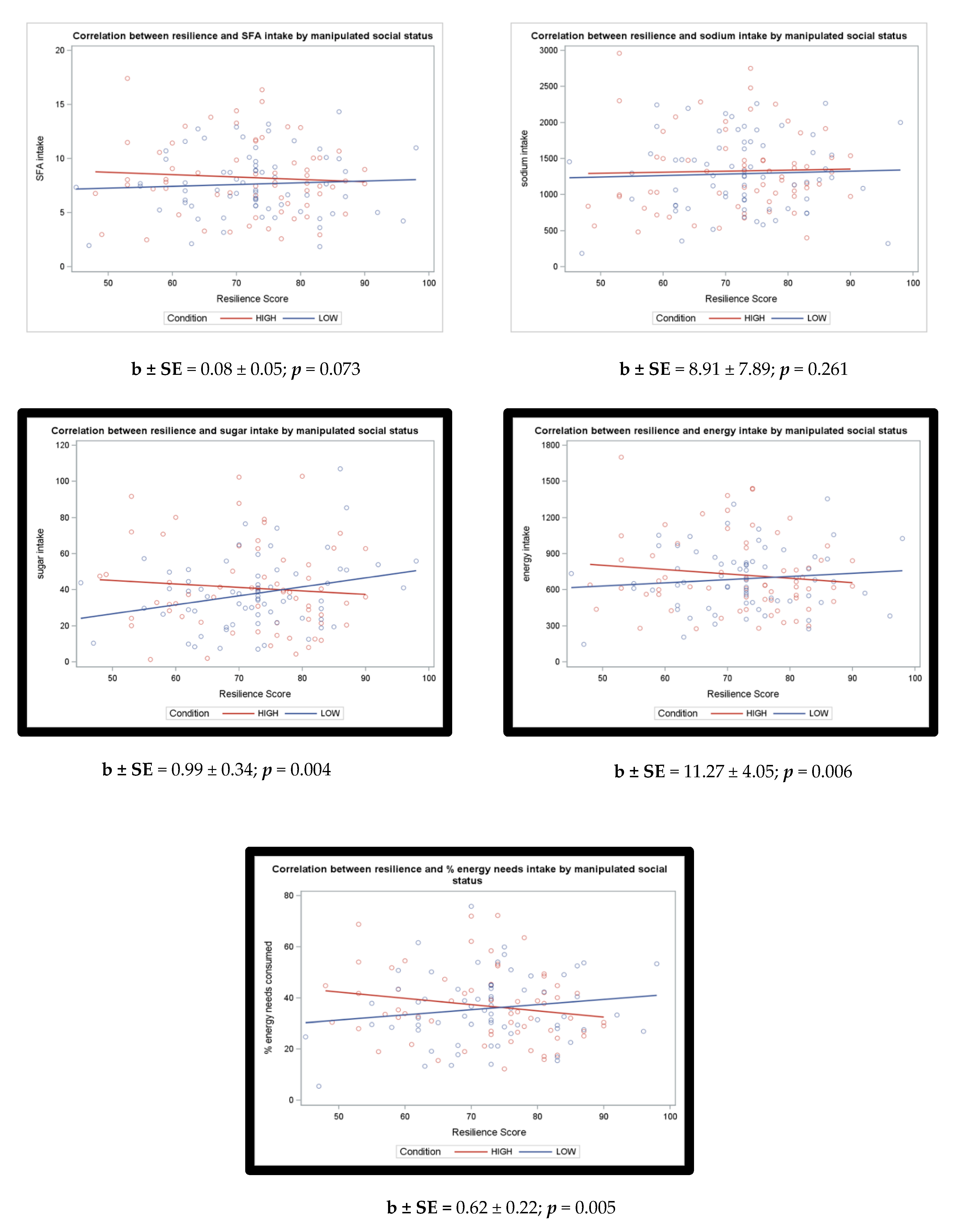
| Resilience X Low SS | b ± SE | 0.08 ± 0.05 | 8.91 ± 7.89 | 0.99 ± 0.34 | 11.27 ± 4.05 | 0.62 ± 0.22 |
| p | 0.073 | 0.261 | 0.004 * | 0.006 * | 0.005 * | |
4. Discussion
4.1. Strengths and Limitations
4.2. Future Directions
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A
| Food | Weight (g) | Calories (kcal) | Fat (g) | Saturated Fat (g) | Carbohydrate (g) | Protein (g) | Sugar (g) | Sodium (mg) | Fiber (g) |
|---|---|---|---|---|---|---|---|---|---|
| Meat Lasagna | 283 | 410 | 19 | 8 | 40 | 20 | 6 | 750 | 3 |
| Green Beans | 411 | 70 | 0 | 0 | 14 | 3.5 | 7 | 1015 | 7 |
| Macaroni and Cheese | 227 | 280 | 14 | 4.5 | 30 | 7 | 1 | 800 | 2 |
| Doritos Nacho Cheese | 88 | 420 | 24 | 3 | 48 | 6 | 0 | 630 | 3 |
| Classic Applesauce | 113 | 90 | 0 | 0 | 20 | 0 | 17 | 20 | 2 |
| Fruit Cup | 113 | 70 | 0 | 0 | 18 | 0 | 17 | 0 | 1 |
| Oreo Cookies | 68 | 320 | 13 | 3.5 | 49 | 3 | 27 | 270 | 1 |
| Bottled Water | 500 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Cola | 355 | 160 | 0 | 0 | 43 | 0 | 43 | 35 | 0 |
| Pink Lemonade | 355 | 150 | 0 | 0 | 42 | 0 | 40 | 50 | 0 |
| Dietary Intake Variable | All (n = 132) | Manipulated High SS Group | Manipulated Low SS Group | ||
|---|---|---|---|---|---|
| Resilience < 73 (n = 26) | Resilience ≥ 73 (n = 38) | Resilience < 73 (n = 29) | Resilience ≥ 73 (n = 39) | ||
| Total SFA, g (mean, SD) | 7.9 ± 3.2 | 8.5 ± 3.9 | 8.1 ± 3.2 | 7.7 ± 3.0 | 7.6 ± 2.9 |
| Sodium, mg (mean, SD) | 1307 ± 541 | 1306 ± 660 | 1342 ± 505 | 1320 ± 551 | 1265 ± 496 |
| Total sugar, g (mean, SD) | 39.3 ± 21.9 | 44.3 ± 26.7 | 38.6 ± 22.8 | 34.1 ± 17.3 | 40.6 ± 20.4 |
| Total energy, kcal (mean, SD) | 707 ± 289 | 774 ± 364 | 691 ± 289 | 692 ± 281 | 688 ± 240 |
| % energy needs, (mean, SD) | 36.3 ± 13.7 | 39.1 ± 15.0 | 35.4 ± 13.5 | 34.5 ± 15.0 | 36.8 ± 12.2 |
| Total SFA, g (mean, SD) | 7.9 ± 3.2 | 8.5 ± 3.9 | 8.1 ± 3.2 | 7.7 ± 3.0 | 7.6 ± 2.9 |
| Effect of Resilience | |||||
|---|---|---|---|---|---|
| Outcome | SS Condition | Coefficient | Standard Error | t Value | p-Value * |
| SFA (g) | High | −0.056 | 0.033 | −1.70 | 0.092 |
| Low | 0.028 | 0.033 | 0.86 | 0.393 | |
| Sodium (mg) | High | −4.302 | 5.584 | −0.77 | 0.443 |
| Low | 4.604 | 5.560 | 0.83 | 0.409 | |
| Sugar (g) | High | −0.373 | 0.241 | −1.55 | 0.125 |
| Low | 0.621 | 0.240 | 2.59 | 0.011 | |
| Energy (kcal) | High | −7.165 | 2.866 | −2.50 | 0.014 |
| Low | 4.105 | 2.854 | 1.44 | 0.153 | |
| % Energy needs | High | −0.394 | 0.153 | −2.57 | 0.011 |
| Low | 0.228 | 0.153 | 1.49 | 0.138 | |
References
- Skinner, A.C.; Perrin, E.M.; Skelton, J.A. Prevalence of obesity and severe obesity in US children, 1999–2014. Obesity 2016, 24, 1116–1123. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Powell, L.M.; Wada, R.; Krauss, R.C.; Wang, Y. Ethnic disparities in adolescent body mass index in the United States: The role of parental socioeconomic status and economic contextual factors. Soc. Sci. Med. 2012, 75, 469–476. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Galobardes, B.; Morabia, A.; Bernstein, M.S. Diet and socioeconomic position: Does the use of different indicators matter? Int. J. Epidemiol. 2001, 30, 334–340. [Google Scholar] [CrossRef] [Green Version]
- Quon, E.C.; McGrath, J.J. Subjective socioeconomic status and adolescent health: A meta-analysis. Health Psychol. 2014, 33, 433–447. [Google Scholar] [CrossRef] [Green Version]
- Cundiff, J.M.; Matthews, K.A. Is subjective social status a unique correlate of physical health? A meta-analysis. Health Psychol. 2017, 36, 1109–1125. [Google Scholar] [CrossRef]
- Zell, E.; Strickhouser, J.E.; Krizan, Z. Subjective social status and health: A meta-analysis of community and society ladders. Heal. Psychol. 2018, 37, 979–987. [Google Scholar] [CrossRef]
- Goodman, E.; Adler, N.E.; Daniels, S.R.; Morrison, J.A.; Slap, G.B.; Dolan, L.M. Impact of objective and subjective social status on obesity in a biracial cohort of adolescents. Obes. Res. 2003, 11, 1018–1026. [Google Scholar] [CrossRef]
- Rahal, D.; Huynh, V.; Cole, S.; Seeman, T.; Fuligni, A. Subjective Social Status and Health During High School and Young Adulthood. Dev. Psychol. 2020, 56, 1220–1232. [Google Scholar] [CrossRef] [PubMed]
- Goodman, E.; Huang, B.; Schafer-Kalkhoff, T.; Adler, N.E. Perceived Socioeconomic Status: A New Type of Identity That Influences Adolescents’ Self-Rated Health. J. Adolesc. Health 2007, 41, 479–487. [Google Scholar] [CrossRef] [Green Version]
- Cardel, M.I.; Tong, S.; Pavela, G.; Dhurandhar, E.; Miller, D.; Boles, R.; Haemer, M. Youth Subjective Social Status (SSS) is Associated with Parent SSS, Income, and Food Insecurity but not Weight Loss Among Low-Income Hispanic Youth. Obesity 2018, 26, 1923–1930. [Google Scholar] [CrossRef]
- Benner, A.D.; Wang, Y.; Shen, Y.; Boyle, A.E.; Polk, R.; Cheng, Y.P. Racial/ethnic discrimination and well-being during adolescence: A meta-analytic review. Am. Psychol. 2018, 72, 855. [Google Scholar] [CrossRef]
- Pavela, G.; Lewis, D.W.; Dawson, J.A.; Cardel, M.; Allison, D.B. Social status and energy intake: A randomized controlled experiment. Clin. Obes. 2017, 7, 316–322. [Google Scholar] [CrossRef] [PubMed]
- Cheon, B.K.; Hong, Y.Y. Mere experience of low subjective socioeconomic status stimulates appetite and food intake. Proc. Natl. Acad. Sci. USA 2017, 114, 72–77. [Google Scholar] [CrossRef] [Green Version]
- Bratanova, B.; Loughnan, S.; Klein, O.; Claassen, A.; Wood, R. Poverty, inequality, and increased consumption of high calorie food: Experimental evidence for a causal link. Appetite 2016, 100, 162–171. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cardel, M.I.; Johnson, S.L.; Beck, J.; Dhurandhar, E.; Keita, A.D.; Tomczik, A.C.; Pavela, G.; Huo, T.; Janicke, D.M.; Muller, K.; et al. The effects of experimentally manipulated social status on acute eating behavior: A randomized, crossover pilot study. Physiol. Behav. 2016, 162, 93–101. [Google Scholar] [CrossRef] [Green Version]
- Sim, A.Y.; Lim, E.X.; Forde, C.G.; Cheon, B.K. Personal relative deprivation increases self-selected portion sizes and food intake. Appetite 2018, 121, 268–274. [Google Scholar] [CrossRef]
- Cardel, M.I.; Pavela, G.; Janicke, D.; Huo, T.; Miller, D.; Lee, A.M.; Gurka, M.J.; Dhurandhar, E.; Peters, J.C.; Caldwell, A.E.; et al. Experimentally Manipulated Low Social Status and Food Insecurity Alter Eating Behavior Among Adolescents: A RCT. Obesity 2020, 28, 2010–2019. [Google Scholar] [CrossRef] [PubMed]
- Sim, A.Y.; Lim, E.X.; Leow, M.K.; Cheon, B.K. Low subjective socioeconomic status stimulates orexigenic hormone ghrelin—A randomised trial. Psychoneuroendocrinology 2018, 89, 103–112. [Google Scholar] [CrossRef] [PubMed]
- O’Leary, V.E. Strength in the face of adversity: Individual and social thriving. J. Soc. Issues 1998, 54, 425–446. [Google Scholar] [CrossRef]
- Gallo, L.C.; Matthews, K.A. Understanding the association between socioeconomic status and physical health: Do negative emotions play a role? Psychol. Bull. 2003, 129, 10. [Google Scholar] [CrossRef]
- Myers, H.F. Ethnicity-and socio-economic status-related stresses in context: An integrative review and conceptual model. J. Behav. Med. 2009, 32, 9–19. [Google Scholar] [CrossRef]
- Gallo, L.C.; Espinosa De Los Monteros, K.; Shivpuri, S. Socioeconomic status and health: What is the role of reserve capacity? Curr. Dir. Psychol. Sci. 2009, 18, 269–274. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lachman, M.E.; Weaver, S.L. The Sense of Control as a Moderator of Social Class Differences in Health and Well-Being. J. Pers. Soc. Psychol. 1998, 74, 763. [Google Scholar] [CrossRef] [PubMed]
- Chen, E.; Miller, G.E. “Shift-and-Persist” Strategies: Why Low Socioeconomic Status Isn’t Always Bad for Health. Perspect. Psychol. Sci. 2012, 7, 135–158. [Google Scholar] [CrossRef] [PubMed]
- Mauss, I.B.; Cook, C.L.; Cheng, J.Y.J.; Gross, J.J. Individual differences in cognitive reappraisal: Experiential and physiological responses to an anger provocation. Int. J. Psychophysiol. 2007, 66, 116–124. [Google Scholar] [CrossRef] [PubMed]
- Foster, B.A.; Weinstein, K. Moderating Effects of Components of Resilience on Obesity Across Income Strata in the National Survey of Children’s Health. Acad. Pediatr. 2019, 19, 58–66. [Google Scholar] [CrossRef]
- Thurston, I.B.; Hardin, R.; Kamody, R.C.; Herbozo, S.; Kaufman, C. The moderating role of resilience on the relationship between perceived stress and binge eating symptoms among young adult women. Eat. Behav. 2018, 29, 114–119. [Google Scholar] [CrossRef] [PubMed]
- Tiainen, A.M.K.; Männistö, S.; Lahti, M.; Blomstedt, P.A.; Lahti, J.; Perälä, M.M.; Räikkönen, K.; Kajantie, E.; Eriksson, J.G. Personality and Dietary Intake—Findings in the Helsinki Birth Cohort Study. PLoS ONE 2013, 8, e68284. [Google Scholar] [CrossRef] [Green Version]
- Whatnall, M.C.; Patterson, A.J.; Siew, Y.Y.; Kay-Lambkin, F.; Hutchesson, M.J. Are psychological distress and resilience associated with dietary intake Among Australian university students? Int. J. Environ. Res. Public Health 2019, 16, 4099. [Google Scholar] [CrossRef] [Green Version]
- Tinker, L.F.; Rosal, M.C.; Young, A.F.; Perri, M.G.; Patterson, R.E.; Van Horn, L.; Assaf, A.R.; Bowen, D.J.; Ockene, J.; Hays, J.; et al. Predictors of Dietary Change and Maintenance in the Women’s Health Initiative Dietary Modification Trial. J. Am. Diet. Assoc. 2007, 107, 1155–1165. [Google Scholar] [CrossRef]
- Giltay, E.J.; Geleijnse, J.M.; Zitman, F.G.; Buijsse, B.; Kromhout, D. Lifestyle and dietary correlates of dispositional optimism in men: The Zutphen Elderly Study. J. Psychosom. Res. 2007, 63, 483–490. [Google Scholar] [CrossRef]
- Singh-Manoux, A.; Marmot, M.G.; Adler, N.E. Does subjective social status predict health and change in health status better than objective status? Psychosom. Med. 2005, 67, 855–861. [Google Scholar] [CrossRef]
- Nicklett, E.J.; Burgard, S.A. Downward social mobility and major depressive episodes among latino and Asian-American immigrants to the United States. Am. J. Epidemiol. 2009, 170, 793–801. [Google Scholar] [CrossRef] [Green Version]
- Hager, E.R.; Quigg, A.M.; Black, M.M.; Coleman, S.M.; Heeren, T.; Rose-Jacobs, R.; Cook, J.T.; Ettinger De Cuba, S.A.; Casey, P.H.; Chilton, M.; et al. Development and validity of a 2-item screen to identify families at risk for food insecurity. Pediatrics 2010, 126, e26–e32. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goodman, E.; Adler, N.E.; Kawachi, I.; Frazier, A.L.; Huang, B.; Colditz, G.A. Adolescents’ perceptions of social status: Development and evaluation of a new indicator. Pediatrics 2001, 108, e31. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Adler, N.E.; Epel, E.S.; Castellazzo, G.; Ickovics, J.R. Relationship of subjective and objective social status with psychological and physiological functioning: Preliminary data in healthy white women. Health Psychol. 2000, 19, 586. [Google Scholar] [CrossRef]
- Connor, K.M.; Davidson, J.R.T. Development of a new Resilience scale: The Connor-Davidson Resilience scale (CD-RISC). Depress. Anxiety 2003, 18, 76–82. [Google Scholar] [CrossRef]
- Jørgensen, I.E.; Seedat, S. Factor structure of the Connor-Davidson Resilience Scale in South African adolescents. Int. J. Adolesc. Med. Health 2008, 20, 23–32. [Google Scholar] [CrossRef] [PubMed]
- Fu, C.; Leoutsakos, J.M.; Underwood, C. An examination of resilience cross-culturally in child and adolescent survivors of the 2008 China earthquake using the Connor-Davidson Resilience Scale (CD-RISC). J. Affect. Disord. 2014, 155, 149–152. [Google Scholar] [CrossRef]
- Ekelund, U.; Yngve, A.; Brage, S.; Westerterp, K.; Sjöström, M. Body movement and physical activity energy expenditure in children and adolescents: How to adjust for differences in body size and age. Am. J. Clin. Nutr. 2004, 79, 851–856. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Choi, L.; Liu, Z.; Matthews, C.E.; Buchowski, M.S. Validation of accelerometer wear and nonwear time classification algorithm. Med. Sci. Sports Exerc. 2011, 43, 357. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bassett, D.R.; Howley, E.T.; Thompson, D.L.; King, G.A.; Strath, S.J.; McLaughlin, J.E.; Parr, B.B. Validity of inspiratory and expiratory methods of measuring gas exchange with a computerized system. J. Appl. Physiol. 2001, 91, 218–224. [Google Scholar] [CrossRef]
- Cooper, J.A.; Watras, A.C.; O’Brien, M.J.; Luke, A.; Dobratz, J.R.; Earthman, C.P.; Schoeller, D.A. Assessing Validity and Reliability of Resting Metabolic Rate in Six Gas Analysis Systems. J. Am. Diet. Assoc. 2009, 109, 128–132. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aiken, L.S.; West, S.G. The effects of predictor scaling on coefficients of regression equations. Mult. Regres. Test. Interpret. Interact. 1991, 3, 28–48. [Google Scholar]
- Hartley, M.T. Examining the relationships between resilience, mental health, and academic persistence in undergraduate college students. J. Am. Coll. Heal. 2011, 59, 596–604. [Google Scholar] [CrossRef] [PubMed]
- Otto, L.M.; Howerter, A.; Bell, I.R.; Jackson, N. Exploring measures of whole person wellness: Integrative well-being and psychological flourishing. Explor. J. Sci. Health 2010, 6, 364–370. [Google Scholar] [CrossRef] [Green Version]
- DeCoster, J.; Gallucci, M.; Iselin, A.-M.R. Best Practices for Using Median Splits, Artificial Categorization, and their Continuous Alternatives. J. Exp. Psychopathol. 2011, 2, 197–209. [Google Scholar] [CrossRef]
- Heimpel, S.A.; Wood, J.V.; Marshall, M.A.; Brown, J.D. Do people with low self-esteem really want to feel better? Self-esteem differences in motivation to repair negative moods. J. Pers. Soc. Psychol. 2002, 82, 128. [Google Scholar] [CrossRef]
- Dumont, M.; Provost, M.A. Resilience in adolescents: Protective role of social support, coping strategies, self-esteem, and social activities on experience of stress and depression. J. Youth Adolesc. 1999, 28, 343–363. [Google Scholar] [CrossRef]
- Eley, D.S.; Robert Cloninger, C.; Walters, L.; Laurence, C.; Synnott, R.; Wilkinson, D. The relationship between resilience and personality traits in doctors: Implications for enhancing well being. PeerJ. 2013, 1, e216. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Balgiu, B.A. Self-esteem, personality and resilience. Study of a students emerging adults group. J. Educ. Sci. Psychol. 2017, 7, 93–99. [Google Scholar]
- Thayer, R.E.; Newman, J.R.; McClain, T.M. Self-Regulation of Mood: Strategies for Changing a Bad Mood, Raising Energy, and Reducing Tension. J. Pers. Soc. Psychol. 1994, 67, 910. [Google Scholar] [CrossRef] [PubMed]
- Spangler, R.; Wittkowski, K.M.; Goddard, N.L.; Avena, N.M.; Hoebel, B.G.; Leibowitz, S.F. Opiate-like effects of sugar on gene expression in reward areas of the rat brain. Mol. Brain Res. 2004, 124, 134–142. [Google Scholar] [CrossRef]
- Avena, N.M.; Rada, P.; Hoebel, B.G. Evidence for sugar addiction: Behavioral and neurochemical effects of intermittent, excessive sugar intake. Neurosci. Biobehav. Rev. 2008, 32, 20–39. [Google Scholar] [CrossRef] [Green Version]
- Colantuoni, C.; Rada, P.; McCarthy, J.; Patten, C.; Avena, N.M.; Chadeayne, A.; Hoebel, B.G. Evidence that intermittent, excessive sugar intake causes endogenous opioid dependence. Obes. Res. 2002, 10, 478–488. [Google Scholar] [CrossRef] [PubMed]
- Miller, G.E.; Cohen, S.; Janicki-Deverts, D.; Brody, G.H.; Chen, E. Health Psychology Viral Challenge Reveals Further Evidence of Skin-Deep Resilience in African Americans From Disadvantaged Backgrounds. Health Psychol. 2016, 35, 1225. [Google Scholar] [CrossRef] [PubMed]
- Chen, E.; Miller, G.E.; Brody, G.H.; Lei, M.K. Neighborhood Poverty, College Attendance, and Diverging Profiles of Substance Use and Allostatic Load in Rural African American Youth. Clin. Psychol. Sci. 2015, 3, 675–685. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brody, G.H.; Yu, T.; Chen, E.; Miller, G.E.; Kogan, S.M.; Beach, S.R.H. Is Resilience Only Skin Deep? Rural African Americans’ Socioeconomic Status-Related Risk and Competence in Preadolescence and Psychological Adjustment and Allostatic Load at Age 19. Psychol. Sci. 2013, 24, 1285–1293. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- James, S.A.; Hartnett, S.A.; Kalsbeek, W.D. John Henryism and blood pressure differences among black men. J. Behav. Med. 1983, 6, 259–278. [Google Scholar] [CrossRef] [PubMed]
- Brody, G.H.; Yu, T.; Miller, G.E.; Ehrlich, K.B.; Chen, E. John Henryism Coping and Metabolic Syndrome among Young Black Adults. Psychosom. Med. 2018, 80, 216. [Google Scholar] [CrossRef] [PubMed]
- Morote, R.; Hjemdal, O.; Uribe, P.M.; Corveleyn, J. Psychometric properties of the Resilience Scale for Adults (RSA) and its relationship with life-stress, anxiety and depression in a Hispanic Latin-American community sample. PLoS ONE 2017, 12, e0187954. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dulin, A.J.; Dale, S.K.; Earnshaw, V.A.; Fava, J.L.; Mugavero, M.J.; Napravnik, S.; Hogan, J.W.; Carey, M.P.; Howe, C.J. Resilience and HIV: A review of the definition and study of resilience. AIDS Care Psychol. Socio Medical Asp. AIDS/HIV 2018, 30, S6–S17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hales, C.M.; Carroll, M.D.; Fryar, C.D.; Ogden, C.L. Prevalence of Obesity among Adults and Youth: United States, 2015–2016; NCHS data brief, no 288; National Center for Health Statistics: Hyattsville, MD, USA, 2017. [Google Scholar]

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Guazzelli Williamson, V.; Lee, A.M.; Miller, D.; Huo, T.; Maner, J.K.; Cardel, M. Psychological Resilience, Experimentally Manipulated Social Status, and Dietary Intake among Adolescents. Nutrients 2021, 13, 806. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13030806
Guazzelli Williamson V, Lee AM, Miller D, Huo T, Maner JK, Cardel M. Psychological Resilience, Experimentally Manipulated Social Status, and Dietary Intake among Adolescents. Nutrients. 2021; 13(3):806. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13030806
Chicago/Turabian StyleGuazzelli Williamson, Victoria, Alexandra M. Lee, Darci Miller, Tianyao Huo, Jon K. Maner, and Michelle Cardel. 2021. "Psychological Resilience, Experimentally Manipulated Social Status, and Dietary Intake among Adolescents" Nutrients 13, no. 3: 806. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13030806