
Sugar-Sweetened Beverage Consumption and Calcified Atherosclerotic Plaques in the Coronary Arteries: The NHLBI Family Heart Study

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
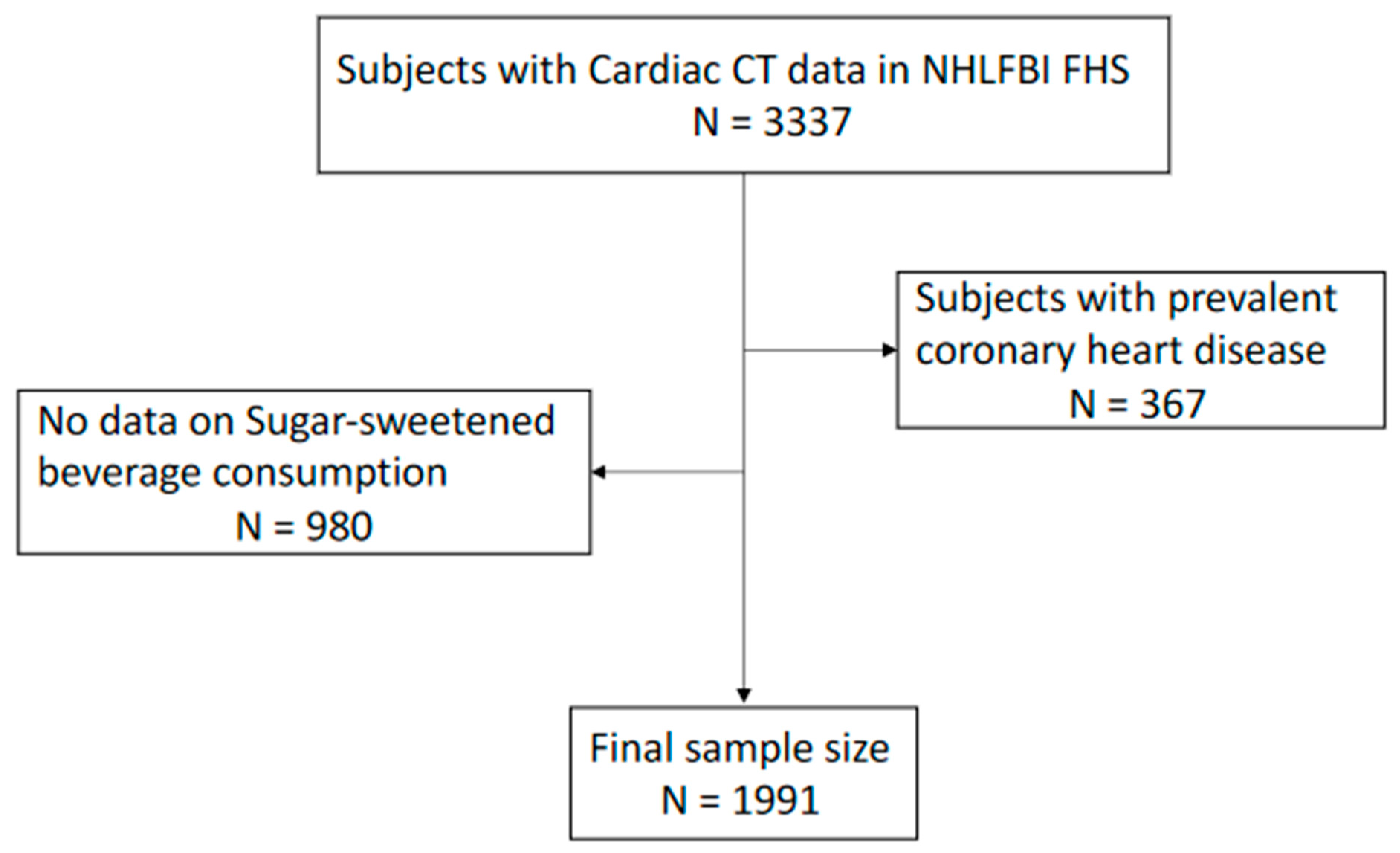
2.1. Study Population
2.2. Assessment of SSB Consumption
2.3. Measurement of Calcified Atherosclerotic Plaque in the Coronary Arteries
2.4. Other Variables
3. Statistical Analysis
4. Results
4.1. SSB Consumption
4.2. Regular Soda, Diet Soda, and Fruit Punch/Kool Aid Consumption
5. Discussion
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| SSB | sugar-sweetened beverages |
| CAC | coronary artery calcium |
| NHLBI FHS | National Heart, Lung, and Blood Institute Family Heart Study |
| CHD | coronary heart disease |
References
- Basu, S.; McKee, M.; Galea, G.; Stuckler, D. Relationship of Soft Drink Consumption to Global Overweight, Obesity, and Diabetes: A Cross-National Analysis of 75 Countries. Am. J. Public Health 2013, 103, 2071–2077. [Google Scholar] [CrossRef]
- De Ruyter, J.C.; Olthof, M.R.; Seidell, J.C.; Katan, M.B. A Trial of Sugar-free or Sugar-Sweetened Beverages and Body Weight in Children. N. Engl. J. Med. 2012, 367, 1397–1406. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ebbeling, C.B.; Feldman, H.A.; Chomitz, V.R.; Antonelli, T.A.; Gortmaker, S.L.; Osganian, S.K.; Ludwig, D.S. A Randomized Trial of Sugar-Sweetened Beverages and Adolescent Body Weight. N. Engl. J. Med. 2012, 367, 1407–1416. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Malik, V.S.; Pan, A.; Willett, W.C.; Hu, F.B. Sugar-sweetened beverages and weight gain in children and adults: A systematic review and meta-analysis. Am. J. Clin. Nutr. 2013, 98, 1084–1102. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- The InterAct Consortium. Consumption of sweet beverages and type 2 diabetes incidence in European adults: Results from EPIC-InterAct. Diabetologia 2013, 56, 1520–1530. [Google Scholar] [CrossRef]
- Hu, F.B.; Malik, V.S. Sugar-sweetened beverages and risk of obesity and type 2 diabetes: Epidemiologic evidence. Physiol. Behav. 2010, 100, 47–54. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Malik, V.S.; Popkin, B.M.; Bray, G.A.; Després, J.-P.; Willett, W.C.; Hu, F.B. Sugar-Sweetened Beverages and Risk of Metabolic Syndrome and Type 2 Diabetes: A meta-analysis. Diabetes Care 2010, 33, 2477–2483. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Malik, V.S.; Popkin, B.M.; Bray, G.A.; Després, J.-P.; Hu, F.B. Sugar-Sweetened Beverages, Obesity, Type 2 Diabetes Mellitus, and Cardiovascular Disease Risk. Circulation 2010, 121, 1356–1364. [Google Scholar] [CrossRef]
- Nettleton, J.A.; Lutsey, P.L.; Wang, Y.; Lima, J.A.; Michos, E.D.; Jacobs, D.R., Jr. Diet Soda Intake and Risk of Incident Metabolic Syndrome and Type 2 Diabetes in the Multi-Ethnic Study of Atherosclerosis (MESA). Diabetes Care 2009, 32, 688–694. [Google Scholar] [CrossRef] [Green Version]
- Lutsey, P.L.; Steffen, L.M.; Stevens, J. Dietary Intake and the Development of the Metabolic Syndrome: The Atherosclerosis Risk in Communities study. Circulation 2008, 117, 754–761. [Google Scholar] [CrossRef] [Green Version]
- Dhingra, R.; Sullivan, L.; Jacques, P.F.; Wang, T.J.; Fox, C.S.; Meigs, J.B.; D’Agostino, R.B.; Gaziano, J.M.; Vasan, R.S. Soft Drink Consumption and Risk of Developing Cardiometabolic Risk Factors and the Metabolic Syndrome in Middle-Aged Adults in the Community. Circulation 2007, 116, 480–488. [Google Scholar] [CrossRef] [Green Version]
- Fung, T.T.; Malik, V.; Rexrode, K.M.; Manson, J.E.; Willett, W.C.; Hu, F.B. Sweetened beverage consumption and risk of coronary heart disease in women. Am. J. Clin. Nutr. 2009, 89, 1037–1042. [Google Scholar] [CrossRef] [Green Version]
- de Koning, L.; Malik, V.S.; Kellogg, M.D.; Rimm, E.B.; Willett, W.C.; Hu, F.B. Sweetened Beverage Consumption, Incident Coronary Heart Disease, and Biomarkers of Risk in Men. Circulation 2012, 125, 1735–1741. [Google Scholar] [CrossRef] [Green Version]
- Eshak, E.S.; Iso, H.; Kokubo, Y.; Saito, I.; Yamagishi, K.; Inoue, M.; Tsugane, S. Soft drink intake in relation to incident ischemic heart disease, stroke, and stroke subtypes in Japanese men and women: The Japan Public Health Centre–based study cohort I. Am. J. Clin. Nutr. 2012, 96, 1390–1397. [Google Scholar] [CrossRef] [Green Version]
- Singh, G.M.; Micha, R.; Khatibzadeh, S.; Lim, S.; Ezzati, M.; Mozaffarian, D. Estimated Global, Regional, and National Disease Burdens Related to Sugar-Sweetened Beverage Consumption in 2010. Circulation 2015, 132, 639–666. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Greenland, P.; Bonow, R.O.; Brundage, B.H.; Budoff, M.J.; Eisenberg, M.J.; Grundy, S.M.; Lauer, M.S.; Post, W.S.; Raggi, P.; Redberg, R.F.; et al. ACCF/AHA 2007 Clinical Expert Consensus Document on Coronary Artery Calcium Scoring by Computed Tomography in Global Cardiovascular Risk Assessment and in Evaluation of Patients With Chest Pain: A report of the American College of Cardiology Foundation Clinical Expert Consensus Task Force (ACCF/AHA Writing Committee to Update the 2000 Expert Consensus Document on Electron Beam Computed Tomography). Circulation 2007, 115, 402–426. [Google Scholar] [CrossRef]
- Haberl, R.; Becker, A.; Leber, A.; Knez, A.; Becker, C.; Lang, C.; Brüning, R.; Reiser, M.; Steinbeck, G. Correlation of coronary calcification and angiographically documented stenoses in patients with suspected coronary artery disease: Results of 1,764 patients. J. Am. Coll. Cardiol. 2001, 37, 451–457. [Google Scholar] [CrossRef] [Green Version]
- Higgins, M.; Province, M.; Heiss, G.; Eckfeldt, J.; Ellison, R.C.; Folsom, A.R.; Rao, D.C.; Sprafka, J.M.; Williams, R. NHLBI Family Heart Study: Objectives and Design. Am. J. Epidemiol. 1996, 143, 1219–1228. [Google Scholar] [CrossRef] [Green Version]
- Djoussé, L.; Arnett, D.K.; Carr, J.J.; Eckfeldt, J.H.; Hopkins, P.N.; Province, M.A.; Ellison, R.C. Dietary Linolenic Acid Is Inversely Associated With Calcified Atherosclerotic Plaque in the Coronary Arteries: The National Heart, Lung, and Blood Institute Family Heart Study. Circulation 2005, 111, 2921–2926. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Willett, W.C.; Sampson, L.; Stampfer, M.J.; Rosner, B.; Bain, C.; Witschi, J.; Hennekens, C.H.; Speizer, F.E. Reproducibility and validity of a Semiquantitative food frequency questionnaire. Am. J. Epidemiol. 1985, 122, 51–65. [Google Scholar] [CrossRef] [PubMed]
- Rimm, E.B.; Giovannucci, E.L.; Stampfer, M.J.; Colditz, G.A.; Litin, L.B.; Willett, W.C. Reproducibility and Validity of an Expanded Self-Administered Semiquantitative Food Frequency Questionnaire among Male Health Professionals. Am. J. Epidemiol. 1992, 135, 1114–1126. [Google Scholar] [CrossRef] [PubMed]
- Stein, A.D.; Shea, S.; Basch, C.E.; Contento, I.R.; Zyberf, P. Consistency of the Willett Semiquantitative Food Frequency Questionnaire and 24-Hour Dietary Recalls in Estimating Nutrient Intakes of Preschool Children. Am. J. Epidemiol. 1992, 135, 667–677. [Google Scholar] [CrossRef] [PubMed]
- Hoffmann, U.; Brady, T.J.; Muller, J. Use of New Imaging Techniques to Screen for Coronary Artery Disease. Circulation 2003, 108, 50–53. [Google Scholar] [CrossRef]
- Malik, V.S.; Schulze, M.B.; Hu, F.B. Intake of sugar-sweetened beverages and weight gain: A systematic review. Am. J. Clin. Nutr. 2006, 84, 274–288. [Google Scholar] [CrossRef] [PubMed]
- Cohen, L.; Curhan, G.; Forman, J. Association of Sweetened Beverage Intake with Incident Hypertension. J. Gen. Intern. Med. 2012, 27, 1127–1134. [Google Scholar] [CrossRef] [PubMed]
- Choi, H.K.; Curhan, G. Soft drinks, fructose consumption, and the risk of gout in men: Prospective cohort study. BMJ 2008, 336, 309–312. [Google Scholar] [CrossRef] [Green Version]
- Miller, A.; Adeli, K. Dietary fructose and the metabolic syndrome. Curr. Opin. Gastroenterol. 2008, 24, 204–209. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stanhope, K.L.; Bremer, A.A.; Medici, V.; Nakajima, K.; Ito, Y.; Nakano, T.; Chen, G.; Fong, T.H.; Lee, V.; Menorca, R.I.; et al. Consumption of Fructose and High Fructose Corn Syrup Increase Postprandial Triglycerides, LDL-Cholesterol, and Apolipoprotein-B in Young Men and Women. J. Clin. Endocrinol. Metab. 2011, 96, E1596–E1605. [Google Scholar] [CrossRef] [PubMed]
- Stanhope, K.L.; Medici, V.; Bremer, A.A.; Lee, V.; Lam, H.D.; Nunez, M.V.; Chen, G.X.; Keim, N.L.; Havel, P.J. A dose-response study of consuming high-fructose corn syrup–sweetened beverages on lipid/lipoprotein risk factors for cardiovascular disease in young adults. Am. J. Clin. Nutr. 2015, 101, 1144–1154. [Google Scholar] [CrossRef] [Green Version]
- Stanhope, K.L.; Schwarz, J.M.; Keim, N.L.; Griffen, S.C.; Bremer, A.A.; Graham, J.L.; Hatcher, B.; Cox, C.L.; Dyachenko, A.; Zhang, W.; et al. Consuming fructose-sweetened, not glucose-sweetened, beverages increases visceral adiposity and lipids and decreases insulin sensitivity in overweight/obese humans. J. Clin. Investig. 2009, 119, 1322–1334. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aeberli, I.; Hochuli, M.; Gerber, P.A.; Sze, L.; Murer, S.B.; Tappy, L.; Spinas, G.A.; Berneis, K.; Espeland, M.A.; Bryan, R.N.; et al. Moderate Amounts of Fructose Consumption Impair Insulin Sensitivity in Healthy Young Men: A randomized controlled trial. Diabetes Care 2012, 36, 150–156. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aeberli, I.; Gerber, P.A.; Hochuli, M.; Kohler, S.; Haile, S.R.; Gouni-Berthold, I.; Berthold, H.K.; Spinas, G.A.; Berneis, K. Low to moderate sugar-sweetened beverage consumption impairs glucose and lipid metabolism and promotes inflammation in healthy young men: A randomized controlled trial. Am. J. Clin. Nutr. 2011, 94, 479–485. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Frequency of Sugar-Sweetened Beverage Consumption (1 Drink) | ||||||
|---|---|---|---|---|---|---|
| Almost Never (N = 168) | 1–3/Month (N = 132) | 1/Week (N = 250) | 2–6/Week (N = 464) | 1/Day (N = 439) | ≥2/Day (N = 538) | |
| Age (years) | 62.9 ± 12.1 | 59.7 ± 13.6 | 58.8 ± 12.2 | 58.4 ± 12.7 | 55.8 ± 12.7 | 52.1 ± 11.9 |
| BMI (kg/m2) | 27.3 ± 5.1 | 28.1 ± 5.6 | 28.1 ± 5.1 | 28.6 ± 5.7 | 28.6 ± 5.2 | 30.1 ± 6.3 |
| Male (%) | 23.8 | 27.3 | 32.8 | 41.4 | 47.2 | 49.1 |
| Smoking (pack years) | 13.2 ± 25.7 | 8.6 ± 21.1 | 6.8 ± 15.3 | 8.9 ± 18.1 | 7.0 ± 17.0 | 10.6 ± 19.4 |
| Alcohol (drinks/week) | 3.6 ± 6.4 | 2.6 ± 5.4 | 2.4 ± 5.0 | 3.4 ± 10.3 | 3.3 ± 6.1 | 4.3 ± 8.8 |
| Hypertension (%) | 37.5 | 34.9 | 33.6 | 36.4 | 38.8 | 37.4 |
| Diabetes (%) | 10.7 | 7.6 | 9.2 | 8.6 | 10.3 | 10.4 |
| Income (%) | ||||||
| <$25,000 | 19.9 | 13.6 | 12.7 | 12.9 | 11.0 | 10.2 |
| $25,000–<$75,000 | 54.7 | 56.8 | 57.0 | 57.0 | 53.0 | 52.5 |
| ≥$75,000 | 15.4 | 29.6 | 30.3 | 30.1 | 36.0 | 37.3 |
| Exercise (MET-min/week) | 443 (1025) | 501 (1028) | 436 (802) | 443 (775) | 376 (872) | 358 (886) |
| Calories (kcal/d) | 1385 (663) | 1592 (751) | 1503 (793) | 1561 (696) | 1649 (844) | 1945 (966) |
| Cases/n | Age and Sex Adjusted | Model 1 * | |
|---|---|---|---|
| Sugar-sweetened beverage (1 glass) | |||
| Almost never | 49/168 | 1 | 1 |
| 1-3/month | 34/132 | 1.08 (0.60–1.96) | 1.36 (0.70–2.63) |
| 1/week | 70/250 | 1.36 (0.81–2.29) | 1.69 (0.93–3.09) |
| 2-6/week | 126/464 | 1.16 (0.72–1.90) | 1.21 (0.69–2.12) |
| 1/day | 94/439 | 0.97 (0.60–1.58) | 1.05 (0.60–1.84) |
| ≥2/day | 102/538 | 1.39 (0.82–2.37) | 1.58 (0.85–2.94) |
| p for trend | 0.51 | 0.32 | |
| Regular soda (1 glass) | |||
| Almost never | 246/858 | 1 | 1 |
| 1–3/month | 62/279 | 0.55 (0.28–1.06) | 0.69 (0.32–1.48) |
| 1/week | 53/214 | 0.56 (0.32–0.98) | 0.58 (0.30–1.14) |
| 2–6/week | 62/288 | 0.65 (0.43–0.99) | 0.72 (0.44–1.18) |
| 1/day | 32/177 | 0.66 (0.44–0.98) | 0.82 (0.51–1.33) |
| ≥2/day | 20/175 | 0.72 (0.49–1.05) | 1.07 (0.69–1.66) |
| p for trend | 0.066 | 0.44 | |
| Diet soda (1 glass) | |||
| Almost never | 194/878 | 1 | 1 |
| 1–3/month | 46/203 | 1.48 (0.99–2.21) | 1.21 (0.73–2.00) |
| 1/week | 36/125 | 1.45 (0.96–2.18) | 1.44 (0.88–2.36) |
| 2–6/week | 76/278 | 1.12 (0.78–1.60) | 0.97 (0.64–1.46) |
| 1/day | 62/227 | 1.11 (0.66–1.88) | 1.06 (0.58–1.93) |
| ≥2/day | 61/280 | 0.96 (0.61–1.52) | 1.01 (0.59–1.74) |
| p for trend | 0.30 | 0.76 | |
| Fruit punch/kool aid (1 glass) | |||
| Almost never | 248/900 | 1 | 1 |
| 1–3/month | 89/389 | 0.87 (0.34–2.25) | 1.76 (0.51–6.14) |
| 1/week | 49/250 | 1.06 (0.54–2.08) | 2.12 (0.98–4.59) |
| 2–6/week | 59/300 | 0.76 (0.51–1.13) | 1.28 (0.81–2.03) |
| 1/day | 23/105 | 0.58 (0.37–0.90) | 0.82 (0.50–1.36) |
| ≥2/day | 7/47 | -- # | -- # |
| p for trend | 0.18 | 0.25 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Patel, Y.R.; Imran, T.F.; Ellison, R.C.; Hunt, S.C.; Carr, J.J.; Heiss, G.; Arnett, D.K.; Pankow, J.S.; Gaziano, J.M.; Djoussé, L. Sugar-Sweetened Beverage Consumption and Calcified Atherosclerotic Plaques in the Coronary Arteries: The NHLBI Family Heart Study. Nutrients 2021, 13, 1775. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13061775
Patel YR, Imran TF, Ellison RC, Hunt SC, Carr JJ, Heiss G, Arnett DK, Pankow JS, Gaziano JM, Djoussé L. Sugar-Sweetened Beverage Consumption and Calcified Atherosclerotic Plaques in the Coronary Arteries: The NHLBI Family Heart Study. Nutrients. 2021; 13(6):1775. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13061775
Chicago/Turabian StylePatel, Yash R., Tasnim F. Imran, R. Curtis Ellison, Steven C. Hunt, John Jeffrey Carr, Gerardo Heiss, Donna K. Arnett, James S. Pankow, J. Michael Gaziano, and Luc Djoussé. 2021. "Sugar-Sweetened Beverage Consumption and Calcified Atherosclerotic Plaques in the Coronary Arteries: The NHLBI Family Heart Study" Nutrients 13, no. 6: 1775. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13061775