
Acute Beetroot Juice Ingestion Does Not Alter Renal Hemodynamics during Normoxia and Mild Hypercapnia in Healthy Young Adults

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Instrumentation and Measurements
2.3. Experimental Protocol
2.4. Data and Statistical Analyses
3. Results
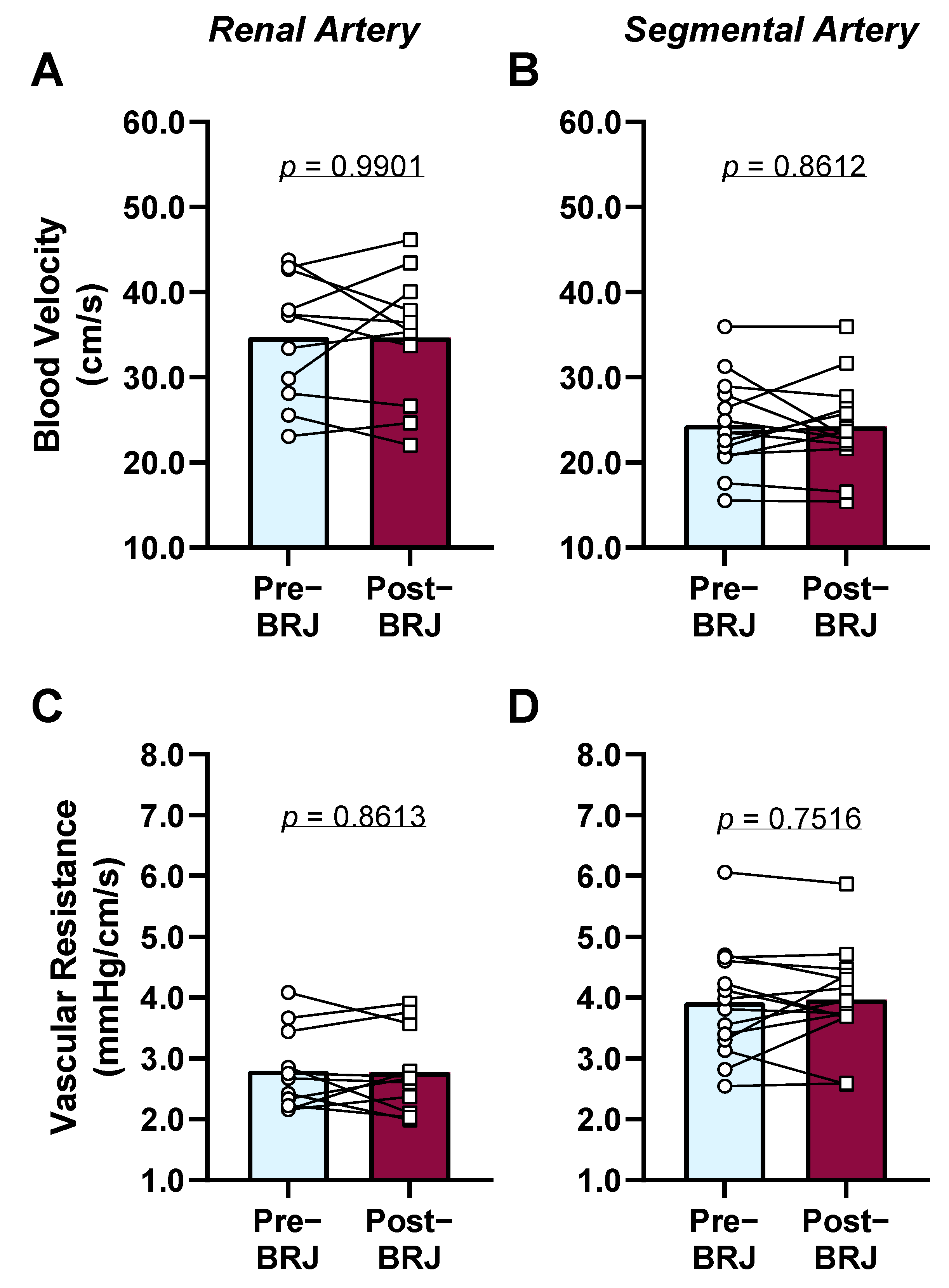
3.1. Effect of Beetroot Juice Consumption during Room Air Breathing
3.2. Effect of Beetroot Juice Consumption during CO2 Breathing
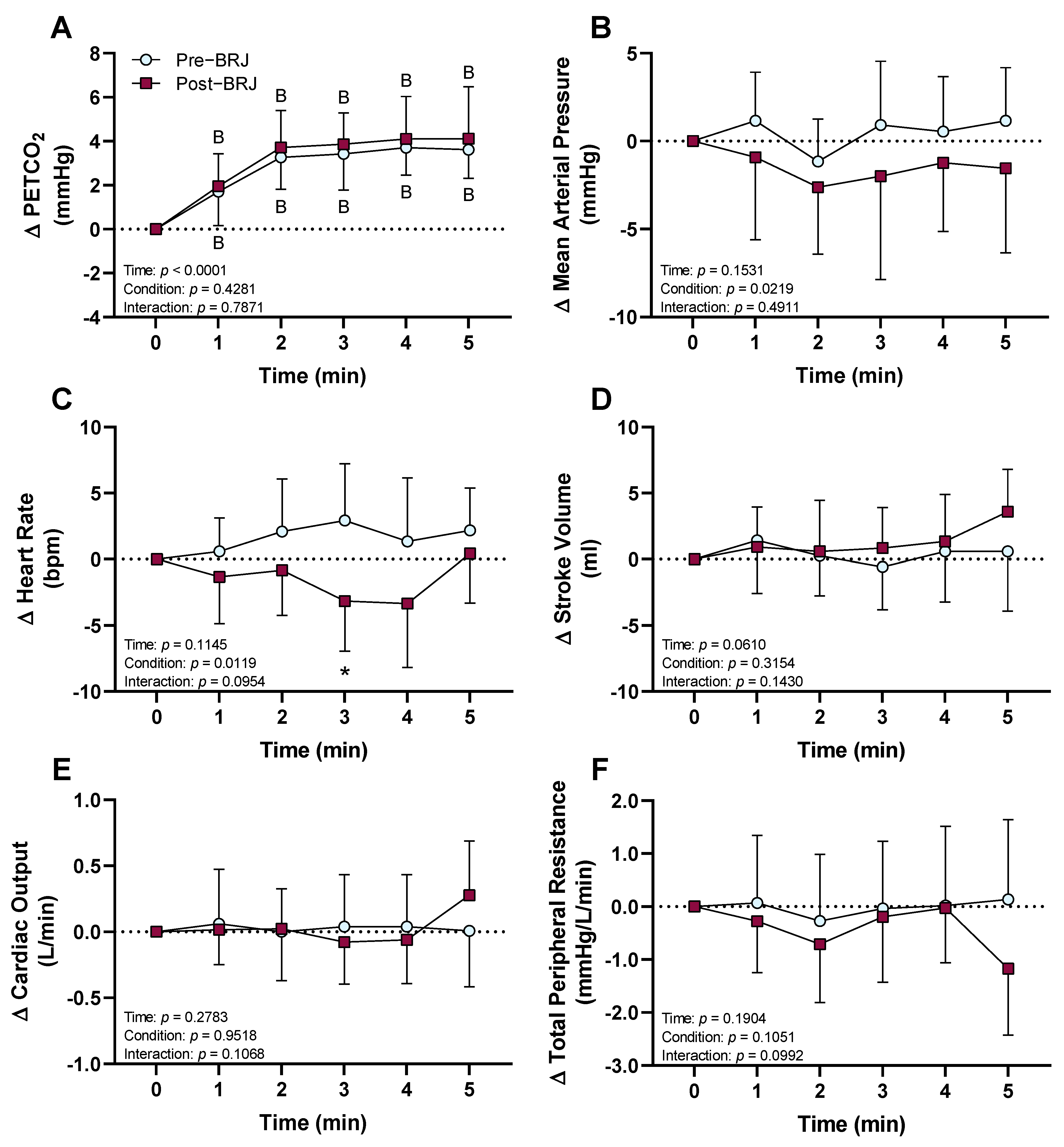
3.2.1. PETCO2 and Cardiovascular Responses
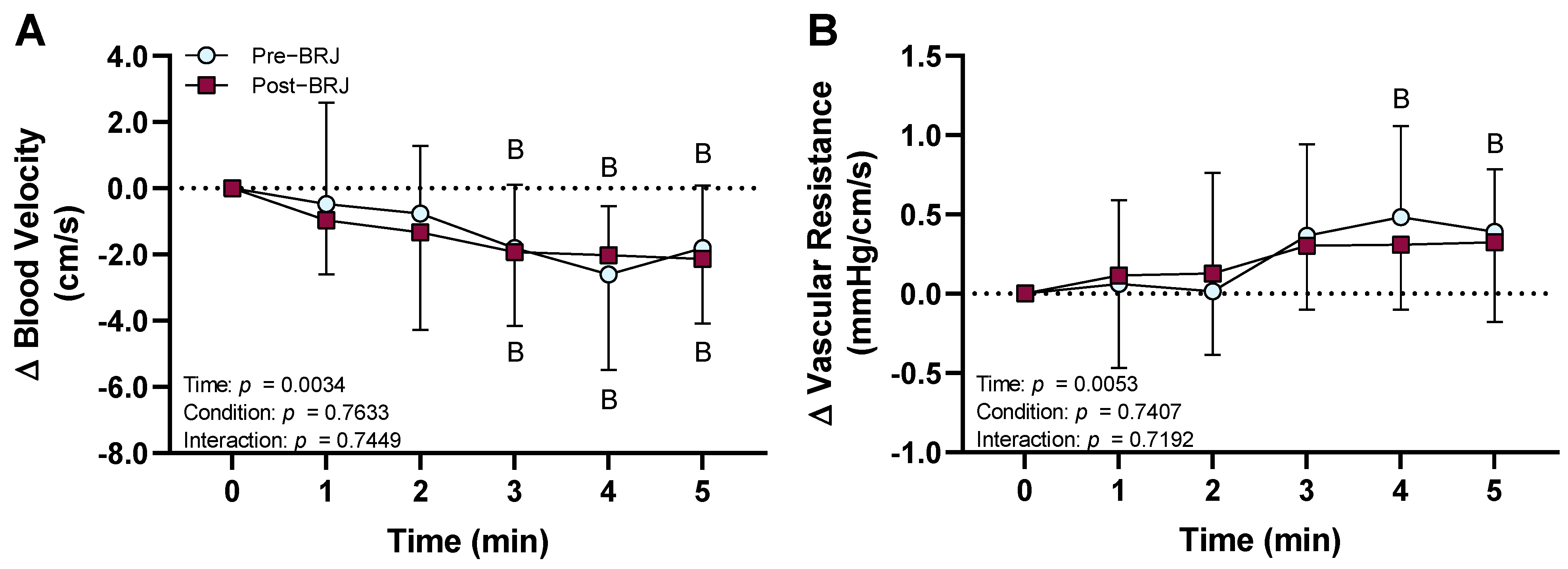
3.2.2. Segmental Artery Hemodynamics
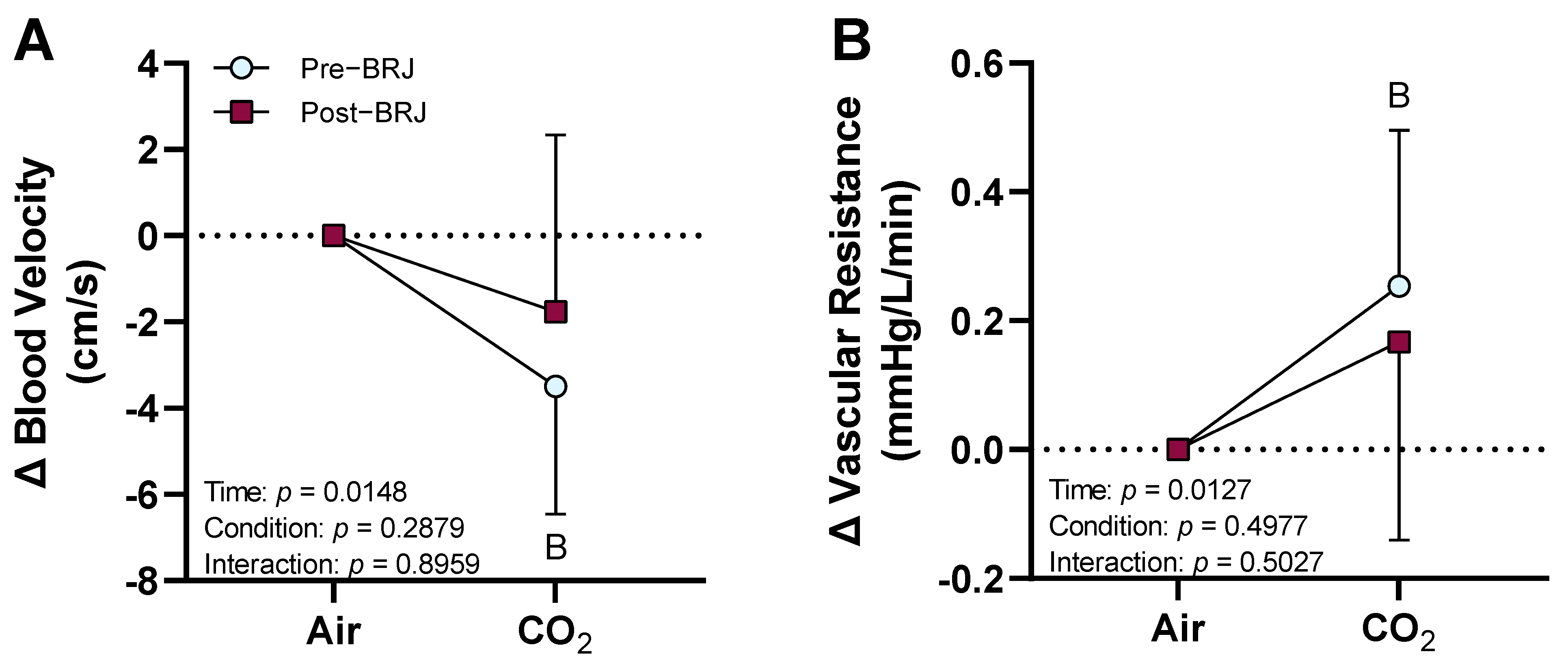
3.2.3. Renal Artery Hemodynamics
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Visconti, L.; Santoro, D.; Cernaro, V.; Buemi, M.; Lacquaniti, A. Kidney-lung connections in acute and chronic diseases: Current perspectives. J. Nephrol. 2016, 29, 341–348. [Google Scholar] [CrossRef] [PubMed]
- Barakat, M.; McDonald, H.; Collier, T.; Smeeth, L.; Nitsch, D.; Quint, J. Acute kidney injury in stable COPD and at exacerbation. Int. J. Chron. Obs. Pulmon. Dis. 2015, 10, 2067. [Google Scholar] [CrossRef] [Green Version]
- Corsonello, A.; Aucella, F.; Pedone, C.; Antonelli-Incalzi, R. Chronic kidney disease: A likely underestimated component of multimorbidity in older patients with chronic obstructive pulmonary disease. Geriatr. Gerontol. Int. 2017, 17, 1770–1788. [Google Scholar] [CrossRef] [PubMed]
- Greulich, T.; Weist, B.J.; Koczulla, A.R.; Janciauskiene, S.; Klemmer, A.; Lux, W.; Alter, P.; Vogelmeier, C.F. Prevalence of comorbidities in COPD patients by disease severity in a German population. Respir. Med. 2017, 132, 132–138. [Google Scholar] [CrossRef]
- Ko, G.J.; Rabb, H.; Hassoun, H.T. Kidney-lung crosstalk in the critically ill patient. Blood Purif. 2009, 28, 75–83. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lai, C.-C.; Wu, C.-H.; Wang, Y.-H.; Wang, C.-Y.; Wu, V.-C.; Chen, L. The association between COPD and outcomes of patients with advanced chronic kidney disease. Int. J. Chronic Obstr. Pulm. Dis. 2018, 13, 2899. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kawata, N.; Tatsumi, K.; Terada, J.; Tada, Y.; Tanabe, N.; Takiguchi, Y.; Kuriyama, T. Daytime hypercapnia in obstructive sleep apnea syndrome. Chest 2007, 132, 1832–1838. [Google Scholar] [CrossRef]
- Brill, S.E.; Wedzicha, J.A. Oxygen therapy in acute exacerbations of chronic obstructive pulmonary disease. Int. J. Chronic Obstr. Pulm. Dis 2014, 9, 1241–1252. [Google Scholar] [CrossRef] [Green Version]
- Moloney, E.D.; Kiely, J.L.; McNicholas, W.T. Controlled oxygen therapy and carbon dioxide retention during exacerbations of chronic obstructive pulmonary disease. Lancet 2001, 357, 526–528. [Google Scholar] [CrossRef]
- Chapman, C.L.; Schlader, Z.J.; Reed, E.L.; Worley, M.L.; Johnson, B.D. Renal and segmental artery hemodynamic response to acute, mild hypercapnia. Am. J. Physiol. Regul. Integr. Comp. Physiol. 2020, 318, R822–R827. [Google Scholar] [CrossRef]
- Clements, W.T.; Lee, S.R.; Bloomer, R.J. Nitrate ingestion: A review of the health and physical performance effects. Nutrients 2014, 6, 5224–5264. [Google Scholar] [CrossRef] [Green Version]
- Kerley, C.P.; Cahill, K.; Bolger, K.; McGowan, A.; Burke, C.; Faul, J.; Cormican, L. Dietary nitrate supplementation in COPD: An acute, double-blind, randomized, placebo-controlled, crossover trial. Nitric Oxide 2015, 44, 105–111. [Google Scholar] [CrossRef]
- Friis, A.L.; Steenholt, C.B.; Løkke, A.; Hansen, M. Dietary beetroot juice-effects on physical performance in COPD patients: A randomized controlled crossover trial. Int. J. Chronic Obstr. Pulm. Dis. 2017, 12, 1765–1773. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kemmner, S.; Lorenz, G.; Wobst, J.; Kessler, T.; Wen, M.; Günthner, R.; Stock, K.; Heemann, U.; Burkhardt, K.; Baumann, M.; et al. Dietary nitrate load lowers blood pressure and renal resistive index in patients with chronic kidney disease: A pilot study. Nitric Oxide 2017, 64, 7–15. [Google Scholar] [CrossRef] [PubMed]
- Lundberg, J.O.; Weitzberg, E.; Gladwin, M.T. The nitrate-nitrite-nitric oxide pathway in physiology and therapeutics. Nat. Rev. Drug Discov. 2008, 7, 156–167. [Google Scholar] [CrossRef] [PubMed]
- Ahmad, A.; Dempsey, S.K.; Daneva, Z.; Azam, M.; Li, N.; Li, P.L.; Ritter, J.K. Role of Nitric Oxide in the Cardiovascular and Renal Systems. Int. J. Mol. Sci. 2018, 19, 2605. [Google Scholar] [CrossRef] [Green Version]
- Lahera, V.; Salom, M.G.; Miranda-Guardiola, F.; Moncada, S.; Romero, J.C. Effects of NG-nitro-L-arginine methyl ester on renal function and blood pressure. Am. J. Physiol. 1991, 261, F1033–F1037. [Google Scholar] [CrossRef]
- Sakuma, I.; Togashi, H.; Yoshioka, M.; Saito, H.; Yanagida, M.; Tamura, M.; Kobayashi, T.; Yasuda, H.; Gross, S.S.; Levi, R. NG-methyl-L-arginine, an inhibitor of L-arginine-derived nitric oxide synthesis, stimulates renal sympathetic nerve activity in vivo. A role for nitric oxide in the central regulation of sympathetic tone? Circ. Res. 1992, 70, 607–611. [Google Scholar] [CrossRef] [Green Version]
- Guelen, I.; Westerhof, B.E.; Van Der Sar, G.L.; Van Montfrans, G.A.; Kiemeneij, F.; Wesseling, K.H.; Bos, W.J. Validation of brachial artery pressure reconstruction from finger arterial pressure. J. Hypertens. 2008, 26, 1321–1327. [Google Scholar] [CrossRef]
- Chapman, C.L.; Benati, J.M.; Johnson, B.D.; Vargas, N.T.; Lema, P.C.; Schlader, Z.J. Renal and segmental artery hemodynamics during whole body passive heating and cooling recovery. J. Appl. Physiol. 2019, 127, 974–983. [Google Scholar] [CrossRef]
- Chapman, C.L.; Grigoryan, T.; Vargas, N.T.; Reed, E.L.; Kueck, P.J.; Pietrafesa, L.D.; Bloomfield, A.C.; Johnson, B.D.; Schlader, Z.J. High-fructose corn syrup-sweetened soft drink consumption increases vascular resistance in the kidneys at rest and during sympathetic activation. Am. J. Physiol. Renal. Physiol. 2020, 318, F1053–F1065. [Google Scholar] [CrossRef]
- Chapman, C.L.; Johnson, B.D.; Hostler, D.; Lema, P.C.; Schlader, Z.J. Reliability and agreement of human renal and segmental artery hemodynamics measured using Doppler ultrasound. J. Appl. Physiol. 2020, 128, 627–636. [Google Scholar] [CrossRef]
- Chapman, C.L.; Johnson, B.D.; Vargas, N.T.; Hostler, D.; Parker, M.D.; Schlader, Z.J. Both hyperthermia and dehydration during physical work in the heat contribute to the risk of acute kidney injury. J. Appl. Physiol. 2020, 128, 715–728. [Google Scholar] [CrossRef]
- Schlader, Z.J.; Chapman, C.L.; Benati, J.M.; Gideon, E.A.; Vargas, N.T.; Lema, P.C.; Johnson, B.D. Renal Hemodynamics During Sympathetic Activation Following Aerobic and Anaerobic Exercise. Front. Physiol. 2018, 9, 1928. [Google Scholar] [CrossRef]
- Chapman, C.L.; Johnson, B.D.; Parker, M.D.; Hostler, D.; Pryor, R.R.; Schlader, Z. Kidney physiology and pathophysiology during heat stress and the modification by exercise, dehydration, heat acclimation and aging. Temperature 2020, 8, 108–159. [Google Scholar] [CrossRef]
- Drew, R.C.; Blaha, C.A.; Herr, M.D.; Cui, R.; Sinoway, L.I. Muscle mechanoreflex activation via passive calf stretch causes renal vasoconstriction in healthy humans. Am. J. Physiol. Regul. Integr. Comp. Physiol. 2017, 312, R956–R964. [Google Scholar] [CrossRef] [Green Version]
- Momen, A.; Leuenberger, U.A.; Ray, C.A.; Cha, S.; Handly, B.; Sinoway, L.I. Renal vascular responses to static handgrip: Role of muscle mechanoreflex. Am. J. Physiol. Heart Circ. Physiol. 2003, 285, H1247–H1253. [Google Scholar] [CrossRef] [Green Version]
- Govoni, M.; Jansson, E.A.; Weitzberg, E.; Lundberg, J.O. The increase in plasma nitrite after a dietary nitrate load is markedly attenuated by an antibacterial mouthwash. Nitric Oxide 2008, 19, 333–337. [Google Scholar] [CrossRef] [PubMed]
- Bock, J.M.; Ueda, K.; Schneider, A.C.; Hughes, W.E.; Limberg, J.K.; Bryan, N.S.; Casey, D.P. Inorganic nitrate supplementation attenuates peripheral chemoreflex sensitivity but does not improve cardiovagal baroreflex sensitivity in older adults. Am. J. Physiol. Heart Circ. Physiol. 2018, 314, H45–H51. [Google Scholar] [CrossRef]
- Hughes, W.E.; Ueda, K.; Treichler, D.P.; Casey, D.P. Effects of acute dietary nitrate supplementation on aortic blood pressure and aortic augmentation index in young and older adults. Nitric Oxide 2016, 59, 21–27. [Google Scholar] [CrossRef]
- Casey, D.P.; Treichler, D.P.; Ganger, C.T.t.; Schneider, A.C.; Ueda, K. Acute dietary nitrate supplementation enhances compensatory vasodilation during hypoxic exercise in older adults. J. Appl. Physiol. 2015, 118, 178–186. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wylie, L.J.; Kelly, J.; Bailey, S.J.; Blackwell, J.R.; Skiba, P.F.; Winyard, P.G.; Jeukendrup, A.E.; Vanhatalo, A.; Jones, A.M. Beetroot juice and exercise: Pharmacodynamic and dose-response relationships. J. Appl. Physiol. 2013, 115, 325–336. [Google Scholar] [CrossRef] [Green Version]
- Kenjale, A.A.; Ham, K.L.; Stabler, T.; Robbins, J.L.; Johnson, J.L.; Vanbruggen, M.; Privette, G.; Yim, E.; Kraus, W.E.; Allen, J.D. Dietary nitrate supplementation enhances exercise performance in peripheral arterial disease. J. Appl. Physiol. 2011, 110, 1582–1591. [Google Scholar] [CrossRef] [PubMed]
- Wesseling, K.H.; Jansen, J.R.; Settels, J.J.; Schreuder, J.J. Computation of aortic flow from pressure in humans using a nonlinear, three-element model. J. Appl. Physiol. 1993, 74, 2566–2573. [Google Scholar] [CrossRef]
- Norman, J.; MacIntyre, J.; Shearer, J.; Craigen, I.M.; Smith, G. Effect of carbon dioxide on renal blood flow. Am. J. Physiol. 1970, 219, 672–676. [Google Scholar] [CrossRef]
- Mirmiran, P.; Houshialsadat, Z.; Gaeini, Z.; Bahadoran, Z.; Azizi, F. Functional properties of beetroot (Beta vulgaris) in management of cardio-metabolic diseases. Nutr. Metab. 2020, 17, 3. [Google Scholar] [CrossRef] [Green Version]
- Ramick, M.G.; Kirkman, D.L.; Stock, J.M.; Muth, B.J.; Farquhar, W.B.; Chirinos, J.A.; Doulias, P.T.; Ischiropoulos, H.; Edwards, D.G. The effect of dietary nitrate on exercise capacity in chronic kidney disease: A randomized controlled pilot study. Nitric Oxide 2021, 106, 17–23. [Google Scholar] [CrossRef] [PubMed]
- Van Ryswyk, E.; Mukherjee, S.; Chai-Coetzer, C.L.; Vakulin, A.; McEvoy, R.D. Sleep Disorders, Including Sleep Apnea and Hypertension. Am. J. Hypertens. 2018, 31, 857–864. [Google Scholar] [CrossRef]
- Finks, S.W.; Rumbak, M.J.; Self, T.H. Treating Hypertension in Chronic Obstructive Pulmonary Disease. N. Engl. J. Med. 2020, 382, 353–363. [Google Scholar] [CrossRef]
- Beierwaltes, W.H.; Harrison-Bernard, L.M.; Sullivan, J.C.; Mattson, D.L. Assessment of renal function; clearance, the renal microcirculation, renal blood flow, and metabolic balance. Compr. Physiol. 2013, 3, 165–200. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Pre-Beetroot Juice | Post-Beetroot Juice | p-Value |
|---|---|---|---|
| PETCO2 (mmHg) | 45 (3) | 45 (3) | 0.8557 |
| Mean arterial pressure (mmHg) | 91 (5) | 92 (7) | 0.3929 |
| Heart rate (bpm) | 61 (6) | 63 (9) | 0.2413 |
| Stroke volume (mL) | 93 (14) | 88 (18) | 0.1689 |
| Cardiac output (L/min) | 5.7 (0.8) | 5.4 (0.9) | 0.2234 |
| Total peripheral resistance (mmHg/L/min) | 16.4 (2.6) | 17.7 (3.1) | 0.1021 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chapman, C.L.; Schlader, Z.J.; Reed, E.L.; Worley, M.L.; Johnson, B.D. Acute Beetroot Juice Ingestion Does Not Alter Renal Hemodynamics during Normoxia and Mild Hypercapnia in Healthy Young Adults. Nutrients 2021, 13, 1986. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13061986
Chapman CL, Schlader ZJ, Reed EL, Worley ML, Johnson BD. Acute Beetroot Juice Ingestion Does Not Alter Renal Hemodynamics during Normoxia and Mild Hypercapnia in Healthy Young Adults. Nutrients. 2021; 13(6):1986. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13061986
Chicago/Turabian StyleChapman, Christopher L., Zachary J. Schlader, Emma L. Reed, Morgan L. Worley, and Blair D. Johnson. 2021. "Acute Beetroot Juice Ingestion Does Not Alter Renal Hemodynamics during Normoxia and Mild Hypercapnia in Healthy Young Adults" Nutrients 13, no. 6: 1986. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13061986