
Contextually Appropriate Tools and Solutions to Facilitate Healthy Eating Identified by People with Type 2 Diabetes

 , and
, and
Abstract
:
1. Introduction
2. Materials and Methods
2.1. Design
2.2. Participants
2.3. Procedure
- Select whole and less refined foods instead of processed foods, such as sugar-sweetened beverages, fast foods and refined grains.
- Reduce caloric intake to achieve and maintain a healthier body weight.
- Pay attention to both carbohydrate quality and quantity.
- Select unsaturated oils and nuts as the preferred dietary fats.
- Choose lean animal proteins. Select more vegetable protein.
2.4. Data Analysis
3. Results
3.1. General Characteristics, Background, and Health
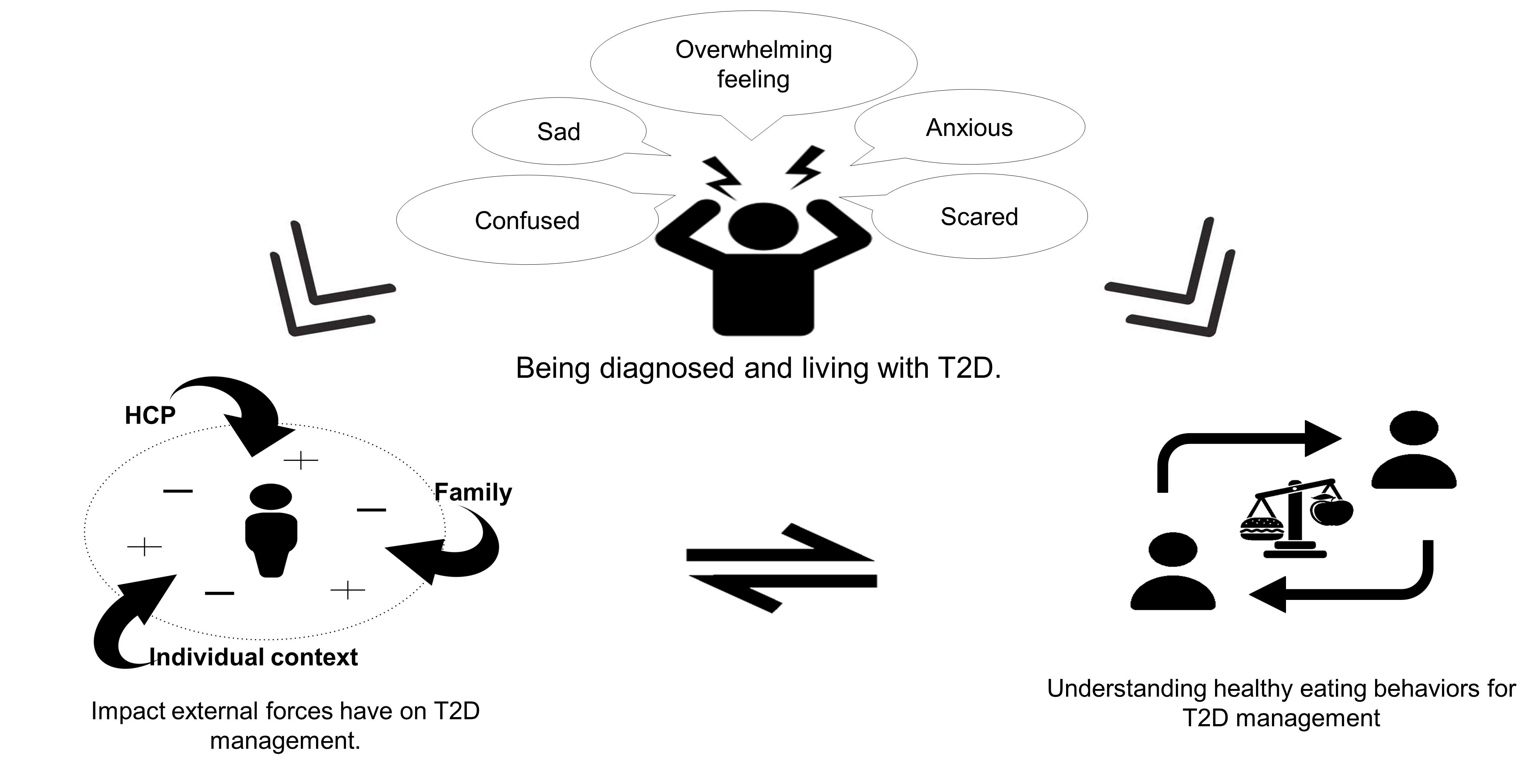
3.1.1. Theme 1: Dealing with Being Diagnosed and Living with T2D
3.1.2. Theme 2: Impact of External Forces on T2D Management
3.1.3. Theme 3: Understanding Healthy Eating Behaviors for T2D Management
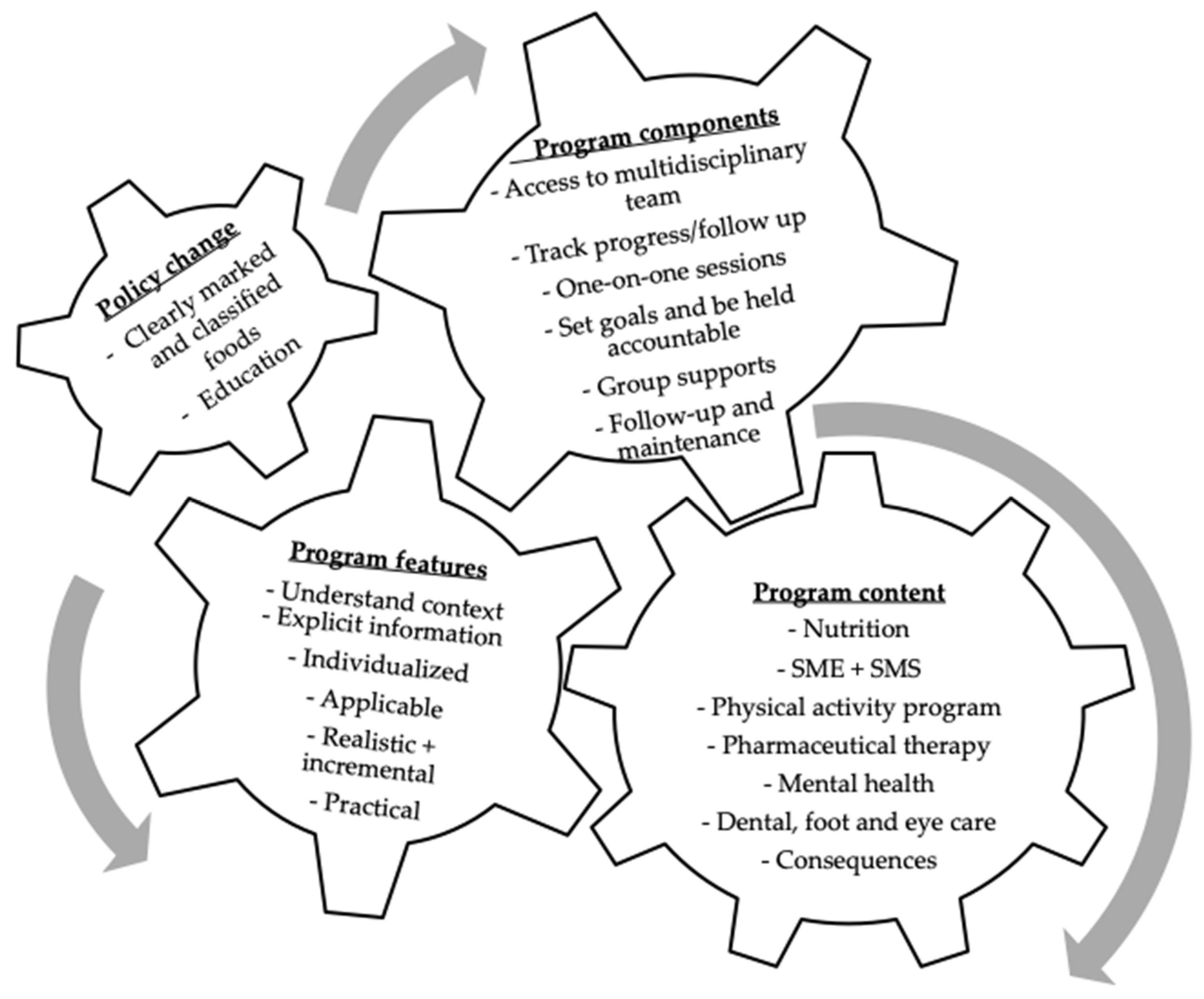
3.1.4. Theme 4: Understanding Needs and Identifying Intervention Components
Program Content
Program Features
Program Components
Policy Change
3.1.5. Theme 5: Participant Advice
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Pearson, E.R. Type 2 diabetes: A multifaceted disease. Diabetologia 2019, 62, 1107–1112. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Diabetes Canada Clinical Practice Guidelines Expert Committee. Diabetes Canada 2018 Clinical Practice Guidelines for the Prevention and Management of Diabetes in Canada. Can. J. Diabetes 2018, 42 (Suppl. S1), S1–S325. [Google Scholar]
- Chen, L.; Pei, J.-H.; Kuang, J.; Chen, H.-M.; Chen, Z.; Li, Z.-W.; Yang, H.-Z. Effect of lifestyle intervention in patients with type 2 diabetes: A meta-analysis. Metabolism 2015, 64, 338–347. [Google Scholar] [CrossRef]
- Lim, L.L.; Lau, E.S.; Kong, A.P.; Davies, M.J.; Levitt, N.S.; Eliasson, B.; Aguilar-Salinas, C.A.; Ning, G.; Seino, Y.; So, W.Y. Aspects of multicomponent integrated care promote sustained improvement in surrogate clinical outcomes: A systematic review and meta-analysis. Diabetes Care 2018, 41, 1312–1320. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brown, S.A. Studies of educational interventions and outcomes in diabetic adults: A meta-analysis revisited. Patient Educ. Couns. 1990, 16, 189–215. [Google Scholar] [CrossRef]
- Johansen, M.Y.; Karstoft, K.; MacDonald, C.S.; Hansen, K.B.; Ellingsgaard, H.; Hartmann, B.; Albrechtsen, N.J.W.; Vaag, A.A.; Holst, J.J.; Pedersen, B.K. Effects of an intensive lifestyle intervention on the underlying mechanisms of improved glycaemic control in individuals with type 2 diabetes: A secondary analysis of a randomised clinical trial. Diabetologia 2020, 63, 2410–2422. [Google Scholar] [CrossRef]
- Cochran, J.; Conn, V.S. Meta-analysis of quality of life outcomes following diabetes self-management training. Diabetes Educ. 2008, 34, 815–823. [Google Scholar] [CrossRef] [Green Version]
- Sherifali, D.; Berard, L.D.; Gucciardi, E.; MacDonald, B.; MacNeill, G. Self-management education and support. Can. J. Diabetes 2018, 42, S36–S41. [Google Scholar] [CrossRef] [Green Version]
- Tricco, A.C.; Ivers, N.M.; Grimshaw, J.M.; Moher, D.; Turner, L.; Galipeau, J.; Halperin, I.; Vachon, B.; Ramsay, T.; Manns, B. Effectiveness of quality improvement strategies on the management of diabetes: A systematic review and meta-analysis. Lancet 2012, 379, 2252–2261. [Google Scholar] [CrossRef]
- Ong, S.E.; Koh, J.J.K.; Toh, S.-A.E.S.; Chia, K.S.; Balabanova, D.; McKee, M.; Perel, P.; Legido-Quigley, H. Assessing the influence of health systems on type 2 diabetes mellitus awareness, treatment, adherence and control: A systematic review. PLoS ONE 2018, 13, e0195086. [Google Scholar] [CrossRef]
- Flood, D.; Hane, J.; Dunn, M.; Brown, S.J.; Wagenaar, B.H.; Rogers, E.A.; Heisler, M.; Rohloff, P.; Chopra, V. Health system interventions for adults with type 2 diabetes in low-and middle-income countries: A systematic review and meta-analysis. PLoS Med. 2020, 17, e1003434. [Google Scholar] [CrossRef]
- Attridge, M.; Creamer, J.; Ramsden, M.; Cannings-John, R.; Hawthorne, K. Culturally appropriate health education for people in ethnic minority groups with type 2 diabetes mellitus. Cochrane Database Syst. Rev. 2014. [Google Scholar] [CrossRef]
- Archundia-Herrera, M.; Subhan, F.B.; Sakowsky, C.; Watkins, K.; Chan, C.B. A Mixed Methods Evaluation of a Randomized Control Trial to Evaluate the Effectiveness of the Pure Prairie Living Program in Type 2 Diabetes Participants. Healthcare 2020, 8, 153. [Google Scholar] [CrossRef]
- Sievenpiper, J.L.; Chan, C.B.; Dworatzek, P.D.; Freeze, C.; Williams, S.L. Nutrition therapy. Can. J. Diabetes 2018, 42, S64–S79. [Google Scholar] [CrossRef]
- Forouhi, N.G.; Misra, A.; Mohan, V.; Taylor, R.; Yancy, W. Dietary and nutritional approaches for prevention and management of type 2 diabetes. Bmj 2018, 361, k2234. [Google Scholar] [CrossRef] [Green Version]
- Baker, P.; Machado, P.; Santos, T.; Sievert, K.; Backholer, K.; Hadjikakou, M.; Russell, C.; Huse, O.; Bell, C.; Scrinis, G. Ultra-processed foods and the nutrition transition: Global, regional and national trends, food systems transformations and political economy drivers. Obes. Rev. 2020, 21, e13126. [Google Scholar] [CrossRef]
- Slater, J. Is cooking dead? The state of Home Economics Food and Nutrition education in a Canadian province. Int. J. Consum. Stud. 2013, 37, 617–624. [Google Scholar] [CrossRef]
- Booth, A.O.; Lowis, C.; Dean, M.; Hunter, S.J.; McKinley, M.C. Diet and physical activity in the self-management of type 2 diabetes: Barriers and facilitators identified by patients and health professionals. Prim. Health Care Res. Dev. 2013, 14, 293–306. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mohr, D.C.; Burns, M.N.; Schueller, S.M.; Clarke, G.; Klinkman, M. Behavioral intervention technologies: Evidence review and recommendations for future research in mental health. Gen. Hosp. Psychiatry 2013, 35, 332–338. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Armstrong, C.; University of Alberta, Edmonton, AB, Canada; Fettig, A.; University of Alberta, Edmonton, AB, Canada. Exploring Patient Experience of Healthy Eating Behaviour Change for Type 2 Diabetes Self-Management. Personal communication, 2020. [Google Scholar]
- Laranjo, L.; Neves, A.L.; Costa, A.; Ribeiro, R.T.; Couto, L.; Sá, A.B. Facilitators, barriers and expectations in the self-management of type 2 diabetes—A qualitative study from Portugal. Eur. J. Gen. Pract. 2015, 21, 103–110. [Google Scholar] [CrossRef]
- Abel, S.; Whitehead, L.; Coppell, K. Making dietary changes following a diagnosis of prediabetes: A qualitative exploration of barriers and facilitators. Diabet. Med. 2018, 35, 1693–1699. [Google Scholar] [CrossRef]
- Carolan, M.; Holman, J.; Ferrari, M. Experiences of diabetes self-management: A focus group study among A ustralians with type 2 diabetes. J. Clin. Nurs. 2015, 24, 1011–1023. [Google Scholar] [CrossRef] [PubMed]
- Patton, M.Q. Qualitative Research & Evaluation Methods: Integrating Theory and Practice; Sage Publications: Southend Oaks, CA, USA, 2014; p. 30. [Google Scholar]
- Tong, A.; Sainsbury, P.; Craig, J. Consolidated criteria for reporting qualitative research (COREQ): A 32-item checklist for interviews and focus groups. Int. J. Qual. Health Care 2007, 19, 349–357. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Campbell-Scherer, D.L.; Asselin, J.; Osunlana, A.M.; Fielding, S.; Anderson, R.; Rueda-Clausen, C.F.; Johnson, J.A.; Ogunleye, A.A.; Cave, A.; Manca, D. Implementation and evaluation of the 5As framework of obesity management in primary care: Design of the 5As Team (5AsT) randomized control trial. Implement. Sci. 2014, 9, 78. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Braun, V.; Clarke, V. Using thematic analysis in psychology. Qual. Res. Psychol. 2006, 3, 77–101. [Google Scholar] [CrossRef] [Green Version]
- Vaismoradi, M.; Turunen, H.; Bondas, T. Content analysis and thematic analysis: Implications for conducting a qualitative descriptive study. Nurs. Health Sci. 2013, 15, 398–405. [Google Scholar] [CrossRef]
- Gustafsson, K.; Andersson, I.; Andersson, J.; Fjellström, C.; Sidenvall, B. Older Women’s Perceptions of Independence Versus Dependence in Food-Related Work. Public Health Nurs. 2003, 20, 237–247. [Google Scholar] [CrossRef] [PubMed]
- Crossley, M.L. Would you consider yourself a healthy person?: Using focus groups to explore health as a moral phenomenon. J. Health Psychol. 2003, 8, 501–514. [Google Scholar] [CrossRef]
- Chambers, S.; Lobb, A.; Butler, L.T.; Traill, W.B. The influence of age and gender on food choice: A focus group exploration. Int. J. Consum. Stud. 2008, 32, 356–365. [Google Scholar] [CrossRef]
- Atkins, L.; Michie, S. Designing interventions to change eating behaviours. Proc. Nutr. Soc. 2015, 74, 164–170. [Google Scholar] [CrossRef]
- Povey, R.; Conner, M.; Sparks, P.; James, R.; Shepherd, R. Interpretations of healthy and unhealthy eating, and implications for dietary change. Health Educ. Res. 1998, 13, 171–183. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lake, A.A.; Hyland, R.M.; Rugg-Gunn, A.J.; Wood, C.E.; Mathers, J.C.; Adamson, A.J. Healthy eating: Perceptions and practice (the ASH30 study). Appetite 2007, 48, 176–182. [Google Scholar] [CrossRef] [PubMed]
- Paquette, M.-C. Perceptions of healthy eating: State of knowledge and research gaps. Can. J. Public Health 2005, 96, S16–S21. [Google Scholar] [CrossRef]
- Bisogni, C.A.; Jastran, M.; Seligson, M.; Thompson, A. How people interpret healthy eating: Contributions of qualitative research. J. Nutr. Educ. Behav. 2012, 44, 282–301. [Google Scholar] [CrossRef]
- Fritschi, C.; Martyn-Nemeth, P.; Zhu, B.; Jung Kim, M. Active learning: Lessons from women with type 2 diabetes in a walking program. Diabetes Educ. 2019, 45, 370–379. [Google Scholar] [CrossRef]
- Mamykina, L.; Heitkemper, E.M.; Smaldone, A.M.; Kukafka, R.; Cole-Lewis, H.J.; Davidson, P.G.; Mynatt, E.D.; Cassells, A.; Tobin, J.N.; Hripcsak, G. Personal discovery in diabetes self-management: Discovering cause and effect using self-monitoring data. J. Biomed. Inform. 2017, 76, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Asselin, J.; Osunlana, A.; Ogunleye, A.; Sharma, A.; Campbell-Scherer, D. Challenges in interdisciplinary weight management in primary care: Lessons learned from the 5As Team study. Clin. Obes. 2016, 6, 124–132. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Torti, J.; Luig, T.; Borowitz, M.; Johnson, J.A.; Sharma, A.M.; Campbell-Scherer, D.L. The 5As team patient study: Patient perspectives on the role of primary care in obesity management. BMC Fam. Pract. 2017, 18, 19. [Google Scholar]
- Luig, T.; Anderson, R.; Sharma, A.; Campbell-Scherer, D. Personalizing obesity assessment and care planning in primary care: Patient experience and outcomes in everyday life and health. Clin. Obes. 2018, 8, 411–423. [Google Scholar] [CrossRef]
- Wharton, S.; Lau, D.C.; Vallis, M.; Sharma, A.M.; Biertho, L.; Campbell-Scherer, D.; Adamo, K.; Alberga, A.; Bell, R.; Boulé, N. Obesity in adults: A clinical practice guideline. CMAJ 2020, 192, E875–E891. [Google Scholar] [CrossRef]
- Black, C.; Lawrence, W.; Cradock, S.; Ntani, G.; Tinati, T.; Jarman, M.; Begum, R.; Inskip, H.; Cooper, C.; Barker, M. Healthy conversation skills: Increasing competence and confidence in front-line staff. Public Health Nutr. 2014, 17, 700–707. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rains, S.A.; Peterson, E.B.; Wright, K.B. Communicating social support in computer-mediated contexts: A meta-analytic review of content analyses examining support messages shared online among individuals coping with illness. Commun. Monogr. 2015, 82, 403–430. [Google Scholar] [CrossRef]
- White, M.; Barquera, S. Mexico Adopts Food Warning Labels, Why Now? Health Syst. Reform 2020, 6, e1752063. [Google Scholar] [CrossRef] [PubMed]
- Ferdinands, A.R.; Olstad, D.L.; Milford, K.M.; Maximova, K.; Nykiforuk, C.I.; Raine, K.D. A Nutrition Report Card on food environments for children and youth: 5 years of experience from Canada. Public Health Nutr. 2020, 23, 2088–2099. [Google Scholar] [CrossRef]
- Moore, A.P.; Rivas, C.A.; Stanton-Fay, S.; Harding, S.; Goff, L.M. Designing the Healthy Eating and Active Lifestyles for Diabetes (HEAL-D) self-management and support programme for UK African and Caribbean communities: A culturally tailored, complex intervention under-pinned by behaviour change theory. BMC Public Health 2019, 19, 1146. [Google Scholar] [CrossRef] [PubMed]
- Sandelowski, M. Sample size in qualitative research. Res. Nurs. Helath 1995, 18, 179–183. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Variables | Mean (Min–Max) | |
|---|---|---|
| Age (years) | 61.4 (33–79) | |
| Diabetes diagnosis (years) | 12.6 (5–25) | |
| n (%) | ||
| Gender | Female | 8 (53) |
| Male | 7 (47) | |
| Ethnicity | Aboriginal | 3 (20) |
| Black | 1 (7) | |
| White | 11 (73) | |
| Education | High school or less | 1 (7) |
| More than high school | 14 (93) | |
| Employment status | Working | 4 (27) |
| Retirement | 7 (47) | |
| Other | 3 (20) | |
| Not reported | 1 (7) | |
| Household annual income | <$59,999 | 4 (27) |
| >$60,000 | 9 (60) | |
| Not reported | 2 (29) | |
| Annual income | <Meet needs | 1 (7) |
| >Meet needs | 13 (87) | |
| Not reported | 1 (7) | |
| SME + SMS | Nutrition Therapy | Physical Activity | Pharmacological Therapy |
|---|---|---|---|
|
|
|
|
| Theme | Example Quotes |
|---|---|
| Theme 1: Dealing with being diagnosed and living with diabetes | |
| Feelings | “Lots of anxiety. Sometimes I will just be like ‘why waste my time? I’m dying anyway.”—PT153 |
| “Doing a whole change like [DM management] … it’s overwhelming.”—PT300 | |
| Engagement | “I have a family history of diabetes. My father was diagnosed at approximately the same age that I was. Uh, he did not particularly look after himself that well, as a result of which he died at age 70 from diabetes complications. And I am determined that I am not gonna go the same way. I will do what I need to do to maintain my health as best as I can.”—PT364 |
| “People who have a reason to live take better care of their bodies than people who don’t have a reason to live. The fact that I have, uh, a grandson now that I adore and I’m more open to going back to the diet and exercise than I was 6 months ago or 6 years ago, that’s not coincidental. That’s just the way life goes.”—PT132 | |
| Theme 2: The impact that external forces have on T2D management | |
| Health care providers | “He was a specialist, first of all, and he was, like, following me really closely and we talked a little bit about things I could do, and he was giving me a purpose. ‘In six months, I want you to come back with lower numbers!’ I was like ‘okay. I’m terrified.’ But six months, I try whatever I can.”—PT153 |
| “My doctor just sent me to diabetes classes […], he had me meet with a nurse as well, every 3 months I believe, to go over, you know, like the—the health issues with the blood pressure, the feet. Stuff like that. So, uh… you know, he’s maintained this… you know, over the last 10 years. Like I go every year for this assistance with the nurse and he… you know, validates my blood work and stuff. So, like, I’ve had the help.”—PT149 | |
| “Completely demeaning... it was painful and awful. And then you walk in to some guy’s office and he looks at—I have a log book of everyday, 5 times a day when I was stabbing myself with insulin, every unit—and he looks at me—he says ‘well, these aren’t the right numbers. I think you’ve got too many zeros on these.’ And I was like ‘I can recall every single stab. Every single time I had fluid pockets under my skin from injecting that much subcutaneous—like you can’t tell me that I’m lying or that I don’t know what I’m talking about.’ So it’s—it was pretty bad... And he sends me back with metformin which, you know, my other—my—my specialist had counseled me was not a good option for breastfeeding. So it was—it was a terrible time.”—PT623 | |
| “So I never went back because she [RD] “This is what you can do. Solve your lunch problem and everything will be fine”. So I thought well how could I go back to tell her I don’t like the plan? It wasn’t working.”—PT38 | |
| Family | “I’m lucky that my wife still likes to cook and that she’s a really good cook and she likes flavorful food, which I do.”—PT70 |
| “My wife supports me. She supports 110% so I’ve got a very good support system.”—PT178 | |
| “My wife still doesn’t understand what I should be eating. I—our diets are separate. I cook my own food. I… buy my own groceries. I eat separately. ‘Cause my wife—I don’t think really has an understanding of what I should or shouldn’t be eating and also it then becomes restrictive on what she can eat.”—PT555 | |
| “I think that’s what a lot of people… that I’ve talked to are missing is that they’ve, you know, they’ve got the diabetes. They’re trying to make the changes. But you’re not eat—you’re not getting the support from your family. And if you’re the one that’s doing the cooking and providing the food and your family’s not willing to change to allow you to have a better diet then… it’s—it’s hard for you to do it.”—PT364 | |
| Life situation | “In my career I also travelled a lot and I think that was probably one of the onsets of diabetes was that I was travelling… in hotels, eating in restaurants continuously… eating very, very badly. Limited activity and bad food.”—PT555 |
| “I’ll buy groceries, I’ll buy this, I’ll buy the cauliflower, I’ll buy the—I like the stuff. And yet, I guess because what I use as an excuse there is I’m driving my husband places. I’m driving my granddaughter places. I’m going out to [grandson’s name]. I’m going out to look after [grandson’s name] a couple times a week. And I get home at 5 or 6 and I don’t feel like cooking much. So I mean it’s a lot easier to have, um… What do I usually… well order a pizza or something.”—PT38 | |
| “The fact that back home I wasn’t really the one cooking...here, I had to cook for myself, which was a new experience [stammers] a—a really new experience for me, coupled with the fact that I had to use ingredients I wasn’t really familiar with.”—PT153 | |
| “Our income is quite limited and a fair amount of stress exists in my head because of that and that affects what we buy, what we do and I’m trying to think of ways to economize and yet, uh, try to get better quality of vegetables, and yet, on the other hand, um, I think I’d like to have some more meat into our diet.”—PT115 | |
| “Now with this Covid, and that’s a poor excuse, but it is a reality too, you know what I mean? Because I had tried to—I had joined the [name] Rec Centre on March 5th. I did one day. And then it was closed after that.”—PT149 | |
| “A lot of people are feeling a strain of not being able to get out and about with all their friends and relatives and that, and that’s making everything more difficult for them.”—PT364 | |
| Theme 3: Understanding healthy eating behaviors for T2D management | |
| Nutrition knowledge | “It’s a balance of things, you gotta do your whole grains, you have to do your fruits, you have to do your vegetables. Um, naturally occurring… I guess sugars if you’re going to consume sugars like from fruit, from watermelons, the things that your body can digest, staying away from the manufactured to the man-made or the artificial stuff. So that’s where I think of… not—healthy eating. Rather than dealing with process, anything that’s natural.”—PT178 |
| “Healthy eating’ would be, um, an equal—you, know, making sure that you put your proteins in. You’re, um, making sure that most of your plate is vegetables and fruit as compared to carbs and proteins.”—PT159 | |
| “Basically following Canada’s food guide. You know, that’s basically how you should do it.”—PT149 | |
| “To me that would mean, um, sort of a mix of foods and—and kind of a balanced mix. So, uh, right amount of vegetables and fruits. Um, uh—um—the—the correct amounts or—or balanced amount of protein, carbohydrates, vegetables, fruits, um, combined with, you know, enough liquids to keep it all working.”—PT70 | |
| Behavior cycle | “There’s that initial transition on diagnosis and trying to—trying to get better control and better behaviors. And—and then there’s the—the kind of the long haul process of, um, trying to follow the guidelines and… the temptation is always around you, all the time. Um… And, you know, over time, I found that I able to… to—to stick with the rules but every once in while that just gets boring or, you know… I just can’t—I don’t want to do that anymore. I take a break for a day or a meal. Um, and then feel guilty about that and get back on track.”—PT70 |
| “I’ve just in to the habit of doing what I think I need to do and, you know, if I… feel that I’m not getting enough exercise, maybe I’ll just go out and do a little bit more or… you know… Yeah, occasionally I’ll eat probably what I shouldn’t eat but then [smacks lips] realizing I’ve done, I try to make the rest of the day or the next day that I’m eating more sensibly and I’m watching what I’m doing to kind of counter balance when I do sort of fall of the wagon.”—PT364 | |
| “My problem, again, is night eating. Even getting up in the middle of the night to eat. So I could eat very healthy throughout the whole day and be within, um, the right category, um, of carbs, sugars, etcetera, and proteins, and then I would have my downfall in the middle of the night.”—PT159 | |
| “Even though I know moving for health is—it’s good just to get out and do a walk… […] So sometimes you say ‘forget it. I’m just not gonna go.’ I become lazy and—and, you know, sedentary and decide not to do it, right?”—PT149 | |
| Theme | Example Quotes |
|---|---|
| Theme 4: Understanding needs and identifying intervention components | |
| Program Content | |
| Nutrition | “What’s in food? How do you read label? So, you know, getting to know that, um… you know, eating a—a bran muffin at Tim Hortons is the same as eating 4 slices of white bread with butter. You know, it was an eye opener.”—PT555 |
| “I’d like a diabetic diet that allowed a blowout once a week or something on stuff you really enjoy as opposed, it just feels like you’re following such a regimen and it’s just you never get to escape it. Or if you do you’re, you’re feeling guilty about it, but.”—PT115 | |
| Physical activity | “Some sort of exercise program where you can encourage people to maybe get together even if it’s just something as simple as walking. You know. Meet every few days, once a week or whatever and just… go for a walk somewhere where you can talk to each other. You’re doing the same activity, you can support each other and, you know, okay, well, you know, you’re getting tired. “Well, why don’t you go just a little bit farther and you’ll feel better type of thing.”—PT364 |
| “Exercise was not my fortitude. Still isn’t. So, like, maybe perhaps someone, uh, to go with me, to train me, that would work.”—PT153 | |
| Hands-on learning | “Help them understand […] something as simple as eating a meal, taking your blood sugars before, during, after, uh, then doing the same thing the next day but going for a walk for 15 min and seeing, you know, doing the same measurements and seeing the change. And it’s like ‘okay. Hmm. That—I—I can see it, you know. I can see what the combination of diet and exercise does for my blood sugars. Even on a short-term basis, so….”—PT70 |
| “Packing an emergency kit and what does that look like.”—PT132 | |
| Mental health | “Having a support system, uh, ack—acknowledging that there’s a, um, there’s a mental, uh, a mental side, um, helps fight the—the disease is really important, cause if you don’t address that… it’s not going to work.”—PT153 |
| “Having the mental health improved is… I think it’s primary. If you need to… If you’re gonna have success with something, I think you need to make sure your brain is working right.”—PT97 | |
| Foot care | “Foot care […] it’s important to always look after your feet, make sure that you don’t—when you put your shoes, that you shake your shoes out. You—you wipe the bottom of your foot off before you put your foot into the shoe. So she’s [nurse] very remindful of that because she knows that the extremities… you can, you know, if you’re stepping on a stone or something in your shoe that, you know, and you don’t feel it—as the diabetes progresses and you don’t feel it, you can get like a sore and sometimes that sore doesn’t heal.”—PT149 |
| Consequences | “They mention, yeah, you’re gonna get heart disease, you’re gonna gain weight. This is gonna happen, yes you can lose a toe, a foot, that—but—but they don’t really show… pictures, they don’t make it graphic.”—PT178 |
| Program features | |
| Understand context | “The idea of trying to… um… trying to understand who the participant and—and sort of where they’re coming from, what they’re… possibilities, opportunities, you know, lifestyle, um… their whole life situation is, uh… will make it easier to… to figure out… how they—what kind of changes they can make most readily that will, you know, be good changes for them to make.”—PT70 |
| “You gotta kind of understand what—you know, where people are at […] find people’s ‘whys.’ People have a ‘why.’ You just gotta find it and then relate it to them. And so that will help them… be on track for things.”—PT623 | |
| Explicit information | “An overall household plan for diet. But the biggest thing, and I’ll you that is really… very specific, you know, if you’re gonna down and have a breakfast, this is what a good breakfast it. This is what a bad breakfast is.”—PT555 |
| “So having someone help me, for example, going for the low-the glycemic index food. And explain how it works. That would be amazing. Because I go for the—I know what it is. Like I said I have a bachelor degree in science, but even that is not helping because I’m just overwhelmed with the fact that I’m the sick person […] Having someone going through the list again and explaining in light of… the dia—the diabetes I have, will be, actually, more effective. Why do you want have low glycemic index food in your—your plate? Uh, how much of this do you want to have? That would be great.”—PT153 | |
| Individualized | “Getting, um, uh, oh, like a guideline, do you know what I mean? As to what I should be eating, how much I should be eating or what—what—how much amount of carbohydrate, protein, and fat and—and—that I should be having at my age and my weight.”—PT149 |
| “The North American diet’s changed so much and as Indigenous people, that was not our diet. Uh, I mean, before contact, you know, we had a very specific diet and probably a very limited diet. And with the in-introduction to refined foods and such, it’s… it’s been really, really bad for Indigenous people so… what is that dietary pattern? What it is? Should—when should we be eating? And what should we be eating.”—PT364 | |
| Applicable | “Kind of train people to look for what that looks like at the drive through window at Tim Hortons or McDonalds.”—PT132 |
| “Teaching them how to go from very big portions to smaller […] learning to wean yourself off of your portion sizes.”—PT178 | |
| Realistic and incremental | “I think what—what maybe help—would help people is instead of just doing a… a whole—well, we gotta change from here to here, um, we need to change your—basically your whole eating habits, maybe—maybe just start ‘okay, we’re gonna try… no pop for these two weeks’ and then ‘okay, you can do that. Alright. Um… the next 2 weeks, let’s not have hamburger. Or if you gotta have hamburger, make it lean’ or… you know, that kind of thing. Uh, ‘eat chicken instead of beef.’ Um… do incremental steps maybe, um… instead of doing the whole—the whole… the whole big change.”—PT300 |
| “What’s feasible for you to do without demanding some extraordinary effort or some kind of effort that’s—that’s really not natural to you. That—that is too significant a change for you to make. Maybe by taking a smaller step, you may eventually achieve a larger set of steps, but, um… So I—to me, I think that’s—that’s part of the core of the practicality of some programs, is that, you know, while holding out sort the ideal… um, showing people that you can—you can at least make progress towards the ideal by taking a small step or two small steps, or you know… Along that line.”—PT70 | |
| Practical | “Getting the cognitive understanding or practicality in regards to that instead of just saying well you should just have less. Well then, with the program of feeling full they said have a hamburger, but cut it in half and have half now and have half later. That was a practical application of exactly what you should do and how to do it. Right?”—PT87 |
| “Maybe you should come up with a line of diabetic fast foods. There’s my assignment for you.”—PT115 | |
| Program components | |
| Access to multidisciplinary team | “Having access to the nurse, from time to time, with this program, it was really good, because now I—I had someone I could actually ask questions from time to time. So that did make the experience a little bit easier to go through.”—PT153 |
| “When I talked about the pharmacy… uh, oh, at [name of pharmacy], that was one of the best sessions because it was a very—it was one to one. It was open. And as the pharmacist said ‘ask any question. There’s no dumb questions here.’ So I really began to ask, you know… a lot of questions and he had a much more, uh, layman explanation for things—simple things.”—PT555 | |
| Track progress/ follow up | “I really do need a coach in a way. I don’t know how assertive the coach has to be with me but just something to remind me or to give me the incentive to keep going.”—PT115 |
| “Having a support to call and say ‘ok, I’m struggling with this.’ ‘How do I… you know, I can’t figure out how to do this with this particular item.’ You know? And I also got this and this on it. You know?”—PT159 | |
| One-on-one sessions | “Somehow we still deal with what we should be doing and maybe more one-on-one time, going over it and asking where we were struggling. What is it, you know, um, allowed us to not complete it? Or just the follow through on it all. I mean, do we have to be babysat? Again, I’m thinking this is an older group that you’re working with, more so, and, um—I don’t know, maybe we need more hand-holding.”—PT159 |
| “How have you changed because of the information you’ve gotten? What have you been able to stick to? What do you have trouble with? And let’s, you know, let’s take another step.’ You know? Or I would even, um, [smacks lips] you know, at first, maybe just—let’s just talk breakfast for a week, right, like just revamp breakfast and then ‘what did you like? What sticks with you?’ You know, it’s just—it’s just that learning isn’t a one-time thing. It has to evolve and change. You know?”—PT555 | |
| Set goals and be held accountable | “Maybe having them set goals? Beforehand and be accountable. And then check in with them, like, ‘why? This is what you wanted. Why—you know, when you’re not here, what do we need tweak, what do we need to change? Do you need to do a repeat? Do you need to, you know…’ but have something, cause in the beginning they will be motivated.”—PT159 |
| “Not getting off so easy if you were supposed to go home and do homework and you came back without—‘oh, I didn’t have time’, you know […] Penalize us. Charge us. Charge us for the course. It’s free but unless you don’t do it, then you have to pay back.”—PT159 | |
| Group support | “I think people are incredibly lonely. I think there is a case to be made for, um, a support group that doesn’t stop. A support group that genuinely cares about one another.”—PT132 |
| “Maybe even sort of a—a mentorship or a one-on-one where somebody that’s had diabetes for a few years can kind of look after or talk to somebody that’s just starting on the—the—the journey through and can let them know that, you know, some of the things that they’re gonna find, some of the problems they may have and that just… I guess let them that there’s somebody there that can help them or just—just talk to them and support them.”—PT364 | |
| Follow-up and maintenance | “I wish they had continued on with them [diabetes classes] and doing them because I think taking something like that every couple of years as sort of a refresher just helps kind of confirm that you’re doing what’s right and, you know, the—you know, the recommendations are changing over time so to make sure you’re doing what they’re recommending nowadays, you do and opposed to what they recommended 5 years ago.”—PT364 |
| “Follow-up, partnerships, groups. It’s the same as dealing with a, a 12-step program. You keep on going to meetings to reinforce. And that’s what [name of commercial program] uses. Right? The support systems.”—PT87 | |
| Policy change | |
| Clearly marked food items | “To have, uh, from the side of the people that are running these stores, spaces that are clearly marked with the good choices, with the good snacks, uh to do something on that side, so that people know this is a good choice. You know, even if it’s a, you know, seal of approval or something from somebody that says this a good thing to eat [...] Have an awards program for the, the, uh, the convenience stores of who does it and how well they do it, and to actually give them some kind of trophy or cash-incentive or something for their good work towards, you know, the health.”—PT132 |
| Education | “If you can get young people where they can get that education, it—it probably is going help them a lot more than… […] just, you know, us talking about it all the time. If you’re learning it when you’re young… […] then you got a better chance of following through later in life.”—PT364 |
| Theme | Example Quotes |
|---|---|
| Theme 5: Participant advice | |
| Healthy habits | “Try and reorganize or recognize your, uh, your stomach as your basic guide and things like eating what you want but only eating half the amount. Things like that where you’re recognizing when you’re full, and uh, that most of the time you’re eating when? you’re not hungry.”—PT87 |
| “We will sit down and come up with ideas about a weekly menu and sort of what we’d like to eat.”—PT70 | |
| “Anything that you can maintain for the rest of life is the kind of change that you want to make.”—PT623 | |
| “I, uh, have gone away from that, uh… sort of, uh, empty calories and such, like I said, I don’t eat in the evenings anymore. So don’t sit in front of the TV and eat potato chips or anything like that.”—PT555 | |
| “Do the medical things, have your eye exam and your… you know… Uh, exam for your… your kidney—your kidney levels and all that sort of stuff and, you know, if they recommend doing it once a year, then try and do it once a year so that if you are gonna start developing problems, you’re—you’re getting ahead of the game and maybe you can prevent them from getting really bad.”—PT364 | |
| “I honestly think… I’m overweight, for the most part of—because of the… size of portions I was having. Um… so I… watched the… quantity I’m actually eating. And… I… I had a bad habit of having soda for super. Um… so I don’t have that anymore and I have—try having water. Um… and yeah. Um… I try to… instead of just having meat and—and pasta and that kind of stuff I try to have a side of salad or vegetables or something like that to go along with the meal […] trying to have fresh vegetables around.”—PT300 | |
| “My wife, when she quit smoking, she started doing the dishes after supper because normally she would finish the meal, go sit on the front porch or whatever to have a cigarette and then clean up. She changed that habit from instead of smoking after supper, she does the dishes, right away. She gave up smoking because she replaced the smoking with doing dishes. Do something to replace the time when you eat. Find out when you always wanna snack, and when you feel that urge, do something. Uh, I don’t know, take up a hobby, do puzzles, do… uh, crosswords, whatever.”—PT178 | |
| Healthy eating | “Eliminate my snacking after supper and changing my meal pattern from largest at supper to the largest meal at breakfast. Or lunch.”—PT178 |
| “Less pop. You know, well, no pop actually, I shouldn’t say less pop. No pop. Carbonated water instead.”—PT159 | |
| “Try to eat seasonally.”—PT70 | |
| “Use the whole grains. Even if I go out, I ask for a whole grain bun.”—PT149 | |
| “Lots of water. Lots of water.”—PT132 | |
| “Just try and remember, eat veggies.”—PT115 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Archundia Herrera, M.C.; Campbell-Scherer, D.L.; Bell, R.C.; Chan, C.B. Contextually Appropriate Tools and Solutions to Facilitate Healthy Eating Identified by People with Type 2 Diabetes. Nutrients 2021, 13, 2301. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13072301
Archundia Herrera MC, Campbell-Scherer DL, Bell RC, Chan CB. Contextually Appropriate Tools and Solutions to Facilitate Healthy Eating Identified by People with Type 2 Diabetes. Nutrients. 2021; 13(7):2301. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13072301
Chicago/Turabian StyleArchundia Herrera, M. Carolina, Denise L. Campbell-Scherer, Rhonda C. Bell, and Catherine B. Chan. 2021. "Contextually Appropriate Tools and Solutions to Facilitate Healthy Eating Identified by People with Type 2 Diabetes" Nutrients 13, no. 7: 2301. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13072301