
The Contribution of Foods and Beverages of Low Nutritional Value to the Diets of Swedish Adolescents, by Food Group, Time and Place. A Nationally Representative Study

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Population an, d Sampling
2.3. Dietary Assessment
2.4. Definition of Discretionary Foods
2.5. The Eating Index Scores SHEIA15 and RADDS
2.6. Data from Questionnaires
2.7. Anthropometry and Blood Sampling
2.8. Biomarkers of Nutritional Status
2.9. Statistics
3. Results
3.1. The Study Population and Mean Intakes of Energy and Macronutrients
3.2. What Are the Main Discretionary Foods Consumed?
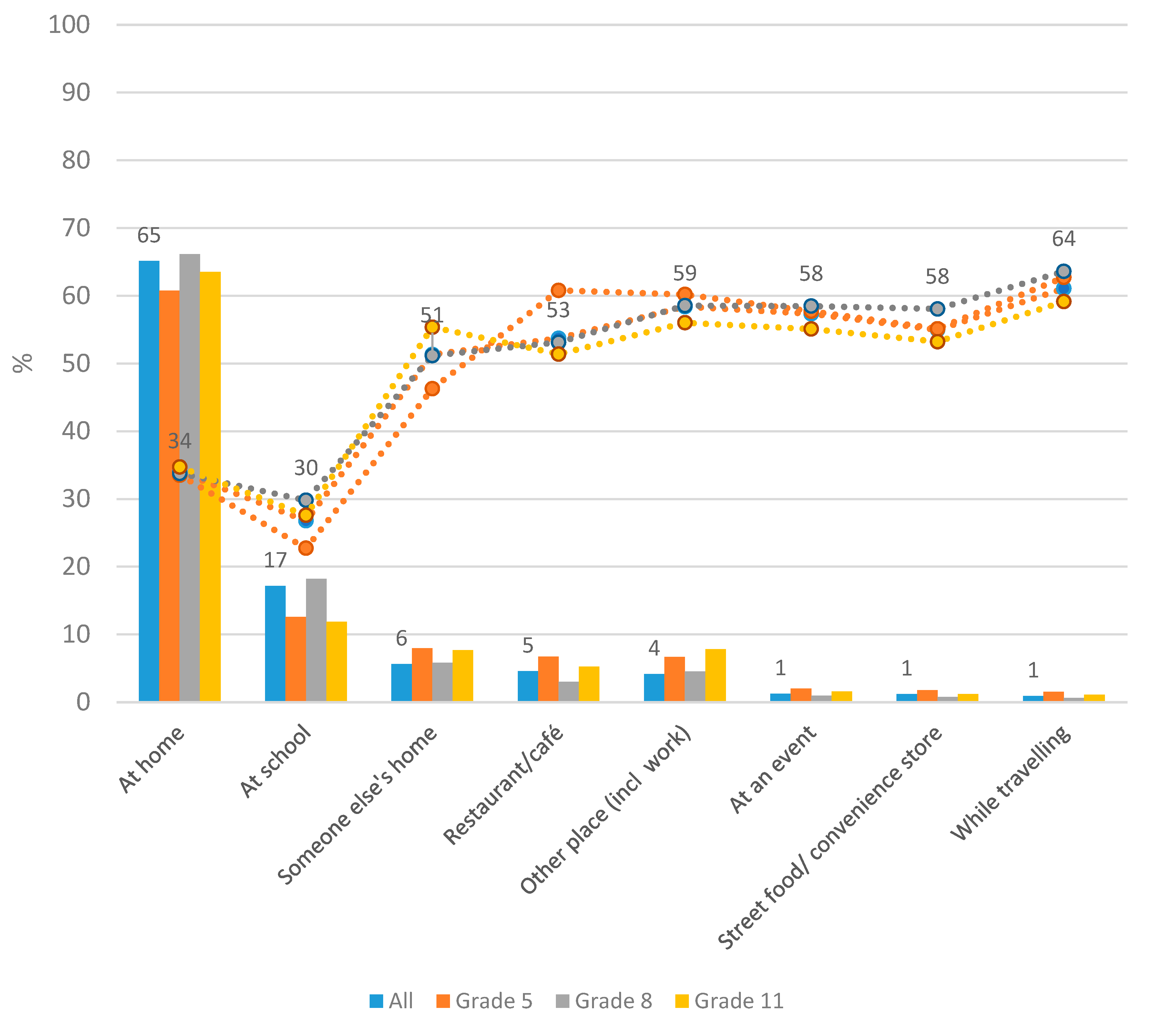
3.3. Where Are Most Discretionary Foods Consumed?
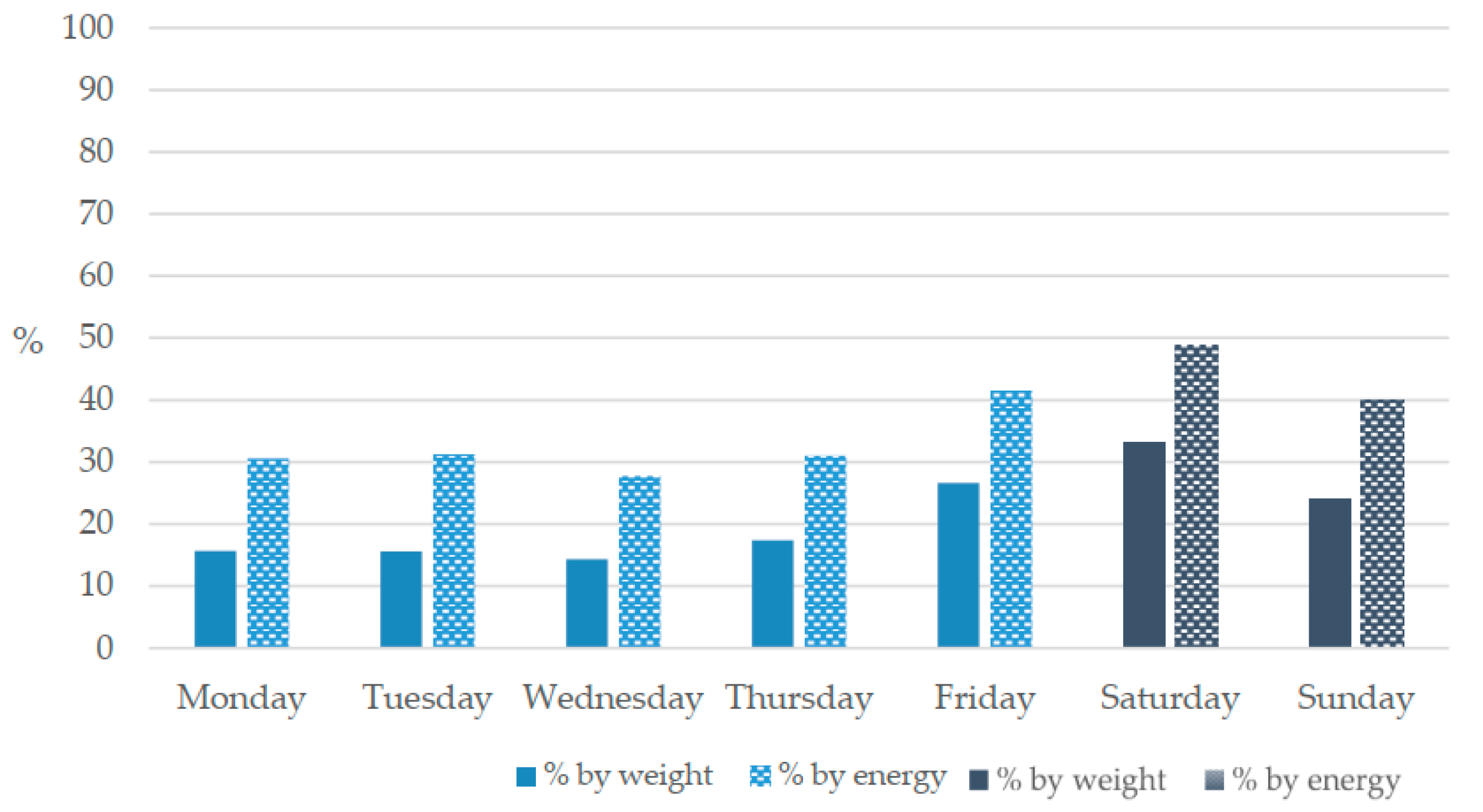
3.4. When Are Most Discretionary Foods Consumed?
3.5. Nutritional Status and Healthy Diet Scores according to Consumption Levels of Discretionary Foods/Beverages
4. Discussion
Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- GBD Risk Factors Collaborators. Global burden of 87 risk factors in 204 countries and territories, 1990–2019: A systematic analysis for the Global Burden of Disease Study 2019. Lancet 2020, 396, 1223–1249. [Google Scholar] [CrossRef]
- Craigie, A.M.; Lake, A.A.; Kelly, S.A.; Adamson, A.J.; Mathers, J.C. Tracking of obesity-related behaviours from childhood to adulthood: A systematic review. Maturitas 2011, 70, 266–284. [Google Scholar] [CrossRef] [Green Version]
- Story, M.; Neumark-Sztainer, D.; French, S. Individual and environmental influences on adolescent eating behaviors. J. Am. Diet. Assoc. 2002, 102, S40–S51. [Google Scholar] [CrossRef]
- Viner, R.M.; Ross, D.; Hardy, R.; Kuh, D.; Power, C.; Johnson, A.; Wellings, K.; McCambridge, J.; Cole, T.J.; Kelly, Y.; et al. Life course epidemiology: Recognising the importance of adolescence. J. Epidemiol. Community Health 2015, 69, 719–720. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moreno, L.A.; Gottrand, F.; Huybrechts, I.; Ruiz, J.R.; González-Gross, M.; DeHenauw, S.; Group, H.S. Nutrition and lifestyle in european adolescents: The Helena (Healthy Lifestyle in Europe by Nutrition in Adolescence) study. Adv. Nutr. 2014, 5, 615S–623S. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Banfield, E.C.; Liu, Y.; Davis, J.S.; Chang, S.; Frazier-Wood, A.C. Poor Adherence to US Dietary Guidelines for Children and Adolescents in the National Health and Nutrition Examination Survey Population. J. Acad. Nutr. Diet. 2016, 116, 21–27. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brettschneider, A.-K.; Lage Barbosa, C.; Haftenberger, M.; Lehmann, F.; Mensink, G.B. Adherence to food-based dietary guidelines among adolescents in Germany according to socio-economic status and region: Results from Eating Study as a KiGGS Module (EsKiMo) II. Public Health Nutr. 2021, 24, 1216–1228. [Google Scholar] [CrossRef]
- Desbouys, L.; Méjean, C.; De Henauw, S.; Castetbon, K. Socio-economic and cultural disparities in diet among adolescents and young adults: A systematic review. Public Health Nutr. 2020, 23, 843–860. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lemming, E.W.; Moraeus, L.; Petrelius Sipinen, J.; Lindroos, A.K. Riksmaten ungdom 2016–17. Del 1. Livsmedelskonsumtion bland ungdomar i åk 5, åk 8 och åk 2 på gymnasiet; Livsmedelverkets Rapportserie nr 14; Livsmedelsverket: Uppsala, Sweden, 2018. [Google Scholar]
- Wanselius, J.; Axelsson, C.; Moraeus, L.; Berg, C.; Mattisson, I.; Larsson, C. Procedure to Estimate Added and Free Sugars in Food Items from the Swedish Food Composition Database Used in the National Dietary Survey Riksmaten Adolescents 2016–17. Nutrients 2019, 11, 1342. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moraeus, L.; Lindroos, A.K.; Warensjö Lemming, E.; Mattisson, I. Diet diversity score and healthy eating index in relation to diet quality and socio-demographic factors: Results from a cross-sectional national dietary survey of Swedish adolescents. Public Health Nutr. 2020, 23, 1754–1765. [Google Scholar] [CrossRef] [Green Version]
- National Health and Medical Research Council. Australian Dietary Guidelines; National Health and Medical Research Council: Canberra, Australia, 2013.
- Lee, A.; Rangan, A.; Allman-Farinelli, M.; Chen, J.; Grech, A.; McDonald, S.; Wilson, A. A Rapid Review of Evidence: Discretionary Food and Drinks; The Australian Prevention Partnership Centre: Glebe, NSW, Australia, 2018. [Google Scholar]
- 001—Australian Health Survey: Users’ Guide, 2011–2013. Available online: https://www.abs.gov.au/ausstats/[email protected]/Lookup/BA1526F0D19FA21DCA257CD2001CA166?opendocument (accessed on 16 July 2021).
- Bell, A.C.; Kremer, P.J.; Magarey, A.M.; Swinburn, B.A. Contribution of ‘noncore’ foods and beverages to the energy intake and weight status of Australian children. Eur. J. Clin. Nutr. 2005, 59, 639–645. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rangan, A.M.; Randall, D.; Hector, D.J.; Gill, T.P.; Webb, K.L. Consumption of ‘extra’ foods by Australian children: Types, quantities and contribution to energy and nutrient intakes. Eur. J. Clin. Nutr. 2008, 62, 356–364. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rangan, A.M.; Schindeler, S.; Hector, D.J.; Gill, T.P.; Webb, K.L. Consumption of ‘extra’ foods by Australian adults: Types, quantities and contribution to energy and nutrient intakes. Eur. J. Clin. Nutr. 2009, 63, 865–871. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Johnson, L.; van Jaarsveld, C.H.M.; Wardle, J. Individual and family environment correlates differ for consumption of core and non-core foods in children. Br. J. Nutr. 2011, 105, 950–959. [Google Scholar] [CrossRef]
- Toumpakari, Z.; Haase, A.M.; Johnson, L. Adolescents’ non-core food intake: A description of what, where and with whom adolescents consume non-core foods. Public Health Nutr. 2016, 19, 1645–1653. [Google Scholar] [CrossRef] [Green Version]
- Toumpakari, Z.; Tilling, K.; Haase, A.M.; Johnson, L. High-risk environments for eating foods surplus to requirements: A multilevel analysis of adolescents’ non-core food intake in the National Diet and Nutrition Survey (NDNS). Public Health Nutr. 2019, 22, 74–84. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aburto, T.C.; Pedraza, L.S.; Sánchez-Pimienta, T.G.; Batis, C.; Rivera, J.A. Discretionary Foods Have a High Contribution and Fruit, Vegetables, and Legumes Have a Low Contribution to the Total Energy Intake of the Mexican Population. J. Nutr. 2016, 146, 1881S–1887S. [Google Scholar] [CrossRef] [Green Version]
- Slining, M.M.; Popkin, B.M. Trends in intakes and sources of solid fats and added sugars among U.S. children and adolescents: 1994–2010. Pediatr. Obes. 2013, 8, 307–324. [Google Scholar] [CrossRef] [Green Version]
- Harnack, L.; Stang, J.; Story, M. Soft drink consumption among US children and adolescents: Nutritional consequences. J. Am. Diet. Assoc. 1999, 99, 436–441. [Google Scholar] [CrossRef]
- Sjoberg, A.; Hulthen, L. Comparison of food habits, iron intake and iron status in adolescents before and after the withdrawal of the general iron fortification in Sweden. Eur. J. Clin. Nutr. 2015, 69, 494–500. [Google Scholar] [CrossRef]
- Moraeus, L.; Lemming, E.W.; Hursti, U.-K.K.; Arnemo, M.; Sipinen, J.P.; Lindroos, A.K. Riksmaten Adolescents 2016–17: A national dietary survey in Sweden-design, methods, and participation. Food Nutr. Res. 2018, 62. [Google Scholar] [CrossRef] [Green Version]
- Lindroos, A.K.; Petrelius Sipinen, J.; Axelsson, C.; Nyberg, G.; Landberg, R.; Leanderson, P.; Arnemo, M.; Warensjö Lemming, E. Use of a Web-Based Dietary Assessment Tool (RiksmatenFlex) in Swedish Adolescents: Comparison and Validation Study. J. Med. Internet Res. 2019, 21, e12572. [Google Scholar] [CrossRef] [Green Version]
- Australian Health Survey—Discretionary Food List. Available online: https://www.abs.gov.au/AUSSTATS/[email protected]/DetailsPage/4363.0.55.0012011-13?OpenDocument (accessed on 16 July 2021).
- Cole, T.J.; Lobstein, T. Extended international (IOTF) body mass index cut-offs for thinness, overweight and obesity. Pediatr. Obes. 2012, 7, 284–294. [Google Scholar] [CrossRef]
- de Onis, M.; Onyango, A.W.; Borghi, E.; Siyam, A.; Nishida, C.; Siekmann, J. Development of a WHO growth reference for school-aged children and adolescents. Bull. World Health Organ. 2007, 85, 660–667. [Google Scholar] [CrossRef] [PubMed]
- Meyer, H.E.; Robsahm, T.E.; Bjørge, T.; Brustad, M.; Blomhoff, R. Vitamin D, season, and risk of prostate cancer: A nested case-control study within Norwegian health studies. Am. J. Clin. Nutr. 2013, 97, 147–154. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Krebs-Smith, S.M.; Kott, P.S.; Guenther, P.M. Mean proportion and population proportion: Two answers to the same question? J. Am. Diet. Assoc. 1989, 89, 671–676. [Google Scholar] [PubMed]
- StataCorp. Stata Statistical Software: Release 15; StataCorp LLC.: College Station, TX, USA, 2018. [Google Scholar]
- Fayet-Moore, F.; McConnell, A.; Kim, J.; Mathias, K.C. Identifying Eating Occasion-Based Opportunities to Improve the Overall Diets of Australian Adolescents. Nutrients 2017, 9, 608. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Patterson, E.; Wärnberg, J.; Kearney, J.; Sjöström, M. Sources of saturated fat and sucrose in the diets of Swedish children and adolescents in the European Youth Heart Study: Strategies for improving intakes. Public Health Nutr. 2010, 13, 1955–1964. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Libuda, L.; Alexy, U.; Buyken, A.E.; Sichert-Hellert, W.; Stehle, P.; Kersting, M. Consumption of sugar-sweetened beverages and its association with nutrient intakes and diet quality in German children and adolescents. Br. J. Nutr. 2009, 101, 1549–1557. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Doherty, A.M.; Lacko, A.M.; Popkin, B.M. Sugar-sweetened beverage (SSB) consumption is associated with lower quality of the non-SSB diet in US adolescents and young adults. Am. J. Clin. Nutr. 2021, 113, 657–664. [Google Scholar] [CrossRef]
- Malik, V.S.; Pan, A.; Willett, W.C.; Hu, F.B. Sugar-sweetened beverages and weight gain in children and adults: A systematic review and meta-analysis. Am. J. Clin. Nutr. 2013, 98, 1084–1102. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tyrrell, R.L.; Greenhalgh, F.; Hodgson, S.; Wills, W.J.; Mathers, J.C.; Adamson, A.J.; Lake, A.A. Food environments of young people: Linking individual behaviour to environmental context. J. Public Health 2017, 39, 95–104. [Google Scholar] [CrossRef] [PubMed]
- Ziauddeen, N.; Page, P.; Penney, T.L.; Nicholson, S.; Kirk, S.F.; Almiron-Roig, E. Eating at food outlets and leisure places and “on the go” is associated with less-healthy food choices than eating at home and in school in children: Cross-sectional data from the UK National Diet and Nutrition Survey Rolling Program (2008–2014). Am. J. Clin. Nutr. 2018, 107, 992–1003. [Google Scholar] [CrossRef] [PubMed]
- Eustachio Colombo, P.; Patterson, E.; Elinder, L.S.; Lindroos, A.K. The importance of school lunches to the overall dietary intake of children in Sweden: A nationally representative study. Public Health Nutr. 2020, 23, 1705–1715. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Svensson, A.; Larsson, C.; Eiben, G.; Lanfer, A.; Pala, V.; Hebestreit, A.; Huybrechts, I.; Fernández-Alvira, J.M.; Russo, P.; Koni, A.C.; et al. European children’s sugar intake on weekdays versus weekends: The IDEFICS study. Eur. J. Clin. Nutr. 2014, 68, 822–828. [Google Scholar] [CrossRef]
- Nordman, M.; Matthiessen, J.; Biltoft-Jensen, A.; Ritz, C.; Hjorth, M.F. Weekly variation in diet and physical activity among 4–75-year-old Danes. Public Health Nutr. 2020, 23, 1350–1361. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Giménez-Legarre, N.; Miguel-Berges, M.L.; Flores-Barrantes, P.; Santaliestra-Pasías, A.M.; Moreno, L.A. Breakfast Characteristics and Its Association with Daily Micronutrients Intake in Children and Adolescents—A Systematic Review and Meta-Analysis. Nutrients 2020, 12, 3201. [Google Scholar] [CrossRef] [PubMed]
- Medin, A.C.; Myhre, J.B.; Diep, L.M.; Andersen, L.F. Diet quality on days without breakfast or lunch—Identifying targets to improve adolescents’ diet. Appetite 2019, 135, 123–130. [Google Scholar] [CrossRef] [PubMed]
- Coulthard, J.D.; Palla, L.; Pot, G.K. Breakfast consumption and nutrient intakes in 4–18-year-olds: UK National Diet and Nutrition Survey Rolling Programme (2008–2012). Br. J. Nutr. 2017, 118, 280–290. [Google Scholar] [CrossRef] [Green Version]
- Lemming, E.W.; Moraeus, L.; Petrelius Sipinen, J.; Lindroos, A.K. Riksmaten ungdom 2016–17. Del 2. Näringsintag och näringsstatus bland ungdomar i åk 5, åk 8 och åk 2 på gymnasiet; Livsmedelverkets Rapportserie nr 23; Livsmedelsverket: Uppsala, Sweden, 2018. [Google Scholar]
- Lamberg-Allardt, C.; Brustad, M.; Meyer, H.E.; Steingrimsdottir, L. Vitamin D—A systematic literature review for the 5th edition of the Nordic Nutrition Recommendations. Food Nutr. Res. 2013, 57, 22671. [Google Scholar] [CrossRef] [Green Version]
- Nordic Council of Ministers. Nordic Nutrition Recommendations 2012. Integrating Nutrition and Physical Activity, 5th ed.; Nordic Council of Ministers: Copenhagen, Denmark, 2014. [Google Scholar] [CrossRef]
- Gasser, C.E.; Mensah, F.K.; Russell, M.; Dunn, S.E.; Wake, M. Confectionery consumption and overweight, obesity, and related outcomes in children and adolescents: A systematic review and meta-analysis. Am. J. Clin. Nutr. 2016, 103, 1344–1356. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Statskontoret. En analys av några offentliga styrmedel för bättre matvanor; Stadskontoret: Stockholm, Sweden, 2019. [Google Scholar]



{kind=link}
{kind=link}
| School Grade: 5th | 8th | 11th | ||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Girls | (N = 599) | Boys | (N = 490) | Girls | (N = 574) | Boys | (N = 476) | Girls | (N = 577) | Boys | (N = 423) | |||||||
| Age (mean, sd) | 11.5 | 0.4 | 11.5 | 0.4 | 14.5 | 0.4 | 14.5 | 0.4 | 17.7 | 0.6 | 17.7 | 0.6 | ||||||
| High SEP, N (%) | 351 | 62.8 | 285 | 58.2 | 347 | 60.5 | 260 | 54.6 | 298 | 51.6 | 217 | 51.3 | ||||||
| Born in Sweden, N (%) | 517 | 92.5 | 442 | 90.2 | 515 | 89.7 | 408 | 85.7 | 507 | 87.9 | 359 | 84.9 | ||||||
| Overweight/obese, N (%) | 125 | 22.4 | 104 | 21.2 | 101 | 17.6 | 80 | 16.8 | 127 | 22.0 | 109 | 25.8 | ||||||
| All foods/beverages | Mean | SD | Mean | SD | Mean | SD | Mean | SD | Mean | SD | Mean | SD | ||||||
| Weight, g | 1990 | 594 | 2109 | 743 | 2114 | 655 | 2599 | 947 | 2303 | 788 | 2872 | 1008 | ||||||
| Energy (MJ) | 7.8 | 2.7 | 8.4 | 3.1 | 8.0 | 2.8 | 10.7 | 4.3 | 8.2 | 2.7 | 10.9 | 3.9 | ||||||
| Protein, g | 75 | 26 | 86 | 33 | 74 | 26 | 108 | 45 | 73 | 26 | 116 | 52 | ||||||
| Total fat, g | 72 | 32 | 78 | 37 | 76 | 33 | 100 | 47 | 79 | 33 | 103 | 42 | ||||||
| Saturated fat, g | 29 | 14 | 31 | 16 | 30 | 15 | 40 | 20 | 30 | 13 | 40 | 18 | ||||||
| Carbohydrates, g | 218 | 79 | 230 | 92 | 221 | 83 | 292 | 132 | 225 | 79 | 287 | 115 | ||||||
| Added sugar, g | 61 | 43 | 49 | 36 | 66 | 45 | 52 | 38 | 67 | 46 | 51 | 41 | ||||||
| Fibre, g | 16 | 6 | 17 | 7 | 17 | 8 | 20 | 10 | 18 | 9 | 20 | 10 | ||||||
| …of which discretionary foods/beverages (%) | ||||||||||||||||||
| Mean | SD | % | Mean | SD | % | Mean | SD | % | Mean | SD | % | Mean | SD | % | Mean | SD | % | |
| Weight, g | 376 | 293 | 19 | 417 | 368 | 20 | 387 | 287 | 18 | 555 | 427 | 21 | 487 | 404 | 21 | 690 | 588 | 24 |
| Energy (MJ) | 2.8 | 2.1 | 36 | 2.8 | 2.3 | 34 | 2.9 | 2.1 | 37 | 3.8 | 3.0 | 36 | 3.2 | 2.1 | 39 | 4.0 | 2.8 | 37 |
| Protein, g | 15 | 13 | 20 | 16 | 16 | 19 | 15 | 14 | 20 | 21 | 21 | 19 | 15 | 13 | 21 | 25 | 28 | 22 |
| Total fat, g | 35 | 27 | 49 | 34 | 31 | 44 | 36 | 27 | 47 | 45 | 36 | 45 | 38 | 27 | 48 | 45 | 33 | 44 |
| Saturated fat, g | 14 | 12 | 48 | 14 | 14 | 45 | 15 | 12 | 50 | 19 | 15 | 48 | 15 | 11 | 50 | 18 | 14 | 45 |
| Carbohydrates, g | 73 | 62 | 33 | 75 | 71 | 33 | 78 | 65 | 35 | 104 | 104 | 36 | 84 | 63 | 37 | 104 | 87 | 36 |
| Added sugar, g | 51 | 42 | 84 | 39 | 34 | 80 | 57 | 43 | 86 | 43 | 37 | 83 | 58 | 45 | 87 | 42 | 39 | 82 |
| Fibre, g | 3 | 3 | 19 | 3 | 4 | 18 | 3 | 4 | 18 | 4 | 5 | 20 | 4 | 4 | 22 | 4 | 5 | 20 |
| N | % of Total E that Is Disc. | p * | |
|---|---|---|---|
| SEP | <0.001 | ||
| Low | 1341 | 37.7 | |
| High | 1758 | 35.5 | |
| Grade | <0.001 | ||
| 5th | 1049 | 34.9 | |
| 8th | 1050 | 36.5 | |
| 11th | 1000 | 37.8 | |
| Gender | 0.001 | ||
| Girls | 1710 | 37.4 | |
| Boys | 1389 | 35.5 | |
| Country of birth | 0.007 | ||
| Sweden | 2748 | 36.7 | |
| Not Sweden | 337 | 34.0 |
| All (N = 3099) | |||||
|---|---|---|---|---|---|
| Foods from Food Group | % of Disc. E | % of Total E | |||
| Sweets, chocolate | 15.7 | 5.7 | |||
| Pies, pizza, sandwiches * | 14.5 | 5.3 | |||
| Sugar-sweetened beverages | 10.8 | 3.9 | |||
| Cakes, biscuits | 10.0 | 3.6 | |||
| Crisps, savoury snacks | 6.2 | 2.3 | |||
| Sausages * | 5.7 | 2.1 | |||
| Sauces, dressings * | 5.0 | 1.8 | |||
| Potato products and dishes * | 4.4 | 1.6 | |||
| Mixed fat spread * | 4.3 | 1.5 | |||
| Desserts, ice cream | 4.2 | 1.5 | |||
| School grade: 5th | |||||
| Girls (N = 599) | Boys (N = 490) | ||||
| % of disc. E | % of total E | % of disc. E | % of total E | ||
| Sweets, chocolate | 16.5 | 5.9 | Pies, pizza, sandwiches * | 14.5 | 4.9 |
| Pies, pizza, sandwiches * | 11.8 | 4.2 | Sweets, chocolate | 13.6 | 4.6 |
| Cakes, biscuits | 11.0 | 3.9 | Sugar-sweetened beverages | 11.0 | 3.7 |
| Sugar-sweetened beverages | 9.1 | 3.3 | Sausages * | 8.8 | 3.0 |
| Sausages * | 6.7 | 2.4 | Cakes, biscuits | 7.4 | 2.5 |
| Crisps, savoury snacks | 5.6 | 2.0 | Crisps, savoury snacks | 6.3 | 2.1 |
| Desserts, ice cream | 5.1 | 1.9 | Potato products and dishes * | 5.0 | 1.7 |
| Mixed fat spread * | 5.1 | 1.8 | Desserts, ice cream | 4.3 | 1.4 |
| Potato products and dishes * | 4.8 | 1.7 | Mixed fat spread * | 4.3 | 1.4 |
| Sauces, dressings * | 4.3 | 1.6 | Sausage dishes | 4.0 | 1.3 |
| 8th | |||||
| Girls (N = 574) | Boys (N = 476) | ||||
| % of disc. E | % of total E | % of disc. E | % of total E | ||
| Sweets, chocolate | 21.4 | 7.9 | Sweets, chocolate | 18.1 | 6.5 |
| Cakes, biscuits | 13.0 | 4.8 | Pies, pizza, sandwiches * | 16.6 | 6.0 |
| Pies, pizza, sandwiches * | 12.4 | 4.6 | Sugar-sweetened beverages | 11.3 | 4.1 |
| Sugar-sweetened beverages | 8.9 | 3.3 | Cakes, biscuits | 8.2 | 2.9 |
| Crisps, savoury snacks | 5.7 | 2.1 | Crisps, savoury snacks | 6.4 | 2.3 |
| Desserts, ice cream | 4.6 | 1.7 | Sausages * | 5.3 | 1.9 |
| Sauces, dressings * | 4.6 | 1.7 | Potato products and dishes * | 4.9 | 1.8 |
| Mixed fat spread * | 4.6 | 1.7 | Sausage dishes | 4.6 | 1.6 |
| Sausage dishes | 4.0 | 1.5 | Sauces, dressings * | 4.3 | 1.5 |
| Sausages * | 3.8 | 1.4 | Mixed fat spread * | 3.6 | 1.3 |
| 11th | |||||
| Girls (N = 577) | Boys (N = 423) | ||||
| % of disc. E | % of total E | % of disc. E | % of total E | ||
| Sweets, chocolate | 15.5 | 6.1 | Pies, pizza, sandwiches * | 17.0 | 6.2 |
| Pies, pizza, sandwiches * | 14.2 | 5.5 | Sugar-sweetened beverages | 13.6 | 5.0 |
| Cakes, biscuits | 12.3 | 4.8 | Sweets, chocolate | 8.6 | 3.2 |
| Sugar-sweetened beverages | 10.9 | 4.3 | Cakes, biscuits | 7.5 | 2.7 |
| Sauces, dressings * | 7.4 | 2.9 | Crisps, savoury snacks | 7.0 | 2.6 |
| Crisps, savoury snacks | 6.2 | 2.4 | Sausages | 6.4 | 2.3 |
| Mixed fat spread * | 4.8 | 1.9 | Sauces, dressings * | 5.1 | 1.9 |
| Desserts, ice cream | 4.5 | 1.8 | Potato products and dishes * | 4.9 | 1.8 |
| Sausages | 3.9 | 1.5 | Desserts, ice cream | 3.5 | 1.3 |
| Potato products and dishes * | 3.8 | 1.5 | Mixed fat spread * | 3.3 | 1.2 |
| All (N = 3099) | ||
|---|---|---|
| % of Total E | % of Which Is Disc. E | |
| Breakfast | 18.7 | 19 |
| Pies, pizza, sandwiches * | 0.9 | |
| Mixed fat spread * | 0.8 | |
| Cakes, biscuits | 0.3 | |
| Lunch | 25.2 | 28 |
| Pies, pizza, sandwiches * | 1.2 | |
| Sausages * | 0.8 | |
| Sugar-sweetened beverages | 0.7 | |
| Dinner | 32.4 | 33 |
| Pies, pizza, sandwiches * | 2.5 | |
| Sugar-sweetened beverages | 1.6 | |
| Potato products and dishes * | 1.0 | |
| Snack/between meal | 9.2 | 36 |
| Cakes, biscuits | 0.9 | |
| Sweets, chocolate | 0.4 | |
| Pies, pizza, sandwiches * | 0.4 | |
| Other | 13.3 | 82 |
| Sweets, chocolate | 4.7 | |
| Cakes, biscuits | 2.0 | |
| Crisps, savoury snacks | 1.8 | |
| Beverage (mainly) | 1.2 | 72 |
| Sugar-sweetened beverages | 0.4 | |
| Cider, alcopops | 0.2 | |
| Beer | 0.1 | |
| School Grade: 5th | 8th | 11th | ||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Girls | Boys | Girls | Boys | Girls | Boys | |||||||||||||||||||
| Biomarkers * | N | mean | sd | P | N | mean | sd | P | N | mean | sd | P | N | mean | sd | P | N | mean | sd | P | N | mean | sd | P |
| Folat (nmol/L) | 0.075 | 0.103 | 0.641 | 0.144 | 0.258 | 0.231 | ||||||||||||||||||
| Quartile 1 | 45 | 14.4 | 5.8 | 43 | 14.1 | 5.9 | 59 | 13.0 | 5.5 | 45 | 14.0 | 5.4 | 57 | 12.3 | 8.0 | 35 | 10.3 | 4.8 | ||||||
| Quartile 2 | 41 | 12.9 | 5.6 | 39 | 13.8 | 5.2 | 59 | 12.6 | 5.6 | 45 | 12.5 | 4.3 | 54 | 11.7 | 5.1 | 34 | 9.5 | 6.2 | ||||||
| Quartile 3 | 43 | 12.7 | 4.9 | 41 | 12.9 | 6.3 | 58 | 11.8 | 5.6 | 44 | 14.3 | 9.5 | 55 | 10.9 | 6.2 | 36 | 9.4 | 5.7 | ||||||
| Quartile 4 | 45 | 12.6 | 5.4 | 40 | 12.1 | 6.5 | 57 | 13.4 | 6.3 | 41 | 11.3 | 5.1 | 54 | 11.0 | 6.4 | 31 | 9.0 | 3.4 | ||||||
| Ferritin (µg/L) | 0.747 | 0.752 | 0.867 | 0.797 | 0.843 | 0.447 | ||||||||||||||||||
| Quartile 1 | 44 | 30.4 | 12.9 | 42 | 41.4 | 25.5 | 58 | 28.1 | 22.0 | 45 | 33.9 | 22.0 | 53 | 31.6 | 24.4 | 35 | 69.8 | 36.8 | ||||||
| Quartile 2 | 40 | 33.2 | 20.1 | 36 | 45.7 | 19.2 | 59 | 28.1 | 23.6 | 43 | 26.6 | 16.5 | 48 | 25.3 | 15.1 | 32 | 48.9 | 23.1 | ||||||
| Quartile 3 | 42 | 35.0 | 19.1 | 41 | 38.1 | 19.0 | 55 | 27.0 | 21.6 | 42 | 36.6 | 19.1 | 45 | 40.1 | 37.1 | 33 | 61.3 | 38.0 | ||||||
| Quartile 4 | 45 | 30.6 | 16.0 | 39 | 40.6 | 16.7 | 56 | 29.0 | 25.1 | 40 | 36.1 | 17.9 | 51 | 28.0 | 21.4 | 29 | 76.2 | 37.2 | ||||||
| 25(OH)D (nmol/L) | 0.668 | 0.214 | 0.723 | 0.424 | 0.157 | 0.353 | ||||||||||||||||||
| Quartile 1 | 43 | 49.8 | 15.3 | 43 | 57.5 | 17.0 | 59 | 49.9 | 17.3 | 45 | 53.5 | 13.7 | 56 | 51.5 | 20.6 | 34 | 46.3 | 17.8 | ||||||
| Quartile 2 | 38 | 48.7 | 12.3 | 38 | 54.8 | 13.1 | 59 | 53.9 | 19.0 | 47 | 55.7 | 16.4 | 54 | 49.3 | 21.1 | 33 | 49.3 | 15.0 | ||||||
| Quartile 3 | 43 | 52.6 | 13.2 | 42 | 55.9 | 11.5 | 59 | 55.0 | 17.8 | 45 | 52.8 | 15.5 | 56 | 55.6 | 23.5 | 36 | 49.2 | 14.8 | ||||||
| Quartile 4 | 42 | 50.4 | 14.7 | 42 | 53.7 | 17.2 | 55 | 51.7 | 15.2 | 41 | 52.1 | 17.8 | 56 | 56.4 | 21.4 | 34 | 41.3 | 15.1 | ||||||
| Weight status | ||||||||||||||||||||||||
| BMI-sds | 0.487 | 0.079 | 0.314 | 0.964 | 0.056 | 0.875 | ||||||||||||||||||
| Quartile 1 | 139 | 0.26 | 1.15 | 116 | 0.51 | 1.18 | 143 | 0.24 | 1.02 | 119 | 0.22 | 1.10 | 140 | 0.29 | 0.92 | 100 | 0.32 | 1.17 | ||||||
| Quartile 2 | 138 | 0.30 | 1.24 | 120 | 0.60 | 1.13 | 142 | 0.06 | 1.00 | 118 | 0.17 | 1.08 | 141 | 0.32 | 0.90 | 101 | 0.41 | 1.15 | ||||||
| Quartile 3 | 139 | 0.42 | 1.18 | 122 | 0.38 | 1.18 | 144 | 0.27 | 0.92 | 119 | 0.13 | 1.06 | 138 | 0.40 | 0.93 | 102 | 0.17 | 1.04 | ||||||
| Quartile 4 | 136 | 0.32 | 0.99 | 121 | 0.31 | 1.17 | 143 | 0.30 | 0.98 | 119 | 0.24 | 1.16 | 138 | 0.49 | 0.96 | 101 | 0.38 | 1.16 | ||||||
| Dietary quality scores * | ||||||||||||||||||||||||
| SHEIA15 | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | ||||||||||||||||||
| Quartile 1 | 140 | 6.2 | 0.6 | 123 | 6.0 | 0.6 | 144 | 6.3 | 0.7 | 119 | 6.1 | 0.8 | 145 | 6.5 | 0.9 | 106 | 6.0 | 0.8 | ||||||
| Quartile 2 | 140 | 6.0 | 0.6 | 122 | 5.8 | 0.7 | 143 | 6.2 | 0.8 | 119 | 5.9 | 0.8 | 144 | 6.1 | 0.7 | 106 | 5.6 | 0.8 | ||||||
| Quartile 3 | 140 | 5.8 | 0.6 | 123 | 5.7 | 0.7 | 144 | 5.9 | 0.7 | 119 | 5.5 | 0.8 | 144 | 5.7 | 0.9 | 106 | 5.5 | 0.8 | ||||||
| Quartile 4 | 139 | 5.5 | 0.7 | 122 | 5.4 | 0.6 | 143 | 5.4 | 0.7 | 119 | 5.3 | 0.8 | 144 | 5.5 | 0.8 | 105 | 5.0 | 0.8 | ||||||
| RADDS | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | ||||||||||||||||||
| Quartile 1 | 140 | 6.3 | 1.7 | 123 | 5.8 | 1.9 | 144 | 6.3 | 1.9 | 119 | 6.1 | 2.1 | 145 | 6.5 | 2.0 | 106 | 6.2 | 1.809 | ||||||
| Quartile 2 | 140 | 6.6 | 1.5 | 122 | 5.9 | 1.5 | 143 | 6.6 | 1.9 | 119 | 5.9 | 1.9 | 144 | 6.2 | 1.8 | 106 | 5.6 | 1.783 | ||||||
| Quartile 3 | 140 | 6.1 | 1.7 | 123 | 5.7 | 1.8 | 144 | 6.2 | 1.8 | 119 | 5.5 | 1.9 | 144 | 5.7 | 1.9 | 106 | 5.5 | 1.858 | ||||||
| Quartile 4 | 139 | 5.5 | 1.7 | 122 | 5.2 | 1.7 | 143 | 5.2 | 1.8 | 119 | 4.7 | 1.8 | 144 | 5.1 | 1.9 | 105 | 4.3 | 1.491 | ||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lindroos, A.K.; Moraeus, L.; Sipinen, J.P.; Lemming, E.W.; Patterson, E. The Contribution of Foods and Beverages of Low Nutritional Value to the Diets of Swedish Adolescents, by Food Group, Time and Place. A Nationally Representative Study. Nutrients 2021, 13, 2450. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13072450
Lindroos AK, Moraeus L, Sipinen JP, Lemming EW, Patterson E. The Contribution of Foods and Beverages of Low Nutritional Value to the Diets of Swedish Adolescents, by Food Group, Time and Place. A Nationally Representative Study. Nutrients. 2021; 13(7):2450. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13072450
Chicago/Turabian StyleLindroos, Anna Karin, Lotta Moraeus, Jessica Petrelius Sipinen, Eva Warensjö Lemming, and Emma Patterson. 2021. "The Contribution of Foods and Beverages of Low Nutritional Value to the Diets of Swedish Adolescents, by Food Group, Time and Place. A Nationally Representative Study" Nutrients 13, no. 7: 2450. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13072450