
Hair EDX Analysis—A Promising Tool for Micronutrient Status Evaluation of Patients with IBD?

 , , ,
, , , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects
2.2. Hair Sample Collection and SEM and EDX Measurement
2.3. Ethical Considerations
2.4. Statistical Analysis
3. Results
3.1. Patient Characteristics
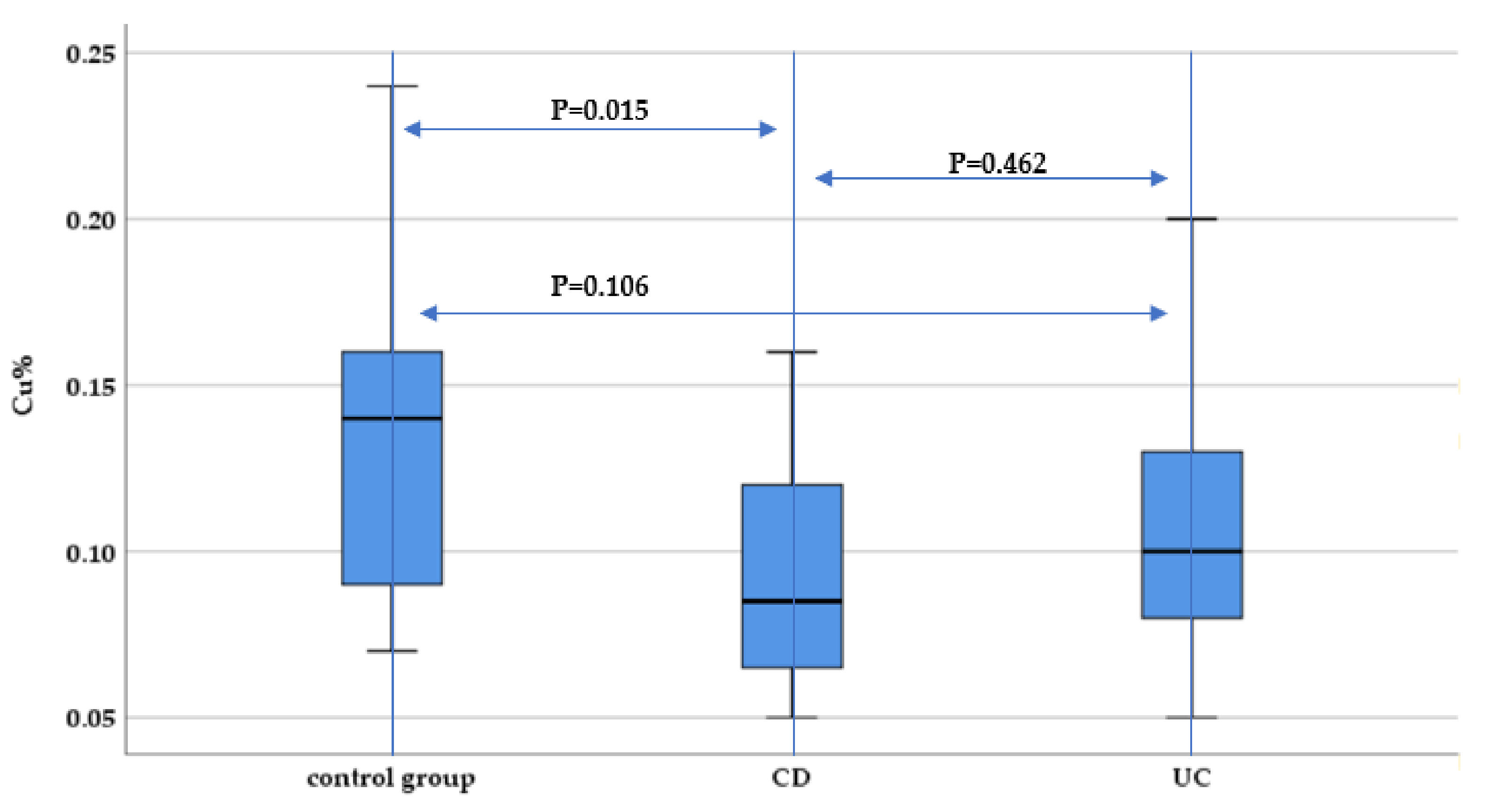
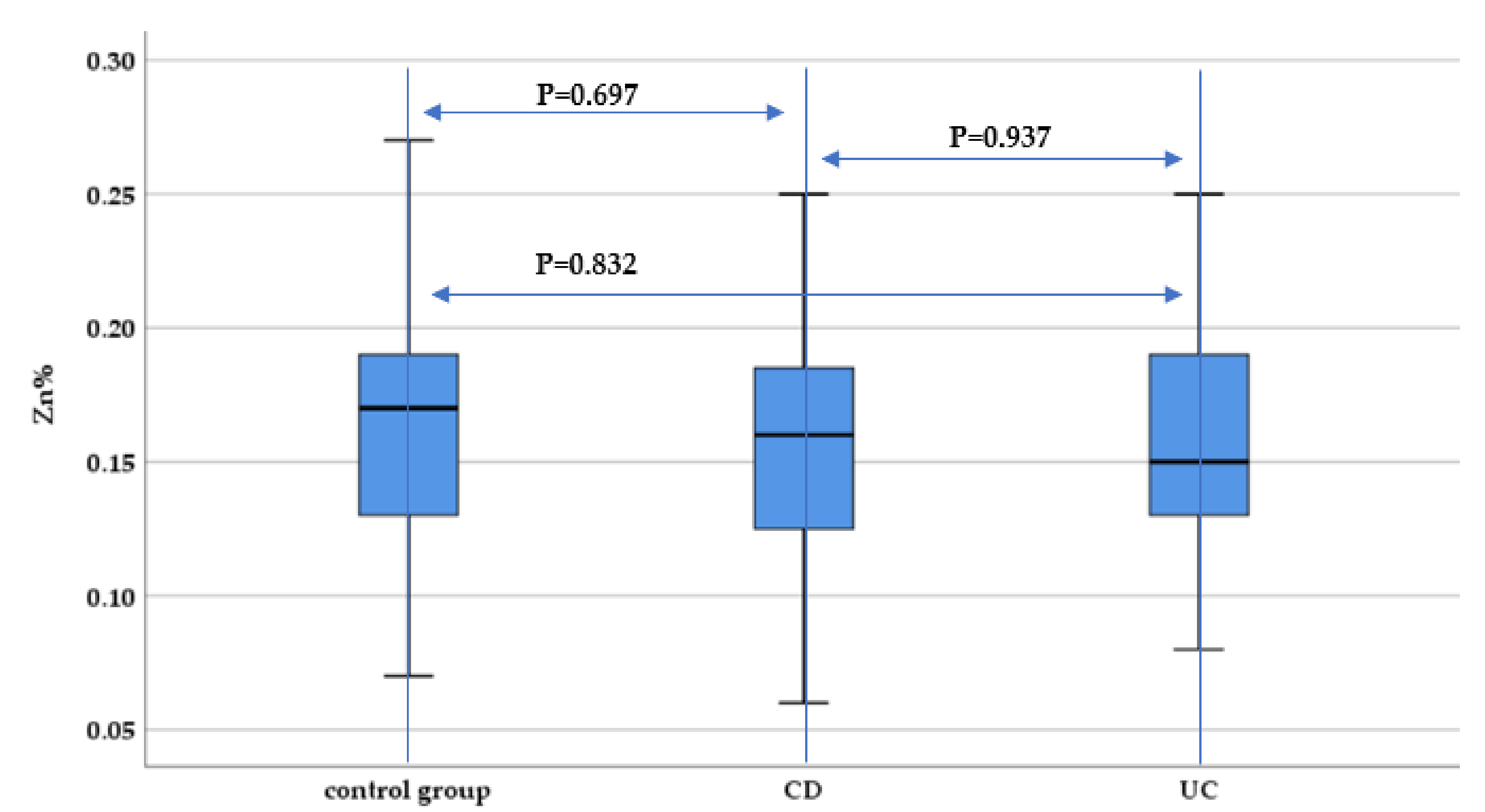
3.2. Hair Concentration of Micronutrients
3.3. Evaluating the Potential Correlations between Disease Activity and Mineral and Trace Elements Status
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Lees, C.W.; Barrett, J.C.; Parkes, M.; Satsangi, J. New IBD genetics: Common pathways with other diseases. Gut 2011, 60, 1739–1753. [Google Scholar] [CrossRef]
- Khalili, H.; Chan, S.; Lochhead, P.; Ananthakrishnan, A.N.; Hart, A.; Chan, A. The role of diet in the aetiopathogenesis of inflammatory bowel disease. Nat. Rev. Gastroenterol. Hepatol. 2018, 15, 525–535. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lane, E.; Zisman, T.; Suskind, D. The microbiota in inflammatory bowel disease: Current and therapeutic insights. J. Inflamm. Res. 2017, 10, 63–73. [Google Scholar] [CrossRef] [Green Version]
- Cho, J.M.; Yang, H.R. Hair mineral and trace element contents as reliable markers of nutritional status compared to serum levels of these elements in children newly diagnosed with inflammatory bowel disease. Biol. Trace Elem. Res. 2018, 185, 20–29. [Google Scholar] [CrossRef]
- O’Sullivan, M. Symposium on ‘The challenge of translating nutrition research into public health nutrition’. Session 3: Joint Nutrition Society and Irish Nutrition and Dietetic Institute symposium on ‘Nutrition and autoimmune disease’. Nutrition in Crohn’s disease. Proc. Nutr. Soc. 2009, 68, 127–134. [Google Scholar] [CrossRef] [Green Version]
- Nguyen, D.L.; Parekh, N.; Bechtold, M.L.; Jamal, M.M. National Trends and In-Hospital Outcomes of Adult Patients with Inflammatory Bowel Disease Receiving Parenteral Nutrition Support. J. Parenter. Enter. Nutr. 2016, 40, 412–416. [Google Scholar] [CrossRef] [PubMed]
- Song, S.M.; Kim, Y.; Oh, S.H.; Kim, K.M. Nutritional status and growth in Korean children with Crohn’s disease: A single-center study. Gut Liver 2014, 8, 500–507. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hess, W.M.; Seegmiller, R.E.; Gardner, J.S.; Allen, J.V.; Barendregt, S. Human hair morphology: A scanning electron microscopy study on a male Caucasoid and a computerized classification of regional differences. Scanning Microsc. 1990, 4, 375–386. [Google Scholar] [PubMed]
- Coroaba, A.; Chiriac, A.E.; Sacarescu, L.; Pinteala, T.; Minea, B.; Ibanescu, S.-A.; Pertea, M.; Moraru, A.; Esanu, I.; Maier, S.S.; et al. New insights into human hair: SAXS, SEM, TEM and EDX for Alopecia Areata investigations. PeerJ 2020, 8, e8376. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nguyen, G.C.; Munsell, M.; Harris, M.L. Nationwide prevalence and prognostic significance of clinically diagnosable protein-calorie malnutrition in hospitalized inflammatory bowel disease patients. Inflamm. Bowel Dis. 2008, 14, 1105–1111. [Google Scholar] [CrossRef]
- Ghoneima, A.S.; Flashman, K.; Dawe, V.; Baldwin, E.; Celentano, V. High risk of septic complications following surgery for Crohn’s disease in patients with preoperative anaemia, hypoalbuminemia and high CRP. Int. J. Colorectal Dis. 2019, 34, 2185–2188. [Google Scholar] [CrossRef] [Green Version]
- Weisshof, R.; Chermesh, I. Micronutrient deficiencies in inflammatory bowel disease. Curr. Opin. Clin. Nutr. Metab. Care 2015, 18, 576–581. [Google Scholar] [CrossRef] [PubMed]
- Yakut, M.; Ustun, Y.; Kabacam, G.; Soykan, I. Serum vitamin B12 and folate status in patients with inflammatory bowel diseases. Eur. J. Intern. Med. 2010, 21, 320–323. [Google Scholar] [CrossRef] [PubMed]
- Hwang, C.; Ross, V.; Mahadevan, U. Micronutrient deficiencies in inflammatory bowel disease: From A to zinc. Inflamm. Bowel Dis. 2012, 18, 1961–1981. [Google Scholar] [CrossRef] [PubMed]
- Duncan, A.; Talwar, D.; McMillan, D.C.; Stefanowicz, F.; O’Reilly, D.S.J. Quantitative data on the magnitude of the systemic inflammatory response and its effect on micronutrient status based on plasma measurements. Am. J. Clin. Nutr. 2012, 95, 64–71. [Google Scholar] [CrossRef] [Green Version]
- Galloway, P.; McMillan, D.C.; Sattar, N. Effect of the inflammatory response on trace element and vitamin status. Ann. Clin. Biochem. 2000, 37, 289–297. [Google Scholar] [CrossRef]
- Wołowiec, P.; Michalak, I.; Chojnacka, K.; Mikulewicz, M. Hair analysis in health assessment. Clin. Chim. Acta 2013, 419, 139–171. [Google Scholar] [CrossRef]
- Hotta, Y.; Fujino, R.; Kimura, O.; Endo, T. Essential and non-essential elements in scalp hair of diabetics: Correlations with glycated hemoglobin (HbA1c). Biol. Pharm. Bull. 2018, 41, 1034–1039. [Google Scholar] [CrossRef] [Green Version]
- Seneczko, M. Selenium balance in patients suffering from psoriasis vulgaris in different development phases Part 1. Concentration of selenium in selected morphotic components and excreta and activity of glutation peroxidase in red blood cells. Postep. Dermatol. Alergol. 2004, 21, 36–46. [Google Scholar]
- Ogasawara, H.; Hayasaka, M.; Maemoto, A.; Furukawa, S.; Ito, T.; Kimura, O.; Endo, T. Stable isotope ratios of carbon, nitrogen and selenium concentration in the scalp hair of Crohn’s disease patients who ingested the elemental diet Elental®. Rapid Commun Mass Spectrom. 2019, 33, 41–48. [Google Scholar] [CrossRef]
- Ha, B.J.; Lee, G.Y.; Cho, I.H.; Park, S. Age- and sex-dependence of five major elements in the development of human scalp hair. Biomater. Res. 2019, 23, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Dignass, A.U.; Gasche, C.; Bettenworth, D.; Birgegård, G.; Danese, S.; Gisbert, J.P.; Gomollon, F.; Iqbal, T.; Katsanos, K.; Koutroubakis, I.; et al. European consensus on the diagnosis and management of iron deficiency and anaemia in inflammatory bowel diseases. J. Crohn’s Colitis 2015, 9, 211–222. [Google Scholar] [CrossRef] [PubMed]
- Niepel, D.; Klag, T.; Malek, N.P.; Wehkamp, J. Practical guidance for the management of iron deficiency in patients with inflammatory bowel disease. Ther. Adv. Gastroenterol. 2018, 11, 1756284818769074. [Google Scholar] [CrossRef] [Green Version]
- De Baaij, J.H.; Hoenderop, J.G.; Bindels, R.J. Magnesium in man: Implications for health and disease. Physiol. Rev. 2015, 95, 1–46. [Google Scholar] [CrossRef] [PubMed]
- Stritt, S.; Nurden, P.; Favier, R.; Favier, M.; Ferioli, S.; Gotru, S.K.; Van Eeuwijk, J.M.M.; Schulze, H.; Nurden, A.T.; Lambert, M.P.; et al. Defects in TRPM7 channel function deregulate thrombopoiesis through altered cellular Mg2+ homeostasis and cytoskeletal architecture. Nat. Commun. 2016, 7, 1–13. [Google Scholar] [CrossRef]
- Workinger, J.L.; Doyle, R.P.; Bortz, J. Challenges in the diagnosis of magnesium status. Nutrients 2018, 10, 1202. [Google Scholar] [CrossRef]
- Kruis, W.; Nguyen, G.P. Iron Deficiency, Zinc, Magnesium, Vitamin Deficiencies in Crohn’s Disease: Substitute or Not? Dig. Dis. 2016, 34, 105–111. [Google Scholar] [CrossRef]
- Christakos, S.; Dhawan, P.; Porta, A.; Mady, L.J.; Seth, T. Vitamin D and intestinal calcium absorption. Mol. Cell. Endocrinol. 2011, 347, 25–29. [Google Scholar] [CrossRef] [Green Version]
- Ghishan, F.; Kiela, P. Advances in the understanding of mineral and bone metabolism in inflammatory bowel diseases. Am. J. Physiol. Gastrointest. Liver Physiol. 2020, 300, G191–G201. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huybers, S.; Apostolaki, M.; Van der Eerden, B.C.; Kollias, G.; Naber, T.H.; Bindels, R.J.; Hoenderop, J.G. Murine TNF ARE Crohn’s Disease Model Displays Diminished Expression of Intestinal Ca2+ Transporters. Inflamm. Bowel Dis. 2008, 14, 803–811. [Google Scholar] [CrossRef]
- Zeng, H. Selenium as an essential micronutrient: Roles in cell cycle and apoptosis. Molecules 2009, 14, 1263–1278. [Google Scholar] [CrossRef] [Green Version]
- Bera, S.; De Rosa, V.; Rachidi, W.; Diamond, A.M. Does a role for selenium in DNA damage repair explain apparent controversies in its use in chemoprevention? Mutagenesis 2013, 28, 127–134. [Google Scholar] [CrossRef] [Green Version]
- Avery, J.C.; Hoffmann, P.R. Selenium, selenoproteins, and immunity. Nutrients 2018, 10, 1203. [Google Scholar] [CrossRef] [Green Version]
- Geerling, B.J.; Badart-Smook, A.; Stockbrugger, R.W.; Brummer, R.J. Comprehensive nutritional status in recently diagnosed patients with inflammatory bowel disease compared with population controls. Eur. J. Clin. Nutr. 2000, 54, 514–521. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lomer, M.C.; Cahill, O.; Baschali, A.; Sarathy, P.P.; Sarantidou, M.; Mantzaris, G.J.; Gaya, D.R.; Katsanos, K.; Christodoulou, D.K.; Gerasimidis, K. A multicentre study of nutrition risk assessment in adult patients with inflammatory bowel disease attending outpatient clinics. Ann. Nutr. Metab. 2019, 74, 18–23. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ohashi, W.; Hara, T.; Takagishi, T.; Hase, K.; Fukada, T. Maintenance of intestinal epithelial homeostasis by zinc transporters. Dig. Dis. Sci. 2019, 64, 2404–2415. [Google Scholar] [CrossRef]
- Vagianos, K.; Bector, S.; McConnell, J.; Bernstein, C.N. Nutrition assessment of patients with inflammatory bowel disease. J. Parenter. Enter. Nutr. 2007, 31, 311–319. [Google Scholar] [CrossRef]
- Alkhouri, R.H.; Hashmi, H.; Baker, R.D.; Gelfond, D.; Baker, S.S. Vitamin and mineral status in patients with inflammatory bowel disease. J. Pediatr. Gastroenterol. Nutr. 2013, 56, 89–92. [Google Scholar] [CrossRef] [PubMed]
- Jin, W.; Zheng, H.; Shan, B.; Wu, Y. Changes of serum trace elements level in patients with alopecia areata: A meta-analysis. J. Dermatol. 2017, 44, 588–591. [Google Scholar] [CrossRef] [PubMed]
- Siva, S.; Rubin, D.T.; Gulotta, G.; Wroblewski, K.; Pekow, J. Zinc deficiency is associated with poor clinical outcomes in patients with inflammatory bowel disease. Inflamm. Bowel Dis. 2017, 23, 152–157. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- MacMaster, M.J.; Damianopoulou, S.; Thomson, C.; Talwar, D.; Stefanowicz, F.; Catchpole, A.; Gerasimidis, K.; Gaya, D.R. A prospective analysis of micronutrient status in quiescent inflammatory bowel disease. Clin. Nutr. 2021, 40, 327–331. [Google Scholar] [CrossRef]
- Kempson, I.; Skinner, W.; Kirkbride, P. The occurrence and incorporation of copper and zinc in hair and their potential role as bioindicators: A review. J. Toxicol. Environ. Health 2007, 10, 611–622. [Google Scholar] [CrossRef]
- Horning, K.J.; Caito, S.W.; Tipps, K.G.; Bowman, A.B.; Aschner, M. Manganese is essential for neuronal health. Annu. Rev. Nutr. 2015, 35, 71–108. [Google Scholar] [CrossRef]
- Choi, E.K.; Aring, L.; Das, N.K.; Solanki, S.; Inohara, N.; Iwase, S.; Samuelson, L.C.; Shah, Y.M.; Seo, Y.A. Impact of dietary manganese on experimental colitis in mice. FASEB J. 2020, 34, 2929–2943. [Google Scholar] [CrossRef] [Green Version]
- Trumbo, P.; Yates, A.A.; Schlicker, S.; Poos, M. Dietary reference intakes: Vitamin A, vitamin K, arsenic, boron, chromium, copper, iodine, iron, manganese, molybdenum, nickel, silicon, vanadium, and zinc. J. Am. Diet. Assoc. 2001, 101, 294–301. [Google Scholar] [CrossRef]
- Malepfane, N.M.; Muchaonyerwa, P. Hair from different ethnic groups vary in elemental composition and nitrogen and phosphorus mineralisation in soil. Environ. Monit. Assess. 2017, 189, 76. [Google Scholar] [CrossRef]
- Ogawa, Y.; Kinoshita, M.; Shimada, S.; Kawamura, T. Zinc and skin disorders. Nutrients 2018, 10, 199. [Google Scholar] [CrossRef] [Green Version]
- Seguí, J.; Gironella, M.; Sans, M.; Granell, S.; Gil, F.; Gimeno, M.; Coronel, P.; Piqué, J.M.; Panés, J. Superoxide dismutase ameliorates TNBS-induced colitis by reducing oxidative stress, adhesion molecule expression, and leukocyte recruitment into the inflamed intestine. J. Leukoc. Biol. 2004, 76, 537–544. [Google Scholar] [CrossRef] [PubMed]
- Mohammadi, E.; Qujeq, D.; Taheri, H.; Hajian-Tilaki, K. Evaluation of serum trace element levels and superoxide dismutase activity in patients with inflammatory bowel disease: Translating basic research into clinical application. Biol. Trace Elem. Res. 2017, 177, 235–240. [Google Scholar] [CrossRef]
- Ojuawo, A.; Keith, L. The serum concentrations of zinc, copper and selenium in children with inflammatory bowel disease. Cent. Afr. J. Med. 2002, 48, 116–119. [Google Scholar]
- Malavolta, M.; Piacenza, F.; Basso, A.; Giacconi, R.; Costarelli, L.; Mocchegiani, E. Serum copper to zinc ratio: Relationship with aging and health status. Mech. Ageing Dev. 2015, 151, 93–100. [Google Scholar] [CrossRef]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient Characteristics | Study Group n = 37 | Control Group n = 31 | p-Value | |
|---|---|---|---|---|
| UC (n = 25) | CD (n = 12) | |||
| Age, median (Q25; Q75) | 43.5 (30; 59.5) | 32 (29; 42) | 0.05 § | |
| 46 (32.5; 65.5) | 33 (27.5; 44.5) | |||
| Sex (M/F), n (%) | 19/18 (51.4/48.6) | 16/15 (51.6/48.4) | 0.981 Ϯ | |
| 13/12 (52/48) | 6/6 (50/50) | |||
| Urban vs. rural area (U/R), n (%) | 29/8 (78.4/21.6) | 28/3 (90.3/9.7) | 0.286 Ϯ | |
| 20/5 (80/20) | 9/3 (75/25) | |||
| BMI (average ± SD) | 21.97 ± 1.5 | 23.08 ± 2.2 | 0.259 # | |
| 22.61 ± 1.95 | 21.97 ± 1.5 | |||
| Disease activity score | Mayo score 3 (1; 7) | CDAI score 146.5 (52.5; 276.5) | ||
| Active disease, n (%) | 22 (59.5%) | NA | NA | |
| 16 (64% *) | 6 (50% *) | NA | 0.65 Ϯ | |
| Disease location * | Proctitis 6 (24%) Left-sided colitis 13 (52%) Pancolitis 6 (24%) | Ileum (L1) 2 (16.6%) Colonic (L2) 7 (58.3%) Ileocolic (L3) 3 (25%) | NA | |
| Treatment followed * | aminosalicylates 18 (72%) azathioprine 1 (4%) biological therapy 4 (16%) first diagnosis-no prior treatment 2 (8%) | azathioprine 6 (50%) biological therapy 4 (33.3%) first diagnosis-no prior treatment 2 (16.7%) | NA | |
| Evaluated Element | CD Disease Activity | UC Disease Activity | ||
|---|---|---|---|---|
| Correlation Coefficient | p-Value | Correlation Coefficient | p-Value | |
| Mg% ╥ | −0.147 | 0.649 | 0.186 | 0.375 |
| S% ^ | 0.585 | 0.046 * | 0.112 | 0.594 |
| Ca% ╥ | −0.772 | 0.003 * | −0.058 | 0.782 |
| Mn% ╥ | −0.269 | 0.398 | 0.133 | 0.525 |
| Fet% ╥ | 0.315 | 0.319 | 0.006 | 0.978 |
| Cu% ╥ | −0.024 | 0.940 | 0.052 | 0.804 |
| Zn% ^ | 0.696 | 0.126 | 0.009 | 0.966 |
| Se% ╥ | 0.269 | 0.398 | −0.006 | 0.978 |
| Evaluated Element | CRP | CRP/ALB | NLR | Fibrinogen | ||||
|---|---|---|---|---|---|---|---|---|
| Correlation Coefficient | p-Value | Correlation Coefficient | p-Value | Correlation Coefficient | p-Value | Correlation Coefficient | p-Value | |
| Mg% ╥ | −0.284 | 0.088 | −0.257 | 0.125 | −0.261 | 0.119 | −0.288 | 0.094 |
| S% ^ | 0.135 | 0.425 | 0.145 | 0.391 | 0.171 | 0.311 | 0.206 | 0.236 |
| Ca% ╥ | −0.297 | 0.074 | −0.301 | 0.07 | −0.266 | 0.112 | −0.119 | 0.497 |
| Mn% ╥ | 0.185 | 0.274 | 0.161 | 0.342 | 0.112 | 0.511 | −0.255 | 0.139 |
| Fe% ╥ | −0.133 | 0.432 | −0.122 | 0.474 | −0.003 | 0.987 | −0.154 | 0.379 |
| Cu% ╥ | −0.110 | 0.516 | −0.130 | 0.442 | 0.016 | 0.987 | −0.279 | 0.105 |
| Zn% ^ | −0.061 | 0.722 | −0.06 | 0.725 | 0.063 | 0.713 | −0.094 | 0.589 |
| Se% ╥ | 0.144 | 0.396 | −0.043 | 0.799 | 0.059 | 0.728 | 0.189 | 0.277 |
| Evaluated Element | UC Patients | CD Patients | Control Group | |||
|---|---|---|---|---|---|---|
| Correlation Coefficient | p-Value | Correlation Coefficient | p-Value | Correlation Coefficient | p-Value | |
| Mg% ╥ | −0.002 | 0.993 | −0.099 | 0.759 | 0.143 | 0.442 |
| S% ^ | −0.01 | 0.962 | 0.333 | 0.290 | −0.2 | 0.917 |
| Ca% ╥ | 0.088 | 0.675 | −0.147 | 0.649 | −0.083 | 0.657 |
| Mn% ╥ | 0.113 | 0.592 | 0.563 | 0.057 | −0.006 | 0.976 |
| Fe% ╥ | 0.023 | 0.911 | −0.011 | 0.974 | −0.268 | 0.144 |
| Cu% ╥ | 0.091 | 0.665 | 0.204 | 0.526 | 0.225 | 0.220 |
| Zn% ^ | −0.087 | 0.678 | 0.409 | 0.187 | −0.198 | 0.285 |
| Se% ╥ | −0.272 | 0.189 | 0.309 | 0.329 | 0.077 | 0.680 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gîlcă-Blanariu, G.-E.; Coroabă, A.; Ciocoiu, M.; Trifan, A.; Dimofte, G.; Diaconescu, S.; Afrăsânie, V.-A.; Balan, G.G.; Pinteală, T.; Ștefănescu, G. Hair EDX Analysis—A Promising Tool for Micronutrient Status Evaluation of Patients with IBD? Nutrients 2021, 13, 2572. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13082572
Gîlcă-Blanariu G-E, Coroabă A, Ciocoiu M, Trifan A, Dimofte G, Diaconescu S, Afrăsânie V-A, Balan GG, Pinteală T, Ștefănescu G. Hair EDX Analysis—A Promising Tool for Micronutrient Status Evaluation of Patients with IBD? Nutrients. 2021; 13(8):2572. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13082572
Chicago/Turabian StyleGîlcă-Blanariu, Georgiana-Emmanuela, Adina Coroabă, Manuela Ciocoiu, Anca Trifan, Gabriel Dimofte, Smaranda Diaconescu, Vlad-Adrian Afrăsânie, Gheorghe G. Balan, Tudor Pinteală, and Gabriela Ștefănescu. 2021. "Hair EDX Analysis—A Promising Tool for Micronutrient Status Evaluation of Patients with IBD?" Nutrients 13, no. 8: 2572. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13082572