
Associations between Infant Dietary Intakes and Liking for Sweetness and Fattiness Sensations in 8-to-12-Year-Old Children

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
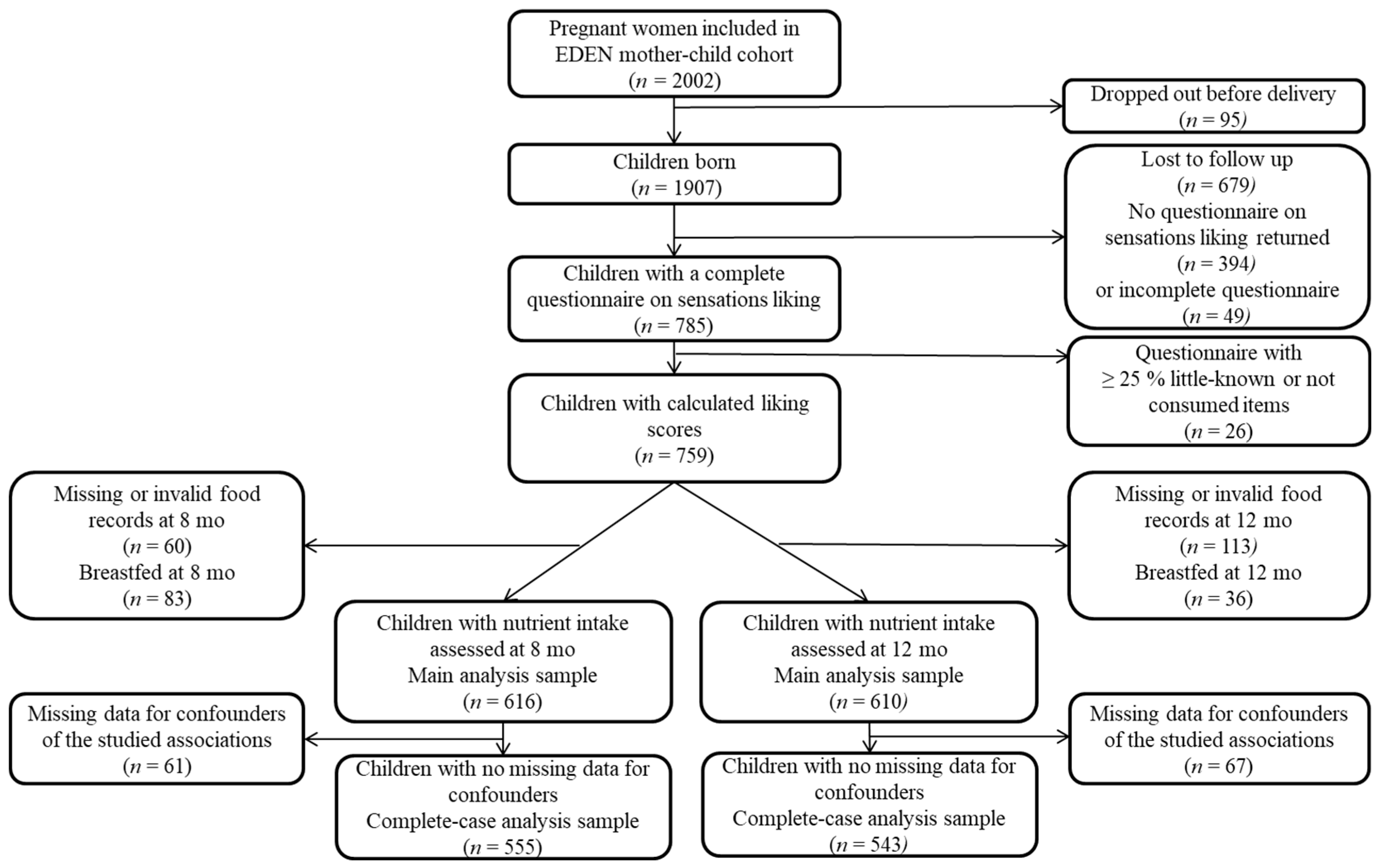
2.1. Study Population
2.2. Infant’s Dietary Intake
2.3. Children’s Liking for Sweetness and Fattiness Sensations
2.4. Familial and Children Characteristics
2.5. Infant’s Feeding Practices
2.6. Sample Selection
2.7. Statistical Analysis
3. Results
3.1. Liking for Sweetness
3.2. Liking for Fattiness Sensation
3.3. Liking for Fattiness-and-Sweetness
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Gluckman, P.D.; Hanson, M.A.; Buklijas, T. A conceptual framework for the developmental origins of health and disease. J. Dev. Orig. Health Dis. 2010, 1, 6–18. [Google Scholar] [CrossRef] [Green Version]
- Mennella, J.A.; Beauchamp, G.K. Flavor experiences during formula feeding are related to preferences during childhood. Early Hum. Dev. 2002, 68, 71–82. [Google Scholar] [CrossRef] [Green Version]
- Nicklaus, S.; Boggio, V.; Chabanet, C.; Issanchou, S. A prospective study of food preferences in childhood. Food Qual. Prefer. 2004, 15, 805–818. [Google Scholar] [CrossRef]
- Skinner, J.D.; Carruth, B.R.; Wendy, B.; Ziegler, P.J. Children’s food preferences: A longitudinal analysis. J. Am. Diet. Assoc. 2002, 102, 1638–1647. [Google Scholar] [CrossRef]
- Lioret, S.; Betoko, A.; Forhan, A.; Charles, M.A.; Heude, B.; de Lauzon-Guillain, B.; Eden Mother-Child Cohort Study Group. Dietary patterns track from infancy to preschool age: Cross-sectional and longitudinal perspectives. J. Nutr. 2015, 145, 775–782. [Google Scholar] [PubMed]
- Northstone, K.; Emmett, P.M. Are dietary patterns stable throughout early and mid-childhood? A birth cohort study. Br. J. Nutr. 2008, 100, 1069–1076. [Google Scholar] [CrossRef] [Green Version]
- Lioret, S.; McNaughton, S.A.; Spence, A.C.; Crawford, D.; Campbell, K.J. Tracking of dietary intakes in early childhood: The Melbourne InFANT Program. Eur. J. Clin. Nutr. 2013, 67, 275–281. [Google Scholar] [CrossRef]
- Nicklaus, S. The Role of Dietary Experience in the Development of Eating Behavior during the First Years of Life. Ann. Nutr. Metab. 2017, 70, 241–245. [Google Scholar] [CrossRef] [Green Version]
- Kiefte-de Jong, J.C.; de Vries, J.H.; Bleeker, S.E.; Jaddoe, V.W.V.; Hofman, A.; Raat, H.; Moll, H.A. Socio-demographic and lifestyle determinants of ‘Western-like’ and ‘Health conscious’ dietary patterns in toddlers. Br. J. Nutr. 2013, 109, 137–147. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Robinson, S.; Marriott, L.; Poole, J.; Crozier, S.; Borland, S.; Lawrence, W.; Law, C.; Godfrey, K.; Cooper, C.; Inskip, H.; et al. Dietary patterns in infancy: The importance of maternal and family influences on feeding practice. Br. J. Nutr. 2007, 98, 1029–1037. [Google Scholar] [CrossRef] [Green Version]
- Smithers, L.G.; Brazionis, L.; Golley, R.K.; Mittinty, M.N.; Northstone, K.; Emmett, P.; McNaughton, S.A.; Campbell, K.J.; Lynch, J.W. Associations between dietary patterns at 6 and 15 months of age and sociodemographic factors. Eur. J. Clin. Nutr. 2012, 66, 658–666. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bell, L.K.; Golley, R.K.; Daniels, L.; Magarey, A.M. Dietary patterns of Australian children aged 14 and 24 months, and associations with socio-demographic factors and adiposity. Eur. J. Clin. Nutr. 2013, 67, 638–645. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Drewnowski, A.; Mennella, J.A.; Johnson, S.L.; Bellisle, F. Sweetness and food preference. J. Nutr. 2012, 142, 1142S–1148S. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Okronipa, H.; Arimond, M.; Arnold, C.D.; Young, R.R.; Adu-Afarwuah, S.; Tamakloe, S.M.; Ocansey, M.E.; Kumordzie, S.M.; Oaks, B.M.; Mennella, J.A.; et al. Exposure to a slightly sweet lipid-based nutrient supplement during early life does not increase the level of sweet taste most preferred among 4- to 6-year-old Ghanaian children: Follow-up of a randomized controlled trial. Am. J. Clin. Nutr. 2019, 109, 1224–1232. [Google Scholar] [CrossRef] [PubMed]
- Okronipa, H.; Arimond, M.; Young, R.R.; Arnold, C.D.; Adu-Afarwuah, S.; Tamakloe, S.M.; Bentil, H.J.; Ocansey, M.E.; Kumordzie, S.M.; Oaks, B.M.; et al. Exposure to a Slightly Sweet Lipid-Based Nutrient Supplement During Early Life Does Not Increase the Preference for or Consumption of Sweet Foods and Beverages by 4-6-y-Old Ghanaian Preschool Children: Follow-up of a Randomized Controlled Trial. J. Nutr. 2019, 149, 532–541. [Google Scholar] [CrossRef]
- Pepino, M.Y.; Mennella, J.A. Factors contributing to individual differences in sucrose preference. Chem. Senses 2005, 30, I319–I320. [Google Scholar] [CrossRef]
- Desor, J.A.; Greene, L.S.; Maller, O. Preferences for sweet and salty in 9- to 15-year-old and adult humans. Science 1975, 190, 686–687. [Google Scholar] [CrossRef]
- Lanfer, A.; Knof, K.; Barba, G.; Veidebaum, T.; Papoutsou, S.; de Henauw, S.; Soos, T.; Moreno, L.A.; Ahrens, W.; Lissner, L. Taste preferences in association with dietary habits and weight status in European children: Results from the IDEFICS study. Int. J. Obes. 2012, 36, 27–34. [Google Scholar] [CrossRef] [Green Version]
- Liem, D.G.; de Graaf, C. Sweet and sour preferences in young children and adults: Role of repeated exposure. Physiol. Behav. 2004, 83, 421–429. [Google Scholar] [CrossRef]
- Divert, C.; Chabanet, C.; Schoumacker, R.; Martin, C.; Lange, C.; Issanchou, S.; Nicklaus, S. Relation between sweet food consumption and liking for sweet taste in French children. Food Qual. Prefer. 2017, 56, 18–27. [Google Scholar] [CrossRef]
- Lampure, A.; Deglaire, A.; Schlich, P.; Castetbon, K.; Peneau, S.; Hercberg, S.; Mejean, C. Liking for fat is associated with sociodemographic, psychological, lifestyle and health characteristics. Br. J. Nutr. 2014, 112, 1353–1363. [Google Scholar] [CrossRef] [Green Version]
- Lampure, A.; Castetbon, K.; Deglaire, A.; Schlich, P.; Peneau, S.; Hercberg, S.; Mejean, C. Associations between liking for fat, sweet or salt and obesity risk in French adults: A prospective cohort study. Int. J. Behav. Nutr. Phys. Act. 2016, 13, 74. [Google Scholar] [CrossRef] [PubMed]
- Papantoni, A.; Shearrer, G.E.; Sadler, J.R.; Stice, E.; Burger, K.S. Longitudinal Associations Between Taste Sensitivity, Taste Liking, Dietary Intake and BMI in Adolescents. Front. Psychol. 2021, 12, 597704. [Google Scholar] [CrossRef] [PubMed]
- Lange, C.; Yuan, W.L.; Schoumacker, R.; Deglaire, A.; de Lauzon-Guillain, B.; Chabanet, C.; Nicklaus, S. Assessment of liking for saltiness, sweetness and fattiness sensations in children: Validation of a questionnaire. Food Qual. Prefer. 2018, 65, 81–91. [Google Scholar] [CrossRef]
- Ricketts, C.D. Fat preferences, dietary fat intake and body composition in children. Eur. J. Clin. Nutr. 1997, 51, 778–781. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Looy, H.; Callaghan, S.; Weingarten, H.P. Hedonic response of sucrose likers and dislikers to other gustatory stimuli. Physiol. Behav. 1992, 52, 219–225. [Google Scholar] [CrossRef]
- Steiner, J.E. Human facial expressions in response to taste and smell stimulation. Adv. Child. Dev. Behav. 1979, 13, 257–295. [Google Scholar] [PubMed]
- Birch, L.L. Children’s preferences for high-fat foods. Nutr. Rev. 1992, 50, 249–255. [Google Scholar] [CrossRef]
- Johnson, S.L.; McPhee, L.; Birch, L.L. Conditioned preferences: Young children prefer flavors associated with high dietary fat. Physiol. Behav. 1991, 50, 1245–1251. [Google Scholar] [CrossRef]
- Kern, D.L.; McPhee, L.; Fisher, J.; Johnson, S.; Birch, L.L. The postingestive consequences of fat condition preferences for flavors associated with high dietary fat. Physiol. Behav. 1993, 54, 71–76. [Google Scholar] [CrossRef]
- Nicklaus, S. The role of food experiences during early childhood in food pleasure learning. Appetite 2016, 104, 3–9. [Google Scholar] [CrossRef] [PubMed]
- Schwartz, C.; Madrelle, J.; Brignot, H.; Delarue, J.; Cuvelier, G.; Nicklaus, S.; Feron, G.; Tournier, C. Acceptance of added fat to first complementary feeding purees: An exploration of fat type, feeding history and saliva composition. Appetite 2018, 131, 160–168. [Google Scholar] [CrossRef] [PubMed]
- Birch, L.L.; McPhee, L.; Steinberg, L.; Sullivan, S. Conditioned flavor preferences in young children. Physiol. Behav. 1990, 47, 501–505. [Google Scholar] [CrossRef]
- Appleton, K.M.; Tuorila, H.; Bertenshaw, E.J.; de Graaf, C.; Mela, D.J. Sweet taste exposure and the subsequent acceptance and preference for sweet taste in the diet: Systematic review of the published literature. Am. J. Clin. Nutr. 2018, 107, 405–419. [Google Scholar] [CrossRef] [PubMed]
- Beauchamp, G.K.; Moran, M. Dietary experience and sweet taste preference in human infants. Appetite 1982, 3, 139–152. [Google Scholar] [CrossRef]
- Beauchamp, G.K.; Moran, M. Acceptance of sweet and salty tastes in 2-year-old children. Appetite 1984, 5, 291–305. [Google Scholar] [CrossRef]
- Huffman, S.L.; Piwoz, E.G.; Vosti, S.A.; Dewey, K.G. Babies, soft drinks and snacks: A concern in low- and middle-income countries? Matern. Child Nutr. 2014, 10, 562–574. [Google Scholar] [CrossRef]
- Blundell, J.E.; MacDiarmid, J.I. Fat as a risk factor for overconsumption: Satiation, satiety, and patterns of eating. J. Am. Diet. Assoc. 1997, 97, S63–S69. [Google Scholar] [CrossRef]
- Bere, E.; Brug, J.; Klepp, K.I. Why do boys eat less fruit and vegetables than girls? Public Health Nutr. 2008, 11, 321–325. [Google Scholar] [CrossRef] [Green Version]
- Yuan, W.L.; Lange, C.; Schwartz, C.; Martin, C.; Chabanet, C.; de Lauzon-Guillain, B.; Nicklaus, S. Infant Dietary Exposures to Sweetness and Fattiness Increase during the First Year of Life and Are Associated with Feeding Practices. J. Nutr. 2016, 146, 2334–2342. [Google Scholar] [CrossRef] [Green Version]
- Cooke, L.J.; Wardle, J. Age and gender differences in children’s food preferences. Br. J. Nutr. 2005, 93, 741–746. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lehto, E.; Ray, C.; Haukkala, A.; Yngve, A.; Thorsdottir, I.; Roos, E. Predicting gender differences in liking for vegetables and preference for a variety of vegetables among 11-year-old children. Appetite 2015, 95, 285–292. [Google Scholar] [CrossRef]
- Caine-Bish, N.L.; Scheule, B. Gender differences in food preferences of school-aged children and adolescents. J. Sch. Health 2009, 79, 532–540. [Google Scholar] [CrossRef]
- Betoko, A.; Charles, M.A.; Hankard, R.; Forhan, A.; Bonet, M.; Saurel-Cubizolles, M.J.; Heude, B.; de Lauzon-Guillain, B.; Eden Mother-Child Cohort Study Group. Infant feeding patterns over the first year of life: Influence of family characteristics. Eur. J. Clin. Nutr. 2013, 67, 631–637. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Camier, A.; Chabanet, C.; Davisse-Paturet, C.; Ksiazek, E.; Lioret, S.; Charles, M.A.; Nicklaus, S.; de Lauzon-Guillain, B. Characterization of Infant Feeding Practices and Related-Family Characteristics in the French Nationwide ELFE Birth Cohort. Nutrients 2020, 13, 33. [Google Scholar] [CrossRef] [PubMed]
- Bournez, M.; Ksiazek, E.; Wagner, S.; Kersuzan, C.; Tichit, C.; Gojard, S.; Thierry, X.; Charles, M.A.; Lioret, S.; de Lauzon-Guillain, B.; et al. Factors associated with the introduction of complementary feeding in the French ELFE cohort study. Matern. Child Nutr. 2018, 14, e12536. [Google Scholar] [CrossRef]
- Luo, S.; Alves, J.; Hardy, K.; Wang, X.; Monterosso, J.; Xiang, A.H.; Page, K.A. Neural processing of food cues in pre-pubertal children. Pediatr. Obes. 2019, 14, e12435. [Google Scholar] [CrossRef]
- Ervina, E.; Berget, I. VLA Investigating the Relationships between Basic Tastes Sensitivities, Fattiness Sensitivity, and Food Liking in 11-Year-Old Children. Foods 2020, 9, 1315. [Google Scholar] [CrossRef]
- Joseph, P.V.; Reed, D.R.; Mennella, J.A. Individual Differences Among Children in Sucrose Detection Thresholds: Relationship With Age, Gender, and Bitter Taste Genotype. Nurs. Res. 2016, 65, 3–12. [Google Scholar] [CrossRef]
- Heude, B.; Forhan, A.; Slama, R.; Douhaud, L.; Bedel, S.; Saurel-Cubizolles, M.J.; Hankard, R.; Thiebaugeorges, O.; De Agostini, M.; Annesi-Maesano, I.; et al. Cohort Profile: The EDEN mother-child cohort on the prenatal and early postnatal determinants of child health and development. Int. J. Epidemiol. 2016, 45, 353–363. [Google Scholar] [CrossRef] [Green Version]
- Deglaire, A.; Méjean, C.; Castetbon, K.; Kesse-Guyot, E.; Urbano, C.; Hercberg, S.; Schlich, P. Development of a questionnaire to assay recalled liking for salt, sweet and fat. Food Qual. Prefer. 2012, 23, 110–124. [Google Scholar] [CrossRef]
- Cole, T.J.; Bellizzi, M.C.; Flegal, K.M.; Dietz, W.H. Establishing a standard definition for child overweight and obesity worldwide: International survey. BMJ 2000, 320, 1240–1243. [Google Scholar] [CrossRef] [Green Version]
- Deschamps, V.; de Lauzon-Guillain, B.; Lafay, L.; Borys, J.M.; Charles, M.A.; Romon, M. Reproducibility and relative validity of a food-frequency questionnaire among French adults and adolescents. Eur. J. Clin. Nutr. 2009, 63, 282–291. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yuan, W.L.; Nicklaus, S.; Lioret, S.; Lange, C.; Forhan, A.; Heude, B.; Charles, M.A.; de Lauzon-Guillain, B. Early factors related to carbohydrate and fat intake at 8 and 12 months: Results from the EDEN mother-child cohort. Eur. J. Clin. Nutr. 2016, 71, 219–226. [Google Scholar] [CrossRef] [PubMed]
- Cole, T.J.; Lobstein, T. Extended international (IOTF) body mass index cut-offs for thinness, overweight and obesity. Pediatr. Obes. 2012, 7, 284–294. [Google Scholar] [CrossRef]
- Keller, K.L.; Kling, S.M.R.; Fuchs, B.; Pearce, A.L.; Reigh, N.A.; Masterson, T.; Hickok, K. A Biopsychosocial Model of Sex Differences in Children’s Eating Behaviors. Nutrients 2019, 11, 682. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- What We Eat in America, NHANES 2017–2018, Individuals 2 Years and over (Excluding Breast-Fed Children), Day 1. Available online: www.ars.usda.gov/nea/bhnrc/fsrg (accessed on 20 November 2020).


{kind=link}
| 8 Months (n = 616) | 12 Months (n = 610) | |||
|---|---|---|---|---|
| n | Mean ± SD or % (n) | n | Mean ± SD or % (n) | |
| Study center | ||||
| Poitiers | 616 | 48 (298) | 610 | 47 (284) |
| Children characteristics | ||||
| Age (y) | 616 | 10.7 ± 0.8 | 610 | 10.7 ± 0.8 |
| Boys | 616 | 51 (313) | 610 | 51 (313) |
| Gestational age (wk) | 616 | 39.3 (1.6) | 610 | 39.3 (1.6) |
| Birthweight (kg) | 616 | 3.3 ± 0.5 | 610 | 3.3 ± 0.5 |
| Overweight at the 9–12-y follow-up (IOTF) 2 | 601 | 10 (63) | 596 | 10 (58) |
| Maternal characteristics | ||||
| Age at delivery (y) | 616 | 30 ± 4.5 | 610 | 30.3 ± 4.5 |
| Primiparous | 615 | 48 (298) | 609 | 47 (289) |
| Pre-pregnancy BMI | 607 | 600 | ||
| <18.5 kg/m2 | 8 (48) | 8 (45) | ||
| 18.5–24.9 kg/m2 | 68 (411) | 69 (415) | ||
| 25.0–29.9 kg/m2 | 18 (109) | 17 (104) | ||
| ≥30.0 kg/m2 | 6 (39) | 6 (36) | ||
| Educational attainment | 613 | 607 | ||
| < high school diploma | 16 (99) | 14 (88) | ||
| high school diploma | 17 (104) | 16 (98) | ||
| 2-y university degree | 25 (153) | 25 (153) | ||
| >2-y university degree | 42 (257) | 44 (268) | ||
| Monthly household income | 612 | 606 | ||
| <€1501 | 8 (46) | 6 (39) | ||
| €1501–2300 | 27 (166) | 26 (160) | ||
| €2301–3000 | 31 (190) | 31 (186) | ||
| >€3000 | 34 (210) | 36 (221) | ||
| Infant feeding practices | ||||
| Any breastfeeding duration | 616 | 610 | ||
| Never | 26 (158) | 23 (143) | ||
| <3.0 months | 28 (173) | 26 (159) | ||
| 3.0–5.9 months | 29 (179) | 27 (167) | ||
| ≥6.0 months | 17 (106) | 23 (141) | ||
| Age at complementary feeding introduction | 616 | 610 | ||
| <4.0 months | 27 (167) | 25 (152) | ||
| 4.0–6.0 months | 71 (438) | 72 (442) | ||
| >6.0 months | 2 (11) | 3 (16) | ||
| 8 Months (n = 616) | 12 Months (n = 610) | |||||||
|---|---|---|---|---|---|---|---|---|
| Total | Boys | Girls | p-Value 2 | Total | Boys | Girls | p-Value 2 | |
| Dietary intake in infancy | ||||||||
| Energy intake (kcal) | 710 ± 131 | 735 ± 138 | 684 ± 118 | <0.0001 | 798 ± 137 | 826 ± 136 | 769 ± 134 | <0.0001 |
| Carbohydrate intake (g/day) | 98 ± 20 | 102 ± 20 | 94 ± 18 | <0.0001 | 108 ± 22 | 112 ± 22 | 104 ± 22 | <0.0001 |
| Sugar intake (g/day) | 58 ± 18 | 59 ± 18 | 58 ± 17 | 0.21 | 69 ± 16 | 71 ± 16 | 67 ± 16 | 0.0007 |
| Consumer of added sugars | 27 (165) | 29 (91) | 24 (74) | 0.19 | 36 (219) | 37 (116) | 35 (103) | 0.54 |
| Fat intake (g/day) | 28 ± 7 | 28 ± 7 | 27 ± 7 | 0.06 | 30 ± 8 | 31 ± 8 | 29 ± 8 | 0.009 |
| Consumer of added fats | 13 (83) | 15 (47) | 12 (36) | 0.25 | 23 (141) | 22 (70) | 24 (71) | 0.65 |
| Liking scores at 8–12-year-old (0–10) | ||||||||
| Sweetness | 4.6 ± 1.3 | 4.7 ± 1.3 | 4.4 ± 1.3 | 0.004 | 4.6 ± 1.3 | 4.8 ± 1.3 | 4.4 ± 1.3 | 0.004 |
| Fattiness | 5.7 ± 1.2 | 5.9 ± 1.8 | 5.7 ± 1.7 | 0.18 | 5.7 ± 1.2 | 5.9 ± 1.8 | 5.7 ± 1.6 | 0.21 |
| Sweetness-and-fattiness | 5.8 ± 1.7 | 5.8 ± 1.3 | 5.6 ± 1.2 | 0.04 | 5.8 ± 1.7 | 5.8 ± 1.3 | 5.7 ± 1.1 | 0.13 |
| Unadjusted | Adjusted 1 Imputed | Adjusted 1 Complete-Case | |
|---|---|---|---|
| Dietary intake at | |||
| 8 months 2 | n = 616 | n = 616 | n = 555 |
| Carbohydrate intake (per 10 g/d) | 0.05 [0.00; 0.11] | 0.03 [−0.02; 0.09] | 0.02 [−0.04; 0.08] |
| Sugar intake (per 10 g/d) | 0.06 [0.00; 0.12] | 0.05 [−0.01; 0.12] | 0.05 [−0.01; 0.12] |
| Consumer of added sugars | −0.01 [−0.26; 0.23] | −0.04 [−0.28; 0.20] | −0.05 [−0.31; 0.21] |
| 12 months 2 | n = 610 | n = 610 | n = 543 |
| Carbohydrate intake (per 10 g/d) | Boys: −0.05 [−0.12; 0.01] | Boys: −0.06 [−0.13; 0.01] 3 Girls: 0.07 [0.00; 0.14] | Boys: −0.08 [−0.15; −0.01] |
| Girls: 0.08 [0.01; 0.15] | Girls: 0.07 [0.00; 0.15] | ||
| Sugar intake (per 10 g/d) | Boys: 0.01 [−0.08; 0.11] | Boys: −0.01 [−0.10; 0.09] 3 Girls: 0.09 [−0.01; 0.19] | Boys: −0.02 [−0.12; 0.07] |
| Girls: 0.11 [0.02; 0.21] | Girls: 0.07 [−0.03; 0.18] | ||
| Consumer of added sugars | 0.01 [−0.21; 0.23] | 0.02 [−0.20; 0.24] | −0.04 [−0.28; 0.20] |
| Unadjusted | Adjusted 1 Imputed | Adjusted 1 Complete-Case | |
|---|---|---|---|
| Dietary intake at | |||
| 8 months 2 | n = 616 | n = 616 | n = 555 |
| Fat intake (per 10 g/d) | 0.07 [−0.07; 0.21] | 0.02 [−0.12; 0.16] | 0.03 [−0.12; 0.17] |
| Consumer of added fats | −0.01 [−0.3; 0.28] | −0.03 [−0.32; 0.27] | 0.08 [−0.24; 0.41] |
| 12 months | n = 610 | n = 610 | n = 543 |
| Fat intake (per 10 g/d) | 0.07 [−0.05; 0.18] | 0.04 [−0.08; 0.16] | 0.05 [−0.08; 0.17] |
| Consumer of added fats | −0.09 [−0.32; 0.14] | −0.05 [−0.28; 0.18] | −0.12 [−0.38; 0.13] |
| Unadjusted | Adjusted 1 Imputed | Adjusted 1 Complete-Case | |
|---|---|---|---|
| Dietary intake at | |||
| 8 months 2 | n = 616 | n = 616 | n = 555 |
| Carbohydrate intake (per 10 g/d) | 0.07 [0.00; 0.14] | 0.09 [0.01; 0.16] | 0.07 [−0.01; 0.14] |
| Sugar intake (per 10 g/d) | 0.04 [−0.04; 0.12] | 0.04 [−0.04; 0.12] | 0.04 [−0.05; 0.12] |
| Consumer of added sugars | −0.06 [−0.46; 0.35] | −0.16 [−0.48; 0.15] | −0.18 [−0.51; 0.16] |
| Fat intake (per 10 g/d) | 0.01 [−0.18; 0.20] | −0.03 [−0.23; 0.17] | −0.01 [−0.21; 0.20] |
| Consumer of added fats | −0.13 [−0.44; 0.18] | −0.05 [−0.47; 0.36] | 0.06 [−0.40; 0.32] |
| 12 months | n = 610 | n = 610 | n = 543 |
| Carbohydrate intake (per 10 g/d) | 0.03 [−0.03; 0.09] | 0.02 [−0.04; 0.08] | 0.01 [−0.06; 0.07] |
| Sugar intake (per 10 g/d) | 0.01 [−0.07; 0.10] | 0.00 [−0.09; 0.09] | −0.01 [−0.10; 0.08] |
| Consumer of added sugars | −0.02 [−0.34; 0.31] | 0.04 [−0.25; 0.32] | 0.03 [−0.28; 0.33] |
| Fat intake (per 10 g/d) | 0.00 [−0.16; 0.17] | −0.02 [−0.18; 0.15] | −0.02 [−0.19; 0.15] |
| Consumer of added fats | 0.00 [−0.28; 0.29] | 0.03 [−0.30; 0.36] | −0.04 [−0.40; 0.32] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yuan, W.L.; Nicklaus, S.; Forhan, A.; Chabanet, C.; Heude, B.; Charles, M.-A.; Lange, C.; de Lauzon-Guillain, B. Associations between Infant Dietary Intakes and Liking for Sweetness and Fattiness Sensations in 8-to-12-Year-Old Children. Nutrients 2021, 13, 2659. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13082659
Yuan WL, Nicklaus S, Forhan A, Chabanet C, Heude B, Charles M-A, Lange C, de Lauzon-Guillain B. Associations between Infant Dietary Intakes and Liking for Sweetness and Fattiness Sensations in 8-to-12-Year-Old Children. Nutrients. 2021; 13(8):2659. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13082659
Chicago/Turabian StyleYuan, Wen Lun, Sophie Nicklaus, Anne Forhan, Claire Chabanet, Barbara Heude, Marie-Aline Charles, Christine Lange, and Blandine de Lauzon-Guillain. 2021. "Associations between Infant Dietary Intakes and Liking for Sweetness and Fattiness Sensations in 8-to-12-Year-Old Children" Nutrients 13, no. 8: 2659. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13082659