
Soy Isoflavones Intake and Obesity in Chinese Adults: A Cross-Sectional Study in Shanghai, China

 , , , and
, , , and
Abstract
:1. Introduction
2. Material and Methods
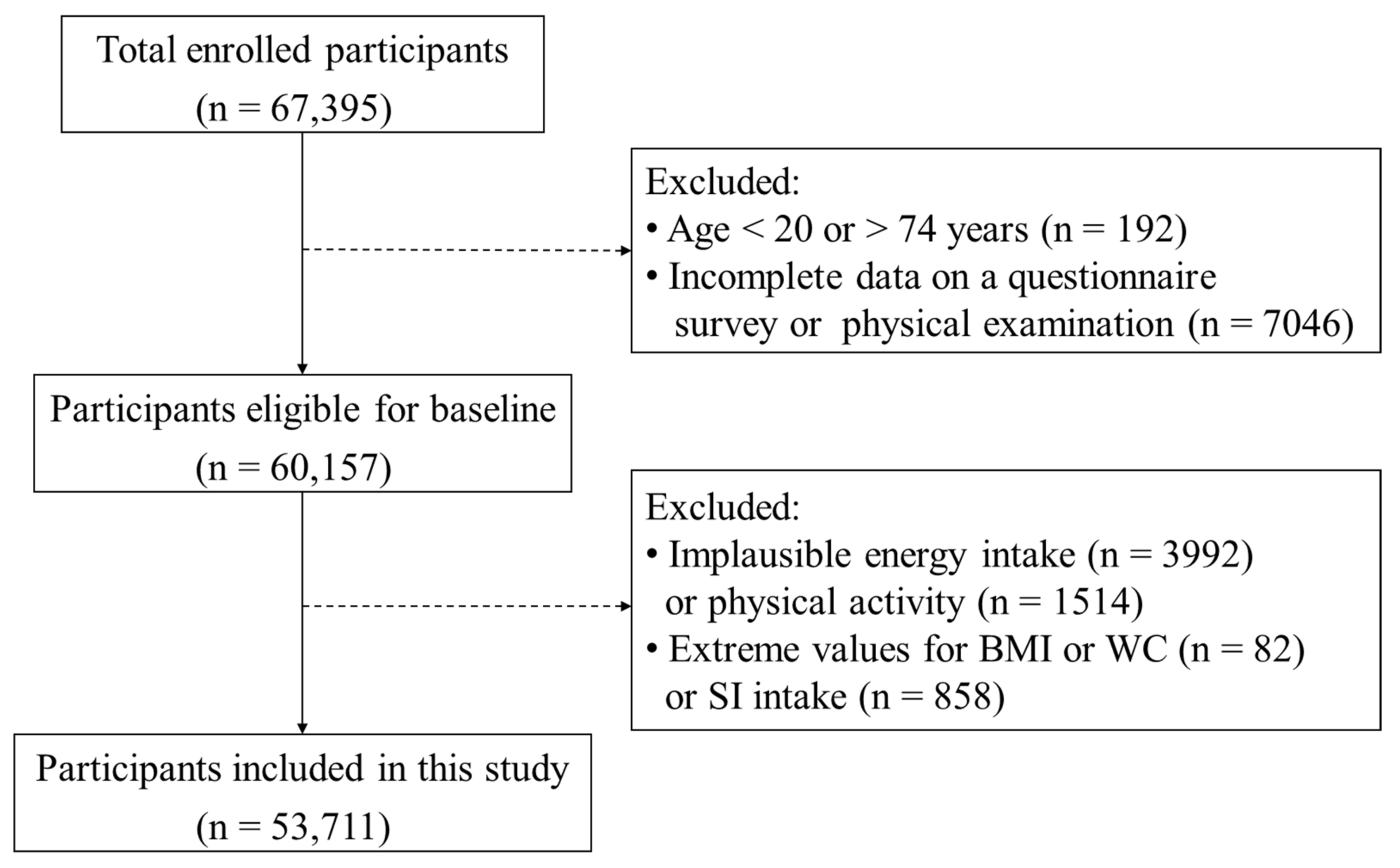
2.1. Study Design and Population
2.2. Estimated Dietary Intake of SI
2.3. Anthropometric Measurement and Outcome Ascertainment
2.4. Assessment of Covariates
2.5. Sensitivity Analysis
2.6. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| SI | Soy isoflavones |
| FFQ | Food frequency questionnaire |
| BMI | Body mass index |
| WC | Waist circumference |
| RCS | Restricted cubic spline |
| OR | Odds ratios |
| CI | Confidence interval |
| PA | Physical activity |
| NCDs | Non-communicable diseases |
| RCTs | Randomized controlled trials |
| SSACB | The Shanghai Suburban Adult Cohort and Biobank study |
| MET | Metabolic equivalent of task |
| IPAQ | International Physical Activity Questionnaire |
| h | Hours |
| SD | Standard deviation |
| IQR | Interquartile range |
| FA | Fatty acids |
| PPARs | Peroxisome proliferator-activated receptors |
| ODMA | O-desmethylangolensin |
References
- Wang, S.; Wang, Y.; Pan, M.H.; Ho, C.T. Anti-obesity molecular mechanism of soy isoflavones: Weaving the way to new therapeutic routes. Food Funct. 2017, 8, 3831–3846. [Google Scholar] [CrossRef] [PubMed]
- Renehan, A.G.; Tyson, M.; Egger, M.; Heller, R.F.; Zwahlen, M. Body-mass index and incidence of cancer: A systematic review and meta-analysis of prospective observational studies. Lancet 2008, 371, 569–578. [Google Scholar] [CrossRef]
- Visscher, T.L.; Seidell, J.C. The public health impact of obesity. Annu. Rev. Public Health 2001, 22, 355–375. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bluher, M. Obesity: Global epidemiology and pathogenesis. Nat. Rev. Endocrinol. 2019, 15, 288–298. [Google Scholar] [CrossRef] [PubMed]
- Diabetes, T.L. Metabolic health: A priority for the post-pandemic era. Lancet Diabetes Endocrinol. 2021, 9, 189. [Google Scholar]
- Report on the Nutrition and Chronic Disease Status of Chinese Residents (2020); National Health Commission of the People’s Republic of China: Beijing, China, 2020.
- Ryan, D.H.; Yockey, S.R. Weight loss and improvement in comorbidity: Differences at 5%, 10%, 15%, and over. Curr. Obes. Rep. 2017, 6, 187–194. [Google Scholar] [CrossRef] [PubMed]
- Mortensen, A.; Kulling, S.E.; Schwartz, H.; Rowland, I.; Ruefer, C.E.; Rimbach, G.; Cassidy, A.; Magee, P.; Millar, J.; Hall, W.L.; et al. Analytical and compositional aspects of isoflavones in food and their biological effects. Mol. Nutr. Food Res. 2009, 53, S266–S309. [Google Scholar] [CrossRef]
- Křížová, L.; Dadáková, K.; Kašparovská, J.; Kašparovský, T. Isoflavones. Molecules 2019, 24, 1076. [Google Scholar] [CrossRef] [Green Version]
- Luo, Q.; Cheng, D.; Huang, C.; Li, Y.; Lao, C.; Xia, Y.; Liu, W.; Gong, X.; Hu, D.; Li, B.; et al. Improvement of colonic immune function with soy isoflavones in high-fat diet-induced obese rats. Molecules 2019, 24, 1139. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tan, J.; Huang, C.; Luo, Q.; Liu, W.; Cheng, D.; Li, Y.; Xia, Y.; Li, C.; Tang, L.; Fang, J.; et al. Soy isoflavones ameliorate fatty acid metabolism of visceral adipose tissue by increasing the AMPK activity in male rats with Diet-Induced Obesity (DIO). Molecules 2019, 24, 2809. [Google Scholar] [CrossRef] [Green Version]
- Crespillo, A.; Alonso, M.; Vida, M.; Pavon, F.J.; Serrano, A.; Rivera, P.; Romero-Zerbo, Y.; Fernandez-Llebrez, P.; Martinez, A.; Perez-Valero, V.; et al. Reduction of body weight, liver steatosis and expression of stearoyl-CoA desaturase 1 by the isoflavone daidzein in diet-induced obesity. Br. J. Pharmacol. 2011, 164, 1899–1915. [Google Scholar] [CrossRef] [Green Version]
- Zhang, Y.; Na, X.; Zhang, Y.; Li, L.; Zhao, X.; Cui, H. Isoflavone reduces body weight by decreasing food intake in ovariectomized rats. Ann. Nutr. Metab. 2009, 54, 163–170. [Google Scholar] [CrossRef] [PubMed]
- Davis, J.; Higginbotham, A.; O’Connor, T.; Moustaid-Moussa, N.; Tebbe, A.; Kim, Y.C.; Cho, K.W.; Shay, N.; Adler, S.; Peterson, R.; et al. Soy protein and isoflavones influence adiposity and development of metabolic syndrome in the obese male ZDF rat. Ann. Nutr. Metab. 2007, 51, 42–52. [Google Scholar] [CrossRef] [PubMed]
- Michael, M.R.; Wolz, E.; Davidovich, A.; Pfannkuch, F.; Edwards, J.A.; Bausch, J. Acute, subchronic and chronic safety studies with genistein in rats. Food Chem. Toxicol. 2006, 44, 56–80. [Google Scholar] [CrossRef]
- Manzoni, M.S.; Rossi, E.A.; Carlos, I.Z.; Vendramini, R.C.; Duarte, A.C.; Damaso, A.R. Fermented soy product supplemented with isoflavones affected fat depots in juvenile rats. Nutrition 2005, 21, 1018–1024. [Google Scholar] [CrossRef] [PubMed]
- Goodman-Gruen, D.; Kritz-Silverstein, D. Usual dietary isoflavone intake is associated with cardiovascular disease risk factors in postmenopausal women. J. Nutr. 2001, 131, 1202–1206. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.; Kim, J.; Jun, S.; Wie, G.; Shin, S.; Joung, H. Association between dietary flavonoid intake and obesity among adults in Korea. Appl. Physiol. Nutr. Metab. 2020, 45, 203–212. [Google Scholar] [CrossRef] [Green Version]
- Goodman-Gruen, D.; Kritz-Silverstein, D. Usual dietary isoflavone intake and body composition in postmenopausal women. Menopause 2003, 10, 427–432. [Google Scholar] [CrossRef] [PubMed]
- Akhlaghi, M.; Zare, M.; Nouripour, F. Effect of soy and soy isoflavones on obesity-related anthropometric measures: A systematic review and meta-analysis of randomized controlled clinical trials. Adv. Nutr. 2017, 8, 705–717. [Google Scholar] [CrossRef]
- Zhang, Y.B.; Chen, W.H.; Guo, J.J.; Fu, Z.H.; Yi, C.; Zhang, M.; Na, X.L. Soy isoflavone supplementation could reduce body weight and improve glucose metabolism in non-Asian postmenopausal women—A meta-analysis. Nutrition 2013, 29, 8–14. [Google Scholar] [CrossRef]
- Wu, J.; Wang, X.; Chiba, H.; Higuchi, M.; Nakatani, T.; Ezaki, O.; Cui, H.; Yamada, K.; Ishimi, Y. Combined intervention of soy isoflavone and moderate exercise prevents body fat elevation and bone loss in ovariectomized mice. Metabolism 2004, 53, 942–948. [Google Scholar] [CrossRef]
- Zheng, W.; Rogoschin, J.; Niehoff, A.; Oden, K.; Kulling, S.E.; Xie, M.; Diel, P. Combinatory effects of phytoestrogens and exercise on body fat mass and lipid metabolism in ovariectomized female rats. J. Steroid Biochem. Mol. Biol. 2018, 178, 73–81. [Google Scholar] [CrossRef]
- Aubertin-Leheudre, M.; Lord, C.; Khalil, A.; Dionne, I.J. Effect of 6 months of exercise and isoflavone supplementation on clinical cardiovascular risk factors in obese postmenopausal women: A randomized, double-blind study. Menopause 2007, 14, 624–629. [Google Scholar] [CrossRef] [PubMed]
- Wu, J.; Oka, J.; Higuchi, M.; Tabata, I.; Toda, T.; Fujioka, M.; Fuku, N.; Teramoto, T.; Okuhira, T.; Ueno, T.; et al. Cooperative effects of isoflavones and exercise on bone and lipid metabolism in postmenopausal Japanese women: A randomized placebo-controlled trial. Metabolism 2006, 55, 423–433. [Google Scholar] [CrossRef]
- Orsatti, F.L.; Nahas, E.A.; Nahas-Neto, J.; Maesta, N.; Orsatti, C.L.; Fernandes, C.E. Effects of resistance training and soy isoflavone on body composition in postmenopausal women. Obstet. Gynecol. Int. 2010, 2010, 156037. [Google Scholar] [CrossRef]
- Maesta, N.; Nahas, E.A.P.; Nahas-Neto, J.; Orsatti, F.L.; Fernandes, C.E.; Traiman, P.; Burini, R.C. Effects of soy protein and resistance exercise on body composition and blood lipids in postmenopausal women. Maturitas 2007, 56, 350–358. [Google Scholar] [CrossRef]
- Choquette, S.; Riesco, É.; Cormier, É.; Dion, T.; Aubertin-Leheudre, M.; Dionne, I.J. Effects of soya isoflavones and exercise on body composition and clinical risk factors of cardiovascular diseases in overweight postmenopausal women: A 6-month double-blind controlled trial. Br. J. Nutr. 2011, 105, 1199–1209. [Google Scholar] [CrossRef] [Green Version]
- Wu, J.; Oka, J.; Tabata, I.; Higuchi, M.; Toda, T.; Fuku, N.; Ezaki, J.; Sugiyama, F.; Uchiyama, S.; Yamada, K.; et al. Effects of isoflavone and exercise on BMD and fat mass in postmenopausal Japanese women: A 1-year randomized placebo-controlled trial. J. Bone Miner. Res. 2006, 21, 780–789. [Google Scholar] [CrossRef] [PubMed]
- Dai, Q.; Shu, X.O.; Jin, F.; Potter, J.D.; Kushi, L.H.; Teas, J.; Gao, Y.T.; Zheng, W. Population-based case-control study of soyfood intake and breast cancer risk in Shanghai. Br. J. Cancer 2001, 85, 372–378. [Google Scholar] [CrossRef] [PubMed]
- Yu, D.; Shu, X.O.; Li, H.; Yang, G.; Cai, Q.; Xiang, Y.B.; Ji, B.T.; Franke, A.A.; Gao, Y.T.; Zheng, W.; et al. Dietary isoflavones, urinary isoflavonoids, and risk of ischemic stroke in women. Am. J. Clin. Nutr. 2015, 102, 680–686. [Google Scholar] [CrossRef] [Green Version]
- Wang, Q.; Liu, L.; Li, H.; Tao, P.; Qi, Y.; Li, J. Effects of High-Order Interactions among IGFBP-3 Genetic Polymorphisms, Body Mass Index and Soy Isoflavone Intake on Breast Cancer Susceptibility. PLoS ONE 2016, 11, e162970. [Google Scholar] [CrossRef]
- Zhang, M.; Xie, X.; Lee, A.H.; Binns, C.W. soy and isoflavone intake are associated with reduced risk of ovarian cancer in Southeast China. Nutr. Cancer 2004, 49, 125–130. [Google Scholar] [CrossRef] [PubMed]
- Zhao, Q.; Chen, B.; Wang, R.; Zhu, M.; Shao, Y.; Wang, N.; Liu, X.; Zhang, T.; Jiang, F.; Wang, W.; et al. Cohort profile: Protocol and baseline survey for the Shanghai Suburban Adult Cohort and Biobank (SSACB) study. BMJ Open 2020, 10, e35430. [Google Scholar] [CrossRef]
- Yang, Y. China Food Composition Standard Edition, 6th ed.; China Peking University Medical Press: Beijing, China, 2018; pp. 284–288. [Google Scholar]
- Park, Y.M.; White, A.J.; Jackson, C.L.; Weinberg, C.R.; Sandler, D.P. Association of exposure to artificial light at night while sleeping with risk of obesity in women. JAMA Intern. Med. 2019, 179, 1061. [Google Scholar] [CrossRef] [PubMed]
- National Health and Family Commission. Criteria of weight for adults. In WS/T 428-2013; China Standards Press: Beijing, China, 2013. [Google Scholar]
- Li, J.; Lv, J.; Gao, M.; Yu, C.; Guo, Y.; Bian, Z.; Pei, P.; Du, H.; Chen, J.; Chen, Z.; et al. Association of body mass index and waist circumference with major chronic diseases in Chinese adults. Chin. J. Epidemiol. 2019, 40, 1541–1542. [Google Scholar]
- Craig, C.L.; Marshall, A.L.; Sjostrom, M.; Bauman, A.E.; Booth, M.L.; Ainsworth, B.E.; Pratt, M.; Ekelund, U.; Yngve, A.; Sallis, J.F.; et al. International physical activity questionnaire: 12-country reliability and validity. Med. Sci. Sports Exerc. 2003, 35, 1381–1395. [Google Scholar] [CrossRef] [Green Version]
- Defining Adult Overweight & Obesity. Available online: https://www.cdc.gov/obesity/adult/defining.html (accessed on 29 July 2021).
- Abdominal Obesity Measurement Guidelines for Different Ethnic Groups. Available online: https://www.hsph.harvard.edu/obesity-prevention-source/waist-circumference-guidelines-for-different-ethnic-groups/ (accessed on 29 July 2021).
- Messina, M.; Nagata, C.; Wu, A.H. Estimated Asian adult soy protein and isoflavone intakes. Nutr. Cancer 2006, 55, 1–12. [Google Scholar] [CrossRef]
- Rietjens, I.; Louisse, J.; Beekmann, K. The potential health effects of dietary phytoestrogens. Br. J. Pharmacol. 2017, 174, 1263–1280. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mauvais-Jarvis, F.; Clegg, D.J.; Hevener, A.L. The role of estrogens in control of energy balance and glucose homeostasis. Endocr. Rev. 2013, 34, 309–338. [Google Scholar] [CrossRef] [Green Version]
- Ørgaard, A.; Jensen, L. The effects of soy isoflavones on obesity. Exp. Biol. Med. 2008, 233, 1066–1080. [Google Scholar] [CrossRef] [Green Version]
- Byung-Cheol, L.; Jongsoon, L. Cellular and molecular players in adipose tissue inflammation in the development of obesity-induced insulin resistance. Biochim. Biophys. Acta 2014, 1842, 446–462. [Google Scholar]
- Yuri, S.; Junko, K.; Mariko, T.; Ayano, N.; Kazuo, K.; Kaoruko, I. The dietary isoflavone daidzein reduces expression of pro-inflammatory genes through PPAR α/γ and JNK pathways in adipocyte and macrophage co-cultures. PLoS ONE 2016, 11, e149676. [Google Scholar]
- Fändriks, L. Roles of the gut in the metabolic syndrome: An overview. J. Intern. Med. 2017, 281, 319–336. [Google Scholar] [CrossRef]
- De Kleijn, M.J.; Van der Schouw, Y.T.; Wilson, P.W.; Adlercreutz, H.; Mazur, W.; Grobbee, D.E.; Jacques, P.F. Intake of dietary phytoestrogens is low in postmenopausal women in the United States: The Framingham study (1–4). J. Nutr. 2001, 131, 1826–1832. [Google Scholar] [CrossRef] [Green Version]
- Setchell, K.D.; Cassidy, A. Dietary isoflavones: Biological effects and relevance to human health. J. Nutr. 1999, 129, 758S–767S. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ajdzanovic, V.; Medigovic, I.; Zivanovic, J.; Mojic, M.; Milosevic, V. Membrane steroid receptor-mediated action of soy isoflavones: Tip of the iceberg. J. Membr. Biol. 2015, 248, 1–6. [Google Scholar] [CrossRef]
- Matsumura, Y.; Nakagawa, Y.; Mikome, K.; Yamamoto, H.; Osakabe, N. Enhancement of energy expenditure following a single oral dose of flavan-3-ols associated with an increase in catecholamine secretion. PLoS ONE 2014, 9, e112180. [Google Scholar] [CrossRef] [PubMed]
- Bhathena, S.J.; Velasquez, M.T. Beneficial role of dietary phytoestrogens in obesity and diabetes. Am. J. Clin. Nutr. 2002, 76, 1191–1201. [Google Scholar] [CrossRef] [Green Version]
- Maskarinec, G.; Aylward, A.G.; Erber, E.; Takata, Y.; Kolonel, L.N. Soy intake is related to a lower body mass index in adult women. Eur. J. Nutr. 2008, 47, 138–144. [Google Scholar] [CrossRef] [Green Version]
- Huang, C.; Pang, D.; Luo, Q.; Chen, X.; Gao, Q.; Shi, L.; Liu, W.; Zou, Y.; Li, L.; Chen, Z. Soy Isoflavones Regulate Lipid Metabolism through an AKT/mTORC1 Pathway in Diet-Induced Obesity (DIO) Male Rats. Molecules 2016, 21, 586. [Google Scholar] [CrossRef] [Green Version]
- Cerhan, J.R.; Moore, S.C.; Jacobs, E.J.; Kitahara, C.M.; Rosenberg, P.S.; Adami, H.O.; Ebbert, J.O.; English, D.R.; Gapstur, S.M.; Giles, G.G.; et al. A pooled analysis of waist circumference and mortality in 650,000 adults. Mayo Clin. Proc. 2014, 89, 335–345. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Power, M.L.; Schulkin, J. Sex differences in fat storage, fat metabolism, and the health risks from obesity: Possible evolutionary origins. Br. J. Nutr. 2008, 99, 931–940. [Google Scholar] [CrossRef]
- Auro, K.; Joensuu, A.; Fischer, K.; Kettunen, J.; Salo, P.; Mattsson, H.; Niironen, M.; Kaprio, J.; Eriksson, J.G.; Lehtimaki, T.; et al. A metabolic view on menopause and ageing. Nat. Commun. 2014, 5, 4708. [Google Scholar] [CrossRef] [Green Version]
- Sijia, T.; Yang, D.; Chorong, O.; No, J. Effects of soy foods in postmenopausal women: A focus on osteosarcopenia and obesity. J. Obes. Metab. Syndr. 2020, 29, 180–187. [Google Scholar]
- Reed, K.E.; Camargo, J.; Hamilton-Reeves, J.; Kurzer, M.; Messina, M. Neither soy nor isoflavone intake affects male reproductive hormones: An expanded and updated meta-analysis of clinical studies. Reprod. Toxicol. 2021, 100, 60–67. [Google Scholar] [CrossRef]
- Kumar, N.B.; Cantor, A.; Allen, K.; Riccardi, D.; Cox, C.E. The specific role of isoflavones on estrogen metabolism in premenopausal women. Cancer 2002, 94, 1166–1174. [Google Scholar] [CrossRef] [PubMed]
- Husain, D.; Khanna, K.; Puri, S.; Haghighizadeh, M. Supplementation of soy isoflavones improved sex hormones, blood pressure, and postmenopausal symptoms. J. Am. Coll. Nutr. 2015, 34, 42–48. [Google Scholar] [CrossRef]
- Soukup, S.T.; Helppi, J.; Muller, D.R.; Zierau, O.; Watzl, B.; Vollmer, G.; Diel, P.; Bub, A.; Kulling, S.E. Phase II metabolism of the soy isoflavones genistein and daidzein in humans, rats and mice: A cross-species and sex comparison. Arch. Toxicol. 2016, 90, 1335–1347. [Google Scholar] [CrossRef] [PubMed]
- Slikker, W.J.; Scallet, A.C.; Doerge, D.R.; Ferguson, S.A. Gender-based differences in rats after chronic dietary exposure to genistein. Int. J. Toxicol. 2001, 20, 175–179. [Google Scholar] [CrossRef]
- Lu, L.J.; Anderson, K.E. Sex and long-term soy diets affect the metabolism and excretion of soy isoflavones in humans. Am. J. Clin. Nutr. 1998, 68, 1500S–1504S. [Google Scholar] [CrossRef] [Green Version]
- Touvier, M.; Druesne-Pecollo, N.; Kesse-Guyot, E.; Andreeva, V.A.; Fezeu, L.; Galan, P.; Hercberg, S.; Latino-Martel, P. Dual association between polyphenol intake and breast cancer risk according to alcohol consumption level: A prospective cohort study. Breast Cancer Res. Treat. 2013, 137, 225–236. [Google Scholar] [CrossRef] [PubMed]
- Yoon, G.A.; Park, S. Antioxidant action of soy isoflavones on oxidative stress and antioxidant enzyme activities in exercised rats. Nutr. Res. Pract. 2014, 8, 618–624. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pabich, M.; Materska, M. Biological effect of soy isoflavones in the prevention of civilization diseases. Nutrients 2019, 11, 1660. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Characteristics | All Subjects | Tertiles of Dietary SI Intake | p Value | ||
|---|---|---|---|---|---|
| (n = 53,711) | T1 (n = 17,667) | T2 (n = 18,309) | T3 (n = 17,735) | ||
| Age (years) | 57.3 ± 11.3 | 58.4 ± 10.3 | 57.6 ± 10.7 | 55.8 ± 12.5 | <0.001 |
| Sex | <0.001 | ||||
| Men | 20,887 (38.9) | 6307 (35.7) | 7041 (38.5) | 7539 (42.5) | |
| Women | 32,824 (61.1) | 11,360 (64.3) | 11,268 (61.5) | 10,196 (57.5) | |
| Education level | <0.001 | ||||
| Primary school or below | 18,212(33.9) | 7646(43.3) | 6488(35.4) | 4078(23.0) | |
| Middle school | 20,552 (38.3) | 6545 (37.1) | 7380 (40.3) | 6627 (37.4) | |
| High school | 8863 (16.5) | 2289 (12.9) | 2797 (15.3) | 3777 (21.3) | |
| College or above | 6084 (11.3) | 1187 (6.7) | 1644 (9.0) | 3253 (18.3) | |
| Marital status | <0.001 | ||||
| Married | 49,046 (91.3) | 16,235 (91.9) | 16,970 (92.7) | 15,841 (89.3) | |
| Others a | 4665 (8.7) | 1432 (8.1) | 1339 (7.3) | 1894 (10.7) | |
| Smoking | 0.185 | ||||
| Never | 42,520 (79.2) | 14,048 (79.5) | 14,417 (78.7) | 14,055 (79.2) | |
| Ever | 11,191 (20.8) | 3619 (20.5) | 3892 (21.3) | 3680 (20.8) | |
| Alcohol drinking | 0.081 | ||||
| Never | 47,368 (88.2) | 15,653 (88.6) | 16,137 (88.1) | 15,578 (87.8) | |
| Ever | 6343 (11.8) | 2014 (11.4) | 2172 (11.9) | 2157 (12.2) | |
| Tea consumption | <0.001 | ||||
| Never | 37,394 (69.6) | 13,015 (73.7) | 13,082 (71.5) | 11,297 (63.7) | |
| Ever | 16,317 (30.4) | 4652 (26.3) | 5227 (28.6) | 6438 (36.3) | |
| Sleep duration (hours) | <0.001 | ||||
| <6 | 10,006 (18.6) | 3310 (18.7) | 3579 (19.6) | 3117 (17.6) | |
| 6–8 | 34,360 (64.0) | 11,143 (63.1) | 11,652 (63.6) | 11,565 (65.2) | |
| ≥8 | 9345 (17.4) | 3214 (18.2) | 3078 (16.8) | 3053 (17.2) | |
| Prevalent chronic diseases b | <0.001 | ||||
| No | 28,943 (53.9) | 9172 (51.9) | 10,055 (54.9) | 9716 (54.8) | |
| Yes | 24,768 (46.1) | 8495 (48.1) | 8254 (45.1) | 8019 (45.2) | |
| Menopausal status (women) | <0.001 | ||||
| Premenopausal | 8237 (25.1) | 2475 (21.8) | 2716 (24.1) | 3046 (29.9) | |
| Postmenopausal | 24,587 (74.9) | 8885 (78.2) | 8552 (75.9) | 7150 (70.1) | |
| Sedentary time (h/day) | 4 (2, 5) | 3 (2, 5) | 4 (2, 5) | 4 (2, 5) | <0.001 |
| PA (METs-h/week) | 60.8 (36.4, 84) | 59.2 (35.2, 84.0) | 56 (36, 84.0) | 66 (39.6, 84.0) | <0.001 |
| PA level | <0.001 | ||||
| Low | 17,675 (32.9) | 5880 (33.3) | 6146 (33.6) | 5649 (31.9) | |
| Moderate | 16,178 (30.1) | 5227 (29.6) | 5633 (30.8) | 5318 (29.9) | |
| High | 19,858 (37.0) | 6560 (37.1) | 6530 (35.7) | 6768 (38.2) | |
| Energy intake (kcal/day) | 1080 (824, 1430) | 880 (696, 1127) | 1058 (833, 1346) | 1368 (1065, 1760) | <0.001 |
| Body Measurements | Tertiles of SI Intake (mg/d) a | p Value | p for Trend | ||
|---|---|---|---|---|---|
| T1 (n = 17,677) | T2 (n = 18,309) | T3 (n = 17,735) | |||
| BMI (kg/m2) | 24.4 ± 3.3 | 24.3 ± 3.3 | 24.2 ± 3.3 | <0.001 | <0.001 |
| WC (cm) | 82.0 ± 9.3 | 81.9 ± 9.3 | 82.1 ± 9.5 | 0.259 | 0.816 |
| Overall obesity b | <0.001 | <0.001 | |||
| Normal | 8370 (47.4) | 8893 (48.6) | 8768 (49.4) | ||
| Overweight | 6931 (39.2) | 7160 (39.1) | 6841 (38.6) | ||
| Obesity | 2366 (13.4) | 2256 (12.3) | 2126 (12.0) | ||
| Central obesity c | <0.001 | <0.001 | |||
| No | 12,168 (68.9) | 12,919 (70.6) | 12,537 (70.7) | ||
| Yes | 5499 (31.1) | 5390 (29.4) | 5198 (29.3) | ||
| No. of Subjects | OR (95% CI) for Dietary Intake of SI (mg/d) | p for Trend | p for Interaction | |||||
|---|---|---|---|---|---|---|---|---|
| T1 (<9.91) | T2 (9.91–18.07) | T3 (≥18.08) | ||||||
| Overweight | Obesity | Overweight | Obesity | |||||
| All subjects | ||||||||
| Model 1 | 53,711 | 1.00 (ref) | 0.97 (0.93, 1.02) | 0.90 (0.84, 0.96) | 0.94 (0.90, 0.99) | 0.86 (0.80, 0.92) | <0.001 | |
| Model 2 | 53,711 | 1.00 (ref) | 0.99 (0.95, 1.04) | 0.93 (0.87, 1.00) | 1.00 (0.95, 1.05) | 0.91 (0.85, 0.98) | 0.028 | |
| Sex a | <0.001 | |||||||
| Men | 20,887 | 1.00 (ref) | 0.96 (0.89, 1.04) | 0.82 (0.73, 0.91) | 1.03 (0.95, 1.11) | 0.89 (0.79, 0.99) | 0.047 | |
| Women b | 32,824 | 1.00 (ref) | 1.01 (0.96, 1.07) | 1.01 (0.93, 1.10) | 0.98 (0.91, 1.04) | 0.91 (0.82, 1.00) | 0.190 | |
| PA level (METs-h/week) a | 0.142 | |||||||
| Low: <50 | 17,675 | 1.00 (ref) | 0.98 (0.91, 1.06) | 0.92 (0.82, 1.04) | 1.00 (0.92, 1.10) | 0.96 (0.84, 1.09) | 0.729 | |
| Moderate: 50–84 | 16,178 | 1.00 (ref) | 1.03 (0.95, 1.12) | 0.86 (0.76, 0.97) | 1.07 (0.98, 1.18) | 0.89 (0.78, 1.02) | 0.017 | |
| High: >84 | 19,858 | 1.00 (ref) | 0.99 (0.91, 1.06) | 1.00 (0.90, 1.12) | 0.94 (0.87, 1.02) | 0.88 (0.78, 1.00) | 0.096 | |
| Menopausal status (women) a | 0.024 | |||||||
| Premenopausal | 8237 | 1.00 (ref) | 1.10 (0.97, 1.26) | 1.25 (1.02, 1.53) | 1.07 (0.94, 1.23) | 1.12 (0.90, 1.39) | 0.446 | |
| Postmenopausal | 24,587 | 1.00 (ref) | 0.99 (0.93, 1.06) | 0.96 (0.87, 1.06) | 0.96 (0.89, 1.03) | 0.86 (0.77, 0.96) | 0.029 | |
| No. of Subjects with Central Obesity (%) | OR (95% CI) for Dietary Intake of SI (mg/d) | p for Trend | p for Interaction | |||
|---|---|---|---|---|---|---|
| T1 (<9.91) | T2 (9.91–18.07) | T3 (≥18.08) | ||||
| All subjects | ||||||
| Model 1 | 16,087 (30.0) | 1.00 (ref) | 0.92 (0.88, 0.97) | 0.92 (0.88, 0.96) | 0.001 | |
| Model 2 | 16,087 (30.0) | 1.00 (ref) | 0.95 (0.90, 0.99) | 0.96 (0.91, 1.01) | 0.124 | |
| Model 3 | 16,087 (30.0) | 1.00 (ref) | 0.95 (0.90, 1.01) | 0.99 (0.93, 1.06) | 0.927 | |
| Sex a | <0.001 | |||||
| Men | 6700 (32.1) | 1.00 (ref) | 1.02 (0.92, 1.12) | 1.11 (1.00, 1.24) | 0.043 | |
| Women b | 9387 (28.6) | 1.00 (ref) | 0.92 (0.85, 1.00) | 0.91 (0.83, 0.99) | 0.026 | |
| PA level (METs-h/week) a | 0.145 | |||||
| Low: <50 | 5041 (28.5) | 1.00 (ref) | 0.97 (0.87, 1.07) | 1.10 (0.97, 1.23) | 0.149 | |
| Moderate: 50–84 | 4833 (29.9) | 1.00 (ref) | 0.91 (0.81, 1.01) | 0.91 (0.80, 1.03) | 0.111 | |
| High: >84 | 6213 (31.3) | 1.00 (ref) | 0.98 (0.89, 1.08) | 0.97 (0.87, 1.07) | 0.508 | |
| Menopausal status (women) a | 0.211 | |||||
| Premenopausal | 1300 (15.8) | 1.00 (ref) | 1.07 (0.88, 1.31) | 0.94 (0.76, 1.16) | 0.577 | |
| Postmenopausal | 8087 (32.9) | 1.00 (ref) | 0.89 (0.82, 0.97) | 0.90 (0.81, 0.99) | 0.015 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhu, J.; Zhao, Q.; Qiu, Y.; Zhang, Y.; Cui, S.; Yu, Y.; Chen, B.; Zhu, M.; Wang, N.; Liu, X.; et al. Soy Isoflavones Intake and Obesity in Chinese Adults: A Cross-Sectional Study in Shanghai, China. Nutrients 2021, 13, 2715. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13082715
Zhu J, Zhao Q, Qiu Y, Zhang Y, Cui S, Yu Y, Chen B, Zhu M, Wang N, Liu X, et al. Soy Isoflavones Intake and Obesity in Chinese Adults: A Cross-Sectional Study in Shanghai, China. Nutrients. 2021; 13(8):2715. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13082715
Chicago/Turabian StyleZhu, Junjie, Qi Zhao, Yun Qiu, Yue Zhang, Shuheng Cui, Yuting Yu, Bo Chen, Meiying Zhu, Na Wang, Xing Liu, and et al. 2021. "Soy Isoflavones Intake and Obesity in Chinese Adults: A Cross-Sectional Study in Shanghai, China" Nutrients 13, no. 8: 2715. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13082715