
Anemia among Women of Reproductive Age: An Overview of Global Burden, Trends, Determinants, and Drivers of Progress in Low- and Middle-Income Countries

Abstract
:1. Introduction
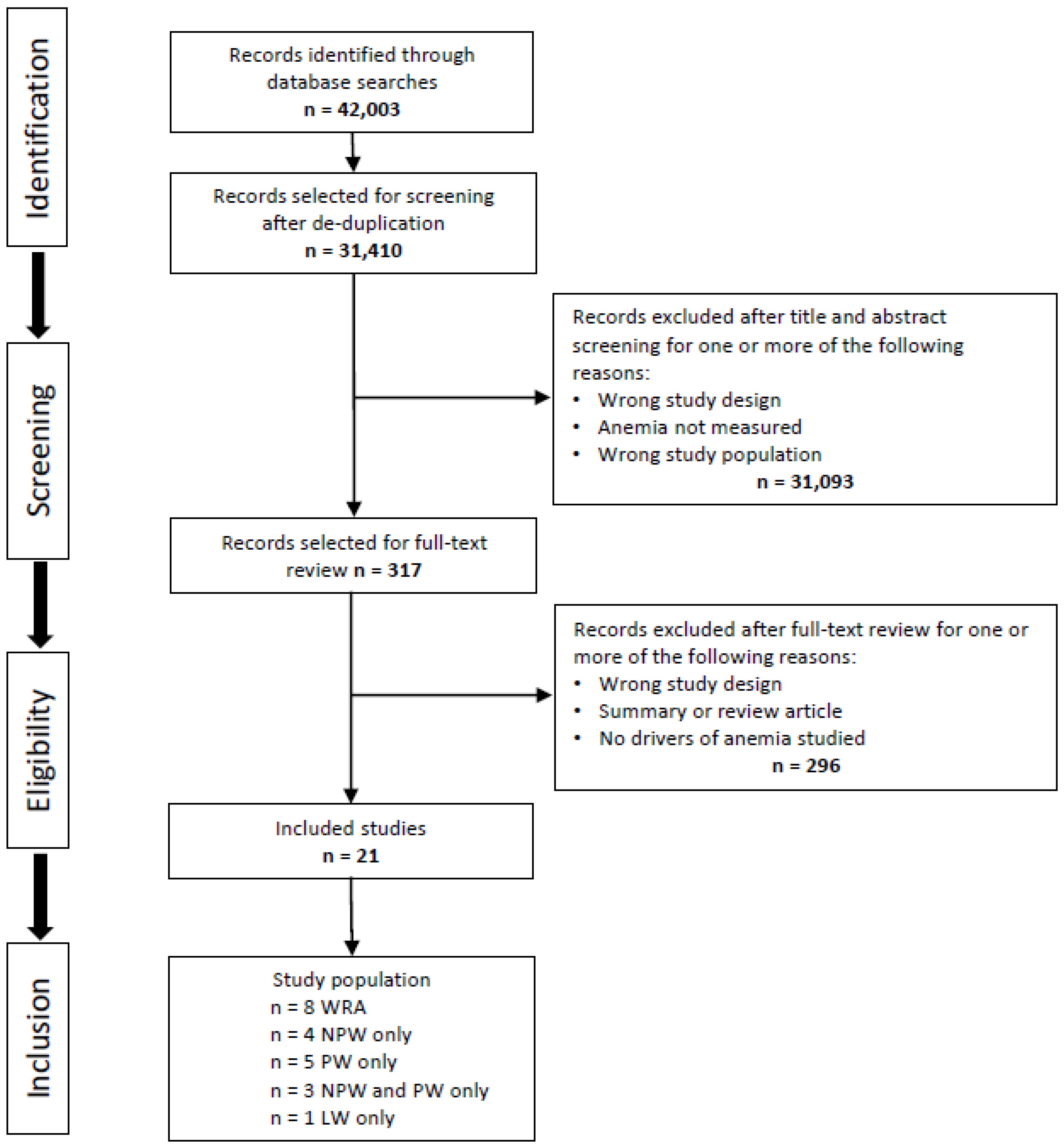
2. Methods
2.1. Search Strategy
- anaemia OR anemia
- low OR deficien*
- hemoglobin OR haemoglobin OR hb OR iron
- 2 AND 3
- 1 OR 4
- driver* OR determinant* OR polic* OR program* OR intervention* OR factor* OR predictor* OR initiativ* OR strateg* OR correlat* OR supplement* OR fortif*
- burden OR trend* OR longitudinal OR reduc* OR trajector* OR chang* OR declin*
- matern* OR pregnan* OR woman* OR women* OR antenatal OR prenatal OR perinatal OR gestat*
- 5 AND 6 AND 7 AND 8.
- Including women of reproductive age (pregnant, non-pregnant, or lactating women) from LMIC;
- Published in English between 1 January 1990 and 31 May 2021;
- Showing a reduction in anemia over two time points in national or large-scale regional studies;
- Examining at least one determinant or driver of anemia.
2.2. Methodological Quality Assessment
2.3. Data Analysis
2.4. Ethics
3. Results
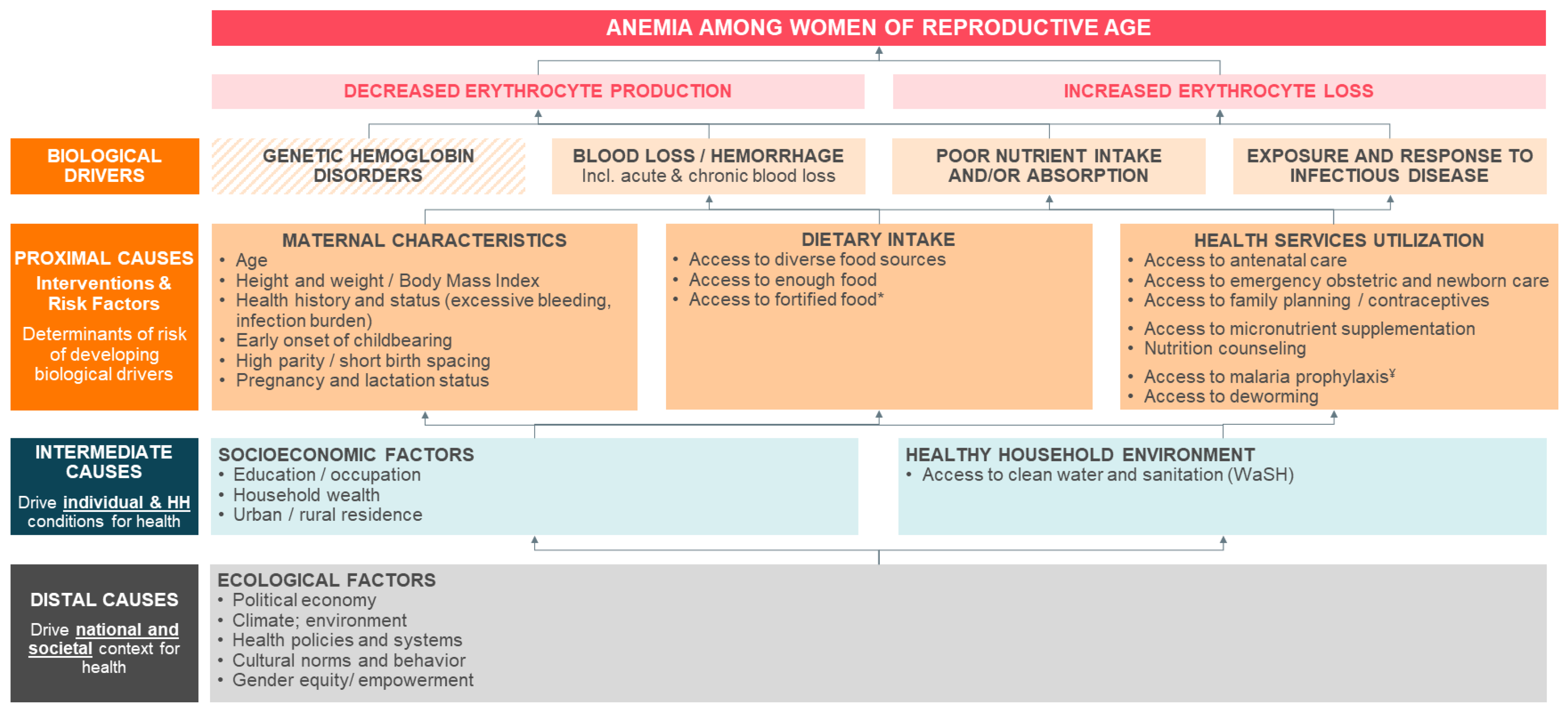
3.1. Conceptual Framework of WRA Anemia Determinants and Drivers
3.2. Study Characteristics
3.3. Proximal Determinants and Drivers of Anemia among WRA
3.3.1. Healthcare Utilization during Pregnancy and Lactation
3.3.2. General Healthcare Utilization
3.3.3. Dietary Intake
Large Scale Food Fortification Programs
3.3.4. Maternal Characteristics
Maternal Age
Marital Status
Parity and Birth Spacing
Infection Burden
BMI
3.4. Intermediate Determinants and Drivers of Anemia among WRA
3.4.1. Woman’s Education and Occupation
3.4.2. Spouse’s Education
3.4.3. Household Wealth
3.4.4. Urban/Rural Residence
3.4.5. Water, Sanitation and Hygiene (WaSH)
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Diseases, G.B.D.; Injuries, C. Global burden of 369 diseases and injuries in 204 countries and territories, 1990–2019: A systematic analysis for the Global Burden of Disease Study 2019. Lancet 2020, 396, 1204–1222. [Google Scholar] [CrossRef]
- WHO. Haemoglobin Concentrations for the Diagnosis of Anaemia and Assessment of Severity; World Health Organization: Geneva, Switzerland, 2011. [Google Scholar]
- Chaparro, C.M.; Suchdev, P.S. Anemia epidemiology, pathophysiology, and etiology in low- and middle-income countries. Ann. N. Y. Acad. Sci. 2019, 1450, 15–31. [Google Scholar] [CrossRef]
- Balarajan, Y.; Ramakrishnan, U.; Ozaltin, E.; Shankar, A.H.; Subramanian, S.V. Anaemia in low-income and middle-income countries. Lancet 2011, 378, 2123–2135. [Google Scholar] [CrossRef]
- Pasricha, S.R.; Drakesmith, H.; Black, J.; Hipgrave, D.; Biggs, B.A. Control of iron deficiency anemia in low- and middle-income countries. Blood 2013, 121, 2607–2617. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Keats, E.C.; Neufeld, L.M.; Garrett, G.S.; Mbuya, M.N.N.; Bhutta, Z.A. Improved micronutrient status and health outcomes in low- and middle-income countries following large-scale fortification: Evidence from a systematic review and meta-analysis. Am. J. Clin. Nutr. 2019, 109, 1696–1708. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Low, M.S.; Speedy, J.; Styles, C.E.; De-Regil, L.M.; Pasricha, S.R. Daily iron supplementation for improving anaemia, iron status and health in menstruating women. Cochrane Database Syst. Rev. 2016, 4, CD009747. [Google Scholar] [CrossRef]
- Wirth, J.P.; Woodruff, B.A.; Engle-Stone, R.; Namaste, S.M.; Temple, V.J.; Petry, N.; Macdonald, B.; Suchdev, P.S.; Rohner, F.; Aaron, G.J. Predictors of anemia in women of reproductive age: Biomarkers Reflecting Inflammation and Nutritional Determinants of Anemia (BRINDA) project. Am. J. Clin. Nutr. 2017, 106, 416S–427S. [Google Scholar] [CrossRef]
- Engle-Stone, R.; Aaron, G.J.; Huang, J.; Wirth, J.P.; Namaste, S.M.; Williams, A.M.; Peerson, J.M.; Rohner, F.; Varadhan, R.; Addo, O.Y.; et al. Predictors of anemia in preschool children: Biomarkers Reflecting Inflammation and Nutritional Determinants of Anemia (BRINDA) project. Am. J. Clin. Nutr. 2017, 106, 402S–415S. [Google Scholar] [CrossRef]
- Black, R.E.; Victora, C.G.; Walker, S.P.; Bhutta, Z.A.; Christian, P.; de Onis, M.; Ezzati, M.; Grantham-McGregor, S.; Katz, J.; Martorell, R.; et al. Maternal and child undernutrition and overweight in low-income and middle-income countries. Lancet 2013, 382, 427–451. [Google Scholar] [CrossRef]
- Haider, B.A.; Olofin, I.; Wang, M.; Spiegelman, D.; Ezzati, M.; Fawzi, W.W.; Nutrition Impact Model Study, G. Anaemia, prenatal iron use, and risk of adverse pregnancy outcomes: Systematic review and meta-analysis. BMJ 2013, 346, f3443. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Young, M.F.; Oaks, B.M.; Tandon, S.; Martorell, R.; Dewey, K.G.; Wendt, A.S. Maternal hemoglobin concentrations across pregnancy and maternal and child health: A systematic review and meta-analysis. Ann. N. Y. Acad. Sci. 2019, 1450, 47–68. [Google Scholar] [CrossRef] [Green Version]
- Alderman, H.; Horton, S. The economics of addressing nutritional anemia. In Nutritional Anemia; Kraemer, K., Zimmermann, M.B., Eds.; Sight and Life Press: Basil, Switzerland, 2007. [Google Scholar]
- Stevens, G.A.; Finucane, M.M.; De-Regil, L.M.; Paciorek, C.J.; Flaxman, S.R.; Branca, F.; Pena-Rosas, J.P.; Bhutta, Z.A.; Ezzati, M.; Nutrition Impact Model Study, G. Global, regional, and national trends in haemoglobin concentration and prevalence of total and severe anaemia in children and pregnant and non-pregnant women for 1995-2011: A systematic analysis of population-representative data. Lancet Glob. Health 2013, 1, e16–e25. [Google Scholar] [CrossRef] [Green Version]
- WHO. The Global Health Observatory. Available online: https://www.who.int/data/gho/data/indicators/indicator-details/GHO/prevalence-of-anaemia-in-women-of-reproductive-age-(-) (accessed on 18 February 2021).
- Wells, G.A.; Shea, B.; O’Connell, D.; Peterson, J.; Welch, V.; Losos, M.; Tugwell, P. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomised Studies in Meta-Analyses; Ottawa Hospital Research Institute: Ottawa, ON, Canada, 2000. [Google Scholar]
- Hossain, M.; Choudhury, N.; Adib Binte Abdullah, K.; Mondal, P.; Jackson, A.A.; Walson, J.; Ahmed, T. Evidence-based approaches to childhood stunting in low and middle income countries: A systematic review. Arch. Dis. Child. 2017, 102, 903–909. [Google Scholar] [CrossRef]
- Akseer, N.; Vaivada, T.; Rothschild, O.; Ho, K.; Bhutta, Z.A. Understanding multifactorial drivers of child stunting reduction in Exemplar countries: A mixed-methods approach. Am. J. Clin. Nutr. 2020, 112, 792S–805S. [Google Scholar] [CrossRef]
- Ara, G.; Khanam, M.; Rahman, A.S.; Islam, Z.; Farhad, S.; Sanin, K.I.; Khan, S.S.; Rahman, M.M.; Majoor, H.; Ahmed, T. Effectiveness of micronutrient-fortified rice consumption on anaemia and zinc status among vulnerable women in Bangladesh. PLoS ONE 2019, 14, e0210501. [Google Scholar] [CrossRef] [PubMed]
- Barkley, J.S.; Wheeler, K.S.; Pachon, H. Anaemia prevalence may be reduced among countries that fortify flour. Br. J. Nutr. 2015, 114, 265–273. [Google Scholar] [CrossRef] [Green Version]
- Casey, G.J.; Tinh, T.T.; Tien, N.T.; Hanieh, S.; Cavalli-Sforza, L.T.; Montresor, A.; Biggs, B.A. Sustained effectiveness of weekly iron-folic acid supplementation and regular deworming over 6 years in women in rural Vietnam. PLoS Negl. Trop. Dis. 2017, 11, e0005446. [Google Scholar] [CrossRef] [Green Version]
- Chakrabarti, S.; George, N.; Majumder, M.; Raykar, N.; Scott, S. Identifying sociodemographic, programmatic and dietary drivers of anaemia reduction in pregnant Indian women over 10 years. Public Health Nutr. 2018, 21, 2424–2433. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chakrabarti, S.; Kishore, A.; Raghunathan, K.; Scott, S.P. Impact of subsidized fortified wheat on anaemia in pregnant Indian women. Matern. Child Nutr. 2019, 15, e12669. [Google Scholar] [CrossRef] [PubMed]
- Engle-Stone, R.; Nankap, M.; Ndjebayi, A.O.; Allen, L.H.; Shahab-Ferdows, S.; Hampel, D.; Killilea, D.W.; Gimou, M.M.; Houghton, L.A.; Friedman, A.; et al. Iron, Zinc, Folate, and Vitamin B-12 Status Increased among Women and Children in Yaounde and Douala, Cameroon, 1 Year after Introducing Fortified Wheat Flour. J. Nutr. 2017, 147, 1426–1436. [Google Scholar] [CrossRef] [PubMed]
- Feng, G.; Simpson, J.A.; Chaluluka, E.; Molyneux, M.E.; Rogerson, S.J. Decreasing burden of malaria in pregnancy in Malawian women and its relationship to use of intermittent preventive therapy or bed nets. PLoS ONE 2010, 5, e12012. [Google Scholar] [CrossRef]
- Fujimori, E.; Sato, A.P.; Szarfarc, S.C.; Veiga, G.V.; Oliveira, V.A.; Colli, C.; Moreira-Araújo, R.S.; Arruda, I.K.; Uchimura, T.T.; Brunken, G.S.; et al. Anemia in Brazilian pregnant women before and after flour fortification with iron. Rev. Saúde Pública 2011, 45, 1027–1035. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Greffeuille, V.; Sophonneary, P.; Laillou, A.; Gauthier, L.; Hong, R.; Hong, R.; Poirot, E.; Dijkhuizen, M.; Wieringa, F.; Berger, J. Inequalities in Nutrition between Cambodian Women over the Last 15 Years (2000–2014). Nutrients 2016, 8, 224. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Heckert, J.; Headey, D.D.; Ndiaye, B.; Brero, M.; Assey, V. Analysis of the Drivers of Change in Women’s Anemia in Tanzania 2005–2015; International Food Policy Research Institute (IFPRI): Washington, DC, USA, 2019. [Google Scholar]
- India State-Level Disease Burden Initiative Malnutrition Collaborators. The burden of child and maternal malnutrition and trends in its indicators in the states of India: The Global Burden of Disease Study 1990–2017. Lancet Child Adolesc. Health 2019, 3, 855–870. [Google Scholar] [CrossRef] [Green Version]
- Kalimbira, A.A.; MacDonald, C.; Simpson, J.R. The impact of an integrated community-based micronutrient and health programme on anaemia in non-pregnant Malawian women. Public Health Nutr. 2010, 13, 1445–1452. [Google Scholar] [CrossRef] [Green Version]
- Lakew, Y.; Biadgilign, S.; Haile, D. Anaemia prevalence and associated factors among lactating mothers in Ethiopia: Evidence from the 2005 and 2011 demographic and health surveys. BMJ Open 2015, 5, e006001. [Google Scholar] [CrossRef] [Green Version]
- Martorell, R.; Ascencio, M.; Tacsan, L.; Alfaro, T.; Young, M.F.; Addo, O.Y.; Dary, O.; Flores-Ayala, R. Effectiveness evaluation of the food fortification program of Costa Rica: Impact on anemia prevalence and hemoglobin concentrations in women and children. Am. J. Clin. Nutr. 2015, 101, 210–217. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nguyen, P.H.; Scott, S.; Avula, R.; Tran, L.M.; Menon, P. Trends and drivers of change in the prevalence of anaemia among 1 million women and children in India, 2006 to 2016. BMJ Glob. Health 2018, 3, e001010. [Google Scholar] [CrossRef] [Green Version]
- Schultz, J.T.; Vatucawaqa, P.T. Impact of Iron Fortified Flour in Child. Bearing Age (CBA) Women in Fiji: 2010 Report; National Food and Nutrition Centre: Suva, Fiji, 2012. [Google Scholar]
- Talukder, A.; Osei, A.K.; Haselow, N.J.; Kroeun, H.; Uddin, A.; Quinn, V. Contribution of homestead food production to improved household food security and nutrition status—Lessons learned from Bangladesh, Cambodia, Nepal and the Philippines. In Improving Diets and Nutrition: Food-Based Approaches; Thompson, B., Amoroso, L., Eds.; Institut Veolia: Aubervilliers, France, 2014. [Google Scholar]
- Wirth, J.; Woodruff, B.A.; Mamady, D.; Beauliere, J.M.; Ayoya, M.; Rohner, F.; Teta, I. Nutrition trends in the past fifteen years in Guinea: Secondary analysis of cross-sectional data on children, adolescent girls and women. Afr. J. Food Agric. Nutr. Dev. 2019, 19, 14889–14915. [Google Scholar] [CrossRef]
- Bellizzi, S.; Pichierri, G.; Panu Napodano, C.M.; Salaris, P.; Fiamma, M.; Fozza, C.; Cegolon, L. Iron deficiency anaemia and low BMI among adolescent girls in India: The transition from 2005 to 2015. Public Health Nutr. 2020, 24, 1577–1582. [Google Scholar] [CrossRef] [PubMed]
- Gona, P.N.; Gona, C.M.; Chikwasha, V.; Haruzivishe, C.; Mapoma, C.C.; Rao, S.R. Intersection of HIV and Anemia in women of reproductive age: A 10-year analysis of three Zimbabwe demographic health surveys, 2005–2015. BMC Public Health 2021, 21, 41. [Google Scholar] [CrossRef] [PubMed]
- Iruhiriye, E.; Olney, D.K.; Ramani, G.V.; Heckert, J.; Niyongira, E.; Frongillo, E.A. Stories of Change—Rwanda, Final Report; International Food Policy Research Institute (IFPRI): Washington, DC, USA, 2019. [Google Scholar]
- Glasier, A.F.; Smith, K.B.; van der Spuy, Z.M.; Ho, P.C.; Cheng, L.; Dada, K.; Wellings, K.; Baird, D.T. Amenorrhea associated with contraception-an international study on acceptability. Contraception 2003, 67, 1–8. [Google Scholar] [CrossRef]
- Bellizzi, S.; Ali, M.M. Effect of oral contraception on anemia in 12 low and middle-income countries. Contraception 2018, 97, 236–242. [Google Scholar] [CrossRef] [PubMed]
- Rai, A.; Khan, M.N.; Thapa, S. Trends and determinants of anaemia in women of Nepal: A multilevel analysis. Matern. Child Nutr. 2020, 16, e13044. [Google Scholar] [CrossRef]
- DeFries, R.; Chhatre, A.; Davis, K.F.; Dutta, A.; Fanzo, J.; Ghosh-Jerath, S.; Myers, S.; Rao, N.D.; Smith, M.R. Impact of Historical Changes in Coarse Cereals Consumption in India on Micronutrient Intake and Anemia Prevalence. Food Nutr. Bull. 2018, 39, 377–392. [Google Scholar] [CrossRef] [PubMed]
- Pei, L.; Ren, L.; Wang, D.; Yan, H. Assessment of maternal anemia in rural Western China between 2001 and 2005: A two-level logistic regression approach. BMC Public Health 2013, 13, 366. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Qin, M.; Falkingham, J.; Padmadas, S.S. Unpacking the Differential Impact of Family Planning Policies in China: Analysis of Parity Progression Ratios from Retrospective Birth History Data, 1971-2005. J. Biosoc. Sci. 2018, 50, 800–822. [Google Scholar] [CrossRef] [Green Version]
- Kumar, S.; Sharma, A.; Sood, A.; Kumar, S. Urban Health in India: Policies, Practices and Current Challenges. J. Health Manag. 2016, 18, 489–498. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Nguyen et al. [33] | Heckert et al. [28] | Iruhiriye et al. [39] | |||
|---|---|---|---|---|---|
| Causes | Category | Determinant/Indicator | India (2006–2016) | Tanzania (2005–2010) | Rwanda (2005–2010) |
| Proximal | Healthcare Utilization | ANC | 7% * | ||
| IFA consumption | 7% * | ||||
| Deworming | 7% * | ||||
| Contraceptive use | 30% | 43% | |||
| Change in fertility | 8% | ||||
| Nutrition counseling | 7% * | ||||
| Dietary intake | Dietary diversity | 1% | |||
| Maternal characteristics | Age | 2% | |||
| Birth spacing | 6% | ||||
| Infection burden | 14% | 46% ¥ | |||
| Intermediate | Socioeconomic factors | Household wealth | 17% | 36% ** | 7% |
| Improved sanitation | 9% | 12% | 3% | ||
| Maternal education | 24% | 36% ** |
| Region | Country | Author, Year | Time Period | Determinants Associated with Decrease in Maternal Anemia |
|---|---|---|---|---|
| Nationally representative studies | ||||
| East Asia and Pacific | Cambodia | Greffeuille, 2016 | 2000 to 2014 | SOCIOECONOMIC FACTORS: Household wealth, urban residence and maternal education |
| Latin America and Caribbean | Costa Rica | Martorell, 2015 | 1996 to 2008–09 | DIETARY INTAKE: National flour fortification program |
| South Asia | India | Bellizzi, 2020 | 2005 to 2015 | MATERNAL CHARACTERISTICS: Age at pregnancy > 20 years |
| India | Chakrabarti, 2018 | 2002–04 to 2012–13 | MATERNAL CHARACTERISTICS: Age DIETARY INTAKE: Dietary diversity SOCIOECONOMIC FACTORS: Urbanization, maternal education HEALTHY HOUSEHOLD: Decrease in open defecation | |
| India | Swaminathan, 2019 | 2010–2017 ¥ | SOCIOECONOMIC FACTORS: Socio-demographic index * Low SDI states: −0.98% (−1.35 to −0.60) Middle SDI states: −0.61% (−0.97 to −0.22) High SDI states: −0.21% (−0.60 to 0.25) | |
| Sub-Saharan Africa | Zimbabwe | Gona, 2021 | 2005 to 2015 | MATERNAL CHARACTERISTICS: Age < 40, BMI > 30, not pregnant/lactating, HIV negative HEALTH SERVICES UTILIZATION: IFA in pregnancy SOCIOECONOMIC FACTORS: Urban residence |
| Ethiopia | Lakew, 2015 | 2005 to 2011 | MATERNAL CHARACTERISTICS: BMI > 18.5, breastfeeding for 2 years HEALTH SERVICES UTILIZATION: 4+ ANC, contraceptive use SOCIOECONOMIC FACTORS: Household wealth, maternal education and occupation | |
| Guinea | Wirth, 2019 | 2005 to 2012 | MATERNAL CHARACTERISTICS: Maternal age 20–29 years, and > normal BMI SOCIOECONOMIC FACTORS: Household wealth, urban residence | |
| Multi-region | Multi-country | Barkley, 2015 | Various | DIETARY INTAKE: National flour fortification programs |
| Subnational/Regional studies | ||||
| East Asia and Pacific | Fiji | Shultz, 2012 | 2004 to 2010 | DIETARY INTAKE: National flour fortification program |
| Viet Nam | Casey, 2017 | 2005 to 2012 | HEALTH SERVICES UTILIZATION: Weekly IFA and regular deworming program | |
| Latin America and Caribbean | Brazil | Fujimori, 2011 | 2002 to 2008 | MATERNAL CHARACTERISTICS: Parity, normal and higher BMI DIETARY INTAKE: National flour fortification program SOCIOECONOMIC FACTORS: Marital status |
| South Asia | Bangladesh | Ara, 2019 | 2014–15 to 2016–17 | MATERNAL CHARACTERISTICS: Maternal age > 35, self-reported history of heavy menstrual flow DIETARY INTAKE: Fortified rice consumption SOCIOECONOMIC FACTORS: Urban residence |
| India | Chakrabarti, 2019 | 2002-04 to 2012-13 | DIETARY INTAKE: State-level flour fortification program | |
| Sub-Saharan Africa | Cameroon | Engle-Stone, 2017 | 2009 to 2012 | DIETARY INTAKE: Large-scale wheat flour fortification |
| Malawi | Feng, 2010 | 1997 to 2006 | HEALTH SERVICES UTILIZATION: Malaria prevention (IPTp and bed-net use) during pregnancy | |
| Malawi | Kalimbira, 2010 | 2000 to 2004 | Micronutrient and health (MICAH) program, incl. DIETARY INTAKE: Flour fortification, weekly IFA, dietary diversification HEALTH SERVICES UTILIZATION: Malaria prevention and regular deworming HEALTHY HOUSEHOLD: Improved WaSH | |
| Multi-region | Bangladesh and Cambodia | Talukder, 2014 | BD: 2003 to 2006 Cam: 2005 to 2007 | DIETARY INTAKE: Homestead food production program (dietary diversity) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Owais, A.; Merritt, C.; Lee, C.; Bhutta, Z.A. Anemia among Women of Reproductive Age: An Overview of Global Burden, Trends, Determinants, and Drivers of Progress in Low- and Middle-Income Countries. Nutrients 2021, 13, 2745. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13082745
Owais A, Merritt C, Lee C, Bhutta ZA. Anemia among Women of Reproductive Age: An Overview of Global Burden, Trends, Determinants, and Drivers of Progress in Low- and Middle-Income Countries. Nutrients. 2021; 13(8):2745. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13082745
Chicago/Turabian StyleOwais, Aatekah, Catherine Merritt, Christopher Lee, and Zulfiqar A. Bhutta. 2021. "Anemia among Women of Reproductive Age: An Overview of Global Burden, Trends, Determinants, and Drivers of Progress in Low- and Middle-Income Countries" Nutrients 13, no. 8: 2745. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13082745