
Effects of Lactobacillus plantarum PS128 on Depressive Symptoms and Sleep Quality in Self-Reported Insomniacs: A Randomized, Double-Blind, Placebo-Controlled Pilot Trial



Abstract
:1. Introduction
2. Materials and Methods
2.1. Experiment Design
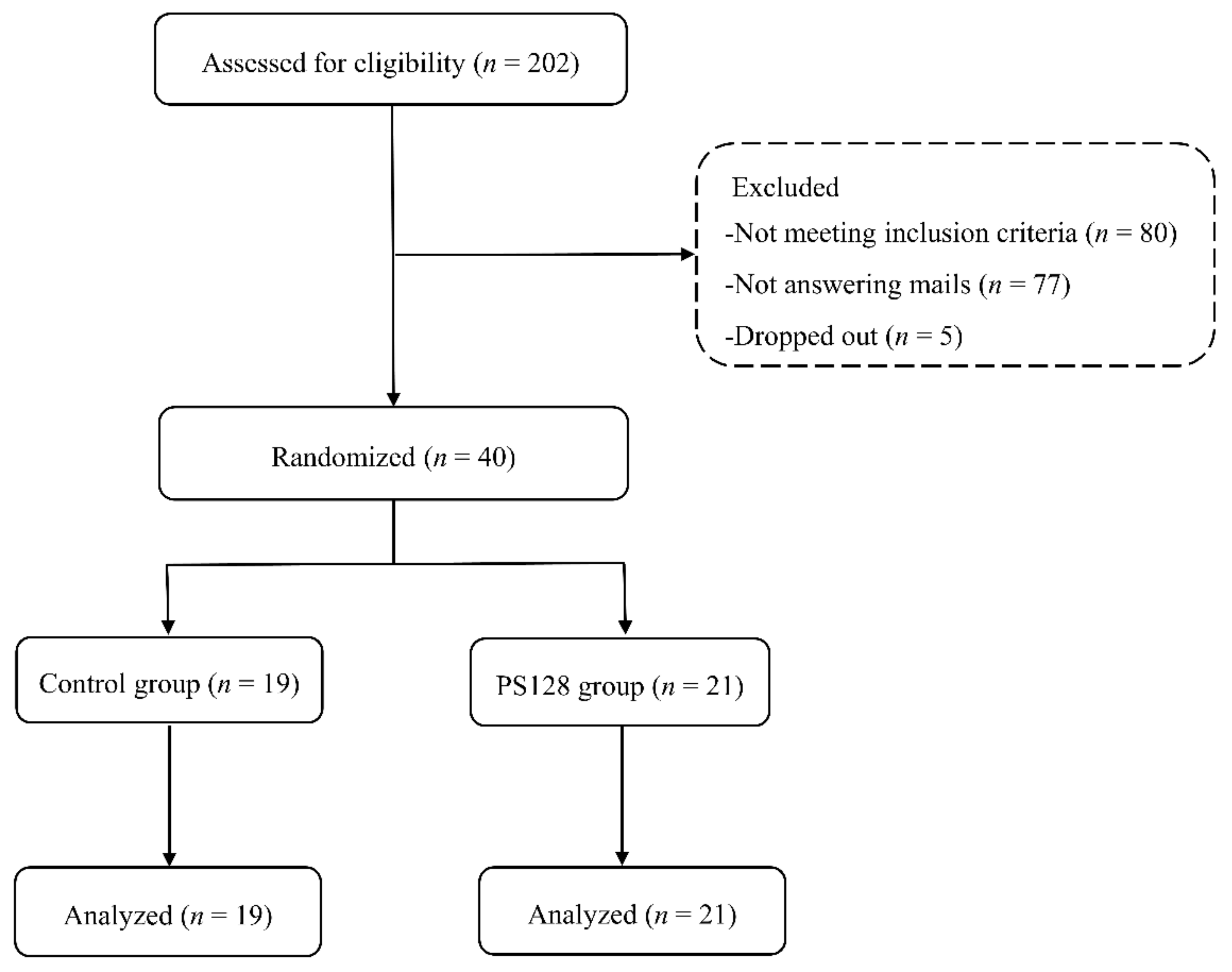
2.2. Participants
2.3. Test Capsules
2.4. Measurement and Analysis of Miniature-PSG
2.5. EEG Power Spectral Analysis
2.6. Heart Rate Variability (HRV) Analysis
2.7. Statistical Analysis
3. Results
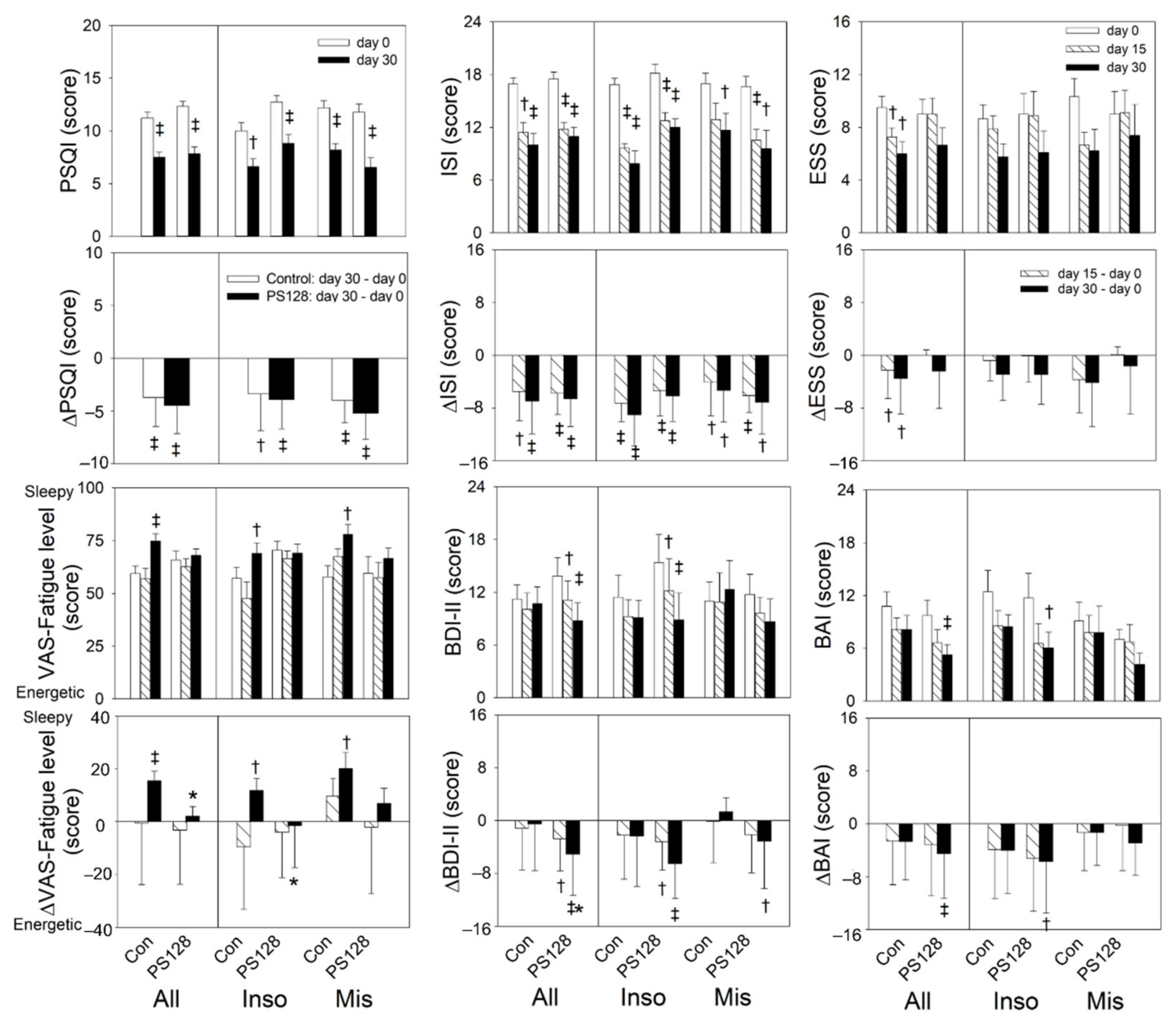
3.1. Effects of PS128 on Subjective Parameters
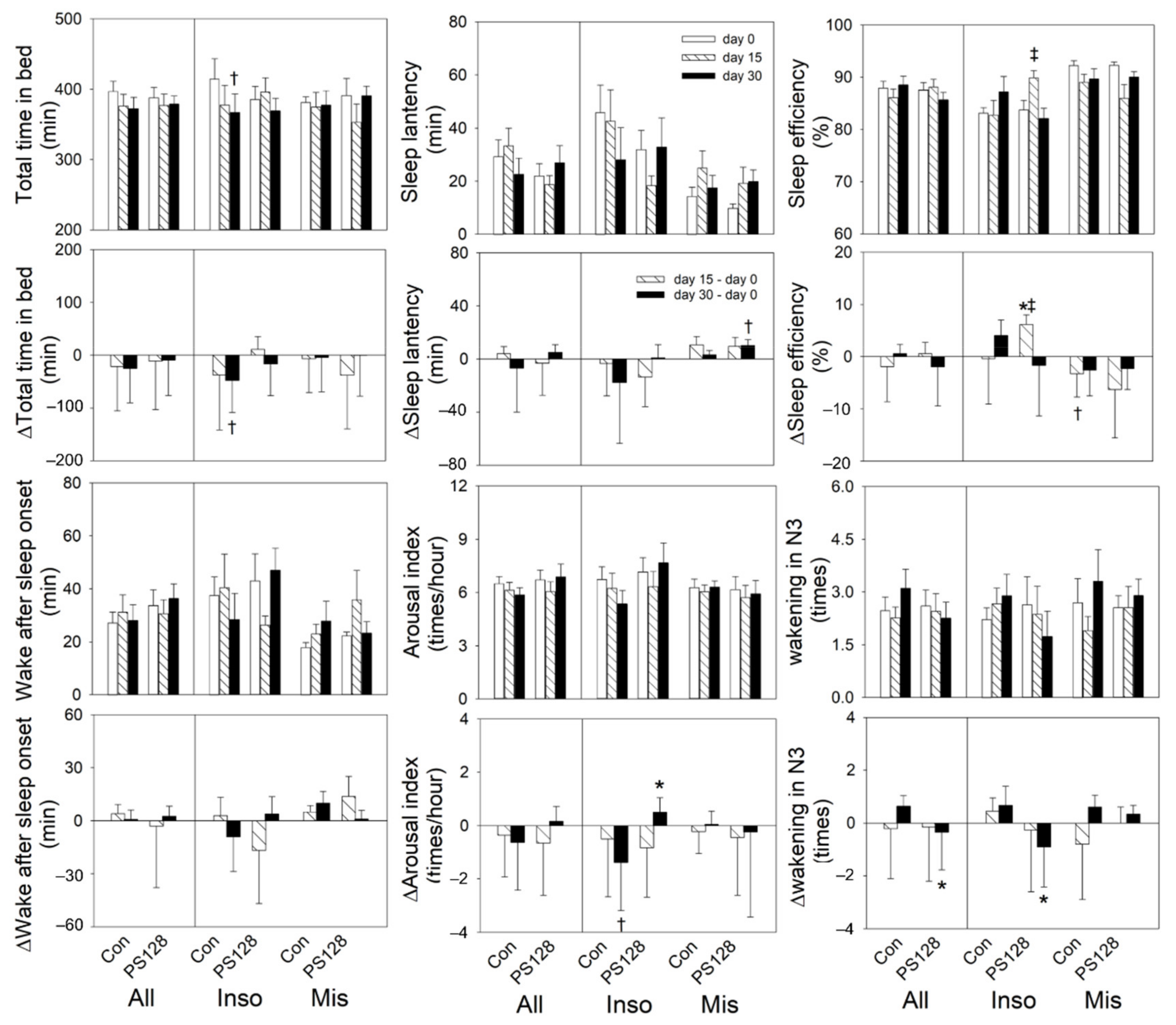
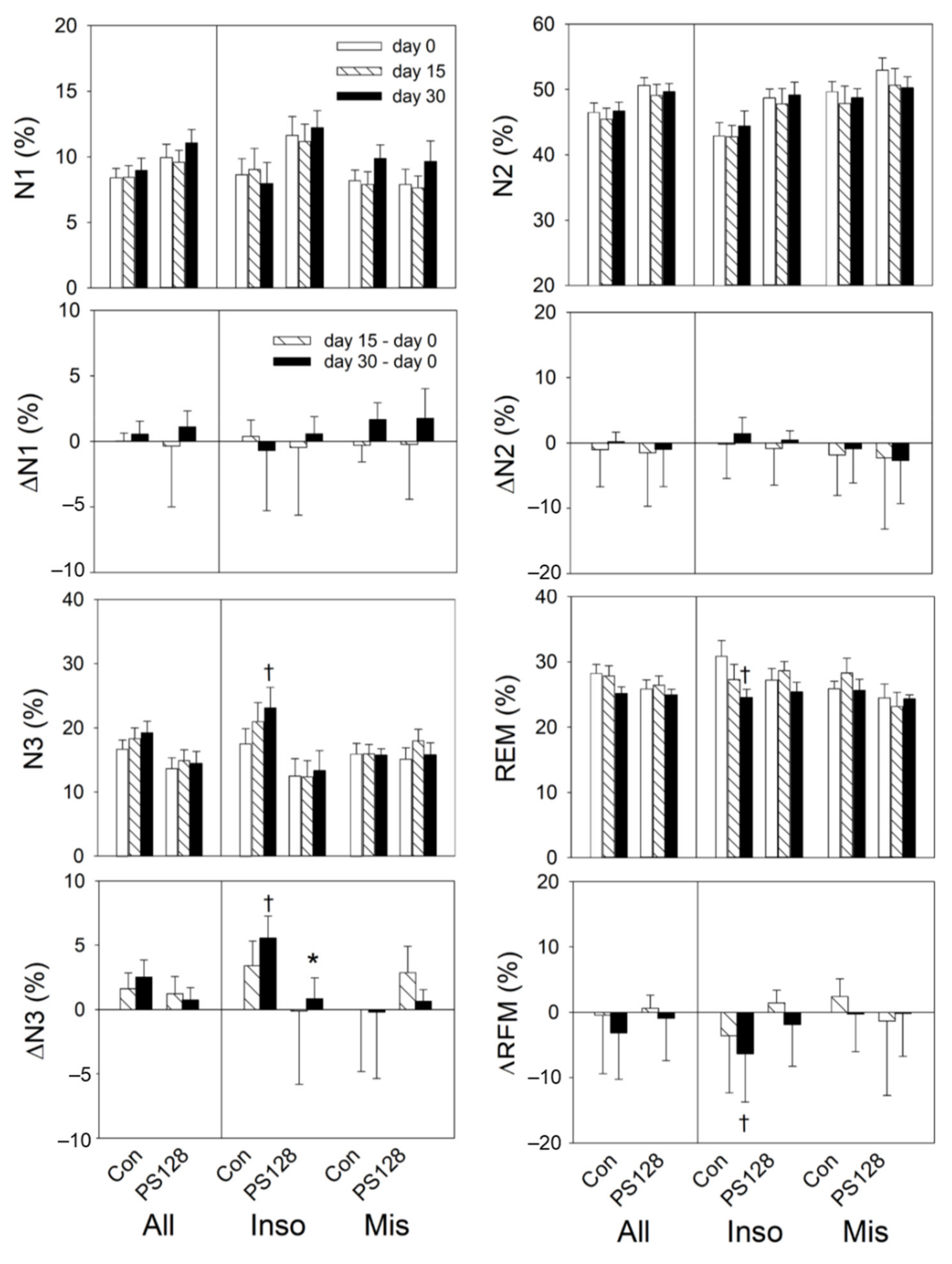
3.2. Effects of PS128 on Sleep EEG
3.3. Effects of PS128 on HRV
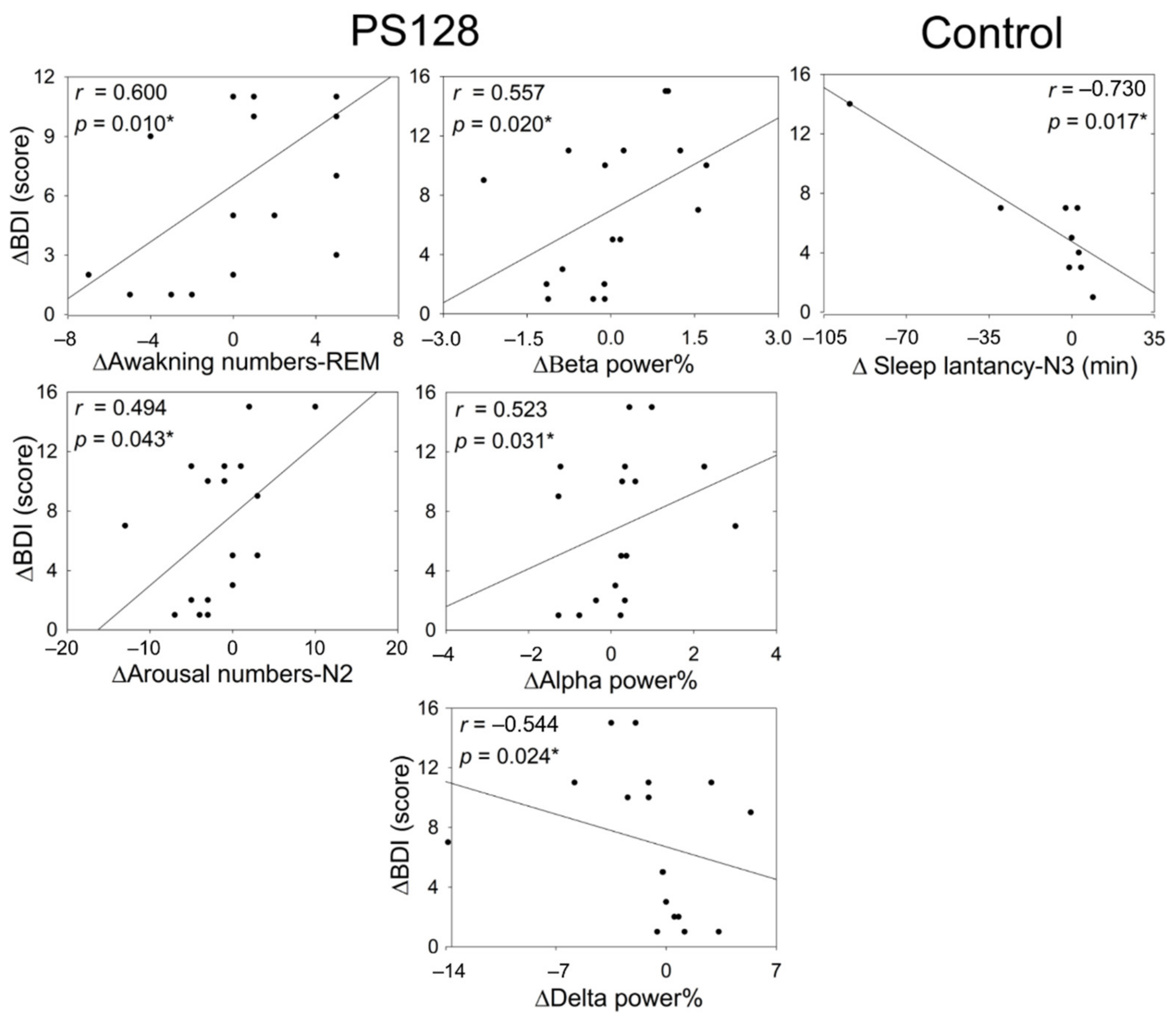
3.4. Correlation between Changes in Objective Parameters and BDI-II Scores
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lin, L.; Zhang, J. Role of intestinal microbiota and metabolites on gut homeostasis and human diseases. BMC Immunol. 2017, 18, 2. [Google Scholar] [CrossRef] [Green Version]
- Bastiaanssen, T.F.S.; Cussotto, S.; Claesson, M.J.; Clarke, G.; Dinan, T.G.; Cryan, J.F. Gutted! Unraveling the Role of the Microbiome in Major Depressive Disorder. Harv. Rev. Psychiatry 2020, 28, 26–39. [Google Scholar] [CrossRef] [PubMed]
- Sampson, T.R.; Debelius, J.W.; Thron, T.; Janssen, S.; Shastri, G.G.; Ilhan, Z.E.; Challis, C.; Schretter, C.E.; Rocha, S.; Gradinaru, V.; et al. Gut Microbiota Regulate Motor Deficits and Neuroinflammation in a Model of Parkinson’s Disease. Cell 2016, 167, 1469–1480. [Google Scholar] [CrossRef] [Green Version]
- Łuc, M.; Misiak, B.; Pawłowski, M.; Stańczykiewicz, B.; Zabłocka, A.; Szcześniak, D.; Pałęga, A.; Rymaszewska, J. Gut microbiota in dementia. Critical review of novel findings and their potential application. Prog. Neuro-Psychopharmacol. Biol. Psychiatry 2021, 104, 110039. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Hao, Y.; Fan, F.; Zhang, B. The Role of Microbiome in Insomnia, Circadian Disturbance and Depression. Front. Psychiatry 2018, 9, 669. [Google Scholar] [CrossRef] [Green Version]
- FAO; WHO. Joint, FAO/WHO Working Group Report on Drafting Guidelines for the Evaluation of Probiotics in Food. 2002. Available online: https://www.who.int/foodsafety/fs_management/en/probiotic_guidelines.pdf (accessed on 31 July 2021).
- Pennisi, E. Meet the psychobiome. Science 2020, 368, 570–573. [Google Scholar] [CrossRef] [PubMed]
- Bhaskar, S.; Hemavathy, D.; Prasad, S. Prevalence of chronic insomnia in adult patients and its correlation with medical comorbidities. J. Fam. Med. Prim. Care 2016, 5, 780–784. [Google Scholar] [CrossRef] [PubMed]
- Roth, T. Insomnia: Definition, prevalence, etiology, and consequences. J. Clin. Sleep Med. 2007, 3, S7–S10. [Google Scholar] [CrossRef] [Green Version]
- American Psychological Association. Depression. Available online: https://www.apa.org/topics/depression/ (accessed on 31 July 2021).
- American Psychological Association. Anxiety. Available online: http://www.apa.org/topics/anxiety/ (accessed on 31 July 2021).
- Seow, L.S.E.; Verma, S.K.; Mok, Y.M.; Kumar, S.; Chang, S.; Satghare, P.; Hombali, A.; Vaingankar, J.; Chong, S.A.; Subramaniam, M. Evaluating DSM-5 Insomnia Disorder and the Treatment of Sleep Problems in a Psychiatric Population. J. Clin. Sleep Med. 2018, 14, 237–244. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Devi, C.B.P.; Samreen, S.; Vaishnavi, B.; Navitha, D.; Kumari, N.K.; Sharma, J.V.C.; Sirisha, P. A review on insomnia: The sleep disorder. Pharma Innov. J. 2018, 7, 227–230. [Google Scholar]
- Van Lier, H.; Drinkenburg, W.H.; Van Eeten, Y.J.; Coenen, A.M. Effects of diazepam and zolpidem on EEG beta frequencies are behavior-specific in rats. Neuropharmacology 2004, 47, 163–174. [Google Scholar] [CrossRef]
- Qaseem, A.; Kansagara, D.; Forciea, M.A.; Cooke, M.; Denberg, T.D. Management of Chronic Insomnia Disorder in Adults: A Clinical Practice Guideline from the American College of Physicians. Ann. Intern. Med. 2016, 165, 125–133. [Google Scholar] [CrossRef]
- Koffel, E.; Bramoweth, A.D.; Ulmer, C.S. Increasing access to and utilization of cognitive behavioral therapy for insomnia (CBT-I): A narrative review. J. Gen. Intern. Med. 2018, 33, 955–962. [Google Scholar] [CrossRef] [Green Version]
- Ong, J.C.; Kuo, T.F.; Manber, R. Who is at risk for dropout from group cognitive-behavior therapy for insomnia? J. Psychosom. Res. 2008, 64, 419–425. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Riemann, D.; Spiegelhalder, K.; Feige, B.; Voderholzer, U.; Berger, M.; Perlis, M.; Nissen, C. The hyperarousal model of insomnia: A review of the concept and its evidence. Sleep Med. Rev. 2010, 14, 19–31. [Google Scholar] [CrossRef]
- Vgontzas, A.N.; Chrousos, G.P. Sleep, the Hypothalamic-Pituitary-Adrenal Axis, and Cytokines: Multiple Interactions and Disturbances in Sleep Disorders. Endocrinol. Metab. Clin. 2002, 31, 15–36. [Google Scholar] [CrossRef]
- Bonnet, M.H.; Arand, D.L. Hyperarousal and insomnia: State of the science. Sleep Med. Rev. 2010, 14, 9–15. [Google Scholar] [CrossRef]
- Ramos, R.W.; Arvelo, A.D.A.; Gomez, J.P. Hyperarousal in insomnia. Sleep Med. 2013, 14, e240–e241. [Google Scholar] [CrossRef]
- Brown, R.E.; Basheer, R.; McKenna, J.T.; Strecker, R.E.; McCarley, R.W. Control of sleep and wakefulness. Physiol. Rev. 2012, 92, 1087–1187. [Google Scholar] [CrossRef] [Green Version]
- Benedict, C.; Vogel, H.; Jonas, W.; Woting, A.; Blaut, M.; Schürmann, A.; Cedernaes, J. Gut microbiota and glucometabolic alterations in response to recurrent partial sleep deprivation in normal-weight young individuals. Mol. Metab. 2016, 5, 1175–1186. [Google Scholar] [CrossRef]
- Reynolds, A.C.; Paterson, J.L.; Ferguson, S.A.; Stanley, D.; Wright, K.P., Jr.; Dawson, D. The shift work and health research agenda: Considering changes in gut microbiota as a pathway linking shift work, sleep loss and circadian misalignment, and metabolic disease. Sleep Med. Rev. 2017, 34, 3–9. [Google Scholar] [CrossRef]
- Summa, K.C.; Voigt, R.M.; Forsyth, C.B.; Shaikh, M.; Cavanaugh, K.; Tang, Y.; Vitaterna, M.H.; Song, S.; Turek, F.W.; Keshavarzian, A. Disruption of the Circadian Clock in Mice Increases Intestinal Permeability and Promotes Alcohol-Induced Hepatic Pathology and Inflammation. PLoS ONE 2013, 8, e67102. [Google Scholar] [CrossRef] [Green Version]
- Savignac, H.M.; Kiely, B.; Dinan, T.G.; Cryan, J.F. Bifidobacteria exert strain-specific effects on stress-related behavior and physiology in BALB/c mice. Neurogastroenterol. Motil. 2014, 26, 1615–1627. [Google Scholar] [CrossRef]
- Nishida, K.; Sawada, D.; Kawai, T.; Kuwano, Y.; Fujiwara, S.; Rokutan, K. Para-psychobiotic Lactobacillus gasseri CP2305 ameliorates stress-related symptoms and sleep quality. J. Appl. Microbiol. 2017, 123, 1561–1570. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Takada, M.; Nishida, K.; Gondo, Y.; Kikuchi-Hayakawa, H.; Ishikawa, H.; Suda, K.; Kawai, M.; Hoshi, R.; Kuwano, Y.; Miyazaki, K.; et al. Beneficial effects of Lactobacillus casei strain Shirota on academic stress-induced sleep disturbance in healthy adults: A double-blind, randomised, placebo-controlled trial. Benef. Microbes 2017, 8, 153–162. [Google Scholar] [CrossRef] [PubMed]
- Saito, H.; Cherasse, Y.; Suzuki, R.; Mitarai, M.; Ueda, F.; Urade, Y. Zinc-rich oysters as well as zinc-yeast- and astaxanthin-enriched food improved sleep efficiency and sleep onset in a randomized controlled trial of healthy individuals. Mol. Nutr. Food Res. 2017, 61, 1600882. [Google Scholar] [CrossRef]
- Liu, W.-H.; Yang, C.-H.; Lin, C.-T.; Li, S.-W.; Cheng, W.-S.; Jiang, Y.-P.; Wu, C.-C.; Chang, C.-H.; Tsai, Y.-C. Genome architecture of Lactobacillus plantarum PS128, a probiotic strain with potential immunomodulatory activity. Gut Pathog. 2015, 7, 22. [Google Scholar] [CrossRef] [Green Version]
- Liu, W.-H.; Chuang, H.-L.; Huang, Y.-T.; Wu, C.-C.; Chou, G.-T.; Wang, S.; Tsai, Y.-C. Alteration of behavior and monoamine levels attributable to Lactobacillus plantarum PS128 in germ-free mice. Behav. Brain Res. 2016, 298, 202–209. [Google Scholar] [CrossRef]
- Liu, Y.-W.; Liu, W.-H.; Wu, C.-C.; Juan, Y.-C.; Wu, Y.-C.; Tsai, H.-P.; Wang, S.; Tsai, Y.-C. Psychotropic effects of Lactobacillus plantarum PS128 in early life-stressed and naïve adult mice. Brain Res. 2016, 1631, 1–12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, K.A.; Hicks, G.; Nino-Murcia, G. Validity and reliability of a scale to assess fatigue. Psychiatry Res. 1991, 36, 291–298. [Google Scholar] [CrossRef]
- Buysse, D.J.; Reynolds, C.F., III; Monk, T.H.; Berman, S.R.; Kupfer, D.J. The Pittsburgh Sleep Quality Index: A new instrument for psychiatric practice and research. Psychiatry Res. 1989, 28, 193–213. [Google Scholar] [CrossRef]
- Morin, C.M.; Belleville, G.; Bélanger, L.; Ivers, H. The Insomnia Severity Index: Psychometric indicators to detect insomnia cases and evaluate treatment response. Sleep 2011, 34, 601–608. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Johns, M.W. Reliability and factor analysis of the Epworth Sleepiness Scale. Sleep 1992, 15, 376–381. [Google Scholar] [CrossRef] [Green Version]
- Beck, A.T.; Steer, R.A.; Brown, G.K. Beck depression inventory-II. Psychol. Corp. 1996, 78, 490–498. [Google Scholar]
- Beck, A.T.; Epstein, N.; Brown, G.; Steer, R.A. An inventory for measuring clinical anxiety: Psychometric properties. J. Consult. Clin. Psychol. 1988, 56, 893. [Google Scholar] [CrossRef] [PubMed]
- Horne, J.A.; Östberg, O. A self-assessment questionnaire to determine morningness-eveningness in human circadian rhythms. Int. J. Chronobiol. 1976, 4, 97–110. [Google Scholar]
- Tsai, H.-J.; Kuo, T.B.; Lin, Y.-C.; Yang, C.C. The association between prolonged sleep onset latency and heart rate dynamics among young sleep-onset insomniacs and good sleepers. Psychiatry Res. 2015, 230, 892–898. [Google Scholar] [CrossRef]
- Tsai, H.; Kuo, T.B.; Lee, G.S.; Yang, C.C. Efficacy of paced breathing for insomnia: Enhances vagal activity and improves sleep quality. Psychophysiology 2015, 52, 388–396. [Google Scholar] [CrossRef]
- Tsai, H.-J.; Kuo, T.B.; Kuo, K.-L.; Yang, C.C. Failure to de-arouse during sleep-onset transitions in the heart rates of individuals with sleep-onset insomnia. J. Psychosom. Res. 2019, 126, 109809. [Google Scholar] [CrossRef] [PubMed]
- Kuo, T.B.J.; Chen, C.Y.; Hsu, Y.-C.; Yang, C.C.H. Performance of the frequency domain indices with respect to sleep staging. Clin. Neurophysiol. 2012, 123, 1338–1345. [Google Scholar] [CrossRef]
- Kuo, T.B.; Yang, C.C. Frequency domain analysis of electrooculogram and its correlation with cardiac sympathetic function. Exp. Neurol. 2009, 217, 38–45. [Google Scholar] [CrossRef]
- Malik, M.; Bigger, J.T.; Camm, A.J.; Kleiger, R.E.; Malliani, A.; Moss, A.J.; Schwartz, P.J. Heart rate variability: Standards of measurement, physiological interpretation, and clinical use. Eur. Heart J. 1996, 17, 354–381. [Google Scholar] [CrossRef] [Green Version]
- Armitage, R.; Emslie, G.J.; Hoffmann, R.F.; Rintelmann, J.; Rush, A.J. Delta sleep EEG in depressed adolescent females and healthy controls. J. Affect. Disord. 2001, 63, 139–148. [Google Scholar] [CrossRef]
- Liu, Y.-W.; Liong, M.T.; Chung, Y.-C.E.; Huang, H.-Y.; Peng, W.-S.; Cheng, Y.-F.; Lin, Y.-S.; Wu, Y.-Y.; Tsai, Y.-C. Effects of Lactobacillus plantarum PS128 on children with autism spectrum disorder in Taiwan: A randomized, double-blind, placebo-controlled trial. Nutrients 2019, 11, 820. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mensi, M.M.; Rogantini, C.; Marchesi, M.; Borgatti, R.; Chiappedi, M. Lactobacillus plantarum PS128 and Other Probiotics in Children and Adolescents with Autism Spectrum Disorder: A Real-World Experience. Nutrients 2021, 13, 2036. [Google Scholar] [CrossRef]
- Kong, X.-J.; Liu, J.; Liu, K.; Koh, M.; Sherman, H.; Liu, S.; Tian, R.; Sukijthamapan, P.; Wang, J.; Fong, M. Probiotic and Oxytocin Combination Therapy in Patients with Autism Spectrum Disorder: A Randomized, Double-Blinded, Placebo-Controlled Pilot Trial. Nutrients 2021, 13, 1552. [Google Scholar] [CrossRef]
- Chang, J.S.; Chiu, Y.H.; Pan, C.C.; Chen, C.H. Probiotics Lactobacillus Plantarum PS128 intervention in two patients with major depressive disorder. Taiwan J. Psychiatry 2019, 33, 116–117. [Google Scholar]
- Markou, A.; Kosten, T.R.; Koob, G.F. Neurobiological Similarities in Depression and Drug Dependence: A Self-Medication Hypothesis. Neuropsychopharmacology 1998, 18, 135–174. [Google Scholar] [CrossRef] [Green Version]
- Monti, J.M.; Jantos, H. The roles of dopamine and serotonin, and of their receptors, in regulating sleep and waking. Prog. Brain Res. 2008, 172, 625–646. [Google Scholar]
- Oikonomou, G.; Altermatt, M.; Zhang, R.-W.; Coughlin, G.M.; Montz, C.; Gradinaru, V.; Prober, D.A. The Serotonergic Raphe Promote Sleep in Zebrafish and Mice. Neuron 2019, 103, 686–701. [Google Scholar] [CrossRef] [Green Version]
- Claustrat, B.; Brun, J.; Chazot, G. The basic physiology and pathophysiology of melatonin. Sleep Med. Rev. 2005, 9, 11–24. [Google Scholar] [CrossRef]
- Monti, J.M.; Monti, D. The involvement of dopamine in the modulation of sleep and waking. Sleep Med. Rev. 2007, 11, 113–133. [Google Scholar] [CrossRef]
- Huang, W.C.; Wei, C.C.; Huang, C.C.; Chen, W.L.; Huang, H.Y. The Beneficial Effects of Lactobacillus plantarum PS128 on High-Intensity, Exercise-Induced Oxidative Stress, Inflammation, and Performance in Triathletes. Nutrients 2019, 11, 353. [Google Scholar] [CrossRef] [Green Version]
- Nishida, M.; Pearsall, J.; Buckner, R.L.; Walker, M.P. REM sleep, prefrontal theta, and the consolidation of human emotional memory. Cereb. Cortex 2009, 19, 1158–1166. [Google Scholar] [CrossRef] [Green Version]
- Hutchison, I.C.; Rathore, S. The role of REM sleep theta activity in emotional memory. Front. Psychol. 2015, 6, 1439. [Google Scholar] [CrossRef] [Green Version]
- Benton, D.; Williams, C.; Brown, A. Impact of consuming a milk drink containing a probiotic on mood and cognition. Eur. J. Clin. Nutr. 2007, 61, 355–361. [Google Scholar] [CrossRef] [Green Version]
- Tillisch, K.; Labus, J.; Kilpatrick, L.; Jiang, Z.; Stains, J.; Ebrat, B.; Guyonnet, D.; Legrain-Raspaud, S.; Trotin, B.; Naliboff, B.; et al. Consumption of fermented milk product with probiotic modulates brain activity. Gastroenterology 2013, 144, 1394–1401. [Google Scholar] [CrossRef] [Green Version]
- Omachi, T.A. Measuring sleep in rheumatologic diseases: The ESS, FOSQ, ISI, and PSQI. Arthritis Care Res. 2011, 63, S287. [Google Scholar] [CrossRef] [Green Version]
- Paulhus, D.L.; Vazire, S. The self-report method. In Handbook of Research Methods in Personality Psychology; Robins, R.W., Fraley, R.C., Krueger, R.F., Eds.; Guilford Press: New York, NY, USA, 2007; pp. 224–239. [Google Scholar]
- Buysse, D.J.; Hall, M.L.; Strollo, P.J.; Kamarck, T.W.; Owens, J.; Lee, L.; Reis, S.E.; Matthews, K.A. Relationships between the Pittsburgh Sleep Quality Index (PSQI), Epworth Sleepiness Scale (ESS), and clinical/polysomnographic measures in a community sample. J. Clin. Sleep Med. 2008, 4, 563–571. [Google Scholar] [CrossRef] [Green Version]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Control (n = 19) | PS128 (n = 21) | p Value * | |||||||
|---|---|---|---|---|---|---|---|---|---|
| All | Inso | Mis | All | Inso | Mis | All | Inso | Mis | |
| Male/female | 8/11 | 2/7 | 6/4 | 5/16 | 2/10 | 3/6 | |||
| Age (year) | 25.47 ± 4.64 | 25.11 ± 5.49 | 25.8 ± 4.02 | 26.43 ± 5.95 | 28.58 ± 6.50 | 25.1 ± 6.05 | 0.58 | 0.21 | 0.23 |
| BMI (kg/m2) | 22.31 ± 2.37 | 21.76 ± 2.76 | 22.81 ± 1.97 | 21.60 ± 1.80 | 22.40 ± 1.57 | 20.89 ± 1.86 | 0.29 | 0.55 | 0.01 * |
| PSQI | 11.26 ± 2.33 | 10.22 ± 2.22 | 12.20 ± 2.10 | 12.33 ± 2.20 | 12.75 ± 2.05 | 11.78 ± 2.87 | 0.14 | 0.01 * | 0.69 |
| ISI | 16.74 ± 3.03 | 16.44 ± 2.30 | 17 ± 3.68 | 17.52 ± 3.49 | 18.17 ± 3.54 | 16.67 ± 3.43 | 0.45 | 0.22 | 0.84 |
| BDI-II | 11.21 ± 6.69 | 11.44 ± 7.59 | 11 ± 6.18 | 13.81 ± 9.64 | 15 ± 11.17 | 13.44 ± 7.89 | 0.33 | 0.55 | 0.65 |
| BAI | 10.32 ± 6.98 | 12.44 ± 7.28 | 8.4 ± 6.47 | 9.81 ± 7.93 | 10.75 ± 9.46 | 8.56 ± 5.59 | 0.83 | 0.70 | 0.88 |
| ESS | 9.63 ± 3.59 | 8.67 ± 3.12 | 10.5 ± 3.92 | 9.05 ± 4.75 | 9.25 ± 5.03 | 8.78 ± 4.63 | 0.67 | 0.76 | 0.39 |
| MEQ | 44.37 ± 10.51 | 47.56 ± 6.39 | 41.5 ± 12.86 | 46.52 ± 13.50 | 45.08 ± 13.62 | 48.44 ± 13.90 | 0.58 | 0.62 | 0.27 |
| STAI | 48.39 ± 10.45 | 50.38 ± 10.76 | 46.8 ± 10.49 | 48.65 ± 12.17 | 46.33 ± 13.77 | 52.13 ± 9.02 | 0.94 | 0.49 | 0.27 |
| SL (min) | 29.29 ± 27.20 | 45.83 ± 30.95 | 14.40 ± 10.41 | 22.43 ± 20.70 | 31.98 ± 22.98 | 9.70 ± 5.01 | 0.37 | 0.50 | 0.23 |
| WASO (min) | 27.23 ± 17.66 | 37.52 ± 21.00 | 17.96 ± 5.48 | 36.04 ± 28.35 | 46.44 ± 34.23 | 22.18 ± 4.48 | 0.25 | 0.88 | 0.09 |
| SE (%) | 87.95 ± 5.52 | 83.16 ± 3.15 | 92.27 ± 2.89 | 87.23 ± 6.38 | 83.46 ± 5.90 | 92.27 ± 2.00 | 0.71 | 0.25 | 1.00 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ho, Y.-T.; Tsai, Y.-C.; Kuo, T.B.J.; Yang, C.C.H. Effects of Lactobacillus plantarum PS128 on Depressive Symptoms and Sleep Quality in Self-Reported Insomniacs: A Randomized, Double-Blind, Placebo-Controlled Pilot Trial. Nutrients 2021, 13, 2820. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13082820
Ho Y-T, Tsai Y-C, Kuo TBJ, Yang CCH. Effects of Lactobacillus plantarum PS128 on Depressive Symptoms and Sleep Quality in Self-Reported Insomniacs: A Randomized, Double-Blind, Placebo-Controlled Pilot Trial. Nutrients. 2021; 13(8):2820. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13082820
Chicago/Turabian StyleHo, Yu-Ting, Ying-Chieh Tsai, Terry B. J. Kuo, and Cheryl C. H. Yang. 2021. "Effects of Lactobacillus plantarum PS128 on Depressive Symptoms and Sleep Quality in Self-Reported Insomniacs: A Randomized, Double-Blind, Placebo-Controlled Pilot Trial" Nutrients 13, no. 8: 2820. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13082820