
Clinical Evaluation of 16-Week Supplementation with 5HMO-Mix in Healthy-Term Human Infants to Determine Tolerability, Safety, and Effect on Growth

Abstract
:1. Introduction
2. Materials and Methods
2.1. Clinical Study—General Aspects and Ethical Compliance
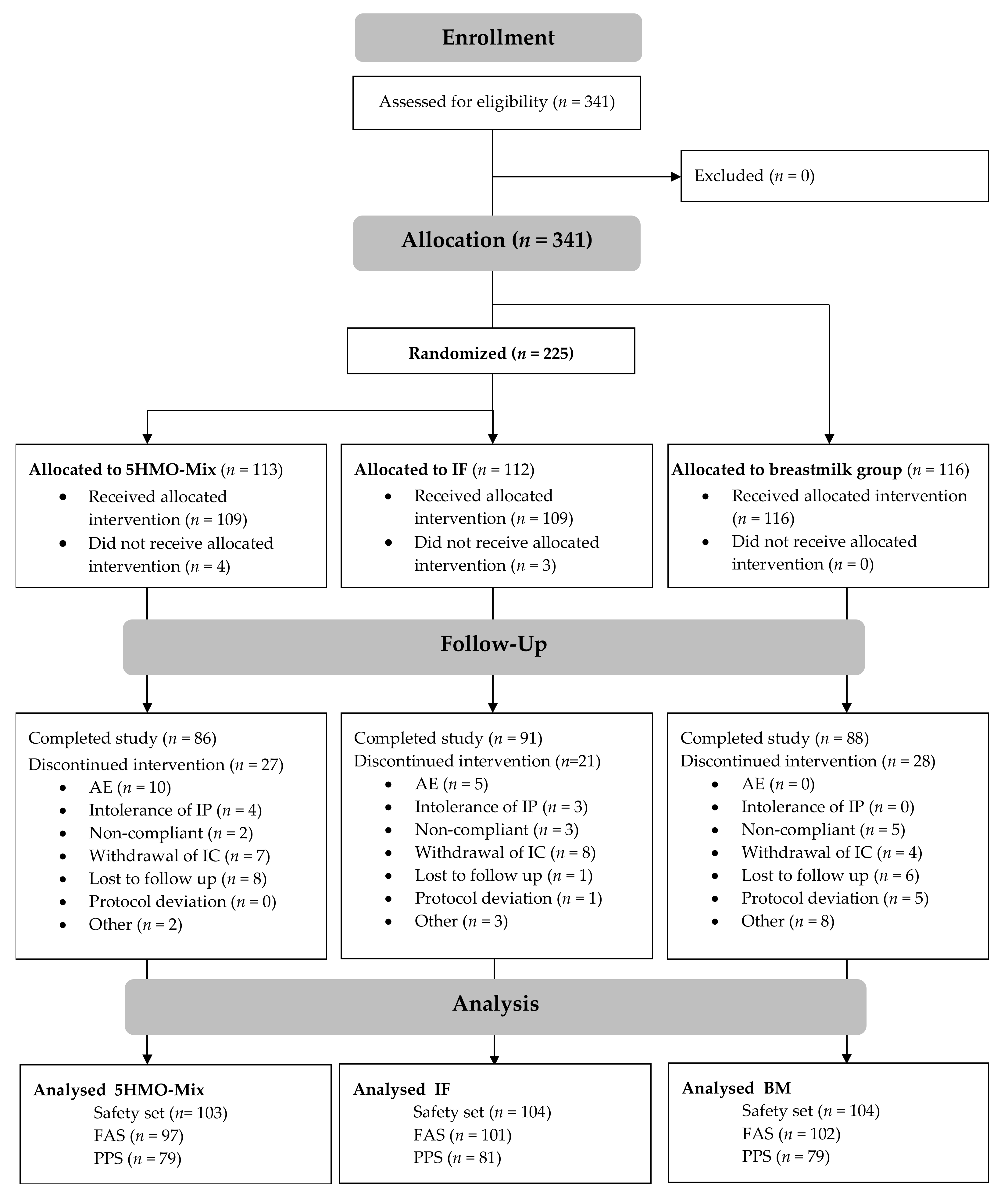
2.2. Participants
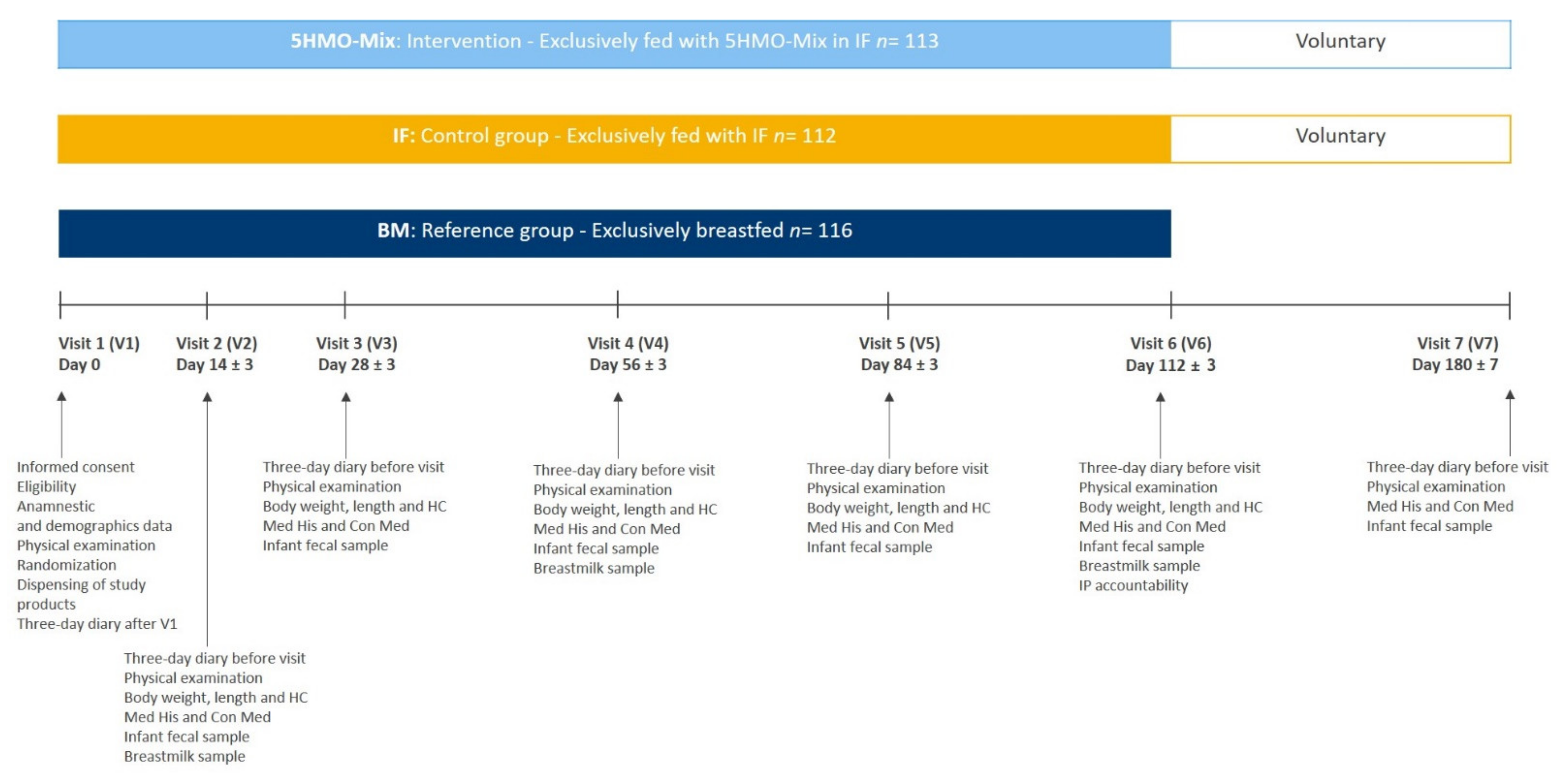
2.3. Study Design
2.4. Study Product
2.5. Outcome Measures
2.6. Statistical Analysis
3. Results
3.1. Subject Characteristics
3.2. Growth Outcomes
3.3. Infant Formula Intake
3.4. Gastrointestinal and Behavioral Tolerance Parameters
3.5. Adverse Events
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Cheng, L.; Akkerman, R.; Kong, C.; Walvoort, M.T.; de Vos, P. More than sugar in the milk: Human milk oligosaccharides as essential bioactive molecules in breast milk and current insight in beneficial effects. Crit. Rev. Food Sci. Nutr. 2021, 61, 1184–1200. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Available online: https://www.who.int/ (accessed on 5 June 2021).
- Urashima, T.; Kitaoka, M.; Asakuma, S.; Messer, M. Milk oligosaccharides. In Advanced Dairy Chemistry; McSweeney, P., Fox, P.F., Eds.; Springer: New York, NY, USA, 2009; pp. 295–349. [Google Scholar]
- Bäckhed, F.; Roswall, J.; Peng, Y.; Feng, Q.; Jia, H.; Kovatcheva-Datchary, P.; Li, Y.; Xia, Y.; Xie, H.; Zhong, H.; et al. Dynamics and stabilization of the human gut microbiome during the first year of life. Cell Host Microbe 2015, 17, 690–703. [Google Scholar] [CrossRef] [Green Version]
- Underwood, M.A.; German, J.B.; Lebrilla, C.B.; Mills, D.A. Bifidobacterium longum subspecies infantis: Champion colonizer of the infant gut. Pediatric Res. 2015, 77, 229–235. [Google Scholar] [CrossRef] [Green Version]
- Sela, D.A.; Chapman, J.; Adeuya, A.; Kim, J.H.; Chen, F.; Whitehead, T.R.; Lapidus, A.; Rokhsar, D.S.; Lebrilla, C.B.; German, J.B.; et al. The genome sequence of Bifidobacterium longum subsp. infantis reveals adaptations for milk utilization within the infant microbiome. Proc. Natl Acad. Sci. USA 2008, 105, 18964–18969. [Google Scholar] [PubMed] [Green Version]
- James, K.; Bottacini, F.; Contreras, J.I.S.; Vigoureux, M.; Egan, M.; Motherway, M.O.C.; Holmes, E.; van Sinderen, D. Metabolism of the predominant human milk oligosaccharide fucosyllactose by an infant gut commensal. Sci. Rep. 2019, 9, 1–20. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thomson, P.; Garrido, D. Human milk oligosaccharides and health promotion through the gut microbiome. In Dairy in Human Health and Disease Across the Lifespan; Watson, R.R., Collier, R.J., Preedy, V.R., Eds.; Academic Press: London, UK, 2017; pp. 73–86. [Google Scholar]
- Thongaram, T.; Hoeflinger, J.L.; Chow, J.; Miller, M.J. Human milk oligosaccharide consumption by probiotic and human-associated bifidobacteria and lactobacilli. J. Dairy Sci. 2017, 100, 7825–7833. [Google Scholar] [CrossRef] [Green Version]
- Lawson, M.A.; O’Neill, I.J.; Kujawska, M.; Javvadi, S.G.; Wijeyesekera, A.; Flegg, Z.; Chalklen, L.; Hall, L.J. Breast milk-derived human milk oligosaccharides promote Bifidobacterium interactions within a single ecosystem. ISME J. 2020, 14, 635–648. [Google Scholar] [CrossRef] [Green Version]
- Gotoh, A.; Katoh, T.; Sakanaka, M.; Ling, Y.; Yamada, C.; Asakuma, S.; Urashima, T.; Tomabechi, Y.; Katayama-Ikegami, A.; Kurihara, S.; et al. Sharing of human milk oligosaccharides degradants within bifidobacterial communities in faecal cultures supplemented with Bifidobacterium bifidum. Sci. Rep. 2018, 8, 13958. [Google Scholar] [CrossRef] [PubMed]
- Marcobal, A.; Sonnenburg, J.L. Human milk oligosaccharide consumption by intestinal microbiota. Clin. Microbiol. Infect. 2012, 18, 12–15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rodríguez-Díaz, J.; Rubio-del-Campo, A.; Yebra, M.J. Lactobacillus casei ferments the N-acetylglucosamine moiety of fucosyl-α-1, 3-N-acetylglucosamine and excretes l-fucose. Appl. Env. Microbiol. 2012, 78, 4613–4619. [Google Scholar] [CrossRef] [Green Version]
- Salli, K.; Hirvonen, J.; Siitonen, J.; Ahonen, I.; Anglenius, H.; Maukonen, J. Selective utilization of the human milk oligosaccharides 2′-fucosyllactose, 3-fucosyllactose, and difucosyllactose by various probiotic and pathogenic bacteria. J. Agric. Food Chem. 2021, 69, 170–182. [Google Scholar] [CrossRef]
- Ayechu-Muruzabal, V.; van Stigt, A.H.; Mank, M.; Willemsen, L.E.; Stahl, B.; Garssen, J.; Van’t Land, B. Diversity of human milk oligosaccharides and effects on early life immune development. Front. Pediatrics 2018, 6, 239. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sodhi, C.P.; Wipf, P.; Yamaguchi, Y.; Fulton, W.B.; Kovler, M.; Niño, D.F.; Zhou, Q.; Banfield, E.; Werts, A.D.; Ladd, M.R.; et al. The human milk oligosaccharides 2’-fucosyllactose and 6’-sialyllactose protect against the development of necrotizing enterocolitis by inhibiting toll-like receptor 4 signaling. Pediatric Res. 2021, 89, 91–101. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.; Zhang, M.; Guo, H.; Yan, J.; Liu, F.; Chen, J.; Li, Y.; Ren, F. Human milk oligosaccharides protect against necrotizing enterocolitis by inhibiting intestinal damage via increasing the proliferation of crypt cells. Mol. Nutr. Food Res. 2019, 63, 1900262. [Google Scholar] [CrossRef] [PubMed]
- Kong, C.; Elderman, M.; Cheng, L.; de Haan, B.J.; Nauta, A.; de Vos, P. Modulation of intestinal epithelial glycocalyx development by human milk oligosaccharides and non-digestible carbohydrates. Mol. Nutr. Food Res. 2019, 63, 1900303. [Google Scholar] [CrossRef]
- Natividad, J.M.; Rytz, A.; Keddani, S.; Bergonzelli, G.; Garcia-Rodenas, C.L. Blends of human milk oligosaccharides confer intestinal epithelial barrier protection in vitro. Nutrients 2020, 12, 3047. [Google Scholar] [CrossRef] [PubMed]
- Wang, B.; Yu, B.; Karim, M.; Hu, H.; Sun, Y.; McGreevy, P.; Petocz, P.; Held, S.; Brand-Miller, J. Dietary sialic acid supplementation improves learning and memory in piglets. Am. J. Clin. Nutr. 2007, 85, 561–569. [Google Scholar] [CrossRef] [Green Version]
- Sakai, F.; Ikeuchi, Y.; Urashima, T.; Fujihara, M.; Ohtsuki, K.; Yanahira, S. Effects of feeding sialyllactose and galactosylated N-acetylneuraminic acid on swimming learning ability and brain lipid composition in adult rats. J. Appl. Glycosci. 2006, 53, 249–254. [Google Scholar] [CrossRef] [Green Version]
- Oliveros, E.; Vázquez, E.; Barranco, A.; Ramírez, M.; Gruart, A.; Delgado-García, J.M.; Buck, R.; Rueda, R.; Martín, M.J. Sialic acid and sialylated oligosaccharide supplementation during lactation improves learning and memory in rats. Nutrients 2018, 10, 1519. [Google Scholar] [CrossRef] [Green Version]
- Docq, S.; Spoelder, M.; Wang, W.; Homberg, J.R. The protective and long-lasting effects of human milk oligosaccharides on cognition in mammals. Nutrients 2020, 12, 3572. [Google Scholar] [CrossRef]
- Berger, P.K.; Plows, J.F.; Jones, R.B.; Alderete, T.L.; Yonemitsu, C.; Poulsen, M.; Ryoo, J.H.; Peterson, B.S.; Bode, L.; Goran, M.I. Human milk oligosaccharide 2′-fucosyllactose links feedings at 1 month to cognitive development at 24 months in infants of normal and overweight mothers. PLoS ONE 2020, 15, e0228323. [Google Scholar] [CrossRef]
- Oliveros, E.; Martín, M.J.; Torres-Espínola, F.J.; Segura-Moreno, M.T.; Ramírez, M.; Santos, A.; Buck, R.; Rueda, R.; Escudero, M.; Catena, A.; et al. Human milk levels of 2′-fucosyllactose and 6′-sialyllactose are positively associated with infant neurodevelopment and are not impacted by maternal BMI or diabetic status. J. Nutr. Food Sci. 2021, 4, 100024. [Google Scholar]
- Walsh, C.; Lane, J.A.; van Sinderen, D.; Hickey, R.M. Human milk oligosaccharides: Shaping the infant gut microbiota and supporting health. J. Funct. Foods 2020, 72, 104074. [Google Scholar] [CrossRef] [PubMed]
- Lis-Kuberka, J.; Orczyk-Pawiłowicz, M. Sialylated oligosaccharides and glycoconjugates of human milk. The impact on infant and newborn protection, development and well-being. Nutrients 2019, 11, 306. [Google Scholar] [CrossRef] [Green Version]
- Craft, K.M.; Townsend, S.D. The human milk glycome as a defense against infectious diseases: Rationale, challenges, and opportunities. ACS Infect. Dis. 2018, 4, 77–83. [Google Scholar] [CrossRef] [PubMed]
- Sprenger, N.; Lee, L.Y.; De Castro, C.A.; Steenhout, P.; Thakkar, S.K. Longitudinal change of selected human milk oligosaccharides and association to infants’ growth, an observatory, single center, longitudinal cohort study. PLoS ONE 2017, 12, e0171814. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ma, L.; McJarrow, P.; Mohamed, H.J.B.J.; Liu, X.; Welman, A.; Fong, B.Y. Lactational changes in the human milk oligosaccharide concentration in Chinese and Malaysian mothers’ milk. Int. Dairy J. 2018, 87, 1–10. [Google Scholar] [CrossRef]
- McGuire, M.K.; Meehan, C.L.; McGuire, M.A.; Williams, J.E.; Foster, J.; Sellen, D.W.; Kamau-Mbuthia, E.W.; Kamundia, E.W.; Mbugua, S.; Moore, S.E.; et al. What’s normal? Oligosaccharide concentrations and profiles in milk produced by healthy women vary geographically. Am. J. Clin. Nutr. 2017, 105, 1086–1100. [Google Scholar] [CrossRef]
- Seferovic, M.D.; Mohammad, M.; Pace, R.M.; Engevik, M.; Versalovic, J.; Bode, L.; Haymond, M.; Aagaard, K.M. Maternal diet alters human milk oligosaccharide composition with implications for the milk metagenome. Sci. Rep. 2020, 10, 22092. [Google Scholar] [CrossRef]
- Thurl, S.; Munzert, M.; Boehm, G.; Matthews, C.; Stahl, B. Systematic review of the concentrations of oligosaccharides in human milk. Nutr. Rev. 2017, 75, 920–933. [Google Scholar] [CrossRef] [Green Version]
- Austin, S.; De Castro, C.A.; Sprenger, N.; Binia, A.; Affolter, M.; Garcia-Rodenas, C.L.; Beauport, L.; Tolsa, J.F.; Fumeaux, C.J.F. Human milk oligosaccharides in the milk of mothers delivering term versus preterm infants. Nutrients 2019, 11, 1282. [Google Scholar] [CrossRef] [Green Version]
- Azad, M.B.; Robertson, B.; Atakora, F.; Becker, A.B.; Subbarao, P.; Moraes, T.J.; Mandhane, P.J.; Turvey, S.E.; Lefebvre, D.L.; Sears, M.R.; et al. Human milk oligosaccharide concentrations are associated with multiple fixed and modifiable maternal characteristics, environmental factors, and feeding practices. J. Nutr. 2018, 148, 1733–1742. [Google Scholar] [CrossRef]
- Samuel, T.M.; Binia, A.; de Castro, C.A.; Thakkar, S.K.; Billeaud, C.; Agosti, M.; Al-Jashi, I.; Costeira, M.J.; Marchini, G.; Martínez-Costa, C.; et al. Impact of maternal characteristics on human milk oligosaccharide composition over the first 4 months of lactation in a cohort of healthy European mothers. Sci. Rep. 2019, 9, 11767. [Google Scholar] [CrossRef]
- Totten, S.M.; Zivkovic, A.M.; Wu, S.; Ngyuen, U.; Freeman, S.L.; Ruhaak, L.R.; Darboe, M.K.; German, J.B.; Prentice, A.M.; Lebrilla, C.B. Comprehensive profiles of human milk oligosaccharides yield highly sensitive and specific markers for determining secretor status in lactating mothers. J. Proteome Res. 2012, 11, 6124–6133. [Google Scholar] [CrossRef] [PubMed]
- Chaturvedi, P.; Warren, C.D.; Altaye, M.; Morrow, A.L.; Ruiz-Palacios, G.; Pickering, L.K.; Newburg, D.S. Fucosylated human milk oligosaccharides vary between individuals and over the course of lactation. Glycobiology 2001, 11, 365–372. [Google Scholar] [CrossRef] [PubMed]
- Thurl, S.; Munzert, M.; Henker, J.; Boehm, G.; Müller-Werner, B.; Jelinek, J.; Stahl, B. Variation of human milk oligosaccharides in relation to milk groups and lactational periods. Br. J. Nutr. 2010, 104, 1261–1271. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, J.; Wu, S.; Huo, J.; Ruan, H.; Xu, X.; Hao, Z.; Wei, Y.A. Systematic characterization and longitudinal study reveal distinguishing features of human milk oligosaccharides in China. Curr. Dev. Nutr. 2020, 4, nzaa113. [Google Scholar] [CrossRef]
- Coppa, G.V.; Pierani, P.; Zampini, L.; Carloni, I.; Carlucci, A.; Gabrielli, O. Oligosaccharides in human milk during different phases of lactation. Acta Paediatr. 1999, 88, 89–94. [Google Scholar] [CrossRef] [PubMed]
- Marriage, B.J.; Buck, R.H.; Goehring, K.C.; Oliver, J.S.; Williams, J.A. Infants fed a lower calorie formula with 2′ FL show growth and 2′ FL uptake like breast-fed infants. J. Pediatric Gastroenterol. Nutr. 2015, 61, 649. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goehring, K.C.; Marriage, B.J.; Oliver, J.S.; Wilder, J.A.; Barrett, E.G.; Buck, R.H. Similar to those who are breastfed, infants fed a formula containing 2′-fucosyllactose have lower inflammatory cytokines in a randomized controlled trial. J. Nutr. 2016, 146, 2559–2566. [Google Scholar] [CrossRef] [Green Version]
- Storm, H.M.; Shepard, J.; Czerkies, L.M.; Kineman, B.; Cohen, S.S.; Reichert, H.; Carvalho, R. 2′-Fucosyllactose is well tolerated in a 100% whey, partially hydrolyzed infant formula with Bifidobacterium lactis: A randomized controlled trial. Glob. Pediatr. Health 2019, 6, 2333794X19833995. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Puccio, G.; Alliet, P.; Cajozzo, C.; Janssens, E.; Corsello, G.; Sprenger, N.; Wernimont, S.; Egli, D.; Gosoniu, L.; Steenhout, P. Effects of infant formula with human milk oligosaccharides on growth and morbidity: A randomized multicenter trial. J. Pediatric Gastroenterol. Nutr. 2017, 64, 624. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vandenplas, Y.; de Halleux, V.; Arciszewska, M.; Lach, P.; Pokhylko, V.; Klymenko, V.; Schoen, S.; Abrahamse-Berkeveld, M.; Mulder, K.A.; Porcel Rubio, R.; et al. A partly fermented infant formula with postbiotics including 3′-GL, specific oligosaccharides, 2′-FL, and milk fat supports adequate growth, is safe and well-tolerated in healthy term infants: A double-blind, randomised, controlled, multi-country trial. Nutrients 2020, 12, 3560. [Google Scholar] [CrossRef] [PubMed]
- Bekkali, N.; Hamers, S.L.; Reitsma, J.B.; Van Toledo, L.; Benninga, M.A. Infant stool form scale: Development and results. J. Pediatrics 2009, 154, 521–526.e1. [Google Scholar] [CrossRef] [PubMed]
- American Academy of Pediatrics Task Force. Clinical Testing of Infant Formulas with Respect to Nutritional Suitability for Term Infants. Available online: http://wayback.archive-it.org/7993/20170722090324/https://www.fda.gov/Food/GuidanceRegulation/GuidanceDocumentsRegulatoryInformation/InfantFormula/ucm170649.htm (accessed on 5 June 2021).
- Puccio, G.; Cajozzo, C.; Meli, F.; Rochat, F.; Grathwohl, D.; Steenhout, P. Clinical evaluation of a new starter formula for infants containing live Bifidobacterium longum BL999 and prebiotics. Nutrition 2007, 23, 1–8. [Google Scholar] [CrossRef]
- Ashley, C.; Johnston, W.H.; Harris, C.L.; Stolz, S.I.; Wampler, J.L.; Berseth, C.L. Growth and tolerance of infants fed formula supplemented with polydextrose (PDX) and/or galactooligosaccharides (GOS): Double-blind, randomized, controlled trial. Nutr. J. 2012, 11, 1–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- FDA Guidance on Conduct of Clinical Trials of Medical Products During the COVID-19 Public Health Emergency. In Guidance for Industry, Investigators, and Institutional Review Boards; Center for Biologics Evaluation and Research, Center for Devices and Radiological Health, Center for Drug Evaluation and Research, Office of the Commissioner, Office of Clinical Policy and Programs, Office of Clinical Policy, Office of Good Clinical Practice: Rockville, MD, USA, 2020.
- EMA Guidance on the Management of Clinical Trials during the COVID-19 (Coronavirus) Pandemic; European Medincine Agency: Amsterdam, The Netherlands, 2020.
- Urashima, T.; Messer, M.; Oftedal, O.T. Oligosaccharides in the milk of other mammals. In Prebiotics and Probiotics in Human Milk; McGuire, M.K., McGuire, M.A., Bode, L., Eds.; Academic Press: London, UK, 2016; pp. 45–139. [Google Scholar]
- Román, E.; Moreno Villares, J.M.; Domínguez Ortega, F.; Carmona Martínez, A.; Picó Sirvent, L.; Santana Sandoval, L.; Casas Rivero, J.; Alshweki, A.; Cercamondi, C.; Dahbane, S.; et al. Real-world study in infants fed with an infant formula with two human milk oligosaccharides. Nutr. Hosp. 2020, 37, 698–706. [Google Scholar] [CrossRef]
- Sievers, E.; Oldigs, H.D.; Santer, R.; Schaub, J. Feeding patterns in breast-fed and formula-fed infants. Ann. Nutr. Metab. 2002, 46, 243–248. [Google Scholar] [CrossRef]
- Bell, K.A.; Wagner, C.L.; Feldman, H.A.; Shypailo, R.J.; Belfort, M.B. Associations of infant feeding with trajectories of body composition and growth. Am. J. Clin. Nutr. 2017, 106, 491–498. [Google Scholar] [CrossRef]
- Li, R.; Magadia, J.; Fein, S.B.; Grummer-Strawn, L.M. Risk of bottle-feeding for rapid weight gain during the first year of life. Arch. Pediatr. Adolesc. Med. 2012, 166, 431–436. [Google Scholar] [PubMed]
- Li, R.; Fein, S.B.; Grummer-Strawn, L.M. Do infants fed from bottles lack self-regulation of milk intake compared with directly breastfed infants? Pediatrics 2010, 125, e1386–e1393. [Google Scholar] [CrossRef] [Green Version]
- Reilly, J.J.; Ashworth, S.; Wells, J.C. Metabolisable energy consumption in the exclusively breast-fed infant aged 3–6 months from the developed world: A systematic review. Br. J. Nutr. 2005, 94, 56–63. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sauer, C.W.; Boutin, M.A.; Kim, J.H. Wide variability in caloric density of expressed human milk can lead to major underestimation or overestimation of nutrient content. J. Hum. Lact. 2017, 33, 341–350. [Google Scholar] [CrossRef] [PubMed]
- Biddulph, C.; Holmes, M.; Kuballa, A.; Davies, P.S.; Koorts, P.; Carter, R.J.; Maher, J. Human milk oligosaccharide profiles and associations with maternal nutritional factors: A scoping review. Nutrients 2021, 13, 965. [Google Scholar] [CrossRef] [PubMed]
- Berger, B.; Porta, N.; Foata, F.; Grathwohl, D.; Delley, M.; Moine, D.; Charpagne, A.; Siegwald, L.; Descombes, P.; Alliet, P.; et al. Linking human milk oligosaccharides, infant fecal community types, and later risk to require antibiotics. Mbio 2020, 11, e03196. [Google Scholar] [CrossRef] [Green Version]
- Butte, N.; Jensen, C.; Moon, J.; Glaze, D.G.; Frost, J.D., Jr. Sleep organization and energy expenditure of breast-fed and formula-fed infants. Pediatr. Res. 1992, 32, 514–519. [Google Scholar] [CrossRef] [Green Version]
- Ramirez-Farias, C.; Baggs, G.E.; Marriage, B.J. Growth, Tolerance, and Compliance of Infants Fed an Extensively Hydrolyzed Infant Formula with Added 2’-FL Fucosyllactose (2′-FL) Human Milk Oligosaccharide. Nutrients 2021, 13, 186. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| 5HMO-Mix | IF | ||||
|---|---|---|---|---|---|
| Unit | Per 100 g Powder | Per 100 mL Ready to Drink | Per 100 g Powder | Per 100 mL Ready to Drink | |
| Energy 1,2 | KJ | 2129 | 280 | 2163 | 283 |
| kcal | 507 | 67 | 515 | 68 | |
| Fat | g | 27 | 3.6 | 27 | 3.6 |
| Saturated | g | 9.3 | 1.2 | 9.3 | 1.2 |
| Monounsaturated | g | 12.6 | 1.7 | 12.6 | 1.7 |
| Polyunsaturated | g | 5.1 | 0.7 | 5.1 | 0.7 |
| Carbohydrate 3 | g | 53 | 7.2 | 57 | 7.2 |
| Lactose | g | 39 | 5.2 | 39 | 5.2 |
| Maltodextrin | g | 11.65 | 4.8 | 16 | 5.4 |
| HMO | g | 4.35 | 0.575 | - | - |
| 2′FL | g | 2.26 | 0.299 | - | - |
| 3-FL | g | 0.57 | 0.075 | - | - |
| LNT | g | 1.13 | 0.150 | - | - |
| 3′-SL | g | 0.17 | 0.023 | - | - |
| 6′-SL | g | 0.22 | 0.028 | - | - |
| Protein | g | 11 | 1.4 | 11 | 1.4 |
| Salt 4 | g | 0.45 | 0.060 | 0.45 | 0.06 |
| 5HMO-Mix n = 103 | IF n = 104 | BM n = 104 | Total n = 311 | |
|---|---|---|---|---|
| Sex, n (%) | ||||
| Male | 54 (52.4) | 55 (52.9) | 52 (50.0) | 161 (51.8) |
| Female | 49 (47.6) | 49 (47.1) | 52 (50.0) | 150 (48.2) |
| Age at enrollment, days | 4.8 ± 3.2 (1–16) | 4.3 ± 2.7 (1–14) | 5.2 ± 3.6 (1–14) | 4.8 ± 3.2 (1–16) |
| Gestational age at birth, weeks | 39.3 ± 1.1 | 39.3 ± 1.2 | 39.4 ± 1.1 | 39.3 ± 1.1 |
| Ethnicity, n (%) | ||||
| Caucasian | 95 (92.2) | 100 (96.2) | 97 (93.3) | 292 (93.9) |
| African | 1 (1.0) | 1 (1.0) | - | 2 (0.6) |
| Mixed | 6 (5.8) | 3 (2.9) | 4 (3.8) | 13 (4.2) |
| Other | 1 (1.0) | - | 3 (2.9) | 4 (1.3) |
| Mode of delivery, n (%) | ||||
| Vaginal | 56 (54.1) | 64 (61.5) | 73 (70.2) | 193 62.1) |
| Cesarean section | 32 (31.1) | 33 (31.7) | 24 (23.1) | |
| Assisted vaginal | 15 (14.6) | 7 (6.7) | 7 (6.7) | 29 (9.3) |
| Birth weight, g | 3321.8 ± 434.7 | 3351.1 ± 405.5 | 3412.0 ± 381.3 | 3361.8 ± 408.1 |
| Birth length, cm | 50.04 ± 2.01 | 50.44 ± 2.23 | 50.54 ± 1.97 | 50.34 ± 20.8 |
| Birth head circumference, cm | 34.65 ± 1.13 | 34.68 ± 1.23 | 34.65 ± 1.48 | 34.66 ± 1.29 |
| APGAR score 1 | 10.0 ± 0.2 (9–10) | 9.9 ± 0.3 (9–10) | 9.9 ± 0.3 (9–10) | 9.9 ± 0.3 (9–10) |
| Use of antibiotics by mother before or during delivery, n (%) | 15 (14.6) | 20 (19.2) | 22 (21.2) | |
| Feeding history from birth up to enrollment, n (%) | ||||
| Breast milk fed | 11 (10.7) | 6 (5.8) | 93 (92.3) | |
| Infant formula fed | 92 (89.3) | 98 (94.2) | 8 (7.7) |
| 5HMO-Mix | IF | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| n | Mean ± SD | Min | Max | n | Mean ± SD | Min | Max | p-Value | |
| V1 | 97 | 3236.5 ± 410.5 | 2480.0 | 4260.0 | 101 | 3274.4 ± 393.9 | 2510.0 | 4230.0 | - |
| V2 | 97 | 3643.2 ± 433.0 | 2863.3 | 4690.0 | 100 | 3682.5 ± 444.1 | 2686.7 | 4790.0 | 0.8441 |
| V3 | 91 | 4212.0 ± 477.5 | 3271.7 | 5710.0 | 97 | 4257.1 ± 468.8 | 3306.7 | 5316.7 | 0.9579 |
| V4 | 88 | 5148.7 ± 537.1 | 3995.0 | 6540.0 | 93 | 5178.9 ± 542.8 | 3906.7 | 6280.0 | 0.8589 |
| V5 | 86 | 5893.7 ± 623.9 | 4595.0 | 8000.0 | 88 | 5867.0 ± 600.4 | 4603.3 | 7490.0 | 0.4245 |
| V6 | 84 | 6578.8 ± 697.6 | 5170.0 | 9195.0 | 89 | 6557.3 ± 672.8 | 5059.3 | 8280.0 | 0.5314 |
| 5HMO-Mix | IF | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| n | Mean ± SD | Median | Min | Max | n | Mean ± SD | Median | Min | Max | |
| V1 | 93 | 101 | ||||||||
| mL | 459.7 ± 137.7 | 455.0 | 23.3 | 990.0 | 442.9 ± 135.4 | 440.0 | 150.0 | 811.7 | ||
| Kcal | 312.6 ± 93.6 | 309.4 | 15.9 | 673.2 | 301.2 ± 92.1 | 299.2 | 102.0 | 551.9 | ||
| V2 | 95 | 100 | ||||||||
| mL | 603.5 ± 134.5 | 605.0 | 70.0 | 900.0 | 617.3 ± 141.6 | 604.2 | 80.0 | 1196.7 | ||
| Kcal | 410.4 ± 91.5 | 411.4 | 47.6 | 612.0 | 419.7 ± 96.3 | 410.8 | 54.4 | 813.7 | ||
| V3 | 89 | 97 | ||||||||
| mL | 744.5 ± 163.2 | 713.3 | 453.3 | 1456.7 | 769.7 ± 161.6 | 766.7 | 410.0 | 1440.0 | ||
| Kcal | 506.3 ± 111.0 | 485.1 | 308.3 | 990.5 | 523.4 ± 109.9 | 521.3 | 278.8 | 979.2 | ||
| V4 | 87 | 94 | ||||||||
| mL | 802.4 ± 152.1 | 786.7 | 490.0 | 1290.0 | 832.7 ± 179.9 | 808.3 | 533.3 | 1910.0 | ||
| Kcal | 545.6 ± 103.4 | 534.9 | 333.2 | 877.2 | 566.2 ± 122.3 | 549.7 | 362.7 | 1298.8 | ||
| V5 | 86 | 92 | ||||||||
| mL | 857.6 ± 189.4‚ | 835.8 | 466.7 | 1430.0 | 871.2 ± 185.4 | 855.0 | 556.7 | 1591.7 | ||
| Kcal | 583.2 ± 128.8 | 568.4 | 317.3 | 972.4‚ | 592.4 ± 126.0 | 581.4 | 378.5 | 1082.3 | ||
| V6 | 83 | 89 | ||||||||
| mL | 902.5 ± 170.0 | 870.0 | 480.0 | 1580.0 | 928.2 ± 165.9 | 900.0 | 636.7 | 1576.7 | ||
| Kcal | 613.7 ± 115.6 | 591.6 | 326.4‚ | 1074.4 | 631.2 ± 112.8 | 612.0 | 432.9 | 1072.1 | ||
| 5HMO-Mix | IF | BM | 5HMO-Mix vs. IF | 5HMO-Mix vs. BM | IF vs. BM | |
|---|---|---|---|---|---|---|
| n | n | n | p-Value | p-Value | p-Value | |
| Gastrointestinal disorders | 64 | 58 | 40 | 0.3975 | 0.0008 | 0.0180 |
| Infections and infestations | 32 | 28 | 34 | 0.5426 | 0.8817 | 0.4486 |
| Skin and subcutaneous tissue disorders | 14 | 21 | 7 | 0.2660 | 0.1129 | 0.0074 |
| Respiratory, thoracic, and mediastinal disorders | 10 | 10 | 7 | 1.0000 | 0.4603 | 0.6140 |
| General disorders and administration site conditions | 6 | 8 | 15 | 0.7831 | 0.0635 | 0.1838 |
| Metabolism and nutrition disorders | 5 | 1 | 3 | 0.1187 | 0.4981 | 0.6214 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Parschat, K.; Melsaether, C.; Jäpelt, K.R.; Jennewein, S. Clinical Evaluation of 16-Week Supplementation with 5HMO-Mix in Healthy-Term Human Infants to Determine Tolerability, Safety, and Effect on Growth. Nutrients 2021, 13, 2871. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13082871
Parschat K, Melsaether C, Jäpelt KR, Jennewein S. Clinical Evaluation of 16-Week Supplementation with 5HMO-Mix in Healthy-Term Human Infants to Determine Tolerability, Safety, and Effect on Growth. Nutrients. 2021; 13(8):2871. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13082871
Chicago/Turabian StyleParschat, Katja, Cathrine Melsaether, Kristina Rasch Jäpelt, and Stefan Jennewein. 2021. "Clinical Evaluation of 16-Week Supplementation with 5HMO-Mix in Healthy-Term Human Infants to Determine Tolerability, Safety, and Effect on Growth" Nutrients 13, no. 8: 2871. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13082871