
Influence of Healthy Habits Counseling on Biochemical and Metabolic Parameters in Children and Adolescents with HIV: Longitudinal Study

 ,
,  , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
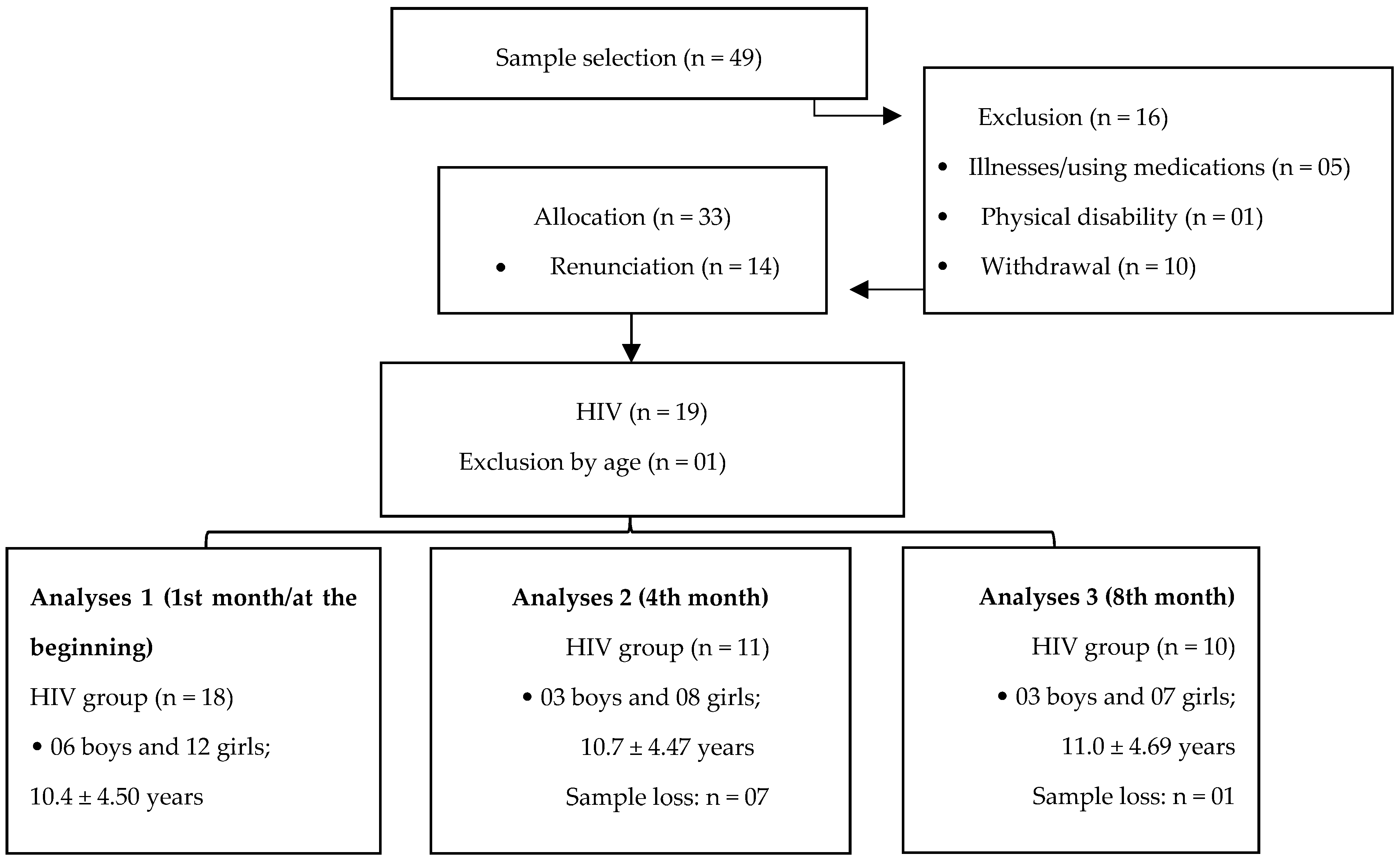
2.1. Sample
2.2. Instruments and Procedures
2.2.1. Anamnesis
2.2.2. Biochemical Parameters
2.2.3. Resting Metabolic Rate (RMR)
2.2.4. Usual Food Intake
2.2.5. Habitual Physical Activity Level (HPAL)
2.2.6. Chronological Age Analysis
2.2.7. Biological Maturation
2.2.8. Body Composition
2.2.9. Interventions: Guidelines for Healthy Eating
2.2.10. Guidance on Physical Activity
2.2.11. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Botros, D.; Somarriba, G.; Neri, D.; Miller, T.L. Interventions to address chronic disease and HIV: Strategies to promote exercise and nutrition among HIV-infected individuals. Curr. HIV AIDS Rep. 2012, 9, 351–363. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Penazzato, M.; Irvine, C.; Vicari, M.; Essajee, S.M.; Sharma, A.; Puthanakit, T.; Abrams, E.J.; Doherty, M. A Global Research Agenda for Pediatric HIV. J. Acquir. Immune Defic. Syndr. 2018, 78, S10–S15. [Google Scholar] [CrossRef] [PubMed]
- De Baros Ramalho, L.C.; Gonçalves, E.; de Carvalho, W.R.G.; Guerra-Junior, G.; Centeville, M.; Aoki, F.H.; Morcillo, A.; Vilela, M.M.D.S.; da Silva, M.T.N. Abnormalities in body composition and nutritional status in HIV-infected children and adolescents on antiretroviral therapy. Int. J. STD AIDS 2011, 22, 453–456. [Google Scholar] [CrossRef] [PubMed]
- Nielsen-Saines, K. Neuroscience and Biobehavioral Reviews Perinatal HIV as an infectious cause of developmental regression. Neurosci. Biobehav. Rev. 2019, 102, 417–423. [Google Scholar] [CrossRef]
- Brown, R.J.; Araujo-Vilar, D.; Cheung, P.T.; Dunger, P.D.; Garg, A.; Jack, M.; Mungai, L.; Oral, E.A.; Patni, N.; Rother, K.I.; et al. The diagnosis and management of lipodystrophy syndromes: A multi-society practice guideline. J. Clin. Endocrinol. Metab. 2016, 101, 4500–4511. [Google Scholar] [CrossRef] [PubMed]
- Innes, S.; Abdullah, K.L.; Haubrich, R.; Cotton, M.F.; Browne, S.H. High prevalence of dyslipidemia and insulin resistance in HIV-infected prepubertal African children on antiretroviral therapy. Pediatr. Infect. Dis. J. 2016, 35, e1–e7. [Google Scholar] [CrossRef] [Green Version]
- Almeida, F.J.; Kochi, C.; Aurélio, M.; Sáfadi, P. Influence of the antiretroviral therapy on the growth pattern of children and adolescents living with HIV/AIDS. J. Pediatr. 2019, 95, 95–101. [Google Scholar] [CrossRef]
- Barlow-Mosha, L.; Eckard, A.R.; McComsey, G.A.; Musoke, P.M. Metabolic complications and treatment of perinatally HIV-infected children and adolescents. J. Int. AIDS Soc. 2013, 16, 1–11. [Google Scholar] [CrossRef]
- Da Silva Pontes, L.; Callegari, B.; Magno, L.; Moraes, A.; Silva, B.G.; Manso, K.; Barros, B.; Araújo, A.P.; Silva, M.C.; Dias, G.A.; et al. Variations in plantar pressure and balance in HIV-infected children in antiretroviral therapy. Sci. Rep. 2019, 9, 1–7. [Google Scholar] [CrossRef]
- Mugisha, J.; Kinyanda, E.; Osafo, J.; Nalukenge, W.; Knizek, B.L. Health care professionals’ perspectives on barriers to treatment seeking for formal health services among orphan children and adolescents with HIV/AIDS and mental distress in a rural district in central, Uganda. Child Adolesc. Psychiatry Ment. Health 2020, 14, 1–10. [Google Scholar] [CrossRef]
- Mabaso, M.L.H.; Zungu, N.P.; Rehle, T.; Moyo, S.; Jooste, S.; Zuma, K. Determinants of excellent/good self-rated health among HIV positive individuals in South Africa: Evidence from a 2012 nationally representative household survey. BMC Public Health 2018, 18, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Somarriba, G.; Lopez-Mitnik, G.; Ludwig, D.A.; Neri, D.; Schaefer, N.; Lipshultz, S.E.; Scott, G.B.; Miller, T.L. Physical fitness in children infected with the human immunodeficiency virus: Associations with highly active antiretroviral therapy. AIDS Res. Hum. Retrovir. 2013, 29, 112–120. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martín-Cañavate, R.; Sonego, M.; Sagrado, M.J.; Escobar, G.; Rivas, E.; Ayala, S.; Castañeda, L.; Aparicio, P.; Custodio, E. Dietary patterns and nutritional status of HIV-infected children and adolescents in El Salvador: A cross-sectional study. PLoS ONE 2018, 13, e0196380. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brasil. Ministério da Saúde. Available online: http://indicadores.aids.gov.br/ (accessed on 19 August 2020).
- Sounis, E. Bio Estatística: Princípios Fundamentais, Metodologia Estatística. Aplicação às Ciências Biológicas; McGraw-Hill: Sao Paulo, Brazil, 1971; 228p. [Google Scholar]
- Brasil. Ministério da Saúde. Uso dos Formulários e Registro das Informações no Novo Sistema Informatizado da Vigilância Alimentar e Nutricional. Available online: http://189.28.128.100/nutricao/docs/geral/informe_sisvan_web_040608.pdf (accessed on 19 August 2020).
- Institute of Medicine (US) Subcommittee on Interpretation and Uses of Dietary Reference Intakes; Institute of Medicine (US) Standing Committee on the Scientific Evaluation of Dietary Reference Intakes. DRI Dietary Reference Intakes: Applications in Dietary Assessment; National Academies Press: Washington, DC, USA, 2000. [CrossRef]
- Padovani, R.M.; Amaya-Farfán, J.; Colugnati, F.A.B.; Domene, S.M.-Á. Dietary reference intakes: Aplicabilidade das tabelas em estudos nutricionais. Rev. Nutr. 2006, 19, 741–760. [Google Scholar] [CrossRef] [Green Version]
- Guedes, D.P. Manual Prático para Avaliação em Educação Física, 1st ed.; Editora Manole Ltda: Sao Paolo, Brazil, 2006; pp. 1–484. [Google Scholar]
- Malina, R.M.; Bouchard, C. Atividade Física do Atleta Jovem: Do Crescimento à Maturação; Editora Roca: Sao Paolo, Brazil, 2002; pp. 1–496. [Google Scholar]
- Cabral, S.; Cabral, B.; Pinto, V.M.C.; de Andrade, R.D. Relationship between bone age and anthropometry and physical fitness in young volleyball players. Braz. J. Sport Sci. 2016, 38, 69–75. [Google Scholar]
- Mirwald, R.L.; Baxter-Jones, A.D.G.; Bailey, D.A.; Beunen, G.P. An assessment of maturity from anthropometric measurements. Med. Sci. Sports Exerc. 2002, 34, 689–694. [Google Scholar]
- Leonard, C.M.; Roza, M.A.; Barr, R.D.; Webber, C.E. Reproducibility of DXA measurements of bone mineral density and body composition in children. Pediatr. Radiol. 2009, 39, 148–154. [Google Scholar] [CrossRef]
- Brasil. Ministério da Saúde. Guia Alimentar para a População Brasileira. Available online: https://www.fsp.usp.br/nupens/o-que-e-o-guia-alimentar/ (accessed on 10 August 2019).
- Miller, G.A.; Chapman, J.P. Misunderstanding analysis of covariance. J. Abnorm. Psychol. 2001, 110, 40. [Google Scholar] [CrossRef]
- Landau, S. A Handbook of Statistical Analyses Using SPSS, 1st ed.; Chapman & Hall: New York, NY, USA, 2019; pp. 1–366. [Google Scholar]
- Précoma, D.B.; De Oliveira, G.M.M.; Simão, A.F.; Dutra, O.P.; Coelho, O.R.; Izar, M.C.D.O.; Póvoa, R.M.D.S.; Giuliano, I.D.C.B.; Filho, A.C.D.A.; Machado, C.A.; et al. Updated Cardiovascular Prevention Guideline of the Brazilian Society of Cardiology—2019. Arq. Bras. Cardiol. 2019, 113, 787–891. [Google Scholar] [CrossRef] [PubMed]
- Sonego, M.; Sagrado, M.J.; Escobar, G.; Lazzerini, M.; Rivas, E.; Martín-Cañavate, R.; Perez de Lopes, E.; Ayala, S.; Castaneda, L.; Aparicio, P.; et al. Dyslipidemia, diet and physical exercise in children on treatment with antiretroviral medication in El Salvador: A cross-sectional study. Pediatr. Infect. Dis. J. 2016, 35, 1111–1116. [Google Scholar] [CrossRef] [Green Version]
- Spoulou, V.; Kanaka-Gantenbein, C.; Bathrellou, I.; Mora, S.; Mostrou, G.; Sidossis, L.; Chrousos, G.; Theodoridou, M. Monitoring of lipodystrophic and metabolic abnormalities in HIV-1 infected children on antiretroviral therapy. Hormones 2011, 10, 149–155. [Google Scholar] [CrossRef] [Green Version]
- Alfaro, M.P.; Siegel, R.M.; Baker, R.C.; Heubi, J.E. Resting energy expenditure and body composition in pediatric HIV infection. Pediatr. AIDS HIV Infect. 1995, 6, 276–280. [Google Scholar]
- Shiau, S.; Webber, A.; Strehlau, R.; Patel, F.; Coovadia, A.; Kozakowski, S.; Brodlie, S.; Yin, M.T.; Kuhn, L.; Arpadi, S.M. Dietary Inadequacies in HIV-infected and Uninfected School-aged Children in Johannesburg, South Africa. J. Pediatr. Gastroenterol. Nutr. 2017, 65, 332–337. [Google Scholar] [CrossRef]
- Hillesheim, E.; Lima, L.R.A.; Silva, R.C.R.; Trindade, E.B.S.M. Dietary intake and nutritional status of HIV-1-infected children and adolescents in Florianopolis, Brazil. Int. J. STD AIDS 2014, 25, 439–447. [Google Scholar] [CrossRef]
- Nkengfack Nembongwe, G.S.; Englert, H. Chapter 9—Antioxidants in HIV in Africa: Supplements, Local Diet, and Education. In HIV/AIDS; Academic Press: Cambridge, MA, USA, 2018; pp. 95–106. [Google Scholar]
- Duggal, S.; Das Chugh, T.; Duggal, A.K. HIV and malnutrition: Effects on immune system. Clin. Dev. Immunol. 2012, 2012, 784740. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, L.F.; Latorre, M.D.R.D.D.O.; Da Silva, A.M.; Konstantyner, T.C.R.D.O.; Peres, S.V.; Marques, H.H.D.S. Alta prevalência de sedentarismo em adolescentes que vivem com HIV/AIDS. Rev. Paul. Pediatr. 2015, 33, 327–332. [Google Scholar] [CrossRef] [Green Version]
- Ssewanyana, D.; Abubakar, A.; van Baar, A.; Mwangala, P.N.; Newton, C.R. Perspectives on Underlying Factors for Unhealthy Diet and Sedentary Lifestyle of Adolescents at a Kenyan Coastal Setting. Front. Public Health 2018, 6, 11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guimarães, N.S.; Fausto, M.A.; Tupinambás, U. Prevalência de excesso de peso, obesidade central e risco de comorbidades metabólicas em adultos com HIV/AIDS sem terapia antirretroviral. Rev. Bras. Promoção Saúde 2016, 29, 399–405. [Google Scholar] [CrossRef] [Green Version]
- Da Silva Cunha de Medeiros, R.C.; dos Santos, I.K.; de Oliveira, A.L.V.; de Goes, C.J.D.; de Medeiros, J.A.; da Silva, T.A.L.; de Souza Araujo, J.; de Alcântara Varela, P.W.; Cobucci, R.N.; de Araújo Tinoco Cabral, B.G.; et al. Comparison of Muscle Strength, Aerobic Capacity and Body Composition between Healthy Adolescents and Those Living with HIV: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2021, 18, 5675. [Google Scholar] [CrossRef]
- Medeiros, R.C.S.C.; Santos, I.K.; Damasceno de Goes, C.J.; Vasconcelos de Oliveira, A.L.; Medeiros, J.A.; Cobucci, R.N.; Dantas, P.M.S. A comparative analysis of physical fitness of children and adolescents with HIV infection: A systematic review protocol. Medicine 2019, 98, 1–4. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Subject No. | Educational Stage | Per Capita Income (Brazilian Currency) | CD4 (Cells/mm3) | ART (Years) | Therapy |
|---|---|---|---|---|---|
| C1 | First grade | 360.00 | 855 | 6 | AZT/3TC/NVP |
| C3 | First grade | 159.00 | 451 | 2 | AZT/3TC/EFZ |
| C4 | Fifth grade | 238.50 | 1.038 | 11 | 3TC/AZT/LPV/r |
| C5 | Preschool | 181.30 | 1.709 | 5 | AZT |
| C6 | First grade | 238.50 | 2.372 | 6 | LPV/r/AZT/3TC |
| C7 | Tenth grade | 1192.50 | 147 | 1 | TDF/3TC/LPV |
| C8 | Sixth grade | 381.60 | 955 | 14 | 3TC/TDF/LPV |
| C9 | Ninth grade | 381.60 | 1.326 | 17 | 3TC/ITRN/IP/II |
| C10 | Tenth grade | 545.10 | 585 | 15 | TDF/3TC/LPV |
| C11 | First grade | 190.80 | 282 | 0 | AZT/LMP/EFZ |
| C12 | Second grade | 572.40 | 366 | 1 | AZT/3TC/EFZ |
| C13 | Fifth grade | 715.50 | 799 | 6 | 3TC/AZT/NVP |
| C14 | Seventh grade | 175.00 | 1.060 | 9 | AZT/3TC/EFZ |
| C15 | Fourth grade | 190.80 | NI | 11 | AZT/3TC/LPV |
| C16 | Second grade | 106.00 | 3.365 | 3 | AZT/3TC/EFZ |
| C17 | Third grade | 159.00 | 507 | 1 | AZT/3TC/EFZ |
| C18 | Sixth grade | 477.00 | 545 | 14 | TDF/3TC/LPV |
| C19 | Third grade | 17.50 | 767 | 2 | AZT/3TC/EFZ |
| Variables | Analyses | ||
|---|---|---|---|
| 1 | 2 | 3 | |
| Height (m) | 1.40 ± 0.20 | 1.42 ± 0.22 | 1.47 ± 0.10 |
| Body weight (kg) | 32.2 ± 12.4 | 34.0 ± 14.0 | * 39.6 ± 9.57 |
| Body mass index (kg/m2) | 15.6 ± 2.10 | 15.6 ± 2.33 | 18.1 ± 2.75 |
| Total F (%) | 24.5 ± 6.13 | 22.2 ± 5.06 | 21.4 ± 9.92 |
| Fat free mass (kg) | 21.2 ± 9.44 | 20.0 ± 12.8 | 20.0 ± 11.4 |
| Bone mineral density (g/cm2) | 0.78 ± 0.18 | 0.71 ± 0.33 | 0.67 ± 0.28 |
| Physical activity index at school | 2.30 ± 0.57 | 2.47 ± 0.55 | 2.48 ± 0.45 |
| Physical activity index active leisure | 2.42 ± 1.31 | 2.45 ± 1.07 | 2.31 ± 1.01 |
| Index of physical activity in free time | 2.52 ± 0.53 | 1.57 ± 0.83 | 2.57 ± 0.67 |
| Habitual physical activity index | 7.23 ± 2.04 | 7.46 ± 2.05 | 7.35 ± 1.63 |
| Resting metabolic rate (Kcal/day) | 0.79 ± 0.20 | * 0.57 ± 0.45 | * 0.62 ± 0.42 |
| Variables | Analyses | F(2.0) | η2p | p | ||
|---|---|---|---|---|---|---|
| 1 | 2 | 3 | ||||
| Glucose (mg/dL) | § 76.8 ± 36.4 | 64.5 ± 42.1 | 62.7 ± 33.9 | 0.16 | 0.50 | 0.007 |
| Triglycerides (mg/dL) | Ϟ 85.4 ± 61.3 | 44.7 ± 49.5 | 56.6 ± 41.9 | 4.53 | 0.60 | 0.01 |
| Total cholesterol (mg/dL) | 116.0 ± 67.6 | 96.4 ± 79.9 | 111.4 ± 64.6 | 1.84 | 0.38 | 0.2 |
| HDL-C (mg/dL) | 27.4 ± 23.5 | 26.0 ± 21.0 | 31.4 ± 19.6 | 0.29 | 0.08 | 0.62 |
| LDL-C (mg/dL) | 55.4 ± 45.8 | 47.9 ± 54.5 | # 68.7 ± 46.8 | 10.7 | 0.78 | 0.04 |
| Urea (mg/dL) | 11.2 ± 7.60 | 12.2 ± 11.1 | # 17.3 ± 9.84 | 11.7 | 0.79 | 0.04 |
| Creatinine (mg/dL) | 0.50 ± 0.34 | ư 0.56 ± 0.28 | 0.43 ± 0.27 | 36.8 | 0.92 | 0.01 |
| Variables | Analyses | F(2.0) | η2p | p | ||
|---|---|---|---|---|---|---|
| 1 | 2 | 3 | ||||
| ETEV: (Kcal) | 1942.6 ± 459.9 | 1570.7 ± 928.0 | 1977.1 ± 548.7 | 1.67 | 0.12 | 0.2 |
| KCAL CONSUMED | 1900.5 ± 507.5 | 1449.5 ± 1013.0 | 17995 ± 503.9 | 1.00 | 0.10 | 0.1 |
| Did not reach ETEV: | 94.5% | 77.8% | 90% | ----- | ----- | ----- |
| >ETEV: | 27.8% | 33.3% | 30% | ----- | ----- | ----- |
| <ETEV: | 66.7% | 44.5% | 60% | ----- | ----- | ----- |
| Proteins | 70.4 ± 19.3 | 54.8 ± 39.8 | 79.0 ± 24.0 | 1.38 | 0.10 | 0.4 |
| %_PROT | 14.5 ± 4.27 | 12.5 ± 6.68 | 17.8 ± 3.29 | 1.91 | 0.13 | 0.1 |
| Lipids | 56.9 ± 16.0 | 52.5 ± 43.1 | 51.9 ± 21.3 | 4.21 | 0.26 | 0.06 |
| %_LIP | 27.2 ± 3.41 | 21.8 ± 15.6 | 26.2 ± 5.86 | 2.11 | 0.15 | 0.1 |
| Carbohydrates | 271.4 ± 84.5 | 178.6 ± 127.3 | 252.3 ± 77.3 | 0.84 | 0.06 | 0.3 |
| %_CARB | 57.1 ± 4.28 | 44.0 ± 23.4 | 56.0 ± 5.91 | 1.00 | 0.07 | 0.33 |
| Total cholesterol (mg) | 251.1 ± 114.3 | 241.6 ± 224.7 | 247.6 ± 94.4 | 0.07 | 0.00 | 0.7 |
| Fibers (g) | 18.6 ± 7.01 | 12.2 ± 7.36 | 15.1 ± 6.18 | 0.01 | 0.00 | 0.9 |
| <DRI | 88.9% | 100% | 100% | ----- | ----- | ----- |
| Calcium (mg) | 480.4 ± 258.8 | 386.3 ± 320.3 | 382.8 ± 297.5 | 0.02 | 0.00 | 0.8 |
| <DRI | 94.45% | 88.9% | 100% | ----- | ----- | ----- |
| Magnesium (mg) | 156.5 ± 59.4 | 118.6 ± 75.4 | 173.9 ± 47.8 | 0.00 | 0.00 | 0.9 |
| <DRI | 83.33% | 77.79% | 50% | ----- | ----- | ----- |
| Phosphorus (mg) | 1508.6 ± 2134.6 | 784.6 ± 586.1 | 1002.3 ± 495.9 | 0.36 | 0.02 | 0.5 |
| <DRI | 61.10% | 44.45% | 40% | ----- | ----- | ----- |
| Iron (mg) | 7.11 ± 3.25 | 5.90 ± 3.94 | 9.18 ± 3.86 | 2.59 | 0.17 | 0.1 |
| <DRI | 100% | 88.89% | 60% | ----- | ----- | ----- |
| Potassium (mg) | 1675.7 ± 394.3 | 1272.9 ± 842.4 | 1807.1 ± 539.3 | 2.13 | 0.15 | 0.16 |
| <DRI | 100% | 100% | 100% | ----- | ----- | ----- |
| Zinc (mg) | 7.14 ± 3.61 | 6.32 ± 4.59 | 10.1 ± 5.35 | 0.11 | 0.00 | 0.7 |
| <DRI | 61.11% | 44.45% | 20% | ----- | ----- | ----- |
| Variables | Analyses | F(2.0) | η2p | p | ||
|---|---|---|---|---|---|---|
| 1 | 2 | 3 | ||||
| Raw Salad | 0.56 ± 0.78 | 0.73 ± 1.27 | 1.00 ± 2.00 | 1.06 | 0.05 | 0.3 |
| Vegetables | 1.50 ± 1.75 | 1.73 ± 2.76 | 1.40 ± 2.22 | 0.01 | 0.00 | 0.9 |
| Fruit | 2.94 ± 2.85 | 2.45 ± 3.04 | # 3.70 ± 2.86 | 5.04 | 0.22 | 0.03 |
| Bean | 4.67 ± 2.74 | 3.09 ± 3.04 | 4.10 ± 3.54 | 0.00 | 0.00 | 0.9 |
| Milk and dairy products | 3.94 ± 3.09 | 2.64 ± 3.17 | 4.10 ± 2.68 | 0.07 | 0.00 | 0.7 |
| Frying | 1.61 ± 2.47 | 0.64 ± 1.20 | 1.40 ± 2.06 | 0.00 | 0.00 | 0.9 |
| Embedded Foods | 2.33 ± 1.97 | 1.64 ± 2.15 | 1.70 ± 1.63 | 0.10 | 0.00 | 0.7 |
| Salty | 2.56 ± 2.87 | 1.27 ± 1.48 | 2.20 ± 2.34 | 1.95 | 0.10 | 0.1 |
| Candy | 2.28 ± 2.49 | 1.18 ± 2.13 | 2.10 ± 2.80 | 0.00 | 0.00 | 0.9 |
| Soft drinks | ° 1.44 ± 1.38 | 0.55 ± 0.82 | ° 1.43 ± 1.50 | 5.72 | 0.25 | 0.02 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
de Medeiros, R.C.d.S.C.; da Silva, T.A.L.; de Oliveira, A.L.V.; de Almeida-Neto, P.F.; de Medeiros, J.A.; Bulhões-Correia, A.; Micussi, F.A.; Ururahy, M.A.G.; de Araújo Tinoco Cabral, B.G.; Dantas, P.M.S. Influence of Healthy Habits Counseling on Biochemical and Metabolic Parameters in Children and Adolescents with HIV: Longitudinal Study. Nutrients 2021, 13, 3237. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13093237
de Medeiros RCdSC, da Silva TAL, de Oliveira ALV, de Almeida-Neto PF, de Medeiros JA, Bulhões-Correia A, Micussi FA, Ururahy MAG, de Araújo Tinoco Cabral BG, Dantas PMS. Influence of Healthy Habits Counseling on Biochemical and Metabolic Parameters in Children and Adolescents with HIV: Longitudinal Study. Nutrients. 2021; 13(9):3237. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13093237
Chicago/Turabian Stylede Medeiros, Rafaela Catherine da Silva Cunha, Tatiane Andreza Lima da Silva, Anna Luiza Vasconcelos de Oliveira, Paulo Francisco de Almeida-Neto, Jason Azevedo de Medeiros, Alexandre Bulhões-Correia, Francisco Americo Micussi, Marcela Abbott Galvao Ururahy, Breno Guilherme de Araújo Tinoco Cabral, and Paulo Moreira Silva Dantas. 2021. "Influence of Healthy Habits Counseling on Biochemical and Metabolic Parameters in Children and Adolescents with HIV: Longitudinal Study" Nutrients 13, no. 9: 3237. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13093237