
Dietary Copper and Selenium Intakes and the Risk of Type 2 Diabetes Mellitus: Findings from the China Health and Nutrition Survey


Abstract
:1. Introduction
2. Materials and Methods
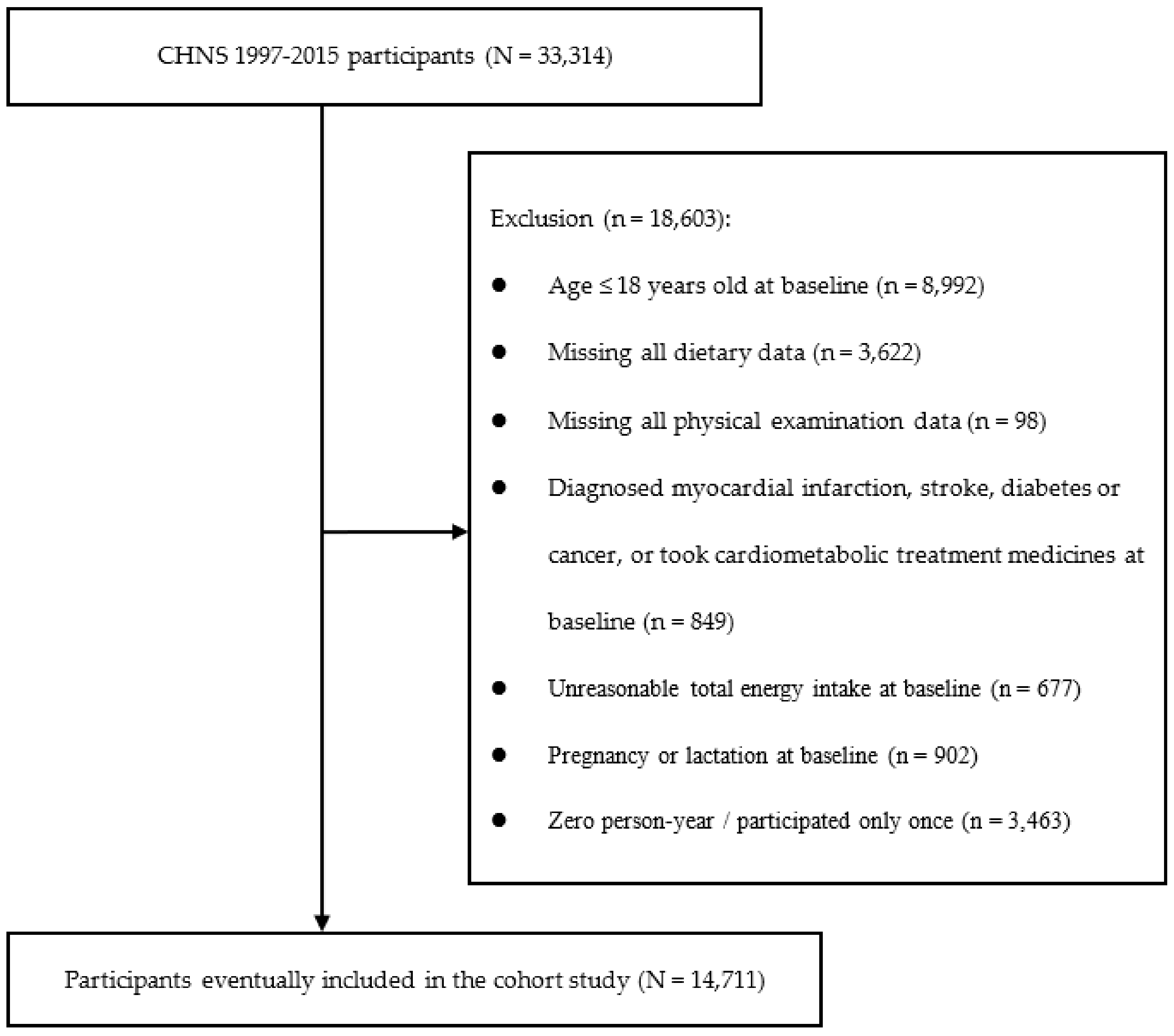
2.1. Study Population
2.2. Dietary Assessment
2.3. Assessment of T2DM
2.4. Assessment of Other Covariates
2.5. Statistical Analysis
3. Results
3.1. Sociodemographic, Anthropometric and Lifestyle Characteristics of Study Participants at Baseline
3.2. Food Sources of Dietary Cu and Se Intakes
3.3. Associations between Dietary Cu and Se Intakes and Risk of T2DM
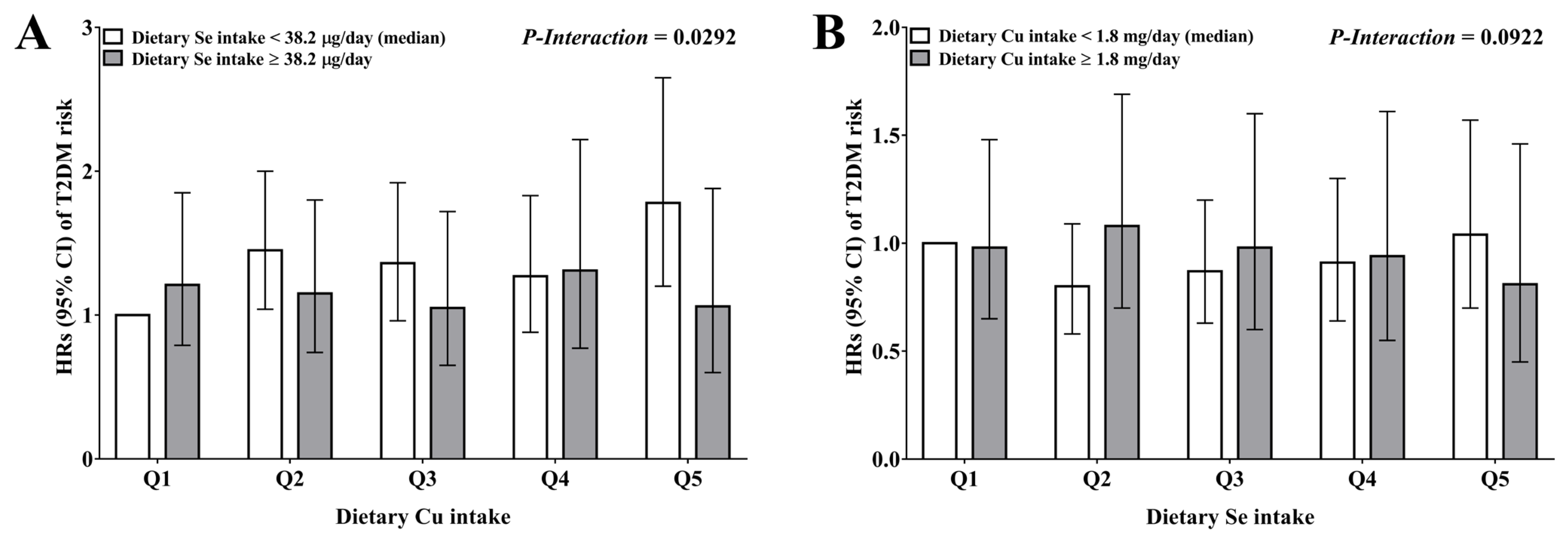
3.4. Associations between Dietary Cu and Se Intakes and Risk of T2DM Based on Potential Effect Modifiers
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Wang, L.; Peng, W.; Zhao, Z.; Zhang, M.; Shi, Z.; Song, Z.; Zhang, X.; Li, C.; Huang, Z.; Sun, X.; et al. Prevalence and Treatment of Diabetes in China, 2013–2018. JAMA 2021, 326, 2498–2506. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Wang, D.D.; Ley, S.H.; Vasanti, M.; Howard, A.G.; He, Y.; Hu, F.B. Time Trends of Dietary and Lifestyle Factors and Their Potential Impact on Diabetes Burden in China. Diabetes Care 2017, 40, 1685–1694. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dubey, P.; Thakur, V.; Chattopadhyay, M. Role of Minerals and Trace Elements in Diabetes and Insulin Resistance. Nutrients 2020, 12, 1864. [Google Scholar] [CrossRef] [PubMed]
- Kaur, B.; Henry, J. Micronutrient status in type 2 diabetes: A review. Adv. Food Nutr. Res. 2014, 71, 55–100. [Google Scholar] [CrossRef] [PubMed]
- Ferns, G.A.; Lamb, D.J.; Taylor, A. The possible role of copper ions in atherogenesis: The Blue Janus. Atherosclerosis 1997, 133, 139–152. [Google Scholar] [CrossRef]
- Mohammadifard, N.; Humphries, K.H.; Gotay, C.; Mena-Sánchez, G.; Salas-Salvadó, J.; Esmaillzadeh, A.; Ignaszewski, A.; Sarrafzadegan, N. Trace minerals intake: Risks and benefits for cardiovascular health. Crit. Rev. Food Sci. Nutr. 2019, 59, 1334–1346. [Google Scholar] [CrossRef] [PubMed]
- Qiu, Q.; Zhang, F.; Zhu, W.; Wu, J.; Liang, M. Copper in Diabetes Mellitus: A Meta-Analysis and Systematic Review of Plasma and Serum Studies. Biol. Trace Elem. Res. 2017, 177, 53–63. [Google Scholar] [CrossRef]
- Eshak, E.S.; Iso, H.; Maruyama, K.; Muraki, I.; Tamakoshi, A. Associations between dietary intakes of iron, copper and zinc with risk of type 2 diabetes mellitus: A large population-based prospective cohort study. Clin. Nutr. 2018, 37, 667–674. [Google Scholar] [CrossRef] [Green Version]
- Tsugane, S. Why has Japan become the world’s most long-lived country: Insights from a food and nutrition perspective. Eur. J. Clin. Nutr. 2021, 75, 921–928. [Google Scholar] [CrossRef]
- Zhang, J.; Wang, H.; Wang, Z.; Huang, F.; Zhang, X.; Du, W.; Su, C.; Ouyang, Y.; Li, L.; Bai, J.; et al. Trajectories of Dietary Patterns and Their Associations with Overweight/Obesity among Chinese Adults: China Health and Nutrition Survey 1991–2018. Nutrients 2021, 13, 2835. [Google Scholar] [CrossRef]
- Yang, Y.; Ge, K. Encyclopedia of Nutrition Science, 2nd ed.; People’s Medical Publishing House: Beijing, China, 2019; Volume I. [Google Scholar]
- Steinbrenner, H.; Duntas, L.H.; Rayman, M.P. The role of selenium in type-2 diabetes mellitus and its metabolic comorbidities. Redox Biol. 2022, 50, 102236. [Google Scholar] [CrossRef] [PubMed]
- Mita, Y.; Nakayama, K.; Inari, S.; Nishito, Y.; Yoshioka, Y.; Sakai, N.; Sotani, K.; Nagamura, T.; Kuzuhara, Y.; Inagaki, K.; et al. Selenoprotein P-neutralizing antibodies improve insulin secretion and glucose sensitivity in type 2 diabetes mouse models. Nat. Commun. 2017, 8, 1658. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.D.; Vatamaniuk, M.Z.; Wang, S.K.; Roneker, C.A.; Simmons, R.A.; Lei, X.G. Molecular mechanisms for hyperinsulinaemia induced by overproduction of selenium-dependent glutathione peroxidase-1 in mice. Diabetologia 2008, 51, 1515–1524. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Misu, H.; Takamura, T.; Takayama, H.; Hayashi, H.; Matsuzawa-Nagata, N.; Kurita, S.; Ishikura, K.; Ando, H.; Takeshita, Y.; Ota, T.; et al. A liver-derived secretory protein, selenoprotein P, causes insulin resistance. Cell Metab. 2010, 12, 483–495. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vinceti, M.; Filippini, T.; Wise, L.A.; Rothman, K.J. A systematic review and dose-response meta-analysis of exposure to environmental selenium and the risk of type 2 diabetes in nonexperimental studies. Environ. Res. 2021, 197, 111210. [Google Scholar] [CrossRef]
- Vinceti, M.; Filippini, T.; Rothman, K.J. Selenium exposure and the risk of type 2 diabetes: A systematic review and meta-analysis. Eur. J. Epidemiol. 2018, 33, 789–810. [Google Scholar] [CrossRef]
- Stranges, S.; Sieri, S.; Vinceti, M.; Grioni, S.; Guallar, E.; Laclaustra, M.; Muti, P.; Berrino, F.; Krogh, V. A prospective study of dietary selenium intake and risk of type 2 diabetes. BMC Public Health 2010, 10, 564. [Google Scholar] [CrossRef] [Green Version]
- Vinceti, M.; Bonaccio, M.; Filippini, T.; Costanzo, S.; Wise, L.A.; Di Castelnuovo, A.; Ruggiero, E.; Persichillo, M.; Cerletti, C.; Donati, M.B.; et al. Dietary selenium intake and risk of hospitalization for type 2 diabetes in the Moli-sani study cohort. Nutr. Metab. Cardiovasc. Dis. 2021, 31, 1738–1746. [Google Scholar] [CrossRef]
- Wei, J.; Zeng, C.; Gong, Q.Y.; Yang, H.B.; Li, X.X.; Lei, G.H.; Yang, T.B. The association between dietary selenium intake and diabetes: A cross-sectional study among middle-aged and older adults. Nutr. J. 2015, 14, 18. [Google Scholar] [CrossRef] [Green Version]
- Siddiqi, S.M.; Sun, C.; Wu, X.; Shah, I.; Mehmood, A. The Correlation between Dietary Selenium Intake and Type 2 Diabetes: A Cross-Sectional Population-Based Study on North Chinese Adults. Biomed. Res. Int. 2020, 2020, 8058463. [Google Scholar] [CrossRef]
- Popkin, B.M.; Du, S.; Zhai, F.; Zhang, B. Cohort Profile: The China Health and Nutrition Survey—Monitoring and understanding socio-economic and health change in China, 1989–2011. Int. J. Epidemiol. 2010, 39, 1435–1440. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, B.; Zhai, F.Y.; Du, S.F.; Popkin, B.M. The China Health and Nutrition Survey, 1989–2011. Obes. Rev. 2014, 15 (Suppl. 1), 2–7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, L.; Wang, H.; Zhang, B.; Popkin, B.M.; Du, S. Elevated Fat Intake Increases Body Weight and the Risk of Overweight and Obesity among Chinese Adults: 1991–2015 Trends. Nutrients 2020, 12, 3272. [Google Scholar] [CrossRef]
- Zhao, J.; Zuo, L.; Sun, J.; Su, C.; Wang, H. Trends and Urban-Rural Disparities of Energy Intake and Macronutrient Composition among Chinese Children: Findings from the China Health and Nutrition Survey (1991 to 2015). Nutrients 2021, 13, 1933. [Google Scholar] [CrossRef] [PubMed]
- Yu, D.; Zhang, X.; Xiang, Y.B.; Yang, G.; Li, H.; Gao, Y.T.; Zheng, W.; Shu, X.O. Adherence to dietary guidelines and mortality: A report from prospective cohort studies of 134,000 Chinese adults in urban Shanghai. Am. J. Clin. Nutr. 2014, 100, 693–700. [Google Scholar] [CrossRef] [Green Version]
- Zhai, F.Y.; Du, S.F.; Wang, Z.H.; Zhang, J.G.; Du, W.W.; Popkin, B.M. Dynamics of the Chinese diet and the role of urbanicity, 1991-2011. Obes. Rev. 2014, 15 (Suppl. 1), 16–26. [Google Scholar] [CrossRef] [Green Version]
- Zhai, F.; Guo, X.; Popkin, B. Evaluation of the 24-Hour Individual Recall Method in China. Food Nutr. Bull. 1996, 17, 154–461. [Google Scholar] [CrossRef] [Green Version]
- Wang, G. Food Composition Table (National Representative Values); People’s Medical Publishing House: Beijing, China, 1991. [Google Scholar]
- Yang, Y.; Wang, G.; Pan, X. China Food Composition Table 2002; Peking University Medical Press: Beijing, China, 2002. [Google Scholar]
- Yang, Y.; He, M.; Pan, X. China Food Composition Table 2004; Peking University Medical Press: Beijing, China, 2004. [Google Scholar]
- Yang, Y.; Wang, G.; Pan, X. China Food Composition Table, 2nd ed.; Peking University Medical Press: Beijing, China, 2009. [Google Scholar]
- Willett, W.; Stampfer, M.J. Total energy intake: Implications for epidemiologic analyses. Am. J. Epidemiol. 1986, 124, 17–27. [Google Scholar] [CrossRef]
- Dodd, H.; Williams, S.; Brown, R.; Venn, B. Calculating meal glycemic index by using measured and published food values compared with directly measured meal glycemic index. Am. J. Clin. Nutr. 2011, 94, 992–996. [Google Scholar] [CrossRef]
- Atkinson, F.S.; Foster-Powell, K.; Brand-Miller, J.C. International tables of glycemic index and glycemic load values: 2008. Diabetes Care 2008, 31, 2281–2283. [Google Scholar] [CrossRef] [Green Version]
- Zhang, Y.; Zhuang, P.; Mao, L.; Chen, X.; Wang, J.; Cheng, L.; Ding, G.; Jiao, J. Current level of fish and omega-3 fatty acid intakes and risk of Type 2 diabetes in China. J. Nutr. Biochem. 2019, 74, 108249. [Google Scholar] [CrossRef] [PubMed]
- He, J.; Fang, A.; Yu, S.; Shen, X.; Li, K. Dietary Nonheme, Heme, and Total Iron Intake and the Risk of Diabetes in Adults: Results From the China Health and Nutrition Survey. Diabetes Care 2020, 43, 776–784. [Google Scholar] [CrossRef] [PubMed]
- Zhuang, P.; Mao, L.; Wu, F.; Wang, J.; Jiao, J.; Zhang, Y. Cooking Oil Consumption Is Positively Associated with Risk of Type 2 Diabetes in a Chinese Nationwide Cohort Study. J. Nutr. 2020, 150, 1799–1807. [Google Scholar] [CrossRef] [PubMed]
- Atkinson, M.A.; Eisenbarth, G.S.; Michels, A.W. Type 1 diabetes. Lancet 2014, 383, 69–82. [Google Scholar] [CrossRef] [Green Version]
- Patterson, C.C.; Dahlquist, G.G.; Gyürüs, E.; Green, A.; Soltész, G. Incidence trends for childhood type 1 diabetes in Europe during 1989–2003 and predicted new cases 2005–20: A multicentre prospective registration study. Lancet 2009, 373, 2027–2033. [Google Scholar] [CrossRef]
- Yan, S.; Li, J.; Li, S.; Zhang, B.; Du, S.; Gordon-Larsen, P.; Adair, L.; Popkin, B. The expanding burden of cardiometabolic risk in China: The China Health and Nutrition Survey. Obes. Rev. 2012, 13, 810–821. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Obesity. Available online: https://www.who.int/news-room/facts-in-pictures/detail/6-facts-on-obesity (accessed on 5 August 2021).
- Hu, Y.; Li, M.; Wu, J.; Wang, R.; Mao, D.; Chen, J.; Li, W.; Yang, Y.; Piao, J.; Yang, L.; et al. Prevalence and Risk Factors for Anemia in Non-pregnant Childbearing Women from the Chinese Fifth National Health and Nutrition Survey. Int. J. Environ. Res. Public Health 2019, 16, 1290. [Google Scholar] [CrossRef] [Green Version]
- Ng, S.W.; Norton, E.C.; Popkin, B.M. Why have physical activity levels declined among Chinese adults? Findings from the 1991-2006 China Health and Nutrition Surveys. Soc. Sci. Med. 2009, 68, 1305–1314. [Google Scholar] [CrossRef] [Green Version]
- Pan, A.; Sun, Q.; Bernstein, A.M.; Schulze, M.B.; Manson, J.E.; Willett, W.C.; Hu, F.B. Red meat consumption and risk of type 2 diabetes: 3 cohorts of US adults and an updated meta-analysis. Am. J. Clin. Nutr. 2011, 94, 1088–1096. [Google Scholar] [CrossRef]
- Hu, F.B.; Stampfer, M.J.; Rimm, E.; Ascherio, A.; Rosner, B.A.; Spiegelman, D.; Willett, W.C. Dietary fat and coronary heart disease: A comparison of approaches for adjusting for total energy intake and modeling repeated dietary measurements. Am. J. Epidemiol. 1999, 149, 531–540. [Google Scholar] [CrossRef] [Green Version]
- Bo, S.; Durazzo, M.; Gambino, R.; Berutti, C.; Milanesio, N.; Caropreso, A.; Gentile, L.; Cassader, M.; Cavallo-Perin, P.; Pagano, G. Associations of dietary and serum copper with inflammation, oxidative stress, and metabolic variables in adults. J. Nutr. 2008, 138, 305–310. [Google Scholar] [CrossRef] [PubMed]
- Sitasawad, S.; Deshpande, M.; Katdare, M.; Tirth, S.; Parab, P. Beneficial effect of supplementation with copper sulfate on STZ-diabetic mice (IDDM). Diabetes Res. Clin. Pract. 2001, 52, 77–84. [Google Scholar] [CrossRef]
- Weksler-Zangen, S.; Raz, I.; Lenzen, S.; Jörns, A.; Ehrenfeld, S.; Amir, G.; Oprescu, A.; Yagil, Y.; Yagil, C.; Zangen, D.H.; et al. Impaired glucose-stimulated insulin secretion is coupled with exocrine pancreatic lesions in the Cohen diabetic rat. Diabetes 2008, 57, 279–287. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Horn, D.; Barrientos, A. Mitochondrial copper metabolism and delivery to cytochrome c oxidase. IUBMB Life 2008, 60, 421–429. [Google Scholar] [CrossRef] [Green Version]
- Aharon-Hananel, G.; Romero-Afrima, L.; Saada, A.; Mantzur, C.; Raz, I.; Weksler-Zangen, S. Cytochrome c Oxidase Activity as a Metabolic Regulator in Pancreatic Beta-Cells. Cells 2022, 11, 929. [Google Scholar] [CrossRef]
- Vashchenko, G.; MacGillivray, R.T. Multi-copper oxidases and human iron metabolism. Nutrients 2013, 5, 2289–2313. [Google Scholar] [CrossRef] [Green Version]
- Kelley, D.S.; Daudu, P.A.; Taylor, P.C.; Mackey, B.E.; Turnlund, J.R. Effects of low-copper diets on human immune response. Am. J. Clin. Nutr. 1995, 62, 412–416. [Google Scholar] [CrossRef]
- Hoque, B.; Shi, Z. Association between selenium intake, diabetes and mortality in adults: Findings from National Health and Nutrition Examination Survey (NHANES) 2003–2014. Br. J. Nutr. 2022, 127, 1098–1105. [Google Scholar] [CrossRef]
- Pouresmaeil, V.; Al Abudi, A.H.; Mahimid, A.H.; Sarafraz Yazdi, M.; Es-Haghi, A. Evaluation of Serum Selenium and Copper Levels with Inflammatory Cytokines and Indices of Oxidative Stress in Type 2 Diabetes. Biol. Trace Elem. Res. 2022; Epub ahead of print. [Google Scholar] [CrossRef]
- Kasaikina, M.V.; Kravtsova, M.A.; Lee, B.C.; Seravalli, J.; Peterson, D.A.; Walter, J.; Legge, R.; Benson, A.K.; Hatfield, D.L.; Gladyshev, V.N. Dietary selenium affects host selenoproteome expression by influencing the gut microbiota. Faseb J. 2011, 25, 2492–2499. [Google Scholar] [CrossRef] [Green Version]
- Qin, J.; Li, Y.; Cai, Z.; Li, S.; Zhu, J.; Zhang, F.; Liang, S.; Zhang, W.; Guan, Y.; Shen, D.; et al. A metagenome-wide association study of gut microbiota in type 2 diabetes. Nature 2012, 490, 55–60. [Google Scholar] [CrossRef]
- Pedersen, H.K.; Gudmundsdottir, V.; Nielsen, H.B.; Hyotylainen, T.; Nielsen, T.; Jensen, B.A.; Forslund, K.; Hildebrand, F.; Prifti, E.; Falony, G.; et al. Human gut microbes impact host serum metabolome and insulin sensitivity. Nature 2016, 535, 376–381. [Google Scholar] [CrossRef] [PubMed]
- Stranges, S.; Marshall, J.R.; Natarajan, R.; Donahue, R.P.; Trevisan, M.; Combs, G.F.; Cappuccio, F.P.; Ceriello, A.; Reid, M.E. Effects of long-term selenium supplementation on the incidence of type 2 diabetes: A randomized trial. Ann. Intern. Med. 2007, 147, 217–223. [Google Scholar] [CrossRef] [PubMed]
- Algotar, A.M.; Hsu, C.H.; Singh, P.; Stratton, S.P. Selenium supplementation has no effect on serum glucose levels in men at high risk of prostate cancer. J. Diabetes 2013, 5, 465–470. [Google Scholar] [CrossRef] [Green Version]
- Karp, D.D.; Lee, S.J.; Keller, S.M.; Wright, G.S.; Aisner, S.; Belinsky, S.A.; Johnson, D.H.; Johnston, M.R.; Goodman, G.; Clamon, G.; et al. Randomized, double-blind, placebo-controlled.d, phase III chemoprevention trial of selenium supplementation in patients with resected stage I non-small-cell lung cancer: ECOG 5597. J. Clin. Oncol. 2013, 31, 4179–4187. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lippman, S.M.; Klein, E.A.; Goodman, P.J.; Lucia, M.S.; Thompson, I.M.; Ford, L.G.; Parnes, H.L.; Minasian, L.M.; Gaziano, J.M.; Hartline, J.A.; et al. Effect of selenium and vitamin E on risk of prostate cancer and other cancers: The Selenium and Vitamin E Cancer Prevention Trial (SELECT). JAMA 2009, 301, 39–51. [Google Scholar] [CrossRef] [Green Version]
- Thompson, P.A.; Ashbeck, E.L.; Roe, D.J.; Fales, L.; Buckmeier, J.; Wang, F.; Bhattacharyya, A.; Hsu, C.H.; Chow, H.H.; Ahnen, D.J.; et al. Selenium Supplementation for Prevention of Colorectal Adenomas and Risk of Associated Type 2 Diabetes. J. Natl. Cancer Inst. 2016, 108, djw152. [Google Scholar] [CrossRef]
- Huston, R.K.; Jelen, B.J.; Vidgoff, J. Selenium supplementation in low-birthweight premature infants: Relationship to trace metals and antioxidant enzymes. JPEN J. Parenter. Enter. Nutr. 1991, 15, 556–559. [Google Scholar] [CrossRef]
- Evans, D.M.; Zhu, G.; Dy, V.; Heath, A.C.; Madden, P.A.; Kemp, J.P.; McMahon, G.; St Pourcain, B.; Timpson, N.J.; Golding, J.; et al. Genome-wide association study identifies loci affecting blood copper, selenium and zinc. Hum. Mol. Genet. 2013, 22, 3998–4006. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Variables | All | Quintiles of Dietary Cu Intakes | Quintiles of Dietary Se Intakes | ||||
|---|---|---|---|---|---|---|---|
| Q1 | Q3 | Q5 | Q1 | Q3 | Q5 | ||
| N | 14,711 | 2942 | 2945 | 2942 | 2943 | 2943 | 2942 |
| Cu, mg/day | 1.9 ± 0.6 | 1.3 ± 0.2 | 1.8 ± 0.1 | 2.7 ± 0.9 | 1.8 ± 0.5 | 1.8 ± 0.5 | 2.0 ± 0.9 |
| Se, μg/day | 41.1 ± 17.6 | 38.8 ± 14.0 | 40.6 ± 16.6 | 44.8 ± 22.8 | 23.9 ± 4.5 | 38.2 ± 1.7 | 65.4 ± 22.9 |
| Age, years | 45 ± 15 | 47 ± 15 | 44 ± 15 | 44 ± 15 | 47 ± 16 | 44 ± 14 | 45 ± 15 |
| Male, n (%) | 7333 (49.8) | 1534 (52.1) | 1434 (48.7) | 1438 (48.9) | 1363 (46.3) | 1504 (51.1) | 1578 (53.6) |
| BMI, kg/m2 | 23.2 ± 3.3 | 23.5 ± 3.4 | 23.1 ± 3.4 | 23.3 ± 3.3 | 22.5 ± 3.4 | 23.3 ± 3.2 | 23.9 ± 3.5 |
| Urbanization index, n (%) | |||||||
| Low | 4902 (33.3) | 553 (18.8) | 1059 (36.0) | 1229 (41.8) | 1581 (53.7) | 940 (31.9) | 467 (15.9) |
| Medium | 4903 (33.3) | 1031 (35.0) | 1032 (35.0) | 788 (26.8) | 876 (29.8) | 1068 (36.3) | 869 (29.5) |
| High | 4906 (33.4) | 1358 (46.2) | 854 (29.0) | 925 (31.4) | 486 (16.5) | 935 (31.8) | 1606 (54.6) |
| Region, n (%) | |||||||
| Northern | 6112 (41.6) | 917 (31.2) | 1198 (40.7) | 1589 (54.0) | 946 (32.1) | 1118 (38.0) | 1630 (55.4) |
| Southern | 8589 (58.4) | 2025 (68.8) | 1747 (59.3) | 1353 (46.0) | 1997 (67.9) | 1825 (62.0) | 1312 (44.6) |
| Education level, n (%) | |||||||
| Primary | 6883 (46.8) | 1075 (36.5) | 1466 (49.8) | 1457 (49.5) | 1827 (62.1) | 1342 (45.6) | 917 (31.2) |
| Middle | 4188 (28.5) | 908 (30.9) | 848 (28.8) | 796 (27.1) | 733 (24.9) | 885 (30.1) | 884 (30.0) |
| High | 3640 (24.7) | 959 (32.6) | 631 (21.4) | 689 (23.4) | 383 (13.0) | 716 (24.3) | 1141 (38.8) |
| Alcohol intake, n (%) | |||||||
| No | 7647 (52.0) | 1618 (55.0) | 1485 (50.4) | 1556 (52.9) | 1695 (57.6) | 1469 (49.9) | 1463 (49.7) |
| Yes | 7064 (48.0) | 1324 (45.0) | 1460 (49.6) | 1386 (47.1) | 1248 (42.4) | 1474 (50.1) | 1479 (50.3) |
| Smoking status, n (%) | |||||||
| No | 9314 (63.3) | 1906 (64.8) | 1842 (62.5) | 1916 (65.1) | 1875 (63.7) | 1829 (62.1) | 1898 (64.5) |
| Yes | 5397 (36.7) | 1036 (35.2) | 1103 (37.5) | 1026 (34.9) | 1068 (36.3) | 1114 (37.9) | 1044 (35.5) |
| Physical activity status, METs-h/week | 103.2 ± 83.8 | 88.3 ± 77.0 | 106.2 ± 82.6 | 111.4 ± 90.5 | 126.0 ± 90.6 | 100.0 ± 82.5 | 82.1 ± 73.9 |
| Hypertension, n (%) | |||||||
| No | 11610 (78.9) | 2271 (77.2) | 2364 (80.3) | 2283 (77.6) | 2345 (79.7) | 2367 (80.4) | 2254 (76.6) |
| Yes | 3101 (21.1) | 671 (22.8) | 581 (19.7) | 659 (22.4) | 598 (20.3) | 576 (19.6) | 688 (23.4) |
| Total energy, kcal/day | 2104.6 ± 136.5 | 2027.5 ± 210.8 | 2125.9 ±95.8 | 2132.0 ± 88.1 | 2054.2 ± 200.7 | 2118.2 ± 113.6 | 2121.7 ± 104.7 |
| Protein, % energy | 12.3 ± 2.7 | 11.8 ± 3.5 | 12.0 ± 2.1 | 13.2 ± 2.8 | 10.5 ± 3.0 | 12.1 ± 1.7 | 14.5 ± 2.7 |
| Animal protein, % energy | 3.8 ± 2.7 | 4.5 ± 2.6 | 3.7 ± 2.4 | 3.4 ± 3.1 | 1.9 ± 1.5 | 3.8 ± 2.0 | 6.0 ± 3.2 |
| Plant protein, % energy | 7.7 ± 2.0 | 6.1 ± 1.8 | 7.8 ± 1.4 | 9.1 ± 2.2 | 7.8 ± 2.1 | 7.7 ± 1.9 | 7.5 ± 2.1 |
| Animal protein: plant protein ratio | 0.6 ± 3.7 | 1.0 ± 8.2 | 0.5 ± 0.5 | 0.5 ± 0.6 | 0.5 ± 8.2 | 0.6 ± 1.0 | 1.0 ± 0.8 |
| Fat, % energy | 31.7 ± 10.5 | 40.0 ± 11.4 | 30.2 ± 8.2 | 26.7 ± 9.9 | 29.2 ± 12.8 | 32.3 ± 9.8 | 33.6 ± 9.1 |
| SFA, % energy | 7.3 ± 3.0 | 9.6 ± 3.4 | 7.0 ± 2.3 | 5.8 ± 2.6 | 6.6 ± 3.5 | 7.5 ± 2.9 | 8.0 ± 2.6 |
| MUFA, % energy | 12.6 ± 5.3 | 16.8 ± 5.9 | 12.1 ± 4.1 | 9.8 ± 4.6 | 11.7 ± 6.3 | 12.9 ± 5.1 | 13.2 ± 4.6 |
| PUFA, % energy | 8.2 ± 4.2 | 9.4 ± 5.5 | 7.7 ± 3.6 | 7.8 ± 3.7 | 7.8 ± 5.3 | 8.3 ± 3.9 | 8.3 ± 3.6 |
| PUFA: SFA ratio | 1.3 ± 0.7 | 1.1 ± 0.6 | 1.2 ± 0.6 | 1.5 ± 0.7 | 1.4 ± 0.9 | 1.3 ± 0.6 | 1.1 ± 0.5 |
| Cholesterol, % energy | 0.07 ± 0.06 | 0.07 ± 0.06 | 0.06 ± 0.05 | 0.06 ± 0.06 | 0.04 ± 0.04 | 0.06 ± 0.05 | 0.10 ± 0.08 |
| Carbohydrate, % energy | 54.3 ± 11.0 | 46.4 ± 11.0 | 56.1 ± 9.2 | 58.2 ± 11.2 | 58.7 ± 12.4 | 54.0 ± 10.0 | 49.8 ± 9.9 |
| Fiber, g/day | 10.4 ± 5.0 | 7.2 ± 3.3 | 10.2 ± 4.1 | 13.9 ± 6.3 | 9.6 ± 4.8 | 10.0 ± 4.3 | 11.6 ± 6.5 |
| Dietary GI | 69.0 ± 6.7 | 68.0 ± 7.8 | 70.0 ± 5.6 | 68.0 ± 7.3 | 68.6 ± 7.0 | 69.3 ± 6.2 | 68.2 ± 7.4 |
| Nutrients | Food Sources | Median (IQR) |
|---|---|---|
| Dietary Cu intakes, mg/day | Grains and tubers | 0.98 (0.67, 1.32) |
| Vegetables, fruits, fungi, and algae | 0.23 (0.15, 0.35) | |
| Legumes | 0.15 (0.05, 0.30) | |
| Meat | 0.06 (0.02, 0.12) | |
| Ethnic foods, cakes, and fast food | 0.06 (0.02, 0.12) | |
| Condiments | 0.04 (0.01, 0.04) | |
| Eggs | 0.02 (0.01, 0.04) | |
| Fish and seafoods | 0.01 (0, 0.02) | |
| Others | 0 (0, 0.03) | |
| Dietary Se intakes, µg/day | Grains and tubers | 14.14 (9.66, 21.39) |
| Meat | 7.52 (3.20, 12.90) | |
| Eggs | 2.73 (0.80, 5.26) | |
| Vegetables, fruits, fungi, and algae | 2.05 (1.36, 2.96) | |
| Fish and seafoods | 1.29 (0, 5.94) | |
| Legumes | 0.87 (0.28, 1.76) | |
| Ethnic foods, cakes, and fast food | 0.51 (0.07, 1.52) | |
| Condiments | 0.47 (0.24, 0.88) | |
| Others | 0 (0, 0.13) |
| Variables | Q1 | Q2 | Q3 | Q4 | Q5 | p-Trend |
|---|---|---|---|---|---|---|
| Dietary Cu intakes, mg/day | ||||||
| Range | 0–1.51 | 1.51–1.73 | 1.73–1.93 | 1.93–2.21 | 2.21–19.66 | |
| Median | 1.34 | 1.63 | 1.83 | 2.05 | 2.46 | |
| Cases (rate, ‰) | 133 (6.44) | 219 (7.24) | 217 (6.42) | 238 (6.99) | 233 (8.20) | |
| Model 1 | 1.00 (Ref) | 0.90 (0.71, 1.13) | 0.73 (0.56, 0.97) | 0.79 (0.55, 1.11) | 0.95 (0.62, 1.47) | 0.17 |
| Model 2 | 1.00 (Ref) | 1.19 (0.93, 1.52) | 1.11 (0.81, 1.53) | 1.22 (0.80, 1.85) | 1.30 (0.77, 2.20) | 0.0130 |
| Dietary Se intakes, µg/day | ||||||
| Range | 0–29.31 | 29.31–35.33 | 35.33–41.35 | 41.35–50.56 | 50.56–433.16 | |
| Median | 25.08 | 32.36 | 38.16 | 45.36 | 59.42 | |
| Cases (rate, ‰) | 190 (6.70) | 204 (6.29) | 214 (6.66) | 233 (7.89) | 199 (8.07) | |
| Model 1 | 1.00 (Ref) | 1.01 (0.81, 1.27) | 1.26 (0.95, 1.67) | 1.68 (1.17, 2.41) | 1.94 (1.25, 2.99) | <0.0001 |
| Model 2 | 1.00 (Ref) | 0.95 (0.75, 1.20) | 0.93 (0.68, 1.26) | 0.92 (0.62, 1.37) | 0.89 (0.54, 1.45) | 0.82 |
| Variables | N | Q1 | Q2 | Q3 | Q4 | Q5 | p-Trend | p-Interaction |
|---|---|---|---|---|---|---|---|---|
| Dietary Cu intakes, mg/day | ||||||||
| Age, years | ||||||||
| <60 | 12,004 | 1.00 (Ref) | 1.11 (0.83, 1.48) | 1.05 (0.73, 1.53) | 1.11 (0.68, 1.82) | 1.17 (0.63, 2.17) | 0.0281 | 0.91 |
| ≥60 | 2707 | 1.00 (Ref) | 1.09 (0.68, 1.76) | 0.82 (0.44, 1.52) | 0.97 (0.44, 2.13) | 0.99 (0.37, 2.62) | 0.34 | |
| Sex | ||||||||
| Male | 7333 | 1.00 (Ref) | 1.33 (0.94, 1.89) | 0.95 (0.59, 1.51) | 0.93 (0.50, 1.71) | 0.90 (0.41, 1.95) | 0.15 | 0.20 |
| Female | 7378 | 1.00 (Ref) | 1.04 (0.73, 1.48) | 1.25 (0.80, 1.95) | 1.52 (0.86, 2.69) | 1.68 (0.82, 3.43) | 0.0236 | |
| BMI, kg/m2 | ||||||||
| <24.0 | 9403 | 1.00 (Ref) | 1.43 (0.96, 2.15) | 1.16 (0.68, 1.98) | 1.52 (0.76, 3.05) | 1.56 (0.66, 3.72) | 0.0119 | 0.14 |
| ≥24.0 | 5308 | 1.00 (Ref) | 1.01 (0.73, 1.38) | 1.09 (0.73, 1.64) | 1.06 (0.62, 1.80) | 1.19 (0.61, 2.32) | 0.21 | |
| Region | ||||||||
| North | 6211 | 1.00 (Ref) | 0.96 (0.65, 1.41) | 0.83 (0.53, 1.30) | 0.94 (0.53, 1.65) | 0.81 (0.40, 1.65) | 0.29 | 0.36 |
| South | 8589 | 1.00 (Ref) | 1.46 (1.05, 2.03) | 1.51 (0.96, 2.40) | 1.56 (0.84, 2.90) | 2.17 (1.00, 4.69) | 0.0180 | |
| Hypertension | ||||||||
| No | 11,610 | 1.00 (Ref) | 1.20 (0.87, 1.66) | 1.24 (0.81, 1.90) | 1.39 (0.80, 2.42) | 1.55 (0.77, 3.12) | 0.0077 | 0.0347 |
| Yes | 3101 | 1.00 (Ref) | 1.14 (0.77, 1.69) | 0.96 (0.58, 1.60) | 1.06 (0.55, 2.04) | 1.08 (0.48, 2.41) | 0.55 | |
| Dietary Se intakes, µg/day | ||||||||
| Age, years | ||||||||
| <60 | 12,004 | 1.00 (Ref) | 0.92 (0.70, 1.21) | 0.78 (0.54, 1.13) | 0.80 (0.50, 1.29) | 0.76 (0.42, 1.37) | 0.41 | 0.08 |
| ≥60 | 2707 | 1.00 (Ref) | 1.02 (0.63, 1.64) | 1.44 (0.78, 2.64) | 1.19 (0.55, 2.55) | 1.11 (0.43, 2.83) | 0.67 | |
| Sex | ||||||||
| Male | 7333 | 1.00 (Ref) | 1.18 (0.82, 1.70) | 0.92 (0.57, 1.50) | 1.21 (0.65, 2.23) | 1.03 (0.48, 2.19) | 0.99 | 0.22 |
| Female | 7378 | 1.00 (Ref) | 0.81 (0.59, 1.11) | 0.99 (0.66, 1.49) | 0.75 (0.44, 1.27) | 0.86 (0.45, 1.65) | 0.87 | |
| BMI, kg/m2 | ||||||||
| <24.0 | 9403 | 1.00 (Ref) | 1.02 (0.72, 1.45) | 0.85 (0.52, 1.39) | 0.88 (0.46, 1.66) | 0.87 (0.39, 1.90) | 0.91 | 0.18 |
| ≥24.0 | 5308 | 1.00 (Ref) | 0.89 (0.65, 1.23) | 1.01 (0.67, 1.51) | 1.07 (0.64, 1.79) | 1.03 (0.55, 1.93) | 0.78 | |
| Region | ||||||||
| North | 6211 | 1.00 (Ref) | 0.83 (0.58, 1.17) | 0.77 (0.50, 1.18) | 0.61 (0.36, 1.06) | 0.57 (0.29, 1.13) | 0.37 | 0.24 |
| South | 8589 | 1.00 (Ref) | 1.00 (0.72, 1.40) | 1.02 (0.63, 1.64) | 1.31 (0.70, 2.43) | 1.21 (0.57, 2.59) | 0.78 | |
| Hypertension | ||||||||
| No | 11,610 | 1.00 (Ref) | 0.98 (0.72, 1.32) | 0.91 (0.61, 1.38) | 0.89 (0.52, 1.52) | 0.70 (0.36, 1.37) | 0.18 | 0.72 |
| Yes | 3101 | 1.00 (Ref) | 0.81 (0.54, 1.19) | 0.81 (0.49, 1.32) | 0.83 (0.45, 1.52) | 1.03 (0.50, 2.13) | 0.19 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cui, Z.; Zhou, H.; Liu, K.; Wu, M.; Li, S.; Meng, S.; Meng, H. Dietary Copper and Selenium Intakes and the Risk of Type 2 Diabetes Mellitus: Findings from the China Health and Nutrition Survey. Nutrients 2022, 14, 2055. https://0-doi-org.brum.beds.ac.uk/10.3390/nu14102055
Cui Z, Zhou H, Liu K, Wu M, Li S, Meng S, Meng H. Dietary Copper and Selenium Intakes and the Risk of Type 2 Diabetes Mellitus: Findings from the China Health and Nutrition Survey. Nutrients. 2022; 14(10):2055. https://0-doi-org.brum.beds.ac.uk/10.3390/nu14102055
Chicago/Turabian StyleCui, Zhixin, Haiyan Zhou, Ke Liu, Man Wu, Shun Li, Shuangli Meng, and Huicui Meng. 2022. "Dietary Copper and Selenium Intakes and the Risk of Type 2 Diabetes Mellitus: Findings from the China Health and Nutrition Survey" Nutrients 14, no. 10: 2055. https://0-doi-org.brum.beds.ac.uk/10.3390/nu14102055