
Recommendations for the Development of Family-Based Interventions Aiming to Prevent Unhealthy Changes in Energy Balance-Related Behavior during the Transition to Parenthood: A Focus Group Study

 , , , ,
, , , ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Design and Participants
2.2. Procedure
2.3. Question Guide
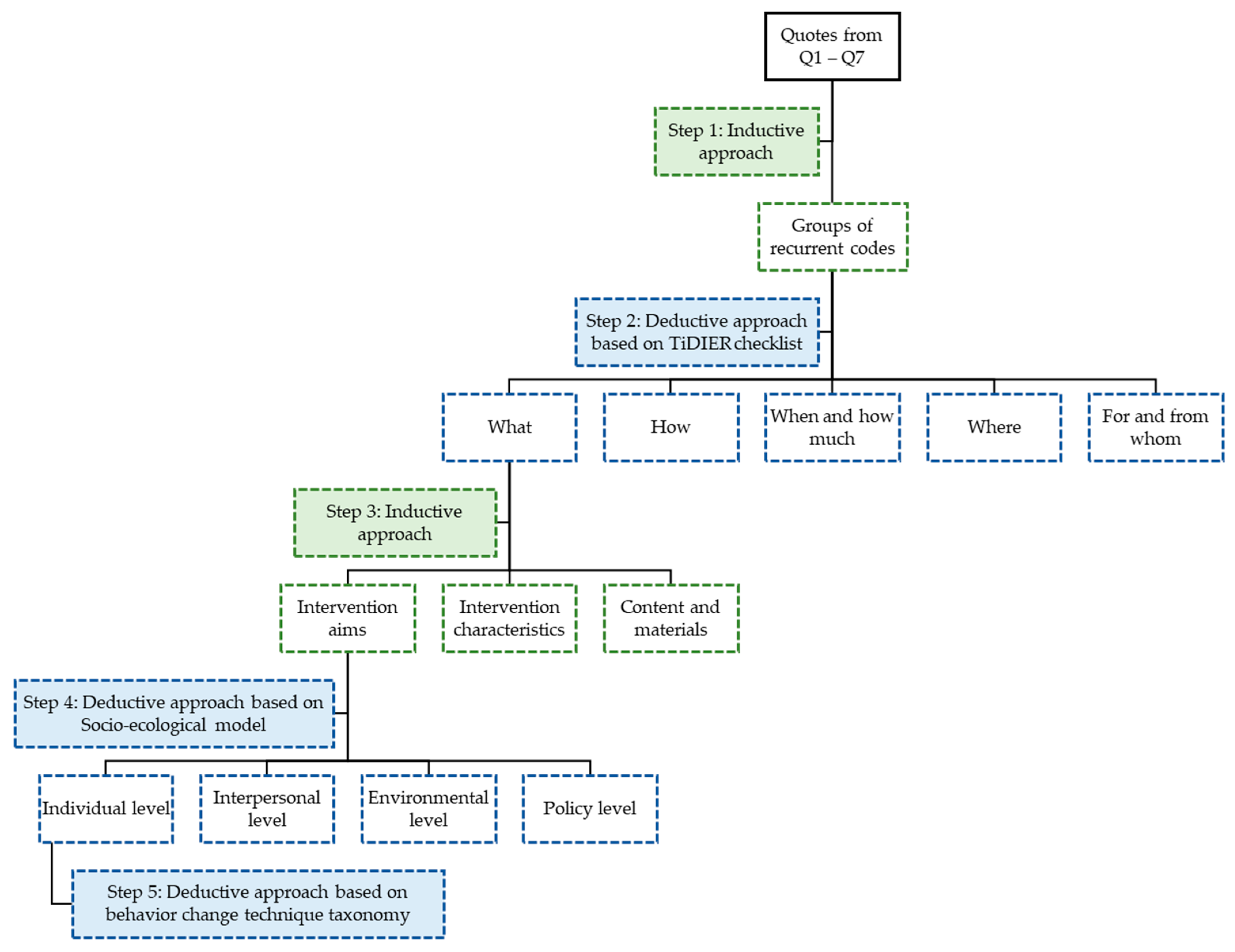
2.4. Data Analysis
3. Results
3.1. Study Sample Characteristics
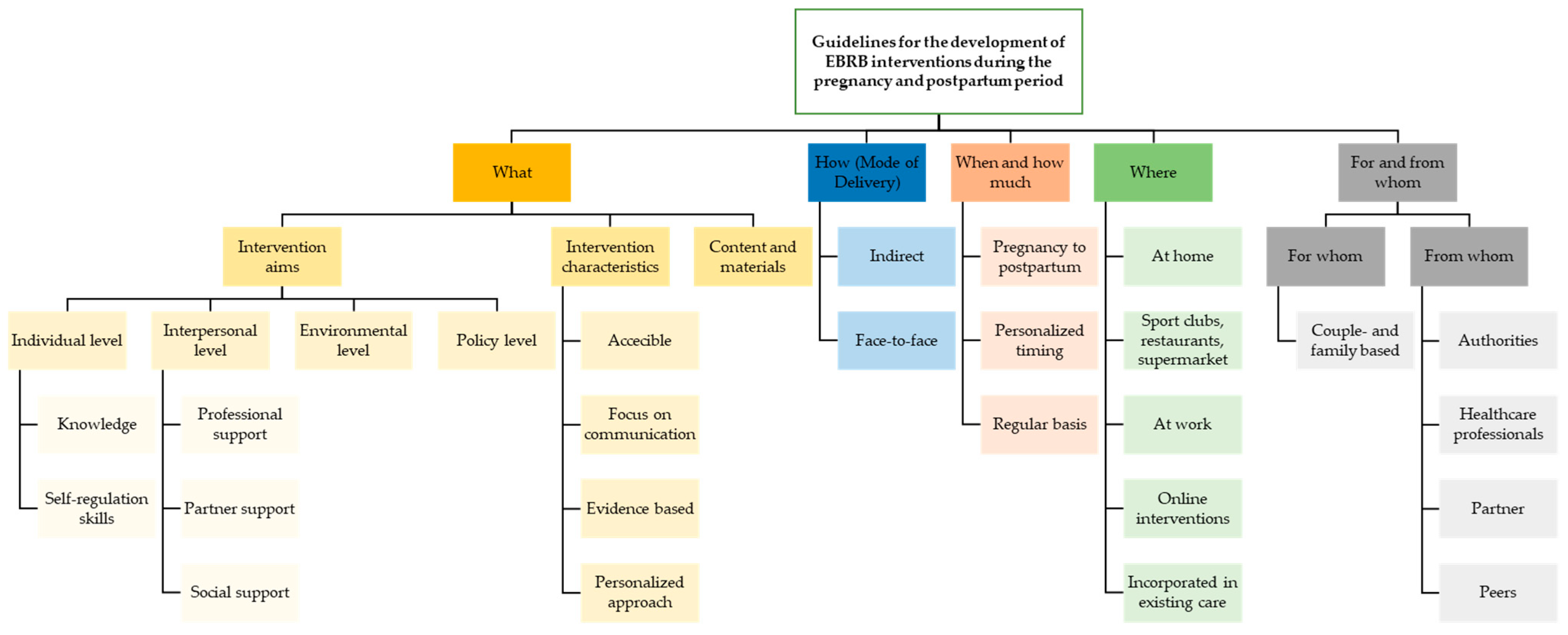
3.2. Intervention Development
3.2.1. What—Content of the Intervention
Intervention Aims
“If I were a healthcare professional, I would say to young parents who just got a child that they should not feel guilty about bringing their child somewhere else and make time for themselves to cook, to eat well or to exercise. I think there are a lot of people who feel guilty about that and it would be good if healthcare professionals told you to actually do these kind of things.”(first-time father)
Intervention Characteristics
“I know these topics such as nutrition are important. We already experience quite some pressure. Especially if you are a young parent and you have children, a family … there are so many things you must consider and then you must start working again and there are all kinds of demands, so there is a lot of pressure to do things well … So, you really must facilitate …”(first-time mother)
Content and Materials
“These apps are always very female oriented, which makes sense, because this is the goal for 90% of the information. But, if it’s not filtered or directed to men, you will have to scroll or search for a very long time, until you finally find what you need. Sometimes it’s fun to read everything, but not all of it is useful to us.”(first-time father)
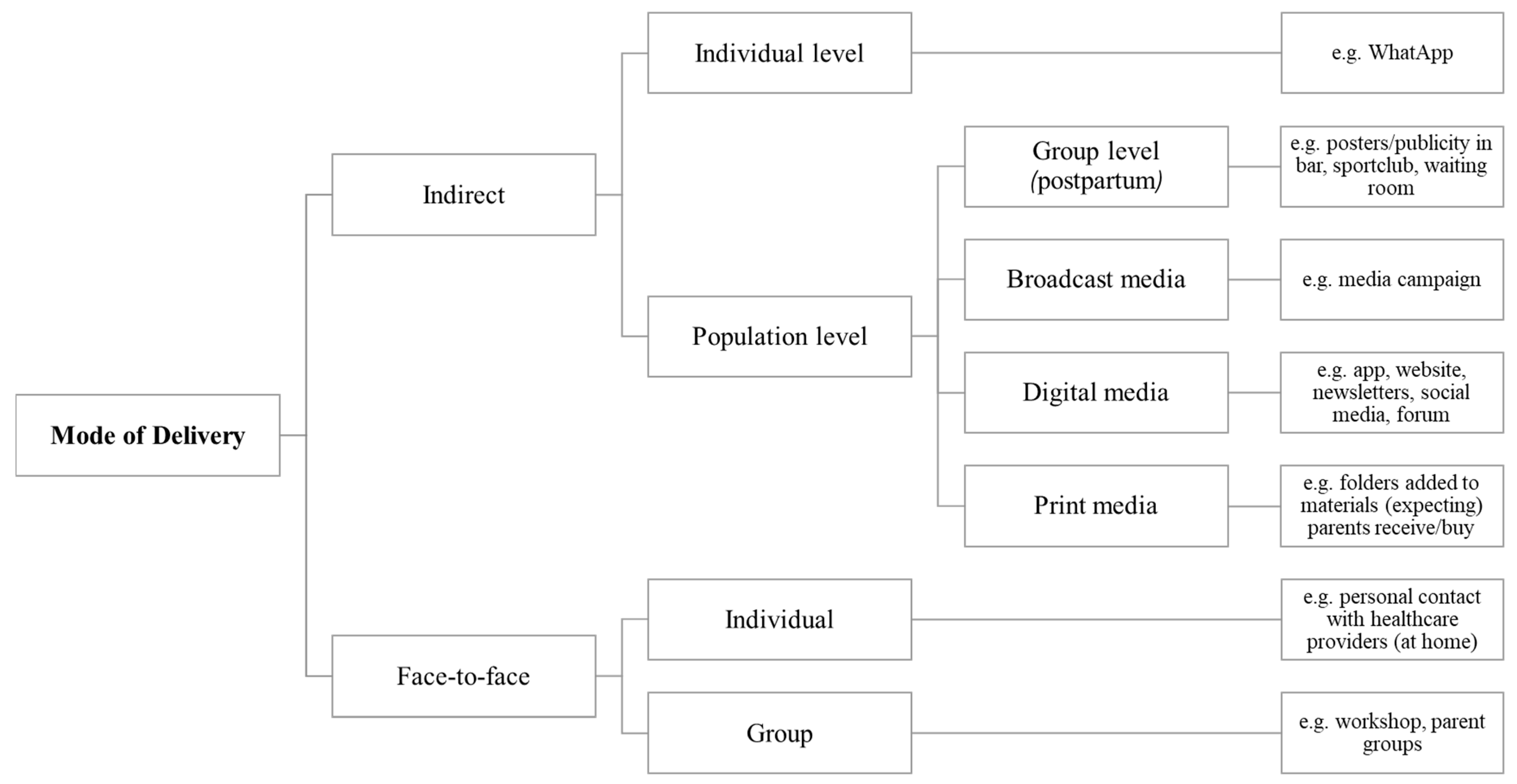
3.2.2. How—Mode of Delivery and Reachability
“The gynecologist should tell you ‘this is a good app, and not those other ones or those websites that you are consulting’.”(first-time father)
3.2.3. Where—Intervention Deployment
“The dietitian I’ve been seeing mostly guided me online. So I didn’t have to go there. She focused on people who are busy, and it was indeed difficult for me to go there with him [the baby], so she has guided me completely via WhatsApp and e-mail. (…) So yes, this guidance fitted very well with my living environment at that time.”(first-time mother)
3.2.4. When and How Much—Intensity and Duration
“We should get better guidance during pregnancy, e.g., now you only get a flyer with tips on how to eat in a varied way. There are so much more possibilities than that. If this topic already gets more attention during pregnancy, in a good, positive and constructive way, it will be easier postpartum to continue with these advices, because you have already learned these skills to eat in a healthy and balanced way.”(first-time mother)
3.2.5. Target Groups—For and from Whom
For Whom
“Sensibilization is needed about physical activity during pregnancy, to get rid of these old ideas about physical activity being bad. They just don’t know because they heard from their moms to sit still. Explain them [social environment] what can be done during pregnancy, otherwise this idea will stay.”(expecting father)
From Whom
“I would prefer to receive information from an organization of which you know that it is reliable such as the Child and Family Organization. If they provide information you will trust it.”(expecting mother)
“Actually in my case, there is only one person who would be able to encourage me to exercise more, and that is my wife herself”(expecting father)
4. Discussion
Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| BMI | Body Mass Index |
| EBRB | Energy Balance Related Behavior |
| GWG | Gestational Weight Gain |
| IM | Intervention Mapping |
| PA | Physical Activity |
| SB | Sedentary Behavior |
References
- Corder, K.; Winpenny, E.M.; Foubister, C.; Guagliano, J.M.; Hartwig, X.M.; Love, R.; Clifford Astbury, C.; van Sluijs, E.M.F. Becoming a parent: A systematic review and meta-analysis of changes in BMI, diet, and physical activity. Obes. Rev. Off. J. Int. Assoc. Study Obes. 2020, 21, e12959. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rong, K.; Yu, K.; Han, X.; Szeto, I.M.; Qin, X.; Wang, J.; Ning, Y.; Wang, P.; Ma, D. Pre-pregnancy BMI, gestational weight gain and postpartum weight retention: A meta-analysis of observational studies. Public Health Nutr. 2015, 18, 2172–2182. [Google Scholar] [CrossRef] [PubMed]
- Rasmussen, K.M.; Yaktine, A.L. Weight Gain during Pregnancy: Reexamining the Guidelines. The National Academies Collection: Reports funded by National Institutes of Health. In Medicine Io, National Research Council Committee to Reexamine IOMPWG, Editors; National Academies Press (US) National Academy of Sciences: Washington, DC, USA, 2009. [Google Scholar]
- Nehring, I.; Schmoll, S.; Beyerlein, A.; Hauner, H.; von Kries, R. Gestational weight gain and long-term postpartum weight retention: A meta-analysis. Am. J. Clin. Nutr. 2011, 94, 1225–1231. [Google Scholar] [CrossRef] [PubMed]
- Saxbe, D.; Corner, G.W.; Khaled, M.; Horton, K.; Wu, B.; Khoddam, H.L. The weight of fatherhood: Identifying mechanisms to explain paternal perinatal weight gain. Health Psychol. Rev. 2018, 12, 294–311. [Google Scholar] [CrossRef]
- Umberson, D.; Liu, H.; Mirowsky, J.; Reczek, C. Parenthood and trajectories of change in body weight over the life course. Soc. Sci. Med. 2011, 73, 1323–1331. [Google Scholar] [CrossRef] [Green Version]
- Deliens, T.; Versele, V.; Vanden Eynde, H.; Clarys, P.; Devlieger, R.; Bogaerts, A.; Gucciardo, L.; Schreurs, A.; Van Holsbeke, C.; Aerenhouts, D. Body weight, body composition and energy balance related behaviour during the transition to parenthood: Study protocol of a multi-centre observational follow-up study (TRANSPARENTS). BMC Public Health 2019, 19, 516. [Google Scholar] [CrossRef] [Green Version]
- Muktabhant, B.; Lawrie, T.A.; Lumbiganon, P.; Laopaiboon, M. Diet or exercise, or both, for preventing excessive weight gain in pregnancy. Cochrane Database Syst. Rev. 2015, Cd007145. [Google Scholar] [CrossRef]
- Pot, N.; Keizer, R. Physical activity and sport participation: A systematic review of the impact of fatherhood. Prev. Med. Rep. 2016, 4, 121–127. [Google Scholar] [CrossRef] [Green Version]
- Sallis, J.F.; Cervero, R.B.; Ascher, W.; Henderson, K.A.; Kraft, M.K.; Kerr, J. An ecological approach to creating active living communities. Annu. Rev. Public Health 2006, 27, 297–322. [Google Scholar] [CrossRef] [Green Version]
- Sallis, J.F.; Owen, N.; Fisher, E. Ecological models of health behavior. Health Behav. Theory Res. Pract. 2015, 5, 41–165. [Google Scholar]
- Versele, V.; Stok, F.M.; Aerenhouts, D.; Deforche, B.; Bogaerts, A.; Devlieger, R.; Clarys, P.; Deliens, T. Determinants of changes in women’s and men’s eating behavior across the transition to parenthood: A focus group study. Int. J. Behav. Nutr. Phys. Act. 2021, 18, 95. [Google Scholar] [CrossRef] [PubMed]
- Versele, V.; Stok, F.M.; Dieberger, A.; Deliens, T.; Aerenhouts, D.; Deforche, B.; Bogaerts, A.; Devlieger, R.; Clarys, P. Determinants of Changes in Women’s and Men’s Physical Activity and Sedentary Behavior across the Transition to Parenthood: A Focus Group Study. Int. J. Environ. Res. Public Health 2022, 19, 2421. [Google Scholar] [CrossRef] [PubMed]
- Phelan, S. Pregnancy: A “teachable moment” for weight control and obesity prevention. Am. J. Obstet. Gynecol. 2010, 202, 135.e1–135.e8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pollak, K.I.; Denman, S.; Gordon, K.C.; Lyna, P.; Rocha, P.; Brouwer, R.N.; Fish, L.; Baucom, D.H. Is pregnancy a teachable moment for smoking cessation among US Latino expectant fathers? A pilot study. Ethn. Health 2010, 15, 47–59. [Google Scholar] [CrossRef] [PubMed]
- Vanstone, M.; Kandasamy, S.; Giacomini, M.; DeJean, D.; McDonald, S.D. Pregnant women’s perceptions of gestational weight gain: A systematic review and meta-synthesis of qualitative research. Matern. Child Nutr. 2017, 13, e12374. [Google Scholar] [CrossRef] [PubMed]
- Rogozińska, E.; Marlin, N.; Betrán, A.P.; Astrup, A.; Barakat, R.; Bogaerts, A.; Jose, G.C.; Devlieger, R.; Dodd, J.M.; El Beltagy, N.; et al. Effect of diet and physical activity based interventions in pregnancy on gestational weight gain and pregnancy outcomes: Meta-analysis of individual participant data from randomised trials. BMJ (Clin. Res. ed) 2017, 358, j3119. [Google Scholar]
- Campbell, F.; Johnson, M.; Messina, J.; Guillaume, L.; Goyder, E. Behavioural interventions for weight management in pregnancy: A systematic review of quantitative and qualitative data. BMC Public Health 2011, 11, 491. [Google Scholar] [CrossRef] [Green Version]
- Kok, G.; Lo, S.H.; Peters, G.-J.Y.; Ruiter, R.A. Changing energy-related behavior: An Intervention Mapping approach. Energy Policy 2011, 39, 5280–5286. [Google Scholar] [CrossRef]
- Kok, G.; Schaalma, H.; Ruiter, R.A.; van Empelen, P.; Brug, J. Intervention mapping: Protocol for applying health psychology theory to prevention programmes. J. Health Psychol. 2004, 9, 85–98. [Google Scholar] [CrossRef] [Green Version]
- Rubin, H.J.; Rubin, I.S. Qualitative Interviewing: The Art of Hearing Data; Sage: Washington, DC, USA, 2011. [Google Scholar]
- Strömmer, S.; Weller, S.; Morrison, L.; Soltani, H.; Stephenson, J.; Whitworth, M.; Rundle, R.; Brewin, J.; Poston, L.; Lawrence, W.; et al. Young women’s and midwives’ perspectives on improving nutritional support in pregnancy: The babies, eating, and LifestyLe in adolescence (BELLA) study. Soc. Sci. Med. 2021, 274, 113781. [Google Scholar] [CrossRef]
- Hsiung, Y.; Lee, C.F.; Chi, L.K.; Huang, J.P. “Moving for My Baby!” Motivators and Perceived Barriers to Facilitate Readiness for Physical Activity during Pregnancy among Obese and Overweight Women of Urban Areas in Northern Taiwan. Int. J. Environ. Res. Public Health 2021, 18, 5275. [Google Scholar] [CrossRef] [PubMed]
- Silverman, D. Qualitative Research; Sage: Washington, DC, USA, 2020. [Google Scholar]
- Tong, A.; Sainsbury, P.; Craig, J. Consolidated criteria for reporting qualitative research (COREQ): A 32-item checklist for interviews and focus groups. Int. J. Qual. Health Care J. Int. Soc. Qual. Health Care 2007, 19, 349–357. [Google Scholar] [CrossRef] [Green Version]
- Parker, C.; Scott, S.; Geddes, A. Snowball sampling. SAGE Res. Methods Found. 2019. [Google Scholar] [CrossRef]
- Krueger, R.A. Focus Groups: A Practical Guide for Applied Research; Sage Publications: Washington, DC, USA, 2014. [Google Scholar]
- Morgan, D.L.; Scannell, A.U. Planning Focus Groups; Sage: Washington, DC, USA, 1998. [Google Scholar]
- Trotter, R.T., 2nd. Qualitative research sample design and sample size: Resolving and unresolved issues and inferential imperatives. Prev. Med. 2012, 55, 398–400. [Google Scholar] [CrossRef]
- Hoffmann, T.C.; Glasziou, P.P.; Boutron, I.; Milne, R.; Perera, R.; Moher, D.; Altman, D.G.; Barbour, V.; Macdonald, H.; Johnston, M. Better reporting of interventions: Template for intervention description and replication (TIDieR) checklist and guide. BMJ (Clin. Res. Ed) 2014, 348, g1687. [Google Scholar] [CrossRef] [Green Version]
- Michie, S.; Richardson, M.; Johnston, M.; Abraham, C.; Francis, J.; Hardeman, W.; Eccles, M.P.; Cane, J.; Wood, C.E. The behavior change technique taxonomy (v1) of 93 hierarchically clustered techniques: Building an international consensus for the reporting of behavior change interventions. Ann. Behav. Med. 2013, 46, 81–95. [Google Scholar] [CrossRef]
- Arden-Close, E.; McGrath, N. Health behaviour change interventions for couples: A systematic review. Br. J. Health Psychol. 2017, 22, 215–237. [Google Scholar] [CrossRef]
- Yee, A.Z.; Lwin, M.O.; Ho, S.S. The influence of parental practices on child promotive and preventive food consumption behaviors: A systematic review and meta-analysis. Int. J. Behav. Nutr. Phys. Act 2017, 14, 47. [Google Scholar] [CrossRef]
- Xu, H.; Wen, L.M.; Rissel, C. Associations of parental influences with physical activity and screen time among young children: A systematic review. J. Obes. 2015, 2015, 546925. [Google Scholar] [CrossRef] [Green Version]
- Henström, M.; Müssener, U.; Campbell, K.J.; Hesketh, K.D.; Rosell, M.; Delisle Nyström, C. The Need for an Evidence-Based Program in Sweden to Support Parents to Create Healthy Lifestyle Behaviors from the Start of Life—Parental Perceptions. Nutrients 2020, 12, 3823. [Google Scholar] [CrossRef] [PubMed]
- Nystrom, K.; Ohrling, K. Parenthood experiences during the child’s first year: Literature review. J. Adv. Nurs. 2004, 46, 319–330. [Google Scholar] [CrossRef]
- Versele, V.; Debekker, P.; Stok, F.M.; Aerenhouts, D.; Clarys, P.; Deforche, B.; D’Hondt, E.; Devlieger, R.; Bogaerts, A.; Deliens, T. Relative Importance of Determinants of Changes in Eating Behavior during the Transition to Parenthood: Priorities for Future Research and Interventions. Nutrients 2021, 13, 2429. [Google Scholar] [CrossRef]
- Schnitman, G.; Wang, T.; Kundu, S.; Turkdogan, S.; Gotlieb, R.; How, J.; Gotlieb, W. The role of digital patient education in maternal health: A systematic review. Patient Educ. Couns. 2021, 105, 586–593. [Google Scholar] [CrossRef]
- Maher, C.A.; Lewis, L.K.; Ferrar, K.; Marshall, S.; De Bourdeaudhuij, I.; Vandelanotte, C. Are health behavior change interventions that use online social networks effective? A systematic review. J. Med. Internet Res. 2014, 16, e40. [Google Scholar] [CrossRef] [Green Version]
- Samdal, G.B.; Eide, G.E.; Barth, T.; Williams, G.; Meland, E. Effective behaviour change techniques for physical activity and healthy eating in overweight and obese adults; systematic review and meta-regression analyses. Int. J. Behav. Nutr. Phys. Act 2017, 14, 42. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bijlholt, M.; Ameye, L.; Van Uytsel, H.; Devlieger, R.; Bogaerts, A. The INTER-ACT E-Health Supported Lifestyle Intervention Improves Postpartum Food Intake and Eating Behavior, but not Physical Activity and Sedentary Behavior-A Randomized Controlled Trial. Nutrients 2021, 13, 1287. [Google Scholar] [CrossRef]
- Lim, S.; Hill, B.; Pirotta, S.; O’Reilly, S.; Moran, L. What Are the Most Effective Behavioural Strategies in Changing Postpartum Women’s Physical Activity and Healthy Eating Behaviours? A Systematic Review and Meta-Analysis. J. Clin. Med. 2020, 9, 237. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Regber, S.; Novak, M.; Eiben, G.; Lissner, L.; Hense, S.; Sandstrom, T.Z.; Ahrens, W.; Marild, S. Assessment of selection bias in a health survey of children and families—The IDEFICS Sweden-study. BMC Public Health 2013, 13, 418. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Question |
|---|
| 1. What could help you to change aspects of your eating behavior, PA and SB during your pregnancy (pregnancy of your partner), or since you became a mother (father)? |
| 2. We will develop an intervention to help couples who are getting (or just got) a first child make healthier choices in terms of eating behavior, PA and SB. What do you think of this? |
| 3. Can you give us advice on what to focus on when promoting healthy eating, adequate PA and limiting SB during pregnancy (during pregnancy of your partner), or after the birth of your child? |
| 4. In which way would you like to be guided and supported to make healthy choices in terms of eating behavior, PA and SB during pregnancy (during the pregnancy of your partner), or after the birth of your child? |
| 5. Through which channels/in which way can we best reach you with such an intervention? |
| 6. In which period (when during pregnancy (in first and second set of focus-groups), shortly after delivery, when your child is a bit older (second set of focus groups)) do you feel the biggest need for support to make healthy choices in terms of eating, PA and SB? |
| 7. If you were a healthcare provider involved in supporting couples expecting or having their first child, name one thing you would do to help couples make healthy choices in terms of eating, PA and SB. |
| Focus Groups on Interventions Targeting Changes in EBRB during Pregnancy | Focus Groups on Interventions Targeting Changes in EBRB Up to 1 Year Postpartum | |||
|---|---|---|---|---|
| Women | Men | Women | Men | |
| Total sample (n) | 22 | 20 | 16 | 16 |
| Ethnicity (% of Caucasian) | 100 | 100 | 100 | 100 |
| Age (years, mean ± SD) | 30.1 ± 2.5 | 31.6 ± 2.5 | 30.3 ± 2.0 | 31.7 ± 3.5 |
| Self-reported pre-pregnancy BMI (kg/m2, mean ± SD) | 22.7 ± 3.1 | 24.0 ± 4.5 | 23.3 ± 4.7 | 25.0 ± 2.4 |
| Respondents with a higher education (%) | 81.8 | 75.0 | 93.8 | 87.5 |
| Perceived health: Respondents reporting to be in good to very good health (%) | 100 | 100 | 62.6 | 81.3 |
| Respondents reporting a healthy to totally healthy eating pattern (%) | 77.3 | 80.0 | 93.8 | 62.6 |
| Respondents reporting being physically active for at least 30 min/day for 5 days or more during the last 7 days (%) | 49.9 | 45.0 | 6.3 | 37.5 |
| % non-smokers (% ex-smokers) | 100 (4.5) | 100 (40.0) | 100 (0.0) | 100 (12.5) |
| Expecting parents (n) | 15 | 14 | ||
| Gestational age (weeks, mean ± SD) | 28.4 ± 8.1 | 28.2 ± 8.6 | ||
| Parents with child (n) * | 7 | 6 | 16 | 16 |
| Age of the newborn (weeks, mean ± SD) | 9.6 ± 2.8 | 9.8 ± 5.2 | 34.8 ± 14.7 | 32.6 ± 15.3 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Versele, V.; Deforche, B.; Aerenhouts, D.; Clarys, P.; Devlieger, R.; Bogaerts, A.; Liel, C.; Löchner, J.; Wolstein, J.; van Poppel, M.; et al. Recommendations for the Development of Family-Based Interventions Aiming to Prevent Unhealthy Changes in Energy Balance-Related Behavior during the Transition to Parenthood: A Focus Group Study. Nutrients 2022, 14, 2346. https://0-doi-org.brum.beds.ac.uk/10.3390/nu14112346
Versele V, Deforche B, Aerenhouts D, Clarys P, Devlieger R, Bogaerts A, Liel C, Löchner J, Wolstein J, van Poppel M, et al. Recommendations for the Development of Family-Based Interventions Aiming to Prevent Unhealthy Changes in Energy Balance-Related Behavior during the Transition to Parenthood: A Focus Group Study. Nutrients. 2022; 14(11):2346. https://0-doi-org.brum.beds.ac.uk/10.3390/nu14112346
Chicago/Turabian StyleVersele, Vickà, Benedicte Deforche, Dirk Aerenhouts, Peter Clarys, Roland Devlieger, Annick Bogaerts, Christoph Liel, Johanna Löchner, Jörg Wolstein, Mireille van Poppel, and et al. 2022. "Recommendations for the Development of Family-Based Interventions Aiming to Prevent Unhealthy Changes in Energy Balance-Related Behavior during the Transition to Parenthood: A Focus Group Study" Nutrients 14, no. 11: 2346. https://0-doi-org.brum.beds.ac.uk/10.3390/nu14112346