
Self-Reported Dietary Choices and Oral Health Care Needs during COVID-19 Quarantine: A Cross-Sectional Study

 , , and
, , and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Group
- Level of SARS-CoV-2 fears during dental treatment and through contact with the dental office.
- Previous and present self-reported dental complaints and attendance characteristics in dental practices.
- A daily number of consumed meals, drinks, and snacks during quarantine.
- Alcohol consumption and smoking frequency in the general population.
2.2. Ethical Approval
2.3. Statistical Analysis
3. Results
3.1. Demographic Characteristics
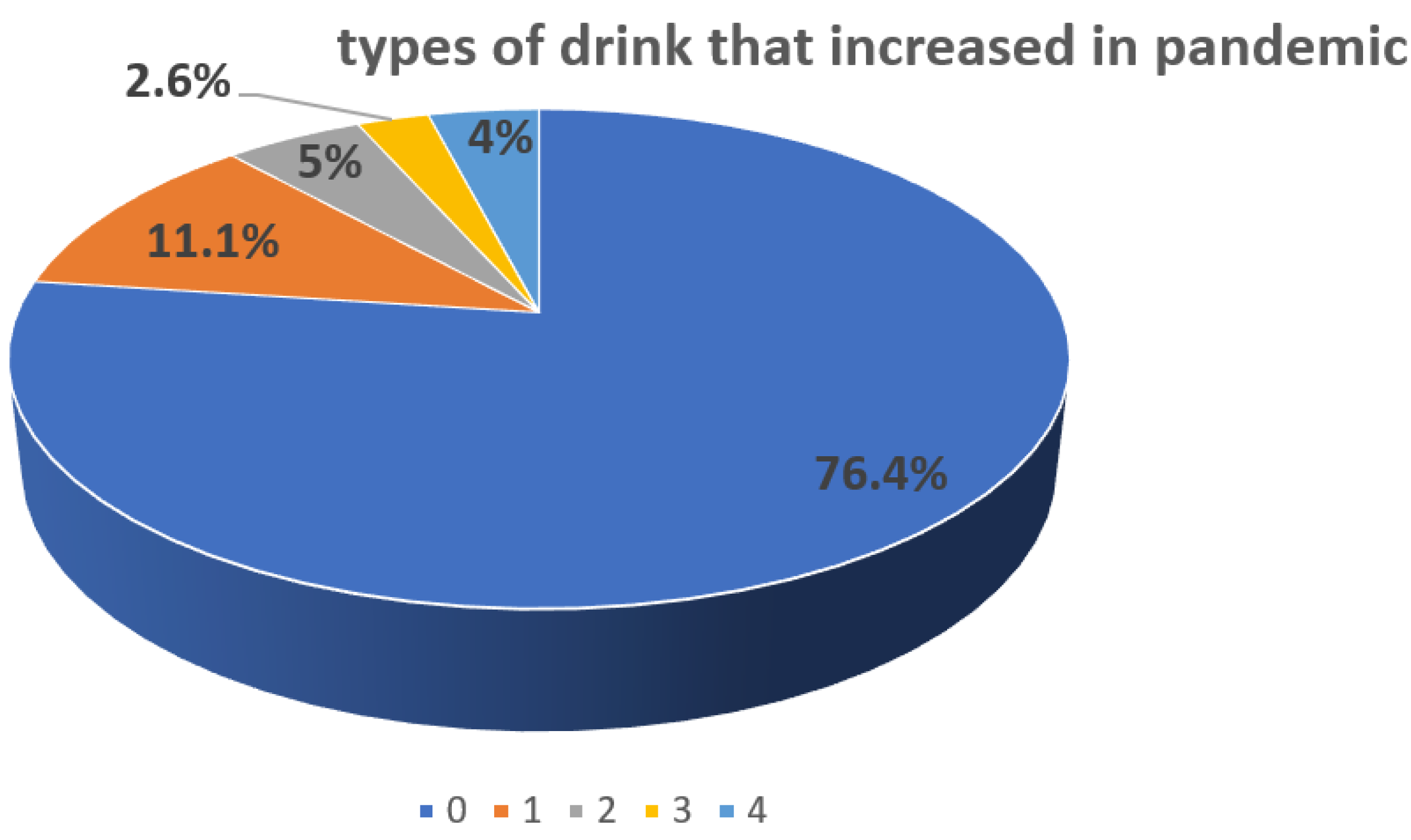
3.2. Eating and Drinking Habits
3.3. Smoking and Alcohol Consumption
3.4. Attendance to Dental Care during the Pandemic
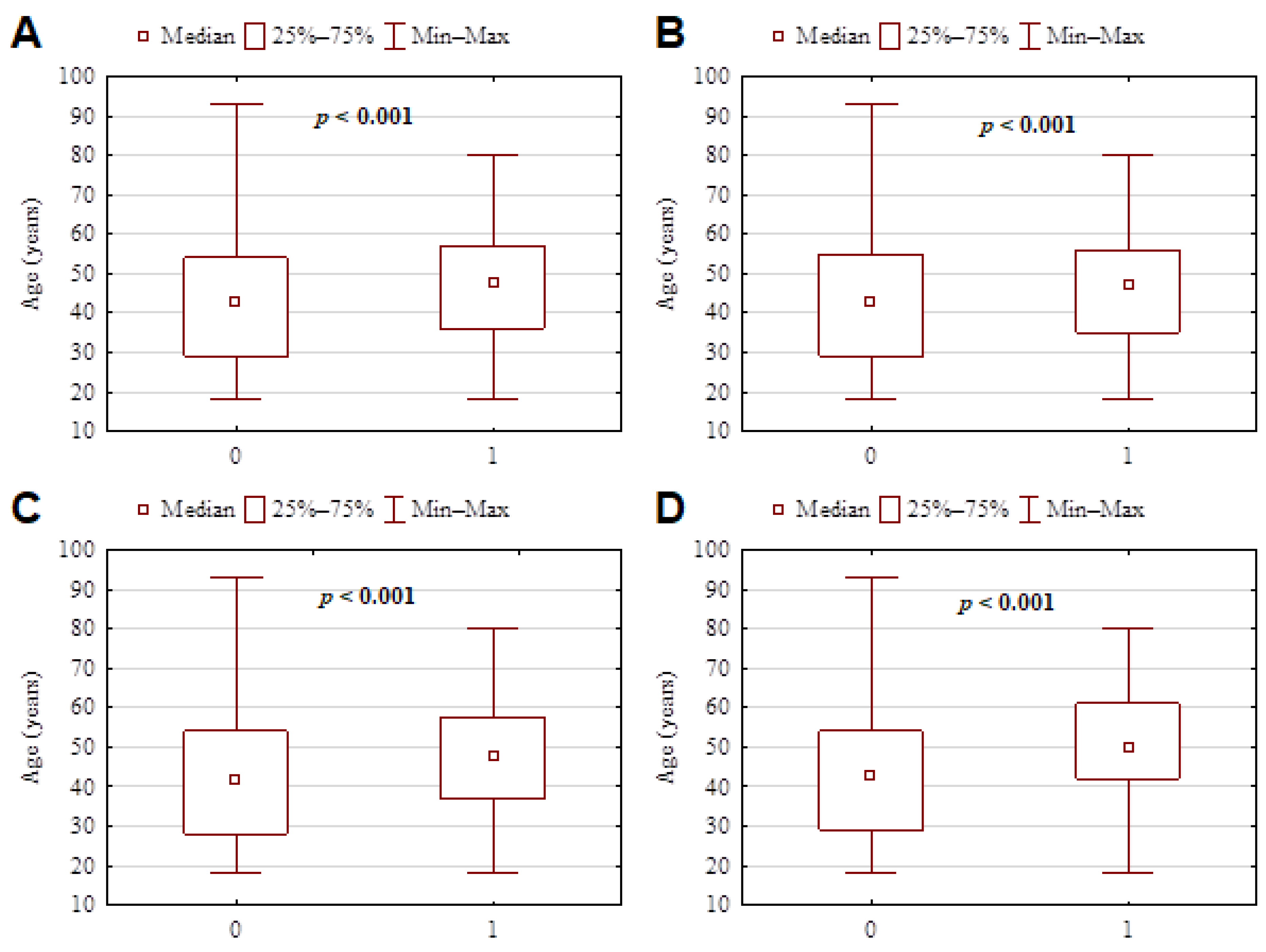
3.5. Correlations
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Meng, L.; Hua, F.; Bian, Z. Coronavirus Disease 2019 (COVID-19): Emerging and future challenges for dental and oral medicine. J. Dent. Res. 2020, 99, 481–487. [Google Scholar] [CrossRef] [Green Version]
- Liu, T.; Yuan, W.J.; Wang, X.D.; Xiao, Y.; Yu, L.Y. Nursing strategy of oral and maxillofacial trauma emergency during epidemic situation of the novel coronavirus pneumonia. China J. Oral Maxillofac. Surg. 2020, 18, 198–203. [Google Scholar]
- Navarro-Pérez, C.F.; Fernández-Aparicio, Á.; González-Jiménez, E.; Montero-Alonso, M.A.; Schmidt-RioValle, J. Effects of COVID-19 lockdown on the dietary habits and lifestyle in a population in southern Spain: A cross-sectional questionnaire. Eur. J. Clin. Nutr. 2021, 1–8. [Google Scholar] [CrossRef]
- Cheikh Ismail, L.; Hashim, M.; Mohamad, M.N.; Hassan, H.; Ajab, A.; Stojanovska, L.; Jarrar, A.H.; Hasan, H.; Abu Jamous, D.O.; Saleh, S.T.; et al. Dietary Habits and Lifestyle During Coronavirus Pandemic Lockdown: Experience From Lebanon. Front. Nutr. 2021, 8, 730425. [Google Scholar] [CrossRef]
- Sidebottom, C.; Ullevig, S.; Cheever, K.; Zhang, T. Effects of COVID-19 pandemic and quarantine period on physical activity and dietary habits of college-aged students. Sports Med. Health Sci. 2021, 3, 228–235. [Google Scholar] [CrossRef] [PubMed]
- Sidor, A.; Rzymski, P. Dietary choices and habits during COVID-19 lockdown: Experience from Poland. Nutrients 2020, 12, 1657. [Google Scholar] [CrossRef]
- COVID-19 Dashboard by the Center for Systems Science and Engineering (CSSE) at Johns Hopkins University (JHU). Available online: https://gisanddata.maps.arcgis.com/apps/opsdashboard/index.html (accessed on 30 June 2021).
- Lanham-New, S.; Hill, T.R.; Gallagher, A.M.; Hester, V.H. Introduction to Human Nutrition, 3rd ed.; Wiley-Blackwell: Hoboken, NJ, USA, 2019. [Google Scholar]
- Sahlqvist, S.; Song, Y.; Bull, F.; Adams, E.; Preston, J.; Ogilvie, D.; iConnect Consortium. Effect of questionnaire length, personalization and reminder type on response rate to a complex postal survey: Randomized controlled trial. BMC Med. Res. Methodol. 2011, 11, 62. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rolstad, S.; Adler, J.; Rydén, A. Response burden and questionnaire length: Is shorter better? A review and meta-analysis. Value Health 2011, 14, 1101–1108. [Google Scholar] [CrossRef] [Green Version]
- Cochran, W.G. Sampling Techniques, 3rd ed.; Wiley: Hoboken, NJ, USA, 1977. [Google Scholar]
- Peloso, R.M.; Pini, N.I.P.; Sundfeld Neto, D.; Mori, A.A.; Oliveria, R.C.G.; Valarelli, F.P.; Freitas, K.M.S. How does the quarantine result from COVID-19 impact dental appointments and patient anxiety levels? Braz. Oral Res. 2020, 34, e084. [Google Scholar] [CrossRef]
- Nair, A.K.; Mathew, P.; Sreela, L.S.; Prasad, T.S.; Jose, M. Knowledge and attitude toward COVID-19 and dental treatment—Its availability and treatment satisfaction during the pandemic among adult population—An online survey. J. Edu. Health Promot. 2021, 10, 77. [Google Scholar] [CrossRef] [PubMed]
- Sekundo, C.; Langowski, E.; Frese, C. Influence of COVID-19 Restrictions on Patients’ Self-reported Oral Health Care Needs. Oral Health Prev. Dent. 2021, 19, 339–343. [Google Scholar]
- González-Olmo, M.J.; Delgado-Ramos, B.; Ortega-Martínez, A.R.; Romero-Maroto, M.; Carrillo-Díaz, M. Fear of COVID-19 in Madrid. Will patients avoid dental care? Int. Dent. J. 2021, 2. [Google Scholar] [CrossRef]
- González-Olmo, M.J.; Ortega-Martínez, A.R.; Delgado-Ramos, B.; Romero-Maroto, M.; Carrillo-Diaz, M. Perceived vulnerability to Coronavirus infection: Impact on dental practice. Braz. Oral Res. 2020, 34, e044. [Google Scholar] [CrossRef]
- Olszewska, A.; Rzymski, P. Children’s Dental Anxiety during the COVID-19 Pandemic: Polish Experience. J. Clin. Med. 2020, 9, 2751. [Google Scholar] [CrossRef]
- Pylińska-Dąbrowska, D.; Starzyńska, A.; Cubała, W.J.; Ragin, K.; Alterio, D.; Jereczek-Fossa, B.A. Psychological functioning of patients undergoing oral surgery procedures during the regime related with SARS-CoV-2 pandemic. J. Clin. Med. 2020, 9, 3344. [Google Scholar] [CrossRef]
- Available online: https://nil.org.pl/aktualnosci/5359-szczepienia-lekarzy-i-lekarzy-dentystow-p-covid-19-w-liczbach (accessed on 4 January 2022).
- Peng, X.; Xu, X.; Li, Y.; Cheng, L.; Zhou, X.; Ren, B. Transmission routes of 2019-nCoV and controls in dental practice. Int. J. Oral Sci. 2020, 12, 9. [Google Scholar] [CrossRef] [PubMed]
- Liu, W.; Zhang, Q.; Chen, J.; Xiang, R.; Song, H.; Shu, S.; Chen, L.; Liang, L.; Zhou, J.; You, L.; et al. Detection of COVID-19 in children in early January 2020 in Wuhan, China. N. Engl. J. Med. 2020, 382, 1370–1371. [Google Scholar] [CrossRef] [PubMed]
- Nijakowski, K.; Cieślik, K.; Łaganowski, K.; Gruszczyński, D.; Surdacka, A. The impact of the COVID-19 pandemic on the spectrum of performed dental procedures. Int. J. Environ. Res. Public Health. 2021, 18, 3421. [Google Scholar] [CrossRef] [PubMed]
- Carrouel, F.; Gonçalves, L.S.; Conte, M.P.; Campus, G.; Fisher, J.; Fraticelli, L.; Gadea-Deschamps, E.; Ottolenghi, L.; Bourgeois, D. Antiviral activity of reagents in mouth rinses against SARS-CoV-2. J. Dent. Res. 2021, 100, 124–132. [Google Scholar] [CrossRef] [PubMed]
- Giudice, A.; Barone, S.; Muraca, D.; Averta, F.; Diodati, F.; Antonelli, A.; Fortunato, L. Can teledentistry improve the monitoring of patients during the COVID-19 dissemination? A descriptive pilot study. Int. J. Environ. Res. Public Health 2020, 17, 3399. [Google Scholar] [CrossRef]
- Bischoff, A. Benefits and risks from telemedicine. MMW Fortschr. Med. 2016, 158, 18–19. [Google Scholar]
- Kautsch, M.; Lichoń, M.; Matuszak, N.; Erskine, J.; Whitfield, M. Are there just barriers? Institutional perspective on the development of e-health in Poland. Eng. Manag. Prod. Serv. 2017, 9, 64–72. [Google Scholar] [CrossRef]
- Telles-Araujo, G.T.; Caminha, R.D.G.; Kallás, M.S.; Santos, P.S.D.S. Teledentistry support in COVID-19 oral care. Clinics 2020, 75, e2030. [Google Scholar] [CrossRef] [PubMed]
- Jenerowicz, D.; Wnuk-Kłosińska, A. Telemedicine and teledermatology an overview of structure, application and medical aspects. In Ethics and the Law in Medicine—In Research and Healthcare; Długosz, J., Joerden, J.C., Paszyńska, E., Steger, F., Eds.; Peter Lang GmbH: Berlin, Germany, 2019. [Google Scholar]
- Trottini, M.; Bossù, M.; Corridore, D.; Ierardo, G.; Luzzi, V.; Saccucci, M.; Polimeni, A. Assessing risk factors for dental caries: A statistical modeling approach. Caries Res. 2015, 49, 226–235. [Google Scholar] [CrossRef] [PubMed]
- Sharma, H.; Suprabha, B.S.; Rao, A. Teledentistry and its applications in paediatric dentistry: A literature review. Pediatr. Dent. J. 2021, 31, 203–215. [Google Scholar] [CrossRef] [PubMed]
- Opichka, K.; Smith, C.; Levine, A.S. Problematic eating behaviors are more prevalent in African American women who are overweight or obese than African American women who are lean or normal weight. Fam. Community Health 2019, 42, 81–89. [Google Scholar] [CrossRef] [PubMed]
- Larsen, S.C.; Heitmann, B.L. More frequent intake of regular meals and less frequent snacking are weakly associated with lower long-term gains in body mass index and fat mass in middle-aged men and women. J. Nutr. 2019, 149, 824–830. [Google Scholar] [CrossRef] [PubMed]
- Proctor, G. Diurnal rhythm and salivary electrolyte. Arch. Oral Biol. 2018, 93, 1–2. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dawes, C.; Pedersen, A.M.; Villa, A.; Ekström, J.; Proctor, G.B.; Vissink, A.; Aframian, D.; McGowan, R.; Aliko, A.; Narayana, N.; et al. The functions of human saliva: A review sponsored by the World Workshop on Oral Medicine VI. Arch. Oral Biol. 2015, 60, 863–874. [Google Scholar] [CrossRef]
- Błaszczyk-Bębenek, E.; Jagielski, P.; Bolesławska, I.; Jagielska, A.; Nitsch-Osuch, A.; Kawalec, P. Nutrition Behaviors in Polish Adults before and during COVID-19 Lockdown. Nutrients 2020, 12, 3084. [Google Scholar] [CrossRef] [PubMed]
- Kriaucioniene, V.; Bagdonaviciene, L.; Rodríguez-Pérez, C.; Petkeviciene, J. Associations between Changes in Health Behaviours and Body Weight during the COVID-19 Quarantine in Lithuania: The Lithuanian COVIDiet Study. Nutrients 2020, 12, 3119. [Google Scholar] [CrossRef]
- Lucini, D.; Gandolfi, C.E.; Antonucci, C.; Cavagna, A.; Valzano, E.; Botta, E.; Chiari, M.; Mameli, L.; Nahum, M.; Brambilla, M.M.; et al. #StayHomeStayFit: UNIMI’s approach to online healthy lifestyle promotion during the COVID-19 pandemic. Acta Biomed. 2020, 91, e2020037. [Google Scholar] [PubMed]
- Walter, E.; von Bronk, L.; Hickel, R.; Huth, K.C. Impact of COVID-19 on Dental care during a national lockdown: A retrospective observational study. Int. J. Environ. Res. Public Health 2021, 18, 7963. [Google Scholar] [CrossRef]
- Kranz, A.M.; Gahlon, G.; Dick, A.W.; Stein, B.D. Characteristics of US adults delaying dental care due to the COVID-19 pandemic. JDR Clin. Trans. Res. 2021, 6, 8–14. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, M.A.; Jouhar, R.; Ahmed, N.; Adnan, S.; Aftab, M.; Zafar, M.S.; Khurshid, Z. Fear and practice modifications among dentists to combat novel coronavirus disease (COVID-19) Outbreak. Int. J. Environ. Res. Public Health 2020, 17, 2821. [Google Scholar] [CrossRef]
- Olszewska, A.; Paszynska, E.; Roszak, M.; Czajka-Jakubowska, A. Management of the oral health of children during the COVID-19 pandemic in Poland. Front. Public Health 2021, 9, 635081. [Google Scholar] [CrossRef] [PubMed]
- Tysiąc-Miśta, M.; Dziedzic, A. The attitudes and professional approaches of dental practitioners during the COVID-19 outbreak in Poland: A cross-sectional survey. Int. J. Environ. Res. Public Health 2020, 17, 4703. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Age (years) mean ± SD (min–max) | 44.4 ± 15.6 (18–93) |
| 18–25, n (%) | 451 (17.8) |
| 26–35, n (%) | 380 (15.0) |
| 36–45, n (%) | 455 (18.0) |
| >45 n (%) | 1248 (49.2) |
| Gender Female, n (%)/Male, n (%) | 1429 (56.3)/1107(43.7) |
| Weight (kg) mean ± SD (min–max) | 74.8 ± 17.0 (34–190) |
| BMI (kg/m2) mean ± SD (min–max) | 25.3 ± 4.9 (13.6–86.7) |
| Underweight (<18.5), n (%) | 87 (3.4) |
| Normal weight (18.5–24.9), n (%) | 1207 (47.8) |
| Overweight (25–29.9), n (%) | 903 (35.8) |
| Obesity (≥30), n (%) | 329 (13.0) |
| Education | |
| Primary n (%) | 51 (2.0) |
| Vocational n (%) | 269 (10.5) |
| Secondary n (%) | 902 (35.3) |
| Higher n (%) | 1332 (52.2) |
| Group n = 2574 | p-Value | Spearman R |
|---|---|---|
| age and dental visits | <0.001 | −0.09 |
| age and increased meals | 0.017 | 0.05 |
| age and increased sweet snacks | <0.001 | −0.07 |
| age and evening time meal | <0.001 | −0.29 |
| age and tobacco smoking | 0.008 | 0.05 |
| BMI and dental visits | 0.004 | −0.06 |
| BMI and increased meals | <0.001 | 0.08 |
| BMI and evening time meal | <0.001 | −0.10 |
| BMI and increased tobacco smoking | <0.001 | 0.07 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Paszynska, E.; Cofta, S.; Hernik, A.; Otulakowska-Skrzynska, J.; Springer, D.; Roszak, M.; Sidor, A.; Rzymski, P. Self-Reported Dietary Choices and Oral Health Care Needs during COVID-19 Quarantine: A Cross-Sectional Study. Nutrients 2022, 14, 313. https://0-doi-org.brum.beds.ac.uk/10.3390/nu14020313
Paszynska E, Cofta S, Hernik A, Otulakowska-Skrzynska J, Springer D, Roszak M, Sidor A, Rzymski P. Self-Reported Dietary Choices and Oral Health Care Needs during COVID-19 Quarantine: A Cross-Sectional Study. Nutrients. 2022; 14(2):313. https://0-doi-org.brum.beds.ac.uk/10.3390/nu14020313
Chicago/Turabian StylePaszynska, Elzbieta, Szczepan Cofta, Amadeusz Hernik, Justyna Otulakowska-Skrzynska, Daria Springer, Magdalena Roszak, Aleksandra Sidor, and Piotr Rzymski. 2022. "Self-Reported Dietary Choices and Oral Health Care Needs during COVID-19 Quarantine: A Cross-Sectional Study" Nutrients 14, no. 2: 313. https://0-doi-org.brum.beds.ac.uk/10.3390/nu14020313