Assessment of Dietary Exposure to Ochratoxin A in Lebanese Students and Its Urinary Biomarker Analysis

 , and
, and
Abstract
:1. Introduction
2. Results and Discussion
2.1. Population Characteristics
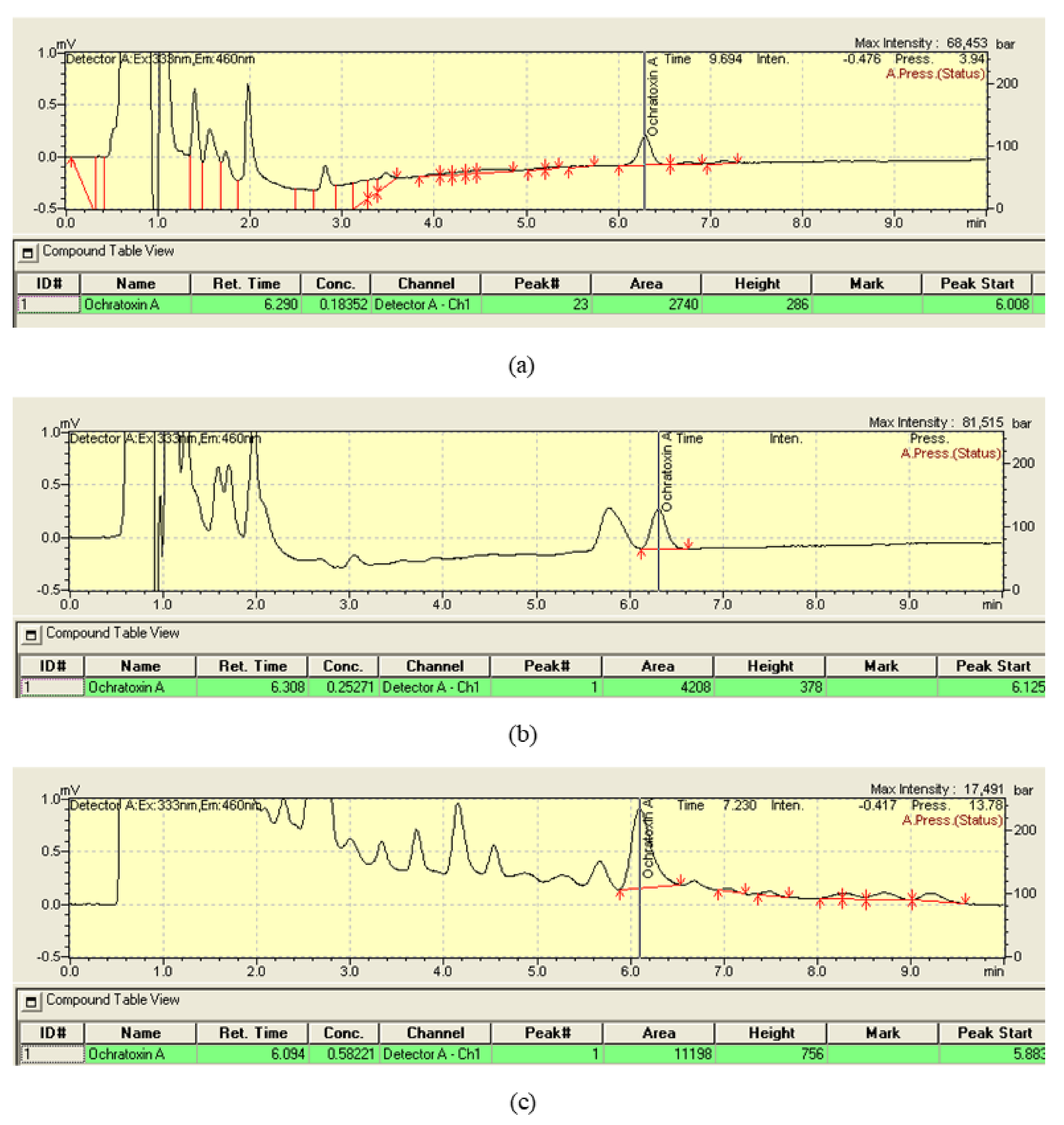
2.2. Performance of the Analytical Method
2.3. Occurrence of OTA in 24 h Diet
2.4. Calculation of PDIs and MOEs from the 24 h Diet
2.5. Occurrence of OTA in Dinner
2.6. Occurrence of OTA in Urine
2.7. Calculation of PDIs and MOEs from Urine
2.8. Differences between Diet-Based PDIs and Urine-Based PDI
2.9. Correlations
3. Conclusions
- (1)
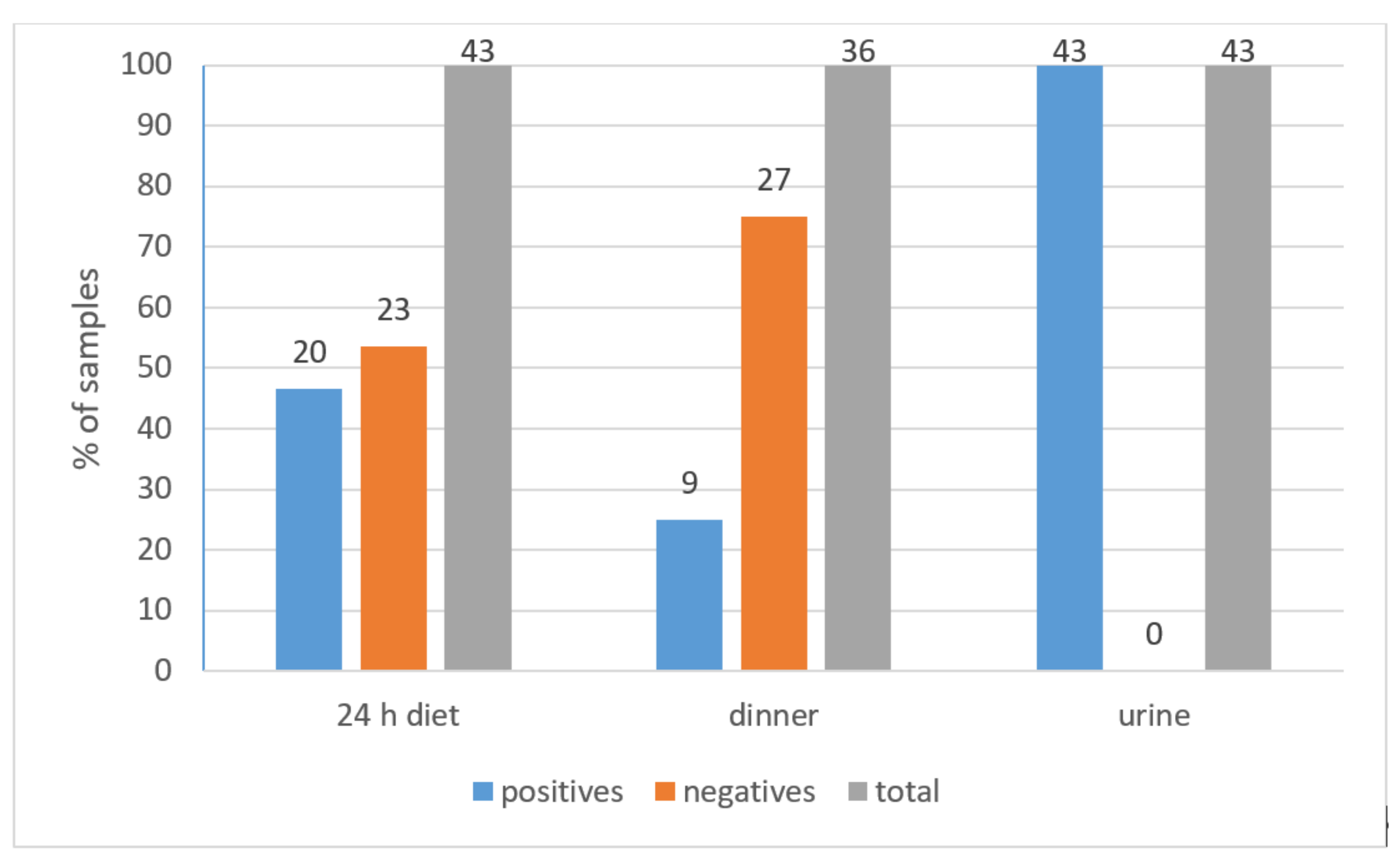
- 46.5% of 24 h diet samples of Lebanese children were positive for OTA with a mean of 0.32 ± 0.1 ng/g. The calculated means of PDI, MOE (neo) and MOE (non-neo) were 2.78 ± 1.65 ng/kg bw, 7907 ± 5922, and 2579 ± 1932, respectively.
- (2)
- 25% of dinner samples were positive for OTA with a mean of 0.32 ± 0.18 ng/g and the calculated mean PDI was 4.9 ± 10.9 ng/kg bw.
- (3)
- All urine samples were positive to OTA with a mean of 0.022 ± 0.012 ng/ml. The calculated means of PDI, MOE (neo) and MOE (non-neo) were 21.73 ± 13.8 ng/kg bw, 961 ± 599, and 313 ± 195, respectively.
- (4)
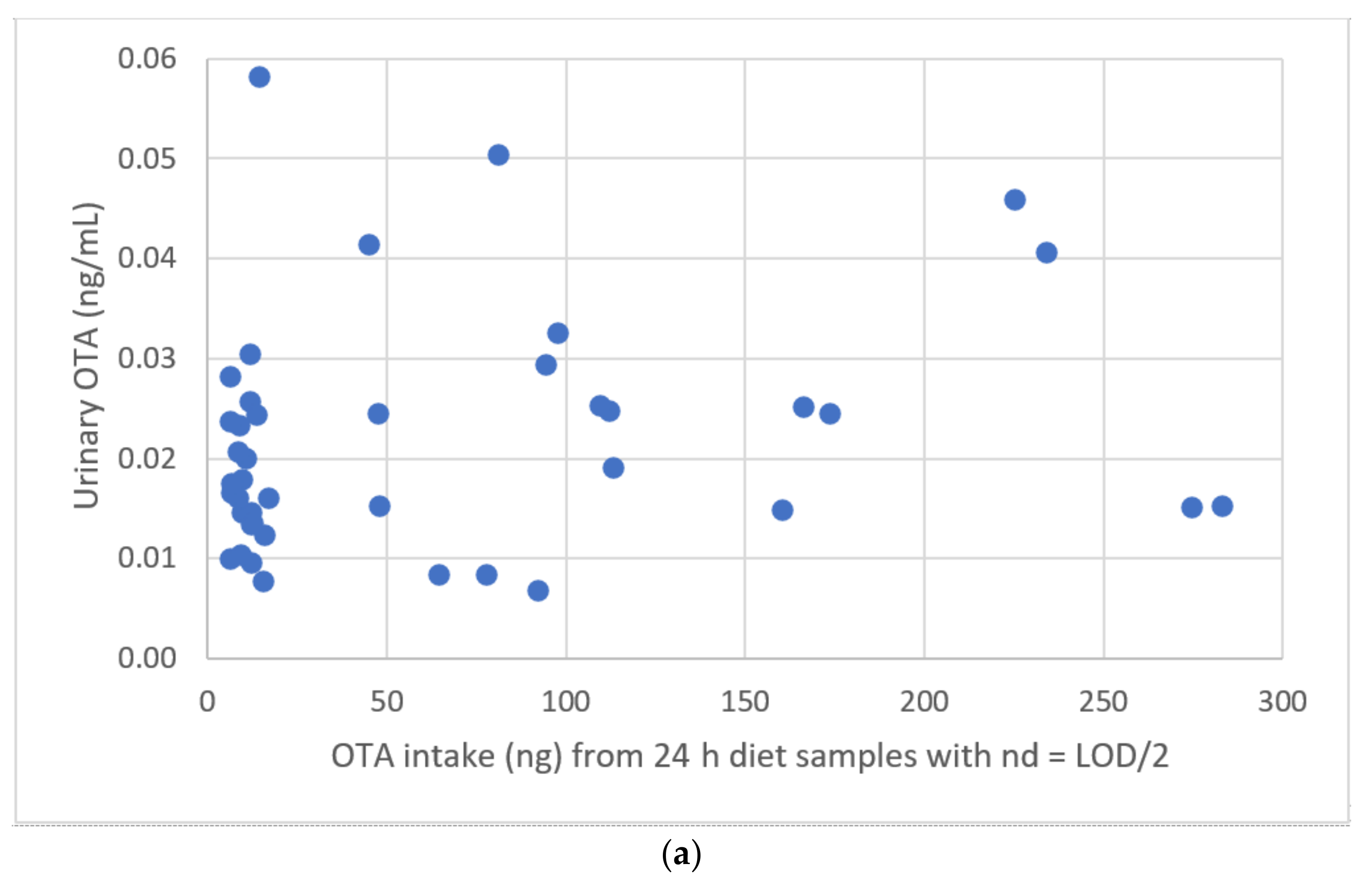
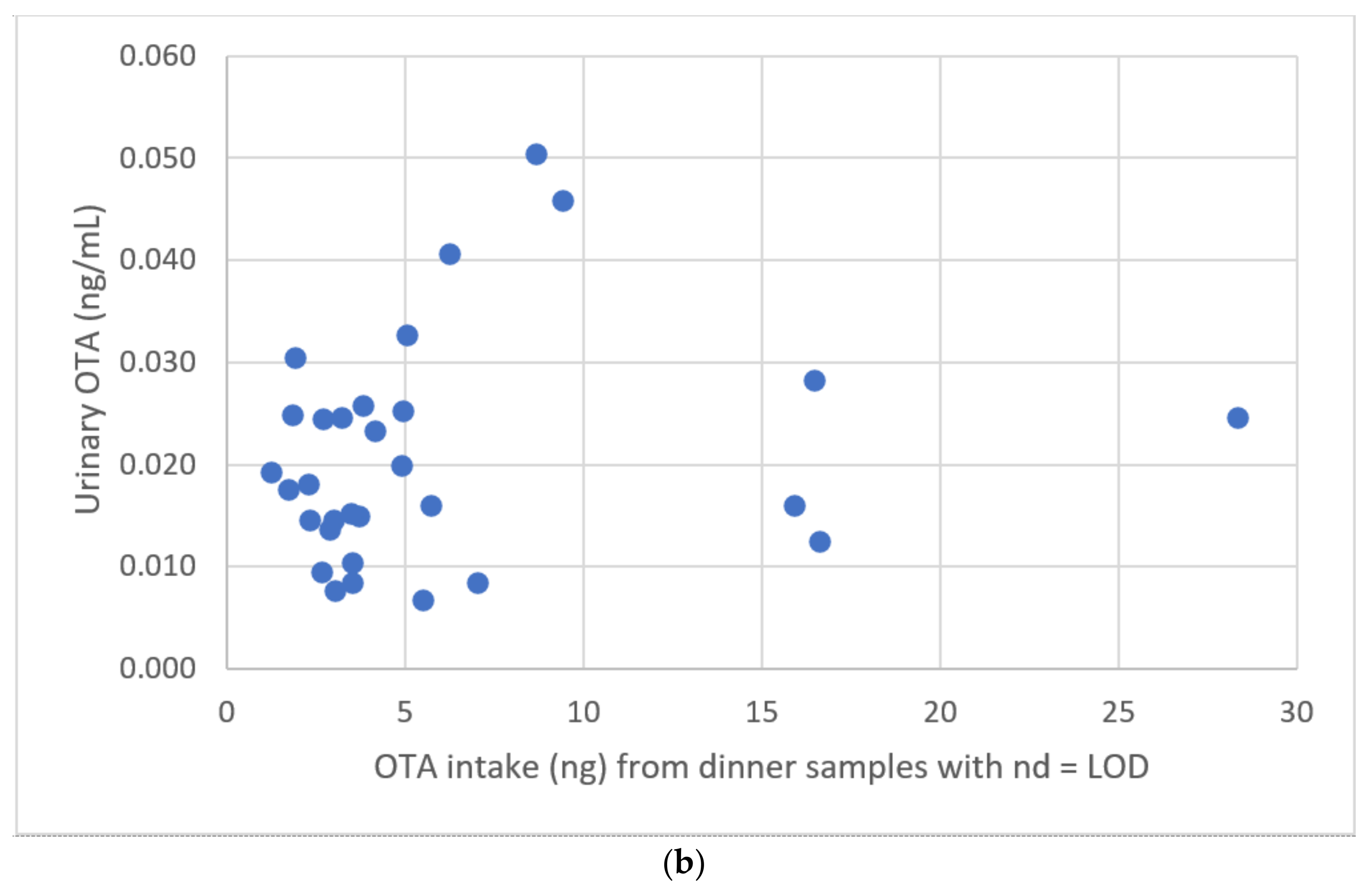
- There was a large difference between the 24 h diet-based mean PDI (2.78 ± 1.65 ng/kg bw) and urine-based mean PDI (21.73 ± 13.8 ng/kg bw). Moreover, no correlation was found between 24 h diet-based PDIs and urinary concentrations of OTA.
4. Materials and Methods
4.1. Subject Background Information and Ethical Approval
4.2. Sampling Design
4.2.1. Education
4.2.2. Materials, Data Collecting Form, and Snack Distribution
4.3. Samples Collection and Preparation until Extraction
4.4. Chemicals and Reagents
4.5. Preparation of Urine Samples
4.6. Preparation of Food Samples
4.7. High-Performance Liquid Chromatography with Fluorescence Detection (HPLC-FLD) Analysis
4.8. Performance of the Analytical Methods
4.8.1. Calibration Curve
4.8.2. Exposure Assessment (Probable Daily Intakes Estimates)
4.8.3. 24 h Diet Approach
- -
- C is OTA level in food (ng/g)
- -
- K is the weight of the consumed food (g)
- -
- bw is the body weight reported by each participant (kg)
4.8.4. Urinary Approach
- -
- C is the urinary OTA concentration of each participant (ng/mL)
- -
- V is the normal daily urine excretion of children i.e., 1 mL/kg/hour (1250 mL/day) that is between 0.5 and 1.5 mL/kg/hour estimated by the centers of disease control and prevention (CDC) (https://www.cdc.gov/dengue/training/cme/ccm/page57297.html accessed 9 November 2021) [76]
- -
- W is the body weight of each participant (kg)
- -
4.8.5. Dinner
- -
- C is OTA level in dinner (ng/g)
- -
- K is the weight of dinner consumed by each participant (g)
4.9. Risk Characterization
4.10. Statistical Analysis
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- EFSA. Risk assessment of ochratoxin A in food. EFSA J. 2020, 18, 1–150. [Google Scholar] [CrossRef]
- EFSA. Panel on Contaminants in the Food Chain. Statement on recent scientific information on the toxicity of Ochratoxin A. EFSA J. 2010, 8, 1626. [Google Scholar] [CrossRef]
- Gallo, A.; Ferrara, M.; Perrone, G. Recent advances on the molecular aspects of ochratoxin A biosynthesis. Curr. Opin. Food Sci. 2017, 17, 49–56. [Google Scholar] [CrossRef]
- Kabak, B.; Brandon, E.F.A.; Var, I.; Blokland, M.; Sips, A.J.A.M. Effects of probiotic bacteria on the bioaccessibility of aflatoxin B1 and ochratoxin A using an in vitro digestion model under fed conditions. J. Environ. Sci. Health 2009, 44, 472–480. [Google Scholar] [CrossRef]
- Castegnaro, M.; Canadas, D.; Vrabcheva, T.; Petkova-Bocharova, T.; Chernozemsky, I.N.; Pfohl-Leszkowicz, A. Balkan endemic nephropathy: Role of ochratoxins A through biomarkers. Mol. Nutr. Food Res. 2006, 50, 519–529. [Google Scholar] [CrossRef]
- Pfohl-Leszkowicz, A.; Tozlovanu, M.; Manderville, R.; Peraica, M.; Castegnaro, M.; Stefanovic, V. New molecular and field evidences for the implication of mycotoxins but not aristolochic acid in human nephropathy and urinary tract tumor. Mol. Nutr. Food Res. 2007, 51, 1131–1146. [Google Scholar] [CrossRef]
- FAO; WHO. Working Document for Information and Use in Discussions Related to Contaminants and Toxins in the GSCTFF; FAO: Rome, Italy; WHO: Geneva, Switzerland, 2019; pp. 1–164. [Google Scholar] [CrossRef]
- Duarte, S.C.; Pena, A.; Lino, C.M. Human ochratoxin A biomarkers-from exposure to effect. Crit. Rev. Toxicol. 2011, 41, 187–212. [Google Scholar] [CrossRef]
- Broom, L.J. Necrotic enteritis; Current knowledge and diet-related mitigation. Worlds Poult. Sci. J. 2017, 73, 281–292. [Google Scholar] [CrossRef]
- Shi, H.; Li, S.; Bai, Y.; Prates, L.L.; Lei, Y.; Yu, P. Mycotoxin contamination of food and feed in China: Occurrence, detection techniques, toxicological effects and advances in mitigation technologies. Food Control 2018, 91, 202–215. [Google Scholar] [CrossRef]
- IARC. Mycotoxins as human carcinogens—The IARC Monographs classification. Mycotoxin Res. 2016, 33, 65–73. [Google Scholar] [CrossRef]
- Jan, A.; Autrup, H.; Bard, D.; Benford, D.; Carere, A.; Costa, L.G.; Cravedi, J.-P.; do Domenico, A.; Fanelli, R.; Fink-Gremmels, J.; et al. Opinion of the scientific panel on contaminants in the food chain on a request from the commission related to ochratoxin A in food. EFSA J. 2006, 365, 1–56. [Google Scholar]
- Raad, F.; Nasreddine, L.; Hilan, C.; Bartosik, M.; Parent-Massin, D. Dietary exposure to aflatoxins, ochratoxin A and deoxynivalenol from a total diet study in an adult urban Lebanese population. Food Chem. Toxicol. 2014, 73, 35–43. [Google Scholar] [CrossRef]
- Paoloni, A.; Solfrizzo, M.; Bibi, R.; Pecorelli, I. Development and validation of LC-MS/MS method for the determination of Ochratoxin A and its metabolite Ochratoxin α in poultry tissues and eggs. J. Environ. Sci. Health 2018, 53, 327–333. [Google Scholar] [CrossRef]
- Han, Z.; Tangni, E.; di Mavungu, J.; Vanhaecke, L.; de Saeger, S.; Wu, A.; Callebaut, A. In vitro glucuronidation of ochratoxin A by rat liver microsomes. Toxins 2013, 5, 2671–2685. [Google Scholar] [CrossRef] [Green Version]
- Vidal, A.; Mengelers, M.; Yang, S.; de Saeger, S.; de Boevre, M. Mycotoxin Biomarkers of Exposure: A Comprehensive Review. Compr. Rev. Food Sci. Food Saf. 2018, 17, 1127–1155. [Google Scholar] [CrossRef] [Green Version]
- Gupta, R.C.; Lasher, M.A.; Mukherjee, I.R.M.; Srivastava, A.; Lall, R. Aflatoxins, ochratoxins and citrinin. In Reproductive and Developmental Toxicology, 2nd ed.; Ramesh, C.G., Ed.; Elsevier Inc.: Amsterdam, The Netherlands, 2017; Volume 48, pp. 945–962. [Google Scholar]
- Antonios, D.; Guitton, V.; Darrozes, S.; Pallardy, M.; Azouri, H. Monitoring the levels of deoxynivalenol (DON) in cereals in Lebanon and validation of an HPLC/UV detection for the determination of DON in crushed wheat (bulgur). Food Addit. Contam. Part B Surveill. 2010, 3, 45–51. [Google Scholar] [CrossRef]
- WHO. Regional per Capita Consumption of Raw and Semi-Processed Agricultural Commodities; WHO: Geneva, Switzerland, 2003. [Google Scholar]
- Pitt, J.I. Toxigenic fungi: Which are important? Med. Mycol. 2000, 38 (Suppl. 1), 17–22. [Google Scholar] [CrossRef]
- Solfrizzo, M.; Gambacorta, L.; Visconti, A. Assessment of Multi-Mycotoxin Exposure in Southern Italy by Urinary Multi-Biomarker Determination. Toxins 2014, 6, 523–538. [Google Scholar] [CrossRef]
- Carballo, D.; Tolosa, J.; Ferrer, E.; Berrada, H. Dietary exposure assessment to mycotoxins through total diet studies. A review. Food Chem. Toxicol. 2019, 128, 8–20. [Google Scholar] [CrossRef]
- Tittlemier, S.A.; Cramer, B.; Dall’Asta, C.; Iha, M.H.; Lattanzio, V.M.T.; Malone, R.J.; Maragos, C.; Solfrizzo, M.; Stranska-Zachariasova, M.; Stroka, J. Developments in mycotoxin analysis: An update for 2018–19. World Mycotoxin J. 2019, 12, 3–29. [Google Scholar] [CrossRef] [Green Version]
- EFSA. Management of left-censored data in dietary exposure assessment of chemical substances. EFSA J. 2010, 8, 1–96. [Google Scholar] [CrossRef] [Green Version]
- Gilbert, J.; Brereton, P.; MacDonald, S. Assessment of dietary exposure to ochratoxin A in the UK using a duplicate diet approach and analysis of urine and plasma samples. Food Addit. Contam. 2001, 18, 1088–1093. [Google Scholar] [CrossRef]
- Bakker, G.; Sizoo, E.; Jekel, A.; Pereboom-De Fauw, D.P.; Schothorst, R.; van Egmond, H. Determination of mean daily intakes of aflatoxin B1, aflatoxin M1, ochratoxin A, trichothecenes and fumonisins in 24-hour diets of children in the Netherlands. World Mycotoxin J. 2009, 2, 451–459. [Google Scholar] [CrossRef]
- Bakker, M.; Pieters, M.N. Risk Assessment of Ochratoxin A in the Netherlands; RIVM Report 388802025/2002; Inspectorate for Health Protection: The Hague, The Netherlands, 2002; pp. 1–24. [Google Scholar]
- Sizoo, E.A.; van Egmond, H.P. Analysis of duplicate 24-hour diet samples for aflatoxin B1, aflatoxin M1 and ochratoxin A. Food Addit. Contam. 2005, 22, 163–172. [Google Scholar] [CrossRef]
- Silva, L.J.G.; Macedo, L.; Pereira, A.M.P.T.; Duarte, S.; Lino, C.M.; Pena, A. Ochratoxin A and Portuguese children: Urine biomonitoring, intake estimation and risk assessment. Food Chem. Toxicol. 2019, 135, 110883. [Google Scholar] [CrossRef] [PubMed]
- Franco, L.T.; Petta, T.; Rottinghaus, G.E.; Bordin, K.; Gomes, G.A.; Alvito, P.; Assunção, R.; Oliveira, C.A.F. Assessment of mycotoxin exposure and risk characterization using occurrence data in foods and urinary biomarkers in Brazil. Food Chem. Toxicol. 2019, 128, 21–34. [Google Scholar] [CrossRef] [PubMed]
- Martins, C.; Vidal, A.; de Boevre, M.; de Saeger, S.; Nunes, C.; Torres, D.; Goios, A.; Lopes, C.; Assunção, R.; Alvito, P. Exposure assessment of Portuguese population to multiple mycotoxins: The human biomonitoring approach. Int. J. Hyg. Environ. Health 2019, 222, 913–925. [Google Scholar] [CrossRef]
- Assaf, H.; Betbeder, A.M.; Creppy, E.E.; Pallardy, M.; Azouri, H. Ochratoxin A levels in human plasma and foods in Lebanon. Hum. Exp. Toxicol. 2004, 23, 495–501. [Google Scholar] [CrossRef]
- Soubra, L. Évaluations Scientifiques des Risques Toxiques Liés a Certaines Substances Chimiques (Additifs Alimentaires) et Contaminants (Mycotoxines). Ph.D. Thesis, L’Institut des Sciences et Industries du Vivant et de l’Environnement, Paris, France, 2008. [Google Scholar]
- Soubra, L.; Sarkis, D.; Hilan, C.; Verger, P. Occurrence of total aflatoxins, ochratoxin A and deoxynivalenol in foodstuffs available on the Lebanese market and their impact on dietary exposure of children and teenagers in Beirut. Food Addit. Contam. 2009, 26, 189–200. [Google Scholar] [CrossRef]
- Azaiez, I.; Font, G.; Ma, J. Survey of mycotoxins in dates and dried fruits from Tunisian and Spanish markets. Food Control 2015, 51, 340–346. [Google Scholar] [CrossRef]
- Mitchell, N.J.; Chen, C.; Palumbo, J.D.; Bianchini, A.; Cappozzo, J.; Stratton, J.; Ryu, D.; Wu, F. A risk assessment of dietary Ochratoxin a in the United States. Food Chem. Toxicol. 2017, 100, 265–273. [Google Scholar] [CrossRef] [Green Version]
- Foerster, C.; Muñoz, K.; Delgado-Rivera, L.; Rivera, A.; Cortés, S.; Müller, A.; Arriagada, G.; Ferreccio, C.; Rios, G. Occurrence of relevant mycotoxins in food commodities consumed in Chile. Mycotoxin Res. 2020, 36, 63–72. [Google Scholar] [CrossRef]
- Al Ayoubi, M.; Solfrizzo, M.; Gambacorta, L.; Watson, I.; El Darra, N. Risk of exposure to aflatoxin B1, ochratoxin A, and fumonisin B1 from spices used routinely in Lebanese cooking. Food Chem. Toxicol. 2021, 147, 111895. [Google Scholar] [CrossRef]
- Meerpoel, C.; Vidal, A.; Andjelkovic, M.; de Boevre, M.; Tangni, E.K.; Huybrechts, B.; Devreese, M.; Croubels, S.; de Saeger, S. Dietary exposure assessment and risk characterization of citrinin and ochratoxin A in Belgium. Food Chem. Toxicol. 2021, 147, 111914. [Google Scholar] [CrossRef]
- Ostry, V.; Malir, F.; Dofkova, M.; Skarkova, J.; Pfohl-Leszkowicz, A.; Ruprich, J. Ochratoxin a dietary exposure of ten population groups in The Czech Republic: Comparison with data over the world. Toxins 2015, 7, 3608–3635. [Google Scholar] [CrossRef] [Green Version]
- Kulahi, A.; Kabak, B. A preliminary assessment of dietary exposure of ochratoxin A in Central Anatolia Region, Turkey. Mycotoxin Res. 2020, 36, 327–337. [Google Scholar] [CrossRef]
- Iqbal, S.Z.; Asi, M.R.; Hanif, U.; Zuber, M.; Jinap, S. The presence of aflatoxins and ochratoxin A in rice and rice products; And evaluation of dietary intake. Food Chem. 2016, 210, 135–140. [Google Scholar] [CrossRef]
- Golge, O.; Kabak, B. First report: Exposure estimates to ochratoxin A through wheat bread and rice intake in Turkey. J. Cereal Sci. 2016, 69, 213–217. [Google Scholar] [CrossRef]
- Hathout, A.S.; Abel-Fattah, S.M.; Abou-Sree, Y.H.; Fouzy, A.S.M. Incidence and exposure assessment of aflatoxins and ochratoxin A in Egyptian wheat. Toxicol. Rep. 2020, 7, 867–873. [Google Scholar] [CrossRef]
- Duarte, S.C.; Bento, J.M.V.; Pena, A.; Lino, C.M. Ochratoxin A exposure assessment of the inhabitants of Lisbon during winter 2007/2008 through bread and urine analysis. Food Addit. Contam. 2009, 26, 1411–1420. [Google Scholar] [CrossRef]
- Tabarani, A.; Zinedine, A.; Bouchriti, N.; Abdennebi, E.H. Exposure assessment to ochratoxin A through the intake of three cereal derivatives from the Moroccan market. Food Res. Int. 2020, 137, 109464. [Google Scholar] [CrossRef]
- Zinedine, A.; Fernández-Franzón, M.; Mañes, J.; Manyes, L. Multi-mycotoxin contamination of couscous semolina commercialized in Morocco. Food Chem. 2017, 214, 440–446. [Google Scholar] [CrossRef]
- Kolakowski, B.; O’rourke, S.M.; Bietlot, H.P.; Kurz, K.; Aweryn, B. Ochratoxin A concentrations in a variety of grain-based and non-grain-based foods on the Canadian retail market from 2009 to 2014. J. Food Prot. 2016, 79, 2143–2159. [Google Scholar] [CrossRef]
- Hassan, A.M.; Sheashaa, H.A.; Fattah, M.F.A.; Ibrahim, A.Z.; Gaber, O.A.; Sobh, M.A. Study of ochratoxin A as an environmental risk that causes renal injury in breast-fed Egyptian infants. Pediatr. Nephrol. 2006, 21, 102–105. [Google Scholar] [CrossRef]
- Huong, B.T.M.; Tuyen, L.D.; Tuan, D.H.; Brimer, L.; Dalsgaard, A. Dietary exposure to aflatoxin B1, ochratoxin A and fuminisins of adults in Lao Cai province, Viet Nam: A total dietary study approach. Food Chem. Toxicol. 2016, 98, 127–133. [Google Scholar] [CrossRef]
- Wikandari, R.; Mayningsih, I.C.; Sari, M.D.P.; Purwandari, F.A.; Setyaningsih, W.; Rahayu, E.S.; Taherzadeh, M.J. Assessment of microbiological quality and mycotoxin in dried chili by morphological identification, molecular detection, and chromatography analysis. Int. J. Environ. Res. Public Health 2020, 17, 1847. [Google Scholar] [CrossRef] [Green Version]
- Gambacorta, L.; Magistà, D.; Perrone, G.; Murgolo, S.; Logrieco, A.F.; Solfrizzo, M. Co-occurrence of toxigenic moulds, aflatoxins, ochratoxin A, Fusarium and Alternaria mycotoxins in fresh sweet peppers (Capsicum annuum) and their processed products. World Mycotoxin J. 2018, 11, 159–174. [Google Scholar] [CrossRef]
- Abrunhosa, L.; Morales, H.; Soares, C.; Calado, T.; Vila-Chã, A.S.; Pereira, M.; Venâncio, A. A Review of Mycotoxins in Food and Feed Products in Portugal and Estimation of Probable Daily Intakes. Crit. Rev. Food Sci. Nutr. 2016, 56, 249–265. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- El Darra, N.; Gambacorta, L.; Solfrizzo, M. Multimycotoxins occurrence in spices and herbs commercialized in Lebanon. Food Control 2019, 95, 63–70. [Google Scholar] [CrossRef]
- Al Jabir, M.; Barcaru, A.; Latiff, A.; Jaganjac, M.; Ramadan, G.; Horvatovich, P. Dietary exposure of the Qatari population to food mycotoxins and reflections on the regulation limits. Toxicol. Rep. 2019, 6, 975–982. [Google Scholar] [CrossRef] [PubMed]
- Muñoz, K.; Cramer, B.; Dopstadt, J.; Humpf, H.U.; Degen, G.H. Evidence of ochratoxin A conjugates in urine samples from infants and adults. Mycotoxin Res. 2017, 33, 39–47. [Google Scholar] [CrossRef]
- Sueck, F.; Specht, J.; Cramer, B.; Humpf, H. Identification of ochratoxin-N-acetyl-L-cysteine as a new ochratoxin A metabolite and potential biomarker in human urine. Mycotoxin Res. 2020, 36, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Solfrizzo, M.; Gambacorta, L.; Lattanzio, V.M.T.; Powers, S.; Visconti, A. Simultaneous LC-MS/MS determination of aflatoxin M1, ochratoxin A, deoxynivalenol, de-epoxydeoxynivalenol, α and β-zearalenols and fumonisin B1 in urine as a multi-biomarker method to assess exposure to mycotoxins. Anal. Bioanal. Chem. 2011, 401, 2831–2841. [Google Scholar] [CrossRef]
- Ali, N.; Degen, G.H. Biological monitoring for ochratoxin A and citrinin and their metabolites in urine samples of infants and children in Bangladesh. Mycotoxin Res. 2020, 36, 409–417. [Google Scholar] [CrossRef]
- Ahna, J.; Kima, D.; Kima, H.; Jahngb, K.Y. Quantitative determination of mycotoxins in urine by LC-MS/MS. Food Addit. Contam. 2010, 27, 1674–1682. [Google Scholar] [CrossRef]
- Lemming, E.W.; Montes, A.M.; Schmidt, J.; Cramer, B.; Humpf, H.; Moraeus, L.; Olsen, M. Mycotoxins in blood and urine of Swedish adolescents—Possible associations to food intake and other background characteristics. Mycotoxin Res. 2019, 36, 193–206. [Google Scholar] [CrossRef] [Green Version]
- Turner, P.C.; Snyder, J.A. Development and limitations of exposure biomarkers to dietary contaminants mycotoxins. Toxins 2021, 13, 314. [Google Scholar] [CrossRef]
- Naja, F.; Hwalla, N.; Itani, L.; Baalbaki, S.; Sibai, A.; Nasreddine, L. A novel Mediterranean diet index from Lebanon: Comparison with Europe. Eur. J. Nutr. 2015, 54, 1229–1243. [Google Scholar] [CrossRef] [Green Version]
- Akdemir, C.; Ulker, O.C.; Basaran, A.; Ozkaya, S.; Karakaya, A. Estimation of ochratoxin A in some Turkish populations: An analysis in urine as a simple, sensitive and reliable biomarker. Food Chem. Toxicol. 2010, 48, 877–882. [Google Scholar] [CrossRef]
- Heyndrickx, E.; Sioen, I.; Huybrechts, B.; Callebaut, A.; de Henauw, S.; de Saeger, S. Human biomonitoring of multiple mycotoxins in the Belgian population: Results of the BIOMYCO study. Environ. Int. 2015, 84, 82–89. [Google Scholar] [CrossRef]
- Mitropoulou, A.; Gambacorta, L.; Warensjö Lemming, E.; Solfrizzo, M.; Olsen, M. Extended evaluation of urinary multi-biomarker analyses of mycotoxins in Swedish adults and children. World Mycotoxin J. 2018, 11, 647–659. [Google Scholar] [CrossRef]
- Jager, A.V.; Tonin, F.G.; Souto, P.C.M.C.; Privatti, R.T. Determination of Urinary Biomarkers for Assessment of Short-Term Human Exposure to Aflatoxins in São Paulo, Brazil. Toxins 2014, 6, 1996–2007. [Google Scholar] [CrossRef] [Green Version]
- Vettorazzi, A.; Trocóniz, I.F.; Gonzalez-Peñas, E.; Corcuera, L.A.; Arbillaga, L.; Gil, A.G.; Nagy, J.M.; Mantle, P.G.; López de Cerain, A. Effects of fasting and gender on ochratoxin A toxicokinetics in F344 rats. Food Chem. Toxicol. 2010, 48, 3159–3166. [Google Scholar] [CrossRef]
- Kouadio, J.H.; Lattanzio, V.M.T.; Ouattara, D.; Kouakou, B.; Visconti, A. Assessment of mycotoxin exposure in Côte D’ivoire (Ivory Coast) through multi-biomarker analysis and possible correlation with food consumption patterns. Toxicol. Int. 2014, 21, 248–257. [Google Scholar] [CrossRef] [Green Version]
- Jeswal, P.; Kumar, D.; Kumar, M. Evaluation of Mycotoxigenic Fungi and Aflatoxins, Ochratoxin A and Citrinin Contamination in some Dried Fruits and Nuts from Bihar (India). Int. J. Biotechnol. Biomed. Sci. 2017, 3, 48–51. [Google Scholar]
- Chen, C.; Wu, F. The need to revisit ochratoxin A risk in light of diabetes, obesity, and chronic kidney disease prevalence. Food Chem. Toxicol. 2017, 103, 79–85. [Google Scholar] [CrossRef]
- El Khoury, R.; Mathieu, F.; Atoui, A.; Kawtharani, H.; El Khoury, A.; Afif, C.; Maroun, R.G.; El Khoury, A. Ability of soil isolated actinobacterial strains to prevent, bind and biodegrade ochratoxin A. Toxins 2017, 9, 222. [Google Scholar] [CrossRef] [Green Version]
- Creppy, E.E.; Baudrimont, I.; Betbeder, A.M. Prevention of nephrotoxicity of ochratoxin A, a food contaminant. Toxicol. Lett. 1995, 82, 869–877. [Google Scholar] [CrossRef]
- Al-Jaal, B.A.; Jaganjac, M.; Barcaru, A.; Horvatovich, P.; Latiff, A. Aflatoxin, fumonisin, ochratoxin, zearalenone and deoxynivalenol biomarkers in human biological fluids: A systematic literature review, 2001–2018. Food Chem. Toxicol. 2019, 129, 211–228. [Google Scholar] [CrossRef] [Green Version]
- Dekant, R.; Langer, M.; Lupp, M.; Adaku Chilaka, C.; Mally, A. In Vitro and In Vivo Analysis of Ochratoxin A-Derived Glucuronides and Mercapturic Acids as Biomarkers of Exposure. Toxins 2021, 13, 587. [Google Scholar] [CrossRef]
- CDC. Urine Output. Available online: https://www.cdc.gov/dengue/training/cme/ccm/page57297.html (accessed on 4 November 2021).
- Gambacorta, L.; Olsen, M.; Solfrizzo, M. Pig urinary concentration of mycotoxins and metabolites reflects regional differences, mycotoxin intake and feed contaminations. Toxins 2019, 11, 378. [Google Scholar] [CrossRef] [PubMed] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| All Participants | Males | Females | Two-Tailed p-Value | |
| N. of participants | 44 | 17 (38.6%) | 27 (61.4%) | N/A |
| Mean body weight (kg) | 52.5 | 51.3 | 53.3 | 0.6037 |
| Mean of 24 h diet weight (g) | 412.36 | 482.8 | 366.3 | 0.0041 |
| Mean of dinner weight (g) | 68.89 | 65.8 | 71.2 | 0.6138 |
| Males | Females | Two-Tailed p-value | ||
| Mean OTA in positive 24 h diet (ng/g) | 0.33 | 0.31 | 0.7671 | |
| Mean OTA in positive dinner (ng/g) | 0.3 | 0.33 | 0.8374 | |
| Mean OTA in urine (ng/mL) | 0.021 | 0.022 | 0.7643 | |
| Positive 24 h Diet | All 24 h Diet a | Urine | Positive Dinner | All Dinner 1 b | All Dinner 2 c | |
|---|---|---|---|---|---|---|
| Mean ± SD e | 0.32 ± 0.1 | 0.16 ± 0.16 (nd = LOD/2) | 0.022 ± 0.012 | 0.32 ± 0.18 | 0.08 ± 0.16 (nd = 0) | 0.12 ± 0.15 (nd = LOD) |
| Median (range) e | 0.29 (0.18–0.55) | 0.03 (0.03–0.55) | 0.019 (0.007–0.058) | 0.23 (0.18–0.76) | 0 (0–0.76) | 0.05 (0.05–0.76) |
| Mean PDI | 2.78 ± 1.65 | 1.4 ± 1.71 | 21.731 ± 13.8 | 19.59 ± 13.89 d | 4.9 ± 10.87 d | 7.62 ± 9.77 d |
| Median (range) PDI | 2.32 (0.6–5.93) | 0.32 (0.1–5.93) | 17.995 (5.6–63.8) | 15.89 (5.63–53.07) d | 0 (0–53.07) d | 3.88 (1.73–53.07) d |
| Mean MOE (neo) ± SD (% of limit) | 7907 ± 5922 (79) | 47342 ± 43827 (473) | 961 ± 599 (10) | N/A | N/A | N/A |
| median MOE (neo) | 6254 | 45414 | 806 | N/A | N/A | N/A |
| Range MOE (neo) (% of limit) | 2447–24344 (24–243) | 2447–152016 (24–1520) | 227–2585 (2–26) | N/A | N/A | N/A |
| mean moe (non–neo) ± SD (% of limit) | 2579 ± 1932 (1290) | 15443 ± 14297 (7722) | 313 ± 195 (157) | N/A | N/A | N/A |
| median MOE (non–neo) | 2040 | 14814 | 263 | N/A | N/A | N/A |
| Range MOE (non–neo) (% of limit) | 798–7941 (399–3971) | 798–49589 (399–24794) | 74–843 (37–422) | N/A | N/A | N/A |
| Mean PDI (ng/kg-bw) | Mean MOE (% of Limit) | ||
|---|---|---|---|
| Diet | |||
| This study | 1.4 | Neo | 47,342 (473) |
| Non-neo | 15,443 (7722) | ||
| Bakker et al., (2009) [26] | 4.1 | Neo | 3537 (35) |
| Non-neo | 1154 (577) | ||
| Sizoo and Van Egmond (2005) [28] | 1.2 | Neo | 12,083 (121) |
| Non-neo | 3942 (1971) | ||
| Bakker and Pieters (2002) [27] | 1 | Neo | 14,500 (145) |
| Non-neo | 4730 (2365) | ||
| Urine | |||
| This study | 21.73 | Neo | 961 (10) |
| Non-neo | 313 (157) | ||
| Solfrizzo et al., (2014) [21] | 139 | Neo | 104 (1) |
| Non-neo | 34 (17) | ||
| Silva et al., (2019) [29] | 33 | Neo | 439 (4) |
| Non-neo | 143 (72) | ||
| Franco et al., (2019) [30] | 31 | Neo | 468 (5) |
| Non-neo | 153 (76) | ||
| Martins et al., (2019) [31] | 5 (median PDI) | Neo | 2900 (29) a |
| Non-neo | 946 (473) a | ||
| Category | Food Type | PDI (EDI) ng/kg-bw/d | Population Age | Country | Reference |
|---|---|---|---|---|---|
| Grains and grain-based products (cereals) | Grains and grain-based products (cereals) d | 0.72 a | Children (11–14) | Czech Republic | (Ostry et al., 2015) [40] |
| 2.215 | Adults | Turkey | (Kulahi & Kabak, 2020) [41] | ||
| Rice | 0 | Adults (46.6 ± 17.0) | Brazil | (Franco et al., 2019) [30] | |
| 0.14 | Adults | Turkey | (Kulahi & Kabak, 2020) [41] | ||
| 24.7 b | - | Pakistan | (Iqbal et al., 2016) [42] | ||
| 0.02 | Adults | Turkey | (Golge & Kabak, 2016) [43] | ||
| 0.309 | 10–17 | Belgium | (Meerpoel et al., 2021) [39] | ||
| Wheat | 50–2170 | Adults | Egypt | (Hathout et al., 2020) | |
| Wheat flour | 0 | Adults (46.6 ± 17.0) | Brazil | (Franco et al., 2019) [30] | |
| 0.016 | 10–17 | Belgium | (Meerpoel et al., 2021) [39] | ||
| Wheat bread | 0.21 | Adults (18–75) | Portugal | (Duarte et al., 2009) [8] | |
| 1.789 | Adults | Turkey | (Kulahi & Kabak, 2020) [41] | ||
| 1.51 | Adults | Morocco | (Tabarani et al., 2020) [46] | ||
| 0.85 | Adults | Turkey | (Golge & Kabak, 2016) [43] | ||
| 0.136 | 10-17 | Belgium | (Meerpoel et al., 2021) [39] | ||
| Couscous semolina | 4 | Adults | Morocco | (Zinedine et al., 2017) [47] | |
| Semolina | 0.18 | Adults | Morocco | (Tabarani et al., 2020) [46] | |
| Pasta | 0.132 | Adults | Turkey | (Kulahi & Kabak, 2020) [41] | |
| 0.25 | Adults | Morocco | (Tabarani et al., 2020) [46] | ||
| Cereal-based snacks | 0.153 | Adults | Turkey | (Kulahi & Kabak, 2020) [41] | |
| Biscuits | 0.094 | 10–17 | Belgium | (Meerpoel et al., 2021) [39] | |
| Confectionery c | Confectionery | 0.1 a | Children (11–14) | Czech Republic | (Ostry et al., 2015) [40] |
| Chocolate | 0.106 | Adults | Turkey | (Kulahi & Kabak, 2020) [41] | |
| Cocoa | Cocoa | 0.015 a | Children (11–14) | Czech Republic | (Ostry et al., 2015) [40] |
| 0.03 | Adolescent (12–18) | United States | (Mitchell et al., 2017) [36] | ||
| Nuts | Nuts | 0.106 | Adults | Turkey | (Kulahi & Kabak, 2020) [41] |
| Dried fruits | Dried fruits | 0.001 | Children (11–14) | Czech Republic | (Ostry et al., 2015) [40] |
| 0.051 | Adults | Turkey | (Kulahi & Kabak, 2020) [41] | ||
| Dried dates | 0.13 | Adults | Tunisia | (Azaiez et al., 2015) | |
| Dried figs | 0.01 | Adolescent (12–18) | United sStates | (Mitchell et al., 2017) [36] | |
| Dried raisins | 0.006 | Adolescent (12–18) | United States | (Mitchell et al., 2017) [36] | |
| Spices, seasoning, and legumes | Spices, seasoning and legumes | 0.155 a | Children (11–14) | Czech Republic | (Ostry et al., 2015) [40] |
| Beans | 0 | Adults (46.6 ± 17.0) | Brazil | (Franco et al., 2019) [30] | |
| Capsicum | 23.8 | Adults | Chile | (Foerster et al., 2019) [30] | |
| Chili | 0.011 | Adults | Turkey | (Kulahi & Kabak, 2020) [41] | |
| Red chili | 0.11 | Adults | Lebanon | (Al Ayoubi et al., 2021) [38] | |
| Black pepper | 0.03 | Adults | Lebanon | (Al Ayoubi et al., 2021) [38] | |
| Herbs | Tea | 0.87 a | Children (11–14) | Czech Republic | (Ostry et al., 2015) [40] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Al Ayoubi, M.; Salman, M.; Gambacorta, L.; El Darra, N.; Solfrizzo, M. Assessment of Dietary Exposure to Ochratoxin A in Lebanese Students and Its Urinary Biomarker Analysis. Toxins 2021, 13, 795. https://0-doi-org.brum.beds.ac.uk/10.3390/toxins13110795
Al Ayoubi M, Salman M, Gambacorta L, El Darra N, Solfrizzo M. Assessment of Dietary Exposure to Ochratoxin A in Lebanese Students and Its Urinary Biomarker Analysis. Toxins. 2021; 13(11):795. https://0-doi-org.brum.beds.ac.uk/10.3390/toxins13110795
Chicago/Turabian StyleAl Ayoubi, Manar, Mohammad Salman, Lucia Gambacorta, Nada El Darra, and Michele Solfrizzo. 2021. "Assessment of Dietary Exposure to Ochratoxin A in Lebanese Students and Its Urinary Biomarker Analysis" Toxins 13, no. 11: 795. https://0-doi-org.brum.beds.ac.uk/10.3390/toxins13110795