Assessment and Management of Platinum-Related Ototoxicity in Children Treated for Cancer


Abstract
:1. Introduction
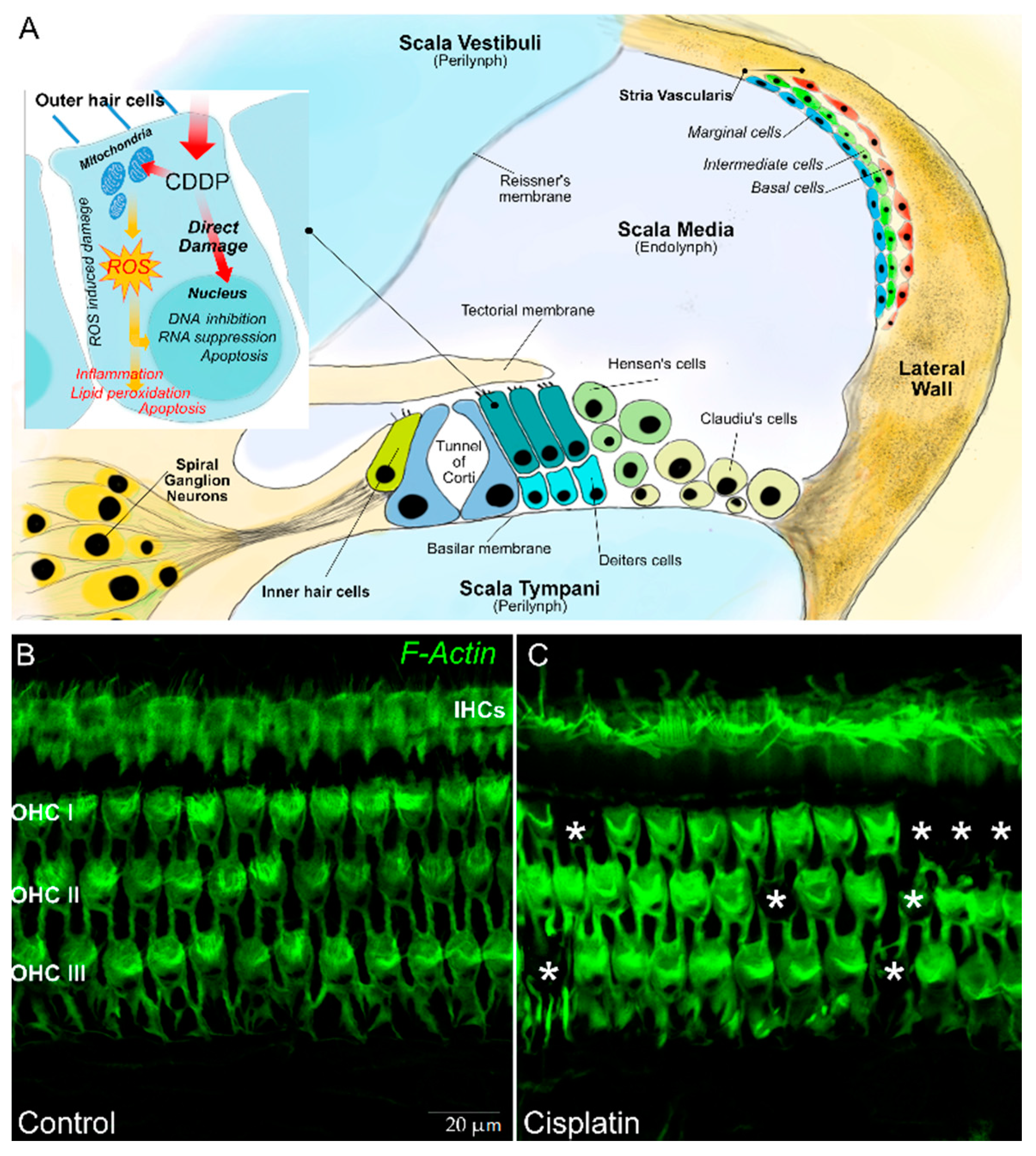
2. Pathogenesis of Hearing Damage from Platinum Compounds
3. Assessment of the Hearing Function during Treatment with Platinum Compounds
4. Audiological Follow-Up after Therapy with Platinum Compounds
5. Strategies of Prevention of Hearing Loss
6. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Knight, K.R.; Kraemer, D.F.; Neuwelt, E.A. Ototoxicity in children receiving platinum chemotherapy: Underestimating a commonly occurring toxicity that may influence academic and social development. J. Clin. Oncol. 2005, 23, 8588–8596. [Google Scholar] [CrossRef] [Green Version]
- Van den Berg, H.; Van den Anker, J.N.; Beijnen, J.H. Cytostatic drugs in infants: A review on pharmacokinetic data in infants. Cancer Treat Rev. 2012, 18, 3–26. [Google Scholar] [CrossRef]
- Ruggiero, A.; Trombatore, G.; Triarico, S.; Arena, R.; Ferrara, P.; Scalzone, M.; Pierri, F.; Riccardi, R. Platinum compounds in children with cancer: Toxicity and clinical management. Anticancer Drugs 2013, 24, 1007–1019. [Google Scholar] [CrossRef]
- Boulikas, T.; Pantos, A.; Bellis, E.; Petros, C. Designing platinum compounds in cancer: Structures and mechanisms. Cancer Ther. 2007, 5, 537–583. [Google Scholar]
- O’Dwyer, P.J.; Stevenson, J.P.; Johnson, S.W. Clinical pharmacokinetics and administration of established platinum drugs. Drugs 2000, 59, 19–27. [Google Scholar] [CrossRef]
- Lokich, J.; Anderson, N. Carboplatin versus cisplatin in solid tumors: An analysis of the literature. Ann. Oncol. 1998, 9, 13–21. [Google Scholar] [CrossRef]
- Peng, B.; English, M.W.; Boddy, A.V.; Price, L.; Wyllie, R.; Pearson, A.D.J.; Tilby, M.J.; Newell, D.R. Cisplatin pharmacokinetics in children with cancer. Eur. J. Cancer 1997, 33, 1823–1828. [Google Scholar] [CrossRef]
- Go, R.S.; Adjei, A.A. Review of the comparative pharmacology and clinical activity of cisplatin and carboplatin. J. Clin. Oncol. 1999, 17, 409–422. [Google Scholar] [CrossRef]
- Breglio, A.M.; Rusheen, A.E.; Shide, E.D.; Fernandez, K.A.; Spielbauer, K.K.; McLachlin, K.M.; Hall, M.D.; Amable, L.; Cunningham, L.L. Cisplatin is retained in the cochlea indefinitely following chemotherapy. Nat. Commun. 2017, 8, 1654. [Google Scholar] [CrossRef] [Green Version]
- UpToDate. Cisplatin: Drug Information. Available online: http://www.uptodate.com (accessed on 30 March 2020).
- Pussegoda, K.; Ross, C.J.; Visscher, H.; Yazdanpanah, M.; Brooks, B.; Rassekh, S.R.; Zada, Y.F.; Dubé, M.P.; Carleton, B.C.; Hayden, M.R.; et al. Replication of TPMT and ABCC3 genetic variants highly associated with cisplatin-induced hearing loss in children. Clin. Pharmacol. Ther. 2013, 94, 243–251. [Google Scholar] [CrossRef]
- Nakamura, T.; Yonezawa, A.; Hashimoto, S.; Katsura, T.; Inui, K. Disruption of multidrug and toxin extrusion MATE1 potentiates cisplatin-induced nephrotoxicity. Biochem. Pharmacol. 2010, 80, 1762–1767. [Google Scholar] [CrossRef] [Green Version]
- Kanat, O.; Ertas, H.; Caner, B. Platinum-induced neurotoxicity: A review of possible mechanisms. World J. Clin. Oncol. 2017, 8, 329–335. [Google Scholar] [CrossRef]
- Knox, R.J.; Friedlos, F.; Lydall, D.A.; Roberts, J.J. Mechanism of cytotoxicity of anticancer platinum drugs: Evidence that cis-diam-minedi-chloroplatinum (II) and cis-diammine (1,1-cyclobutane-diacarbo-xylate) platinum (II) differ only in kinetics of their interaction with DNA. Cancer Res. 1986, 46, 1972–1979. [Google Scholar]
- Micetich, K.C.; Barnes, D.; Erickson, L.C. A comparative study of the cytotoxicity and DNA-damaging effects of cis-(diammino) (1,1- cyclobutanedicarboxylato)-platinum (II) and cis-diamminedichloroplatinum (II) on L1210 cells. Cancer Res. 1985, 45, 4043–4047. [Google Scholar]
- UpToDate. Carboplatin: Drug information. Available online: http://www.uptodate.com (accessed on 30 March 2020).
- Veal, G.J.; Errington, J.; Tilby, M.J.; Pearson, A.D.; Foot, A.B.; McDowell, H.; Ellershaw, C.; Pizer, B.; Nowell, G.M.; Pearson, D.G.; et al. Adaptive dosing and platinum–DNA adduct formation in children receiving high-dose carboplatin for the treatment of solid tumours. Br. J. Cancer 2007, 96, 725–731. [Google Scholar] [CrossRef] [Green Version]
- Lebwohl, D.; Canetta, R. Clinical development of platinum complexes in cancer therapy: An historical perspective and an update. Eur. J. Cancer 1998, 34, 1522–1534. [Google Scholar] [CrossRef]
- Kweekel, D.M.; Gelderblom, H.; Guchelaar, H.J. Pharmacology of oxaliplatin and the use of pharmacogenomics to individualize therapy. Cancer Treat. Rev. 2005, 31, 90–105. [Google Scholar] [CrossRef]
- Di Francesco, A.M.; Ruggiero, A.; Riccardi, R. Cellular and molecular aspects of drugs of the future: Oxaliplatin. Cell. Mol. Life Sci. 2002, 59, 1914–1927. [Google Scholar] [CrossRef]
- Page, J.D.; Husain, I.; Sancar, A.; Chaney, S.G. Effect of the diaminocyclohexane carrier ligand on platinum adduct formation, repair, and lethality. Biochemistry 1990, 29, 1016–1024. [Google Scholar] [CrossRef]
- Fink, D.; Nebel, S.; Aebi, S.; Zheng, H.; Cenni, B.; Nehme, A.; Christen, R.D.; Howell, S.B. The role of DNA mismatch repair in platinum drug resistance. Cancer Res. 1996, 56, 4881–4886. [Google Scholar]
- Vaisman, A.; Varchenko, M.; Umar, A.; Kunkel, T.A.; Risinger, J.I.; Barrett, J.C.; Hamilton, T.C.; Chaney, S.G. The role of hMLH1, hMSH3, and hMSH6 defects in cisplatin and oxaliplatin resistance: Correlation with replicative bypass of platinum–DNA adducts. Cancer Res. 1998, 58, 3579–3585. [Google Scholar]
- Raymond, E.; Lawrence, R.; Izbicka, E.; Faivre, S.; Von Hoff, D.D. Activity of oxaliplatin against human tumor colony forming units. Clin. Cancer Res. 1998, 4, 1021–1029. [Google Scholar]
- Riccardi, A.; Ferlini, C.; Meco, D.; Mastrangelo, R.; Scambia, G.; Riccardi, R. Antitumor activity of oxaliplatin in neuroblastoma cell lines. Eur. J. Cancer 1999, 35, 86–90. [Google Scholar] [CrossRef]
- Bass, J.K.; Knight, K.R.; Yock, T.I.; Chang, K.W.; Cipkala, D.; Grewal, S.S. Evaluation and management of hearing loss in survivors of childhood and adolescent cancers: A report from the children’s oncology group. Pediatr. Blood Cancer 2016, 63, 1152–1162. [Google Scholar] [CrossRef] [Green Version]
- Bertolini, P.; Lassalle, M.; Mercier, G.; Raquin, M.A.; Izzi, G.; Corradini, N.; Hartmann, O. Platinum compound-related ototoxicity in children: Long-term follow-up reveals continuous worsening of hearingloss. J. Pediatr. Hematol. Oncol. 2004, 26, 649–655. [Google Scholar] [CrossRef]
- Hua, C.; Bass, J.K.; Khan, R.; Kun, L.E.; Merchant, T.E. Hearing loss after radiotherapy for Pediatric brain tumors: Effect of cochlear dose. Int. J. Radiat. Oncol. Biol. Phys. 2008, 72, 892–899. [Google Scholar] [CrossRef]
- Kolinsky, D.C.; Hayashi, S.S.; Karzon, R.; Mao, J.; Hayashi, R.J. Late onset hearing loss: A significant complication of cancer survivors treated with cisplatin containing chemotherapy regimens. J. Pediatr. Hematol. Oncol. 2010, 32, 119–123. [Google Scholar] [CrossRef]
- Rybak, L.P.; Whitworth, C.A.; Mukherjea, D.; Ramkumar, V. Mechanisms of cisplatin-induced ototoxicity and prevention. Hear. Res. 2007, 226, 157–167. [Google Scholar] [CrossRef]
- Langer, T.; Zehnhoff-Dinnesen, A.; Radtke, S.; Meitert, J.; Zolk, O. Understanding platinum-induced ototoxicity. Trends Pharmacol. Sci. 2013, 34, 458–469. [Google Scholar] [CrossRef]
- Brock, P.R.; Knight, K.R.; Freyer, D.R.; Campbell, K.C.; Steyger, P.S.; Blakley, B.W.; Rassekh, S.R.; Chang, K.W.; Fligor, B.J.; Rajput, K.; et al. Platinum-induced ototoxicity in children: A consensus review on mechanisms, predisposition, and protection, including a new international society of Pediatric oncology Boston ototoxicity scale. J. Clin. Oncol. 2012, 30, 2408–2417. [Google Scholar] [CrossRef] [Green Version]
- Kopke, R.D.; Liu, W.; Gabaizadeh, R.; Jacono, A.; Feghali, J.; Spray, D.; Garcia, P.; Steinman, H.; Malgrange, B.; Ruben, R.J.; et al. Use of organotypic cultures of Corti’s organ to study the protective effects of antioxidant molecules on cisplatin-induced damage of auditory hair cells. Am. J. Otol. 1997, 18, 559–571. [Google Scholar] [PubMed]
- Dehne, N.; Lautermann, J.; Petrat, F.; Rauen, U.; de Groot, H. Cisplatin ototoxicity: Involvement of iron and enhanced formation of superoxide anion radicals. Toxicol. Appl. Pharmacol. 2001, 174, 27–34. [Google Scholar] [CrossRef] [PubMed]
- Bánfi, B.; Malgrange, B.; Knisz, J.; Steger, K.; Dubois-Dauphin, M.; Krause, K.H. NOX3, a superoxide-generating NADPH oxidase of the inner ear. J. Biol. Chem. 2004, 279, 46065–46072. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rybak, L.P.; Mukherjea, D.; Ramkumar, V. Mechanisms of cisplatin-induced ototoxicity and prevention. In Seminars in Hearing; Thieme Medical Publishers: New York, NY, USA, 2019; Volume 40, pp. 197–204. [Google Scholar] [CrossRef]
- Rybak, L.P.; Husain, K.; Morris, C.; Whitworth, C.; Somani, S. Effect of protective agents against cisplatin ototoxicity. Am. J. Otol. 2000, 21, 513–520. [Google Scholar]
- Paciello, F.; Fetoni, A.; Mezzogori, D.; Rolesi, R.; Di Pino, A.; Paludetti, G.; Grassi, G.; Troiani, D. The dual role of curcumin and ferulic acid in counteracting chemoresistance and cisplatin-induced ototoxicity. Sci. Rep. 2020, 23, 1063. [Google Scholar] [CrossRef] [Green Version]
- Riedemann, L.; Lanvers, C.; Deuster, D.; Peters, U.; Boos, J.; Jürgens, H.; am Zehnhoff-Dinnesen, A. Megalin genetic polymorphisms and individual sensitivity to the ototoxic effect of cisplatin. Pharm. J. 2008, 8, 23–28. [Google Scholar] [CrossRef] [Green Version]
- Xu, X.; Ren, H.; Zhou, B.; Zhao, Y.; Yuan, R.; Ma, R.; Zhou, H.; Liu, Z. Prediction of copper transport protein 1 (CTR1) genotype on severe cisplatin induced toxicity in non-small cell lung cancer (NSCLC) patients. Lung Cancer 2012, 77, 438–442. [Google Scholar] [CrossRef]
- Brusilow, S.W.; Gordes, E. The mutual independence of the endolymphatic potential and the concentrations of sodium and potassium in endolymph. J. Clin. Investig. 1973, 52, 2517–2521. [Google Scholar] [CrossRef] [Green Version]
- Altura, B.M.; Altura, B.T.; Gebrewold, A.; Ising, H.; Günther, T. Magnesium deficiency and hypertension: Correlation between magnesium deficient diets and microcirculatory changes in situ. Science 1984, 223, 1315–1317. [Google Scholar] [CrossRef]
- Brown, R. Ethacrinic acid and furosemide: Possible cochlear sites and mechanisms of ototoxic action. Mednikon 1975, 4, 33–40. [Google Scholar]
- Joachims, Z.; Babisch, W.; Ising, H.; Günther, T.; Handrock, M. Dependence of noise induced hearing loss on perilymph magnesim concentration. J. Acoust. Soc. Am. 1983, 74, 104–108. [Google Scholar] [CrossRef]
- Grewal, S.; Merchant, T.; Reymond, R.; McInerney, M.; Hodge, C.; Shearer, P. Auditory late effects of childhood cancer therapy: A report from the children’s oncology group. Pediatrics 2010, 125, e938–e950. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huang, R.S.; Kistner, E.O.; Bleibel, W.K.; Shukla, S.J.; Dolan, M.E. Effect of population and gender on chemotherapeutic agent-induced cytotoxicity. Mol. Cancer Ther. 2007, 6, 31–36. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martindale, J.L.; Holbrook, N.J. Cellular response to oxidative stress: Signaling for suicide and survival. J. Cell Physiol. 2002, 192, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Faragher, A.J.; Fry, A.M. Nek2A kinase stimulates centrosome disjunction and is required for formation of bipolar mitotic spindles. Mol. Biol. Cell 2003, 14, 2876–2889. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lin, C.P.; Liu, J.D.; Chow, J.M.; Liu, C.R.; Liu, H.E. Small-molecule c-Myc inhibitor, 10058-F4, inhibits proliferation, downregulates human telomerase reverse transcriptase and enhances chemosensitivity in human hepatocellular carcinoma cells. Anticancer Drugs 2007, 18, 161–170. [Google Scholar] [CrossRef]
- Peters, U.; Preisler-Adams, S.; Hebeisen, A.; Hahn, M.; Seifert, E.; Lanvers, C.; Heinecke, A.; Horst, J.; Jürgens, H.; Lamprecht-Dinnesen, A. Glutathione S-transferase genetic polymorphisms and individual sensitivity to the ototoxic effect of cisplatin. Anticancer Drugs 2000, 11, 639–643. [Google Scholar] [CrossRef]
- Oldenburg, J.; Kraggerud, S.M.; Cvancarova, M.; Lothe, R.A.; Fossa, S.D. Cisplatin-induced long-term hearing impairment is associated with specific glutathione S-transferase genotypes in testicular cancer survivors. J. Clin. Oncol. 2007, 25, 708–714. [Google Scholar] [CrossRef]
- Peters, U.; Preisler-Adams, S.; Lanvers-Kaminsky, C.; Jürgens, H.; Lamprecht-Dinnesen, A. Sequence variations of mitochondrial DNA and individual sensitivity to the ototoxic effect of cisplatin. Anticancer Res. 2003, 23, 1249–1255. [Google Scholar]
- Knoll, C.; Smith, R.J.; Shores, C.; Blatt, J. Hearing genes and cisplatin deafness: A pilot study. Laryngoscope 2009, 116, 72–74. [Google Scholar] [CrossRef]
- Clemens, E.; Broer, L.; Langer, T.; Uitterlinden, A.G.; de Vries, A.C.H.; van Grotel, M.; Pluijm, S.F.M.; Binder, H.; Byrne, J.; Broeder, E.V.D.; et al. Genetic variation of cisplatin-induced ototoxicity in non-cranial-irradiated pediatric patients using a candidate gene approach: The International PanCareLIFE Study. Pharm. J. 2020, 20, 294–305. [Google Scholar] [CrossRef]
- Li, Y.; Womer, R.B.; Silber, J.H. Predicting cisplatin ototoxicity in children: The infl uence of age and the cumulative dose. Eur. J. Cancer 2004, 40, 2445–2451. [Google Scholar] [CrossRef] [PubMed]
- Lanvers-Kaminsky, C.; Zehnhoff-Dinnesen, A.A.; Parfitt, R.; Ciarimboli, G. Drug-induced ototoxicity: Mechanisms, pharmacogenetics, and protective strategies. Clin. Pharmacol. Ther. 2017, 101, 491–500. [Google Scholar] [CrossRef] [PubMed]
- Shi, X.; Nuttall, A.L. Upregulated iNOS and oxidative damage to the cochlear stria vascularis due to noise stress. Brain Res. 2003, 967, 1–10. [Google Scholar] [CrossRef]
- Ding, D.; Allman, B.L.; Salvi, R. Ototoxic characteristics of platinum antitumor drugs. Anat. Rec. 2012, 295, 1851–1867. [Google Scholar] [CrossRef] [PubMed]
- Gratton, M.A.; Salvi, R.J.; Kamen, B.A.; Saunders, S.S. Interaction of cisplatin and noise on the peripheral auditory system. Hear. Res. 1990, 50, 211–223. [Google Scholar] [CrossRef]
- Rabiço-Costa, D.; Gil-da-Costa, M.J.; Barbosa, J.P.; Bom-Sucesso, M.; Spratley, J. Platinum-drugs ototoxicity in Pediatric patients with brain tumors: A 10-year review. J. Pediatr. Hematol. Oncol. 2020, 42, e25–e31. [Google Scholar] [CrossRef]
- Khan, A.; Budnick, A.; Barnea, D.; Feldman, D.R.; Oeffinger, K.C.; Tonorezos, E.S. Hearing loss in adult survivors of childhood cancer treated with radiotherapy. Child. Basel 2018, 5, 59. [Google Scholar] [CrossRef] [Green Version]
- Bass, J.K.; Huang, J.; Onar-Thomas, A.; Chang, K.W.; Bhagat, S.P.; Chintagumpala, M.; Bartels, U.; Gururangan, S.; Hassall, T.; Heath, J.A.; et al. Concordance between the Chang and the International Society of Pediatric Oncology (SIOP) Ototoxicity Grading Scales in patients treated with cisplatin for medulloblastoma. Pediatr. Blood Cancer 2014, 61, 601–605. [Google Scholar] [CrossRef] [Green Version]
- Delpire, E.; Lu, J.; England, R.; Dull, C.; Thorne, T. Deafness and imbalance associated with inactivation of the secretory Na-K-2Cl co-transporter. Nat. Genet. 1999, 22, 192–195. [Google Scholar] [CrossRef]
- Farinetti, A.; Raji, A.; Wu, H.; Wanna, B.; Vincent, C. International consensus (ICON) on audiological assessment of hearing loss in children. Eur. Ann. Otorhinolaryngol. Head Neck Dis. 2018, 135, S41–S48. [Google Scholar] [CrossRef] [PubMed]
- Anastasio, A.R.; Radael, R.D.; Cavalcante, J.M.; Hatzopoulos, S. A report of extended high frequency audiometry thresholds in school-age children with no hearing complaints. Audiol. Res. 2012, 17, 2–8. [Google Scholar] [CrossRef]
- Hunter, L.L.; Monson, B.B.; Moore, D.R.; Dhar, S.; Wright, B.A.; Munro, K.J.; Zadeh, L.M.; Blankenship, C.M.; Stiepan, S.M.; Siegel, J.H.; et al. Extended High Frequency Hearing and Speech Perception Implications in Adults and Children. Hear. Res. 2020, 18, 107922. [Google Scholar] [CrossRef] [PubMed]
- Durrant, J.D.; Campbell, K.; Fausti, S.; Guthrie, O.; Jacobson, G.; Lonsbury-Martin, B.L.; Poling, G. American Academy of Audiology Position Statement and Clinical Practice Guidelines: Ototoxicity Monitoring. 2009. Available online: http://www.audiology.org/resources/documentlibrary/Documents/OtoMonGuidelines (accessed on 30 March 2020).
- Fausti, S.A.; Thompson, M.; Williams, J.; Bouchard, K.R.; Farrer, S.M.; Heifer, K.S.; McHaney, V.A.; Tysklind, J.M.; Durrant, J.; Fowler, C.; et al. Audiologic Management of Individuals Receiving Cochleotoxic Drug Therapy, American Speech-Language-Hearing Association. 1994. Available online: http://www.asha.org/policy/GL1994-00003.htm (accessed on 30 March 2020).
- Knight, K.R.; Chen, L.; Freyer, D.; Aplenc, R.; Bancroft, M.; Bliss, B.; Dang, H.; Gillmeister, B.; Hendershot, E.; Kraemer, D.F.; et al. Group-wide, prospective study of ototoxicity assessment in children receiving cisplatin chemotherapy (ACCL05C1): A report from the children’s oncology group. J. Clin. Oncol. 2017, 35, 440–445. [Google Scholar] [CrossRef]
- King, K.A.; Brewer, C.C. Clinical trials, ototoxicity grading scales, and the audiologist’s role in therapeutic decision making. Int. J. Audiol. 2018, 57, S89–S98. [Google Scholar] [CrossRef] [Green Version]
- Clemens, E.; van den Heuvel-Eibrink, M.M.; Mulder, R.L.; Kremer, L.C.M.; Hudson, M.M.; Skinner, R.; Constine, L.S.; Bass, J.K.; Kuehni, C.E.; Langer, T.; et al. International guideline harmonization group ototoxicity group. Recommendations for ototoxicity surveillance for childhood, adolescent, and young adult cancer survivors: A report from the international late effects of childhood cancer guideline harmonization group in collaboration with the pancare consortium. Lancet Oncol. 2019, 20, e29–e41. [Google Scholar] [CrossRef]
- Lewis, M.J.; Du Bois, S.G.; Fligor, B.; Li, X.; Goorin, A.; Grier, H.E. Ototoxicity in children treated for osteosarcoma. Pediatr. Blood Cancer 2009, 52, 387–391. [Google Scholar] [CrossRef]
- Peleva, E.; Emami, N.; Alzahrani, M.; Bezdjian, A.; Gurberg, J.; Carret, A.S.; Daniel, S.J. Incidence of platinum-induced ototoxicity in Pediatric patients in Quebec. Pediatr. Blood Cancer 2014, 61, 2012–2017. [Google Scholar] [CrossRef]
- Stöhr, W.; Langer, T.; Kremers, A.; Bielack, S.; Lamprecht-Dinnesen, A.; Frey, E.; Beck, J.D. german late effects working group in the german society of Pediatric oncology and hematology. Cisplatin-induced ototoxicity in osteosarcoma patients: A report from the late effects surveillance system. Cancer Investig. 2005, 23, 201–207. [Google Scholar] [CrossRef]
- Coradini, P.P.; Cigana, L.; Selistre, S.G.; Rosito, L.S.; Brunetto, A.L. Ototoxicity from cisplatin therapy in childhood cancer. J. Pediatr. Hematol. Oncol. 2007, 29, 355–360. [Google Scholar] [CrossRef]
- Fetoni, A.R.; Ruggiero, A.; Lucidi, D.; De Corso, E.; Sergi, B.; Conti, G.; Paludetti, G. Audiological monitoring in children treated with platinum chemotherapy. Audiol. Neurootol. 2016, 21, 203–211. [Google Scholar] [CrossRef] [PubMed]
- Stachler, R.J.; Chandrasekhar, S.S.; Archer, S.M.; Rosenfeld, R.M.; Schwartz, S.R.; Barrs, D.M.; Brown, S.R.; Fife, T.D.; Ford, P.; Ganiats, T.G.; et al. American academy of otolaryngology-head and neck surgery. Clinical practice guideline: Sudden hearing loss. Otolaryngol. Head Neck Surg. 2012, 146, S1–S35. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- NICE: London. National Institute for Health and Care Excellence. Cochlear Implants for Children and Adults with Severe to Profound Deafness. 2009. Available online: https://www.nice.org.uk/guidance/ta166 (accessed on 30 March 2020).
- New York State Department of Health. Clinical Practice Guideline: Report of the Recommendations. Hearing Loss: Assessment and Intervention for Young Children (Age 0–3 Years). 2007. Available online: https://www.health.ny.gov/community/infants_children/early_intervention/docs/guidelines_hearing_loss_recommendations.pdf (accessed on 30 March 2020).
- American Association of Audiology. Clinical Practice Guidelines on Pediatric Amplification. 2013. Available online: http://galster.net/wp-content/uploads/2013/07/AAA-2013-Pediatric-Amp-Guidelines.pdf (accessed on 30 March 2020).
- Audiology Australia. Professional Practice Standards: Audiological Rehabilitation. 2013. Available online: https://audiology.asn.au/Tenant/C0000013/Position%20Papers/Member%20Resources/Clinical%20Standards%20partb%20-%20whole%20document%20July13%201 (accessed on 30 March 2020).
- Fetoni, A.R.; Paciello, F.; Mezzogori, D.; Rolesi, R.; Eramo, S.L.; Paludetti, G.; Troiani, D. Molecular targets for anticancer redox chemotherapy and cisplatin-induced ototoxicity: The role of curcumin on pSTAT3 and Nrf-2 signalling. Br. J. Cancer 2015, 113, 1434–1444. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fetoni, A.R.; Eramo, S.L.; Paciello, F.; Rolesi, R.; Podda, M.V.; Troiani, D.; Paludetti, G. Curcuma longa (curcumin) decreases in vivo cisplatin-induced ototoxicity through heme oxygenase-1 induction. Otol. Neurotol. 2014, 35, e169–e177. [Google Scholar] [CrossRef]
- Fetoni, A.R.; Sergi, B.; Ferraresi, A.; Paludetti, G.; Troiani, D. Protective effects of alpha-tocopherol and tiopronin against cisplatin-induced ototoxicity. Acta Otolaryngol. 2004, 124, 421–426. [Google Scholar] [CrossRef]
- Lafay-Cousin, L.; Purdy, E.; Huang, A.; Cushing, S.L.; Papaioannou, V.; Nettel-Aguirre, A.; Bouffet, E. Early cisplatin induced ototoxicity profile may predict the need for hearing support in children with medulloblastoma. Pediatr. Blood Cancer 2013, 60, 287–292. [Google Scholar] [CrossRef]
- Van As, J.W.; van den Berg, H.; van Dalen, E.C. Medical interventions for the prevention of platinum-induced hearing loss in children with cancer. Cochrane Database Syst. Rev. 2012, 16, CD009219. [Google Scholar] [CrossRef]
- Fouladi, M.; Chintagumpala, M.; Ashley, D.; Kellie, S.; Gururangan, S.; Hassall, T.; Gronewold, L.; Stewart, C.F.; Wallace, D.; Broniscer, A.; et al. Amifostine protects against cisplatin-induced ototoxicity in children with average-risk medulloblastoma. J. Clin. Oncol. 2008, 26, 3749–3755. [Google Scholar] [CrossRef] [Green Version]
- Katzenstein, H.M.; Chang, K.W.; Krailo, M.; Chen, Z.; Finegold, M.J.; Rowland, J.; Reynolds, M.; Pappo, A.; London, W.B.; Malogolowkin, M.; et al. Children’s Oncology Group. Amifostine does not prevent platinum induced hearing loss associated with the treatment of children with hepatoblastoma: A report of the Intergroup Hepatoblastoma Study P9645 as a part of the Children’s Oncology Group. Cancer 2009, 115, 5828–5835. [Google Scholar] [CrossRef] [Green Version]
- Neuwelt, E.A.; Gilmer-Knight, K.; Lacy, C.; Nicholson, H.S.; Kraemer, D.F.; Doolittle, N.D.; Hornig, G.W.; Muldoon, L.L. Toxicity profile of delayed high dose sodium thiosulfate in children treated with carboplatin in conjunction with blood–brain barrier disruption. Pediatr. Blood Cancer 2006, 47, 174–182. [Google Scholar] [CrossRef]
- Duval, M.; Daniel, S. Meta-analysis of the efficacy of amifostine in the prevention of cisplatin ototoxicity. J. Otolaryngol. Head Neck Surg. 2012, 41, 309–315. [Google Scholar] [PubMed]
- Doolittle, N.D.; Muldoon, L.L.; Brummett, R.E.; Tyson, R.M.; Lacy, C.; Bubalo, J.S.; Kraemer, D.F.; Heinrich, M.C.; Henry, J.A.; Neuwelt, E.A.; et al. Delayed sodium thiosulfate as an otoprotectant against carboplatin-induced hearing loss in patients with malignant brain tumors. Clin. Cancer Res. 2001, 7, 493–500. [Google Scholar] [PubMed]
- Freyer, D.R.; Chen, L.; Krailo, M.D.; Knight, K.; Villaluna, D.; Bliss, B.; Pollock, B.H.; Ramdas, J.; Lange, B.; Van Hoff, D.; et al. Effects of sodium thiosulfate versus observation on development of cisplatin-induced hearing loss in children with cancer (ACCL0431): A multicentre, randomised, controlled, open-label, phase 3 trial. Lancet Oncol. 2017, 18, 63–74. [Google Scholar] [CrossRef] [Green Version]
- Brock, P.R.; Maibach, R.; Childs, M.; Rajput, K.; Roebuck, D.; Sullivan, M.J.; Laithier, V.; Ronghe, M.; Dall’Igna, P.; Hiyama, E.; et al. Sodium thiosulfate for protection from cisplatin-induced hearing loss. N. Engl. J. Med. 2018, 378, 2376–2385. [Google Scholar] [CrossRef] [Green Version]
- Campbell, K.C.; Meech, R.P.; Klemens, J.J.; Gerberi, M.T.; Dyrstad, S.S.; Larsen, D.L.; Mitchell, D.L.; El-Azizi, M.; Verhulst, S.J.; Hughes, L.F.; et al. Prevention of noise- and drug-induced hearing loss with D-methionine. Hear. Res. 2007, 226, 92–103. [Google Scholar] [CrossRef]
- Riga, M.G.; Chelis, L.; Kakolyris, S.; Papadopoulos, S.; Stathakidou, S.; Chamalidou, E.; Xenidis, N.; Amarantidis, K.; Dimopoulos, P.; Danielides, V.; et al. Transtympanic injections of N-acetylcysteine for the prevention of cisplatin-induced ototoxicity: A feasible method with promising efficacy. Am. J. Clin. Oncol. 2018, 36, 1–6. [Google Scholar] [CrossRef]
- Crabb, S.J.; Martin, K.; Abab, J.; Ratcliffe, I.; Thornton, R.; Lineton, B.; Ellis, M.; Moody, R.; Stanton, L.; Galanopoulou, A.; et al. COAST (Cisplatin ototoxicity attenuated by aspirin trial): A phase II double-blind, randomised controlled trial to establish if aspirin reduces cisplatin induced hearing-loss. Eur. J. Cancer 2017, 87, 75–83. [Google Scholar] [CrossRef] [Green Version]
- Freyer, D.R.; Brock, P.; Knight, K.; Reaman, G.; Cabral, S.; Robinson, P.D.; Sung, L. Interventions for cisplatin-induced hearing loss in children and adolescents with cancer. Lancet Child. Adolesc. Health 2019, 3, 578–584. [Google Scholar] [CrossRef]


{kind=link}
| Age | Tests |
|---|---|
| Children younger 7–8 months and not cooperative patients | OAEs measurement |
| ABR | |
| Children between ages of 7–8 months and 24–30 months | Visual reinforcement audiometry |
| Children aged 24 months to 5 or 6 years old | Conditioned play audiometry |
| Children over 7–8 years old | Pure tone audiometry |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Romano, A.; Capozza, M.A.; Mastrangelo, S.; Maurizi, P.; Triarico, S.; Rolesi, R.; Attinà, G.; Fetoni, A.R.; Ruggiero, A. Assessment and Management of Platinum-Related Ototoxicity in Children Treated for Cancer. Cancers 2020, 12, 1266. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers12051266
Romano A, Capozza MA, Mastrangelo S, Maurizi P, Triarico S, Rolesi R, Attinà G, Fetoni AR, Ruggiero A. Assessment and Management of Platinum-Related Ototoxicity in Children Treated for Cancer. Cancers. 2020; 12(5):1266. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers12051266
Chicago/Turabian StyleRomano, Alberto, Michele Antonio Capozza, Stefano Mastrangelo, Palma Maurizi, Silvia Triarico, Rolando Rolesi, Giorgio Attinà, Anna Rita Fetoni, and Antonio Ruggiero. 2020. "Assessment and Management of Platinum-Related Ototoxicity in Children Treated for Cancer" Cancers 12, no. 5: 1266. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers12051266