Male Sexual Function after Allogeneic Hematopoietic Stem Cell Transplantation in Childhood: A Multicenter Study

 , , and
, , and
Abstract
:1. Introduction
2. Results
2.1. Clinical Data and Sex Hormones
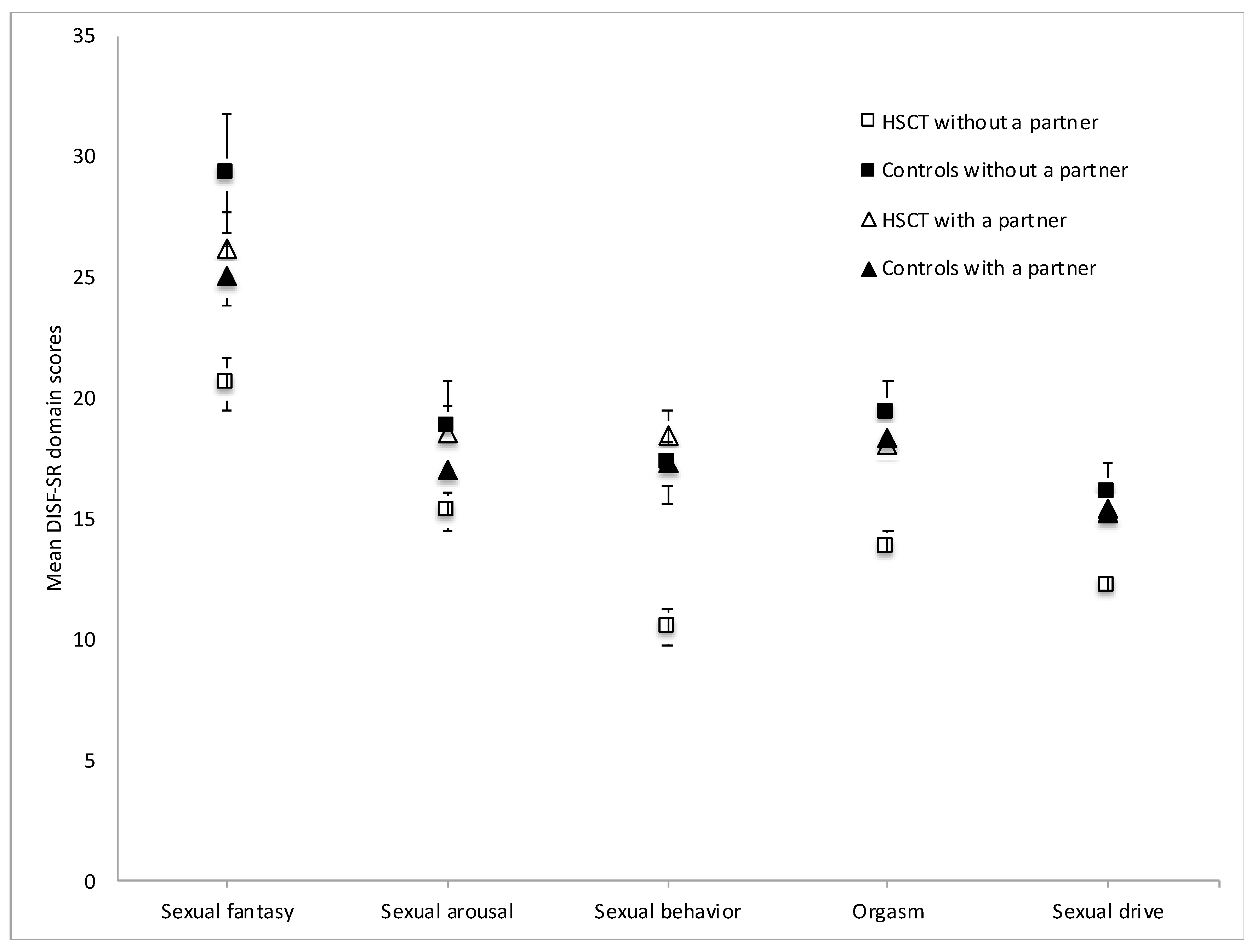
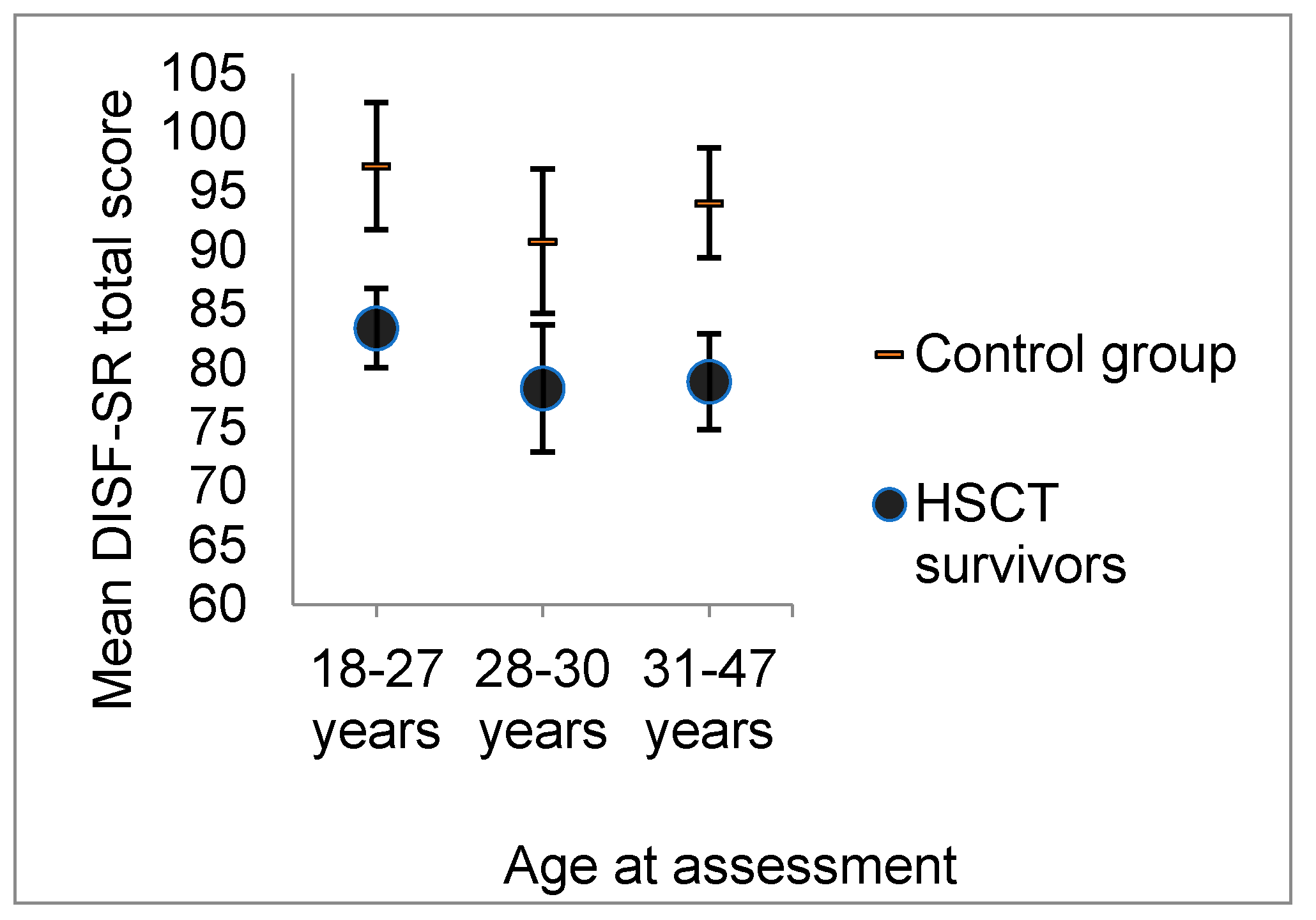
2.2. Sexual Functioning
2.3. Risk Factors for Reduced Sexual Functions within the HSCT Group
3. Discussion
4. Materials and Methods
4.1. Self-Report Measure of Sexual Functioning
4.2. Risk Factors
4.3. Statistical Analyses
4.4. Ethics
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Armenian, S.H.; Sun, C.; Kawashima, T.; Arora, M.; Leisenring, W.; Sklar, C.A.; Baker, K.S.; Francisco, L.; Teh, J.B.; Mills, G.; et al. Long-Term Health-Related Outcomes in Survivors of Childhood Cancer Treated with HSCT Versus Conventional Therapy: A Report from the Bone Marrow Transplant Survivor Study (BMTSS) and Childhood Cancer Survivor Study (CCSS). Blood 2011, 118, 1413–1420. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bhatia, S.; Davies, S.M.; Baker, K.S.; Pulsipher, M.A.; Hansen, J.A. NCI, NHLBI First International Consensus Conference on Late Effects After Pediatric Hematopoietic Cell Transplantation: Etiology and Pathogenesis of Late Effects After HCT Performed in Childhood—Methodological Challenges. Biol. Blood Marrow Transplant. 2011, 17, 1428–1435. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sundberg, K.K.; Wettergren, L.; Frisk, P.; Arvidson, J. Self-Reported Quality of Life in Long-Term Survivors of Childhood Lymphoblastic Malignancy Treated with Hematopoietic Stem Cell Transplantation Versus Conventional Therapy. Pediatr. Blood Cancer 2013, 60, 1382–1387. [Google Scholar] [CrossRef]
- Sanders, J.E.; Hoffmeister, P.A.; Storer, B.E.; Applebaum, F.R.; Storb, R.F.; Syrjala, K.L. The Quality of Life of Adult Survivors of Childhood Hematopoietic Cell Transplant. Bone Marrow Transplant. 2010, 45, 746–754. [Google Scholar] [CrossRef] [Green Version]
- Löf, C.M.; Winiarski, J.; Giesecke, A.; Ljungman, P.; Forinder, U. Health-Related Quality of Life in Adult Survivors After Paediatric Allo-SCT. Bone Marrow Transplant. 2009, 43, 461–468. [Google Scholar] [CrossRef]
- Syrjala, K.L.; Kurland, B.F.; Abrams, J.R.; Sanders, J.E.; Heiman, J.R. Sexual Function Changes during the 5 Years After High-Dose Treatment and Hematopoietic Cell Transplantation for Malignancy, with Case-Matched Controls at 5 Years. Blood 2008, 111, 989–996. [Google Scholar] [CrossRef] [Green Version]
- Claessens, J.J.M.; Beerendonk, C.C.M.; Schattenberg, A.V.M.B. Quality of Life, Reproduction and Sexuality After Stem Cell Transplantation with Partially T-Cell-Depleted Grafts and After Conditioning with a Regimen Including Total Body Irradiation. Bone Marrow Transplant. 2006, 37, 831–836. [Google Scholar] [CrossRef] [Green Version]
- Noerskov, K.H.; Schjødt, I.; Syrjala, K.L.; Jarden, M. Sexual Function 1-Year After Allogeneic Hematopoietic Stem Cell Transplantation. Bone Marrow Transplant. 2016, 51, 833–840. [Google Scholar] [CrossRef] [Green Version]
- Bober, S.L.; Zhou, E.S.; Chen, B.; Manley, P.E.; Kenney, L.B.; Recklitis, C.J. Sexual Function in Childhood Cancer Survivors: A Report from Project REACH. J. Sex. Med. 2013, 10, 2084–2093. [Google Scholar] [CrossRef]
- Thygesen, K.H.; Schjødt, I.; Jarden, M. The Impact of Hematopoietic Stem Cell Transplantation on Sexuality: A Systematic Review of the Literature. Bone Marrow Transplant. 2012, 47, 716–724. [Google Scholar] [CrossRef] [Green Version]
- Haavisto, A.; Henriksson, M.; Heikkinen, R.; Puukko-Viertomies, L.-R.; Jahnukainen, K. Sexual Function in Male Long-term Survivors of Childhood Acute Lymphoblastic Leukemia. Cancer 2016, 122, 2268–2276. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gurney, J.G.; Krull, K.R.; Kadan-Lottick, N.; Nicholson, H.S.; Nathan, P.C.; Zebeck, B.; Tersak, J.M.; Ness, K.K. Social Outcomes in the Childhood Cancer Survivor Study Cohort. J. Clin. Oncol. 2009, 27, 2390–2395. [Google Scholar] [CrossRef] [PubMed]
- Schover, L.R.; Fouladi, R.T.; Warneke, C.L.; Neese, L.; Klein, E.A.; Zippe, C.; Kupelian, P.A. Defining sexual outcomes after treatment for localized prostate carcinoma. Cancer 2002, 95, 1773–1785. [Google Scholar] [CrossRef] [PubMed]
- Janson, C.; Leisenring, W.; Cox, C.; Termuhlen, A.M.; Mertens, A.C.; Whitton, J.A.; Goodman, P.; Zeltzer, L.; Robison, L.L.; Krull, K.R.; et al. Predictors of marriage and divorce in adult survivors of childhood cancers: A report from the childhood cancer survivor study. Cancer Epidemiol. Biomark. Prev. 2009, 18, 2626–2635. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Skinner, R.; Mulder, R.L.; Kremer, L.C.; Hudson, M.M.; Constine, L.S.; Bardi, E.; Boekhout, A.; Borgmann-Staudt, A.; Brown, M.C.; Cohn, R.; et al. Recommendations for gonadotoxicity surveillance in male childhood, adolescent, and young adult cancer survivors: A report from the international late effects of childhood cancer guideline harmonization group in collaboration with the PanCareSurFup consortium. Lancet Oncol. 2017, 18, e75–e90. [Google Scholar] [PubMed] [Green Version]
- Lotti, F.; Corona, G.; Castellini, G.; Maseroli, E.; Fino, M.G.; Cozzolino, M.; Maggi, M. Semen quality impairment is associated with sexual dysfunction according to its severity. Hum. Reprod. 2016, 31, 2668–2680. [Google Scholar] [CrossRef]
- Pastuszak, A.W.; Badhiwala, N.; Lipshultz, L.I.; Khera, M. Depression is correlated with the psychological and physical aspects of sexual dysfunction in men. Int. J. Impot. Res. 2013, 25, 194–199. [Google Scholar] [CrossRef]
- Heinonen, H.; Volin, L.; Uutela, A.; Zevon, M.; Barrick, C.; Ruutu, T. Gender-associated differences in the quality of life after allogeneic BMT. Bone Marrow Transplant. 2001, 28, 503–509. [Google Scholar] [CrossRef] [Green Version]
- Watson, M.; Wheatley, K.; Harrison, G.A.; Zittoun, R.; Gray, R.G.; Goldstone, A.H.; Burnett, A.K. Severe adverse impact on sexual functioning and fertility of bone marrow transplantation, either allogeneic or autologous, compared with consolidation chemotherapy alone: Analysis of the MRC AML 10 trial. Cancer 1999, 86, 1231–1239. [Google Scholar] [CrossRef]
- Mueller, S.M.; Haeusermann, P.; Rovó, A.; Halter, J.P.; Passweg, J.; Itin, P.; Tichelli, A. Genital chronic GVHD in men after hematopoietic stem cell transplantation: A single-center cross-sectional analysis of 155 patients. Biol. Blood Marrow Transplant. 2013, 19, 1574–1580. [Google Scholar] [CrossRef] [Green Version]
- Humphreys, C.T.; Tallman, B.; Altmaier, E.M.; Barnette, V. Sexual functioning in patients undergoing bone marrow transplantation: A longitudinal study. Bone Marrow Transplant. 2007, 39, 491–496. [Google Scholar] [CrossRef]
- Helder, D.I.; Bakker, B.; De Heer, P.; Van der Veen, F.; Vossen, J.M.; Wit, J.M.; Kaptein, A.A. Quality of life in adults following bone marrow transplantation during childhood. Bone Marrow Transplant. 2004, 33, 329–336. [Google Scholar] [CrossRef] [PubMed]
- Mathiesen, S.; Sørensen, K.; Mejdahl Nielsen, M.; Suominen, A.; Ifversen, M.; Grell, K.; Lähteenmäki, P.; Frederiksen, H.; Juul, A.; Müller, K.; et al. Male gonadal function after allogeneic hematopoietic stem cell transplantation in childhood: A cross-sectional, population-based study. Biol. Blood Marrow Transplant. 2020, in press. [Google Scholar]
- Derogatis, L.R. The Derogatis Interview for Sexual Functioning (DISF/DISF-SR): An Introductory Report. J. Sex Marital Ther. 1997, 23, 291–304. [Google Scholar] [CrossRef] [PubMed]
- Beck, A.T.; Steer, R.A.; Garbin, M.G. Psychometric Properties of the Beck Depression Inventory. Twenty-Five Years of Evaluation. Clin. Psychol. Rev. 1988, 8, 77–100. [Google Scholar] [CrossRef]
- Bohannon, R.W.; Wang, Y.; Gershon, R.C. Two-Minute Walk Test Performance by Adults 18 to 85 Years: Normative Values, Reliability, and Responsiveness. Arch. Phys. Med. Rehabil. 2015, 96, 472–477. [Google Scholar] [CrossRef] [PubMed]
- Green, D.M.; Nolan, V.G.; Goodman, P.J.; Whitton, J.A.; Srivastava, D.; Leisenring, W.M.; Neglia, J.P.; Sklar, C.A.; Kaste, S.C.; Hudson, M.M.; et al. The cyclophosphamide equivalent dose as an approach for quantifying alkylating agent exposure: A report from the childhood cancer survivor study. Pediatr. Blood Cancer 2014, 61, 53–67. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vermeulen, A.; Verdonck, L.; Kaufman, J.M. A Critical Evaluation of Simple Methods for the Estimation of Free Testosterone in Serum. J. Clin. Endocrinol. Metab. 1999, 84, 3666–3672. [Google Scholar] [CrossRef]
- Jagasia, M.H.; Greinix, H.T.; Arora, M.; Williams, K.M.; Wolff, D.; Cowen, E.W.; Palmer, J.; Weisdorf, D.; Treister, N.S.; Cheng, G.S.; et al. National institutes of health consensus development project on criteria for clinical trials in chronic graft-versus-host disease: I. the 2014 diagnosis and staging working group report. Biol. Blood Marrow Transplant. 2015, 21, 389–401. [Google Scholar]



{kind=link}
{kind=link}
| Characteristic | HSCT (n = 97) | Range | Controls (n = 56) | Range | p-Value |
|---|---|---|---|---|---|
| Background variables | Mean (SD) | Mean (SD) | |||
| Age at assessment | 28.8 (7.3) | 18.5–47.0 | 29.6 (3.2) | 24.0–36.0 | 0.334 |
| Age at diagnosis | 8.7 (4.4) | 0.2–16.4 | |||
| Age at HSCT | 9.8 (4.2) | 0.4–16.9 | |||
| Follow-up time since HSCT | 19.0 (7.0) | 7.7–34.6 | |||
| Diagnostic groups | n (%) | ||||
| ALL | 45 (46%) | ||||
| NHL | 5 (5%) | ||||
| AML | 9 (9%) | ||||
| SAA | 14 (14%) | ||||
| Other | 24 (25%) | ||||
| Social and demographic variables | n (%) | n (%) | |||
| Married or cohabitating | 34 (35%) | 45 (80%) | <0.001 | ||
| Biological children | 6 (6%) | 24 (43%) | <0.001 | ||
| Highest education | <0.001 | ||||
| Comprehensive school (9 years) | 20 (21%) | 3 (5%) | |||
| Matriculation examination or vocational school (12 years) | 50 (52%) | 20 (36%) | |||
| Lower tertiary education (15 years) | 13 (13%) | 23 (41%) | |||
| Higher tertiary education (min. 17 years) | 14 (14%) | 10 (18%) | |||
| Employment | 0.009 | ||||
| Employed/student (full or part time) | 85 (88%) | 56 (100%) | |||
| Treatment regimens | n (%) | ||||
| Cancer treatment prior to HSCT | 65 (67%) | ||||
| Total body irradiation | 71 (73%) | ||||
| Median | |||||
| Cumulative gonadal irradiation dose (cGy) | 1000 | 0–4130 | |||
| Cumulative CNS irradiation dose (cGy) | 1000 | 0–3600 | |||
| Cumulative cyclophosphamide equivalent doses (mg/m2) 1 | 5113 | 0–28,743 | |||
| Laboratory variables | Median | Median | |||
| Inhibin B (ng/L) 3 | 21.0 | 1.0–247.0 | 157.0 | 74.0–307.0 | <0.001 |
| FSH (IU/L) | 9.8 | 0.01–64.4 | 3.2 | 0.9–11.4 | <0.001 |
| LH (IU/L) | 5.0 | 0.01–31.0 | |||
| SHBG (nmol/L) 1 | 26.4 | 4.8–68.8 | 32.5 | 13.0–70.0 | 0.004 |
| Prolactin (mU/L) | 209 | 44–888 | 216 | 101–634 | 0.350 |
| TSH (mU/L) | 2.5 | 0.03–9.8 | |||
| Total testosterone (nmol/L) | 15.4 | 1.7–53.8 | 18.4 | 7.1–32.6 | 0.010 |
| Free testosterone (pmol/L) 1 | 350 | 38–1470 | 296.5 | 151–406 | 0.002 |
| Mean testicular volume (mL) 2 | 13.5 | 2.0–27.0 | 33.9 | 22.2–63.9 | <0.001 |
| Total sperm count, millions 4 | 0.00 | 0.00–524.8 | 135.5 | 17.0–562.0 | <0.001 |
| Treatment-related variables | n (%) | ||||
| Azoospermia, n (%) 5 | 61 (67%) | 0 | <0.001 | ||
| Ongoing testosterone substitution | 24 (25%) | 0 | <0.001 | ||
| Ongoing thyroxin substitution | 25 (26%) | ||||
| Chronic GvHD at the time of assessment | 27 (28%) | ||||
| Grade 1 | 13 (13%) | ||||
| Grade 2 | 11 (11%) | ||||
| Grade 3 | 3 (3%) |
| Domain Item | HSCT (n = 97) | Controls (n = 56) | p-Value |
|---|---|---|---|
| Sexual fantasy (about) | 22.6 (9.2) | 25.8 (6.6) | 0.023 |
| Attractive person | 5.1 (2.0) | 5.8 (1.6) | 0.074 |
| Erotic parts of a woman | 5.0 (2.0) | 5.5 (2.1) | 0.675 |
| Erotic situation | 4.4 (2.0) | 5.0 (1.6) | 0.204 |
| Foreplay | 4.0 (2.2) | 4.8 (1.8) | 0.029 |
| Intercourse | 4.1 (2.3) | 4.8 (1.6) | 0.074 |
| Sexual arousal (Full erection) | 16.5 (6.5) | 17.3 (5.9) | 0.423 |
| When waking up | 3.2 (1.8) | 3.4 (1.9) | 1.00 |
| During a fantasy | 3.4 (2.0) | 3.6 (2.1) | 1.00 |
| During a visual cue | 3.8 (1.8) | 3.4 (1.7) | 0.651 |
| During masturbation | 3.8 (1.6) | 3.5 (1.6) | 0.342 |
| During intercourse | 2.3 (2.0) | 3.2 (1.7) | 0.002 |
| Sexual behavior | 13.3 (7.0) | 17.3 (4.7) | 0.016 |
| Erotic books | 2.6 (2.0) | 2.0 (1.9) | 0.310 |
| Masturbation | 3.7 (1.5) | 3.2 (1.6) | 0.216 |
| Kissing and petting | 3.0 (2.7) | 5.4 (2.0) | <0.001 |
| Foreplay | 2.1 (2.0) | 3.4 (1.8) | <0.001 |
| Intercourse | 2.0 (2.0) | 3.3 (1.7) | <0.001 |
| Orgasm | 15.3 (5.6) | 18.6 (3.8) | 0.002 |
| Ability | 2.8 (1.1) | 3.4 (0.9) | 0.006 |
| Intensity | 2.7 (1.0) | 3.2 (0.7) | 0.002 |
| Duration | 2.5 (1.1) | 3.0 (0.9) | 0.006 |
| Amount of seminal fluid | 2.2 (1.2) | 3.0 (0.9) | <0.001 |
| Sense of control | 2.3 (1.1) | 2.7 (0.8) | 0.078 |
| Feeling of relaxation afterward | 2.8 (1.0) | 3.3 (0.9) | 0.006 |
| Sexual drive | 13.4 (4.4) | 15.3 (3.4) | 0.022 |
| Ideal frequency of intercourse | 4.6 (1.7) | 4.5 (0.8) | 1.00 |
| Interest in sex | 2.4 (0.9) | 2.8 (0.7) | 0.075 |
| Satisfaction with personal relationship | 1.8 (1.5) | 2.6 (1.1) | <0.001 |
| Quality of current sexual functioning | 4.5 (2.2) | 5.5 (1.8) | 0.012 |
| Domain | Risk Factors | Standardized β | Adjusted R2 |
|---|---|---|---|
| Sexual cognition/fantasy | BDI-21 | −0.234 * | 0.094 |
| Testosterone group | 0.214 * | ||
| Sexual arousal a | 0.146 | ||
| BDI-21 | −0.289 ** | ||
| CNS irradiation exposure | −0.215 * | ||
| Sexual behavior/experience b | 0.043 | ||
| CNS irradiation exposure | −0.231 * | ||
| Orgasm c | 0.368 | ||
| BDI-21 | −0.431 *** | ||
| CNS irradiation exposure | −0.240 ** | ||
| Age | −0.206 * | ||
| Sexual drive/relationship | 0.196 | ||
| BDI-21 | −0.453 *** |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Haavisto, A.; Mathiesen, S.; Suominen, A.; Lähteenmäki, P.; Sørensen, K.; Ifversen, M.; Juul, A.; Mejdahl Nielsen, M.; Müller, K.; Jahnukainen, K. Male Sexual Function after Allogeneic Hematopoietic Stem Cell Transplantation in Childhood: A Multicenter Study. Cancers 2020, 12, 1786. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers12071786
Haavisto A, Mathiesen S, Suominen A, Lähteenmäki P, Sørensen K, Ifversen M, Juul A, Mejdahl Nielsen M, Müller K, Jahnukainen K. Male Sexual Function after Allogeneic Hematopoietic Stem Cell Transplantation in Childhood: A Multicenter Study. Cancers. 2020; 12(7):1786. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers12071786
Chicago/Turabian StyleHaavisto, Anu, Sidsel Mathiesen, Anu Suominen, Päivi Lähteenmäki, Kaspar Sørensen, Marianne Ifversen, Anders Juul, Malene Mejdahl Nielsen, Klaus Müller, and Kirsi Jahnukainen. 2020. "Male Sexual Function after Allogeneic Hematopoietic Stem Cell Transplantation in Childhood: A Multicenter Study" Cancers 12, no. 7: 1786. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers12071786