
Impact of Serum γ-Glutamyltransferase on Overall Survival in Men with Metastatic Castration-Resistant Prostate Cancer Treated with Docetaxel

 , , ,
, , ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Immunohistochemistry
2.3. Statistical Analyses
3. Results
3.1. Characteristics of 107 mCRPC Men Treated with Docetaxel (Full Cohort)
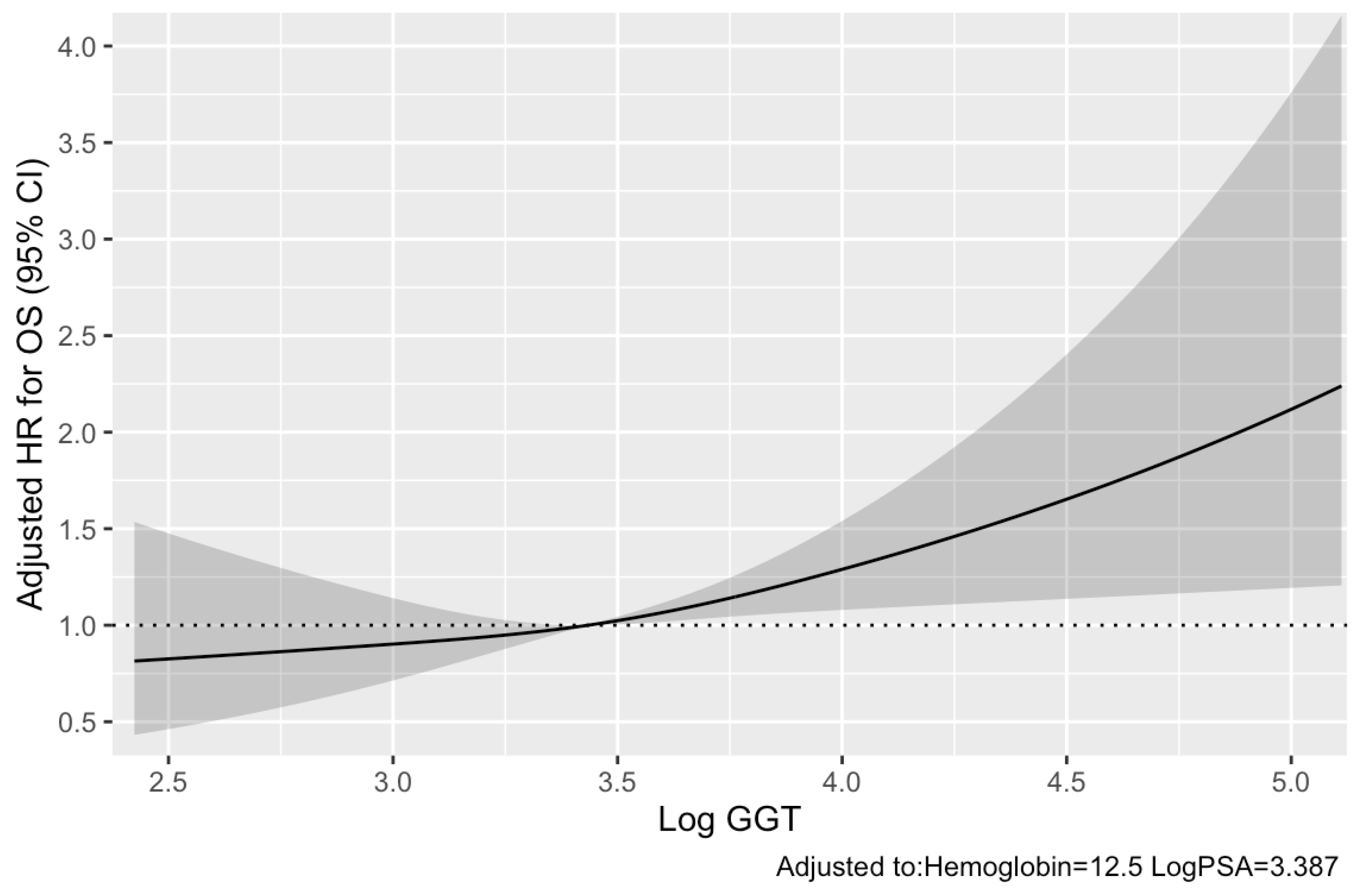
3.2. Pre-Therapeutic Serum GGT and Other Clinicopathological Parameters for Predicting OS
3.3. Pre-Therapeutic Serum GGT and Other Clinicopathological Parameters for Predicting PSA Response in 78 mCRPC Men Treated with Four or More Cycles of Docetaxel (Subcohort)
3.4. Pre-Therapeutic Serum GGT and Other Clinicopathological Parameters for Predicting PFS
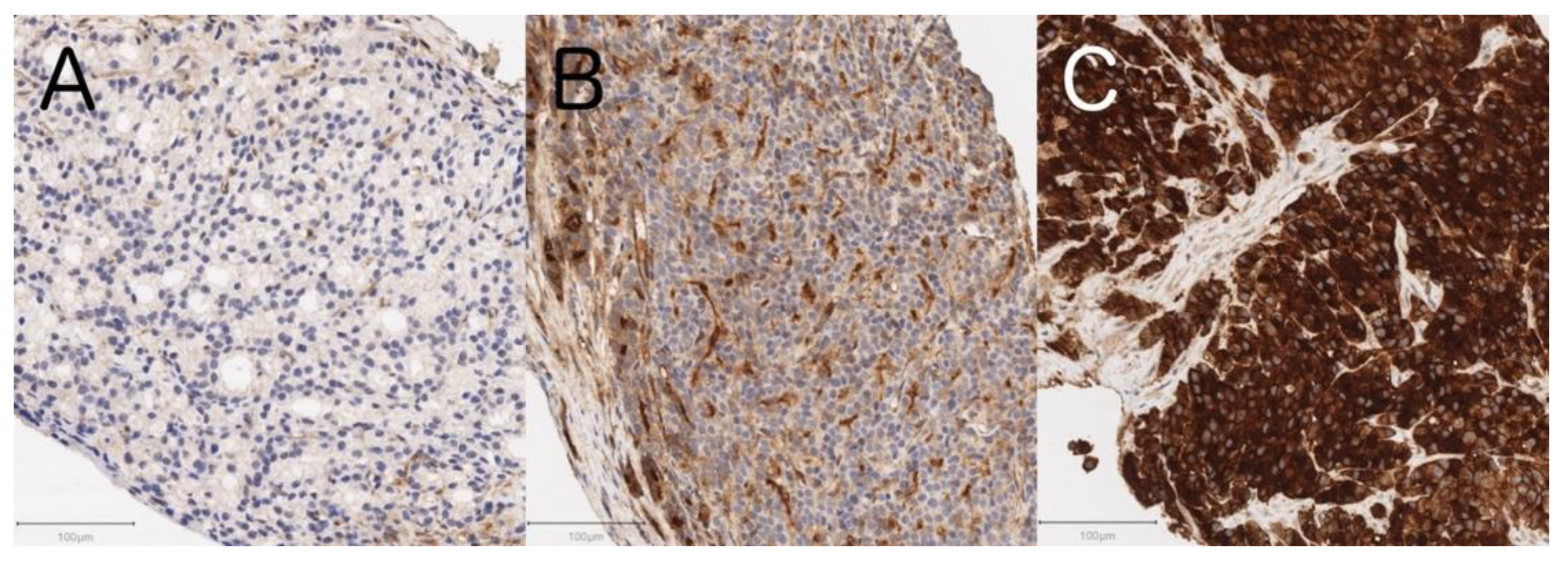
3.5. Tissue GGT Expression Status and Clinicopathological Characteristics including Serum GGT Levels in 29 De Novo mCSPC Men
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Pernar, C.H.; Ebot, E.M.; Wilson, K.M.; Mucci, L.A. The epidemiology of prostate cancer. Cold Spring Harb. Perspect. Med. 2018, 8, a030361. [Google Scholar] [CrossRef]
- James, N.D.; Pirrie, S.J.; Pope, A.M.; Barton, D.; Andronis, L.; Goranitis, I.; Collins, S.; Daunton, A.; McLaren, D.; O’Sullivan, J.; et al. Clinical outcomes and survival following treatment of metastatic castrate-refractory prostate cancer with docetaxel alone or with strontium-89, zoledronic acid, or both: The TRAPEZE randomized clinical trial. JAMA Oncol. 2016, 2, 493–499. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yuan, Y.; Kishan, A.U.; Nickols, N.G. Treatment of the primary tumor in metastatic prostate cancer. World J. Urol. 2019, 37, 2597–2606. [Google Scholar] [CrossRef] [PubMed]
- Tannock, I.F.; de Wit, R.; Berry, W.R.; Horti, J.; Pluzanska, A.; Chi, K.N.; Oudard, S.; Théodore, C.; James, N.D.; Turesson, I.; et al. Docetaxel plus prednisone or mitoxantrone plus prednisone for advanced prostate cancer. N. Engl. J. Med. 2004, 351, 1502–1512. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hussain, M.; Goldman, B.; Tangen, C.; Higano, C.S.; Petrylak, D.P.; Wilding, G.; Akdas, A.M.; Small, E.J.; Donnelly, B.J.; Sundram, S.K.; et al. Prostate-specific antigen progression predicts overall survival in patients with metastatic prostate cancer: Data from Southwest Oncology Group Trials 9346 (Intergroup Study 0162) and 9916. J. Clin. Oncol. 2009, 27, 2450–2456. [Google Scholar] [CrossRef] [PubMed]
- Ritch, C.R.; Cookson, M.S. Advances in the management of castration resistant prostate cancer. BMJ 2016, 355, i4405. [Google Scholar] [CrossRef] [Green Version]
- Halabi, S.; Small, E.J.; Kantoff, P.W.; Kattan, M.W.; Kaplan, E.B.; Dawson, N.A.; Levine, E.G.; Blumenstein, B.A.; Vogelzang, N.J. Prognostic model for predicting survival in men with hormone-refractory metastatic prostate cancer. J. Clin. Oncol. 2003, 21, 1232–1237. [Google Scholar] [CrossRef]
- Halabi, S.; Lin, C.Y.; Kelly, W.K.; Fizazi, K.S.; Moul, J.W.; Kaplan, E.B.; Morris, M.J.; Small, E.J. Updated prognostic model for predicting overall survival in first-line chemotherapy for patients with metastatic castration-resistant prostate cancer. J. Clin. Oncol. 2014, 32, 671–677. [Google Scholar] [CrossRef]
- Smaletz, O.; Scher, H.I.; Small, E.J.; Verbel, D.A.; McMillan, A.; Regan, K.; Kelly, W.K.; Kattan, M.W. Nomogram for overall survival of patients with progressive metastatic prostate cancer after castration. J. Clin. Oncol. 2002, 20, 3972–3982. [Google Scholar] [CrossRef]
- Ito, M.; Saito, K.; Yasuda, Y.; Sukegawa, G.; Kubo, Y.; Numao, N.; Kitsukawa, S.; Urakami, S.; Yuasa, T.; Yamamoto, S.; et al. Prognostic impact of C-reactive protein for determining overall survival of patients with castration-resistant prostate cancer treated with docetaxel. Urology 2011, 78, 1131–1135. [Google Scholar] [CrossRef]
- Hanigan, M.H.; Frierson, H.F. Immunohistochemical detection of gamma-glutamyl transpeptidase in normal human tissue. J. Histochem. Cytochem. 1996, 44, 1101–1108. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Meister, A.; Tate, S.S.; Griffith, O.W. Gamma-glutamyl transpeptidase. Methods Enzymol. 1981, 77, 237–253. [Google Scholar] [PubMed]
- Giommarelli, C.; Corti, A.; Supino, R.; Favini, E.; Paolicchi, A.; Pompella, A.; Zunino, F. Cellular response to oxidative stress and ascorbic acid in melanoma cells overexpressing gamma-glutamyltransferase. Eur. J. Cancer 2008, 44, 750–759. [Google Scholar] [CrossRef]
- Kunutsor, S.K.; Laukkanen, J.A. Gamma-glutamyltransferase and risk of prostate cancer: Findings from the KIHD prospective cohort study. Int. J. Cancer 2017, 140, 818–824. [Google Scholar] [CrossRef] [Green Version]
- Takemura, K. A systematic review of serum γ-glutamyltransferase as a prognostic biomarker in patients with genitourinary cancer. Antioxidants 2021, 10, 549. [Google Scholar] [CrossRef] [PubMed]
- Frierson, H.F.; Theodorescu, D.; Mills, S.E.; Hanigan, M.H. Gamma-glutamyl transpeptidase in normal and neoplastic prostate glands. Mod. Pathol 1997, 10, 1–6. [Google Scholar]
- Franzini, M.; Corti, A.; Fornaciari, I.; Balderi, M.; Torracca, F.; Lorenzini, E.; Baggiani, A.; Pompella, A.; Emdin, M.; Paolicchi, A. Cultured human cells release soluble gamma-glutamyltransferase complexes corresponding to the plasma b-GGT. Biomarkers 2009, 14, 486–492. [Google Scholar] [CrossRef] [PubMed]
- Takemura, K.; Yuasa, T.; Inamura, K.; Amori, G.; Koga, F.; Board, P.G.; Yonese, J. Impact of serum γ-glutamyltransferase on overall survival in patients with metastatic renal cell carcinoma in the era of targeted therapy. Target. Oncol. 2020, 15, 347–356. [Google Scholar] [CrossRef]
- Wang, Q.; Shu, X.; Dong, Y.; Zhou, J.; Teng, R.; Shen, J.; Chen, Y.; Dong, M.; Zhang, W.; Huang, Y.; et al. Tumor and serum gamma-glutamyl transpeptidase, new prognostic and molecular interpretation of an old biomarker in gastric cancer. Oncotarget 2017, 8, 36171–36184. [Google Scholar] [CrossRef]
- Grimm, C.; Hofstetter, G.; Aust, S.; Mutz-Dehbalaie, I.; Bruch, M.; Heinze, G.; Rahhal-Schupp, J.; Reinthaller, A.; Concin, N.; Polterauer, S. Association of gamma-glutamyltransferase with severity of disease at diagnosis and prognosis of ovarian cancer. Br. J. Cancer 2013, 109, 610–614. [Google Scholar] [CrossRef] [Green Version]
- Hanigan, M.H.; Gallagher, B.C.; Townsend, D.M.; Gabarra, V. Gamma-glutamyl transpeptidase accelerates tumor growth and increases the resistance of tumors to cisplatin in vivo. Carcinogenesis 1999, 20, 553–559. [Google Scholar] [CrossRef]
- Reuter, S.; Schnekenburger, M.; Cristofanon, S.; Buck, I.; Teiten, M.H.; Daubeuf, S.; Eifes, S.; Dicato, M.; Aggarwal, B.B.; Visvikis, A.; et al. Tumor necrosis factor alpha induces gamma-glutamyltransferase expression via nuclear factor-kappaB in cooperation with Sp1. Biochem. Pharmacol. 2009, 77, 397–411. [Google Scholar] [CrossRef]
- Khurana, N.; Sikka, S.C. Targeting crosstalk between Nrf-2, NF-κB and androgen receptor signaling inprostate cancer. Cancers 2018, 10, 352. [Google Scholar] [CrossRef] [Green Version]
- Feng, C.; Wang, H.; Lu, N.; Tu, X.M. Log transformation: Application and interpretation in biomedical research. Stat. Med. 2013, 32, 230–239. [Google Scholar] [CrossRef] [PubMed]
- Kita, Y.; Shimizu, Y.; Inoue, T.; Kamba, T.; Yoshimura, K.; Ogawa, O. Reduced-dose docetaxel for castration-resistant prostate cancer has no inferior impact on overall survival in Japanese patients. Int. J. Clin. Oncol. 2013, 18, 718–723. [Google Scholar] [CrossRef] [PubMed]
- Scher, H.I.; Morris, M.J.; Stadler, W.M.; Higano, C.; Basch, E.; Fizazi, K.; Antonarakis, E.S.; Beer, T.M.; Carducci, M.A.; Chi, K.N.; et al. Trial design and objectives for castration-resistant prostate cancer: Updated recommendations from the Prostate Cancer Clinical Trials Working Group 3. J. Clin. Oncol. 2016, 34, 1402–1418. [Google Scholar] [CrossRef] [Green Version]
- Eisenhauer, E.A.; Therasse, P.; Bogaerts, J.; Schwartz, L.H.; Sargent, D.; Ford, R.; Dancey, J.; Arbuck, S.; Gwyther, S.; Mooney, M.; et al. New response evaluation criteria in solid tumours: Revised RECIST guideline (version 1.1). Eur. J. Cancer 2009, 45, 228–247. [Google Scholar] [CrossRef]
- Harrell, F.E.; Califf, R.M.; Pryor, D.B.; Lee, K.L.; Rosati, R.A. Evaluating the yield of medical tests. JAMA 1982, 247, 2543–2546. [Google Scholar] [CrossRef] [PubMed]
- Takemura, K.; Ito, M.; Nakanishi, Y.; Kataoka, M.; Sakamoto, K.; Suzuki, H.; Tobisu, K.I.; Koga, F. Serum γ-glutamyltransferase as a prognostic biomarker in metastatic castration-resistant prostate cancer treated with enzalutamide. Anticancer Res. 2019, 39, 5773–5780. [Google Scholar] [CrossRef]
- Kobayashi, T.; Inoue, T.; Kamba, T.; Ogawa, O. Experimental evidence of persistent androgen-receptor-dependency in castration-resistant prostate cancer. Int. J. Mol. Sci. 2013, 14, 15615–15635. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martin, S.K.; Kyprianou, N. Exploitation of the androgen receptor to overcome taxane resistance in advanced prostate cancer. Adv. Cancer Res. 2015, 127, 123–158. [Google Scholar] [PubMed]
- Bryce, A.H.; Alumkal, J.J.; Armstrong, A.; Higano, C.S.; Iversen, P.; Sternberg, C.N.; Rathkopf, D.; Loriot, Y.; de Bono, J.; Tombal, B.; et al. Radiographic progression with nonrising PSA in metastatic castration-resistant prostate cancer: Post hoc analysis of PREVAIL. Prostate Cancer Prostatic Dis. 2017, 20, 221–227. [Google Scholar] [CrossRef]
- Sella, A.; Sternberg, C.N.; Skoneczna, I.; Kovel, S. Prostate-specific antigen flare phenomenon with docetaxel-based chemotherapy in patients with androgen-independent prostate cancer. BJU Int. 2008, 102, 1607–1609. [Google Scholar] [CrossRef] [PubMed]
- Scher, H.I.; Warren, M.; Heller, G. The association between measures of progression and survival in castrate-metastatic prostate cancer. Clin. Cancer Res. 2007, 13, 1488–1492. [Google Scholar] [CrossRef] [Green Version]
- Godwin, A.K.; Meister, A.; O’Dwyer, P.J.; Huang, C.S.; Hamilton, T.C.; Anderson, M.E. High resistance to cisplatin in human ovarian cancer cell lines is associated with marked increase of glutathione synthesis. Proc. Natl. Acad. Sci. USA 1992, 89, 3070–3074. [Google Scholar] [CrossRef] [Green Version]
- Mohell, N.; Alfredsson, J.; Fransson, Å.; Uustalu, M.; Byström, S.; Gullbo, J.; Hallberg, A.; Bykov, V.J.; Björklund, U.; Wiman, K.G. APR-246 overcomes resistance to cisplatin and doxorubicin in ovarian cancer cells. Cell Death Dis. 2015, 6, e1794. [Google Scholar] [CrossRef] [Green Version]
- Hanigan, M.H. Gamma-glutamyl transpeptidase: Redox regulation and drug resistance. Adv. Cancer Res. 2014, 122, 103–141. [Google Scholar]
- Emdin, M.; Pompella, A.; Paolicchi, A. Gamma-glutamyltransferase, atherosclerosis, and cardiovascular disease: Triggering oxidative stress within the plaque. Circulation 2005, 112, 2078–2080. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Terzyan, S.S.; Burgett, A.W.; Heroux, A.; Smith, C.A.; Mooers, B.H.; Hanigan, M.H. Human γ-Glutamyl transpeptidase 1: Structures of the free enzyme, inhibito-bound tetrahedral transition states, and glutamate-bound enzyme reveal novel movement within the active site during catalysis. J. Biol. Chem. 2015, 290, 17576–17586. [Google Scholar] [CrossRef] [Green Version]
- Russo, G.L.; Russo, M.; Castellano, I.; Napolitano, A.; Palumbo, A. Ovothiol isolated from sea urchin oocytes induces autophagy in the Hep-G2 cell line. Mar. Drugs 2014, 12, 4069–4085. [Google Scholar] [CrossRef] [Green Version]
- Wickham, S.; Regan, N.; West, M.B.; Thai, J.; Cook, P.F.; Terzyan, S.S.; Li, P.K.; Hanigan, M.H. Inhibition of human γ-glutamyl transpeptidase: Development of more potent, physiologically relevant, uncompetitive inhibitors. Biochem. J. 2013, 450, 547–557. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Altman, D.G.; McShane, L.M.; Sauerbrei, W.; Taube, S.E. Reporting recommendations for tumor marker prognostic studies (REMARK): Explanation and elaboration. PLoS Med. 2012, 9, e1001216. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ishiyama, Y.; Kondo, T.; Tachibana, H.; Ishihara, H.; Fukuda, H.; Yoshida, K.; Takagi, T.; Iizuka, J.; Tanabe, K. Predictive role of γ-glutamyltransferase in patients receiving nivolumab therapy for metastatic renal cell carcinoma. Int. J. Clin. Oncol. 2021, 26, 552–561. [Google Scholar] [CrossRef]
- Heisterkamp, N.; Groffen, J.; Warburton, D.; Sneddon, T.P. The human gamma-glutamyltransferase gene family. Hum. Genet. 2008, 123, 321–332. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Characteristic at Docetaxel Initiation | Full Cohort | Subcohort | ||
|---|---|---|---|---|
| (n = 107) | (n = 78) | |||
| Age [years] * | 72.6 | (68.7–76.7) | 71.2 | (68.7–75.5) |
| ECOG PS | ||||
| 0 | 84 | (79%) | 60 | (77%) |
| ≥1 | 23 | (21%) | 18 | (23%) |
| Gleason sum | ||||
| <8 | 8 | (7%) | 7 | (9%) |
| ≥8 | 89 | (83%) | 64 | (82%) |
| unknown | 10 | (9%) | 7 | (9%) |
| Metastatic sites | ||||
| Lymph node only (M1a) | 7 | (7%) | 6 | (8%) |
| Bone/bone + lymph node (M1b) | 82 | (77%) | 58 | (74%) |
| Any visceral (M1c) | 18 | (17%) | 14 | (18%) |
| Opioid use | ||||
| Yes | 19 | (18%) | 13 | (17%) |
| No | 88 | (82%) | 65 | (83%) |
| Pre-docetaxel sequential treatments | ||||
| Bicalutamide | 107 | (100%) | 78 | (100%) |
| Flutamide | 74 | (69%) | 58 | (74%) |
| Estrogen | 34 | (32%) | 24 | (31%) |
| Enzalutamide | 38 | (36%) | 21 | (27%) |
| Abiraterone acetate | 20 | (19%) | 12 | (15%) |
| Number of pre-docetaxel treatments * | 2 | (1–3) | 1 | (1–2) |
| Time from diagnosis to docetaxel [years] * | 2.5 | (1.1–4.4) | 2.4 | (1.0–4.0) |
| Laboratory parameters | ||||
| Hemoglobin [g/L] * | 125 | (113–133) | 126 | (114–133) |
| Albumin [g/L] * | 41 | (38–44) | 41 | (38–44) |
| GGT [U/L] * | 31 | (19–51) | 31 | (19–50) |
| LDH [U/L] * | 201 | (179–253) | 198 | (179–254) |
| ALP [U/L] * | 393 | (252–618) | 356 | (249–543) |
| CRP [mg/L] * | 2.7 | (1.0–7.0) | 2.6 | (1.0–7.0) |
| PSA [ng/mL] * | 29.6 | (7.3–121.2) | 19.3 | (4.6–93.5) |
| Cycles of docetaxel | ||||
| <4 | 29 | (27%) | 0 | (0%) |
| ≥4 | 78 | (73%) | 78 | (100%) |
| Post-docetaxel sequential treatments | ||||
| Flutamide | 1 | (1%) | 0 | (0%) |
| Estrogen | 34 | (32%) | 30 | (38%) |
| Enzalutamide | 38 | (36%) | 31 | (40%) |
| Abiraterone acetate | 30 | (28%) | 21 | (27%) |
| Cabazitaxel | 22 | (21%) | 16 | (21%) |
| Radium-223 | 5 | (5%) | 4 | (5%) |
| Factor | Univariable | Multivariable (Final Model) | ||||
|---|---|---|---|---|---|---|
| HR | (95% CI) | p | HR | (95% CI) | p | |
| Age | 1.01 | (0.97–1.05) | 0.566 | |||
| ECOG PS (≥1 vs. 0) | 1.62 | (0.92–2.85) | 0.092 | |||
| Gleason sum (≥8 vs. <8) | 0.98 | (0.50–1.93) | 0.957 | |||
| Visceral metastasis (Yes vs. no) | 0.87 | (0.45–1.66) | 0.664 | |||
| Opioid use (Yes vs. no) | 2.57 | (1.43–4.62) | 0.002 | |||
| Number of pre-docetaxel treatments | 1.11 | (0.85–1.44) | 0.439 | |||
| Time from diagnosis to docetaxel | 0.98 | (0.91–1.06) | 0.662 | |||
| Hemoglobin | 0.72 | (0.63–0.82) | <0.001 | 0.79 | (0.68–0.92) | 0.002 |
| Albumin | 0.30 | (0.15–0.61) | <0.001 | |||
| Log GGT | 1.37 | (1.06–1.78) | 0.017 | 1.49 | (1.12–1.98) | 0.006 |
| LDH (>ULN vs. ≤ULN) | 2.35 | (1.38–4.00) | 0.002 | |||
| Log ALP | 1.90 | (1.39–2.60) | <0.001 | |||
| CRP | 1.11 | (0.99–1.24) | 0.067 | |||
| Log PSA | 1.52 | (1.32–1.76) | <0.001 | 1.40 | (1.21–1.62) | <0.001 |
| Factor | OR | (95% CI) | p |
|---|---|---|---|
| Age | 1.01 | (0.94–1.08) | 0.767 |
| ECOG PS (≥1 vs. 0) | 1.21 | (0.41–3.57) | 0.731 |
| Gleason sum (≥8 vs. <8) | 4.94 | (0.56–43.50) | 0.150 |
| Visceral metastasis (Yes vs. no) | 0.46 | (0.13–1.61) | 0.222 |
| Opioid use (Yes vs. no) | 1.66 | (0.50–5.51) | 0.408 |
| Number of pre-docetaxel treatments | 0.64 | (0.39–1.05) | 0.075 |
| Time from diagnosis to docetaxel | 0.99 | (0.86–1.14) | 0.855 |
| Hemoglobin | 1.13 | (0.84–1.52) | 0.421 |
| Albumin | 2.69 | (0.81–8.94) | 0.105 |
| Log GGT | 1.50 | (0.82–2.74) | 0.188 |
| LDH (>UNL vs. ≤ULN) | 1.09 | (0.39–3.05) | 0.868 |
| Log ALP | 1.05 | (0.60–1.85) | 0.865 |
| CRP | 0.95 | (0.74–1.21) | 0.671 |
| Log PSA | 0.89 | (0.71–1.11) | 0.298 |
| Factor | Univariable | Multivariable | ||||
|---|---|---|---|---|---|---|
| HR | (95% CI) | p | HR | (95% CI) | p | |
| Age | 1.02 | (0.99–1.05) | 0.121 | |||
| ECOG PS (≥1 vs. 0) | 0.90 | (0.56–1.45) | 0.672 | |||
| Gleason sum (≥8 vs. <8) | 0.62 | (0.37–1.05) | 0.073 | |||
| Visceral metastasis (Yes vs. no) | 0.88 | (0.51–1.53) | 0.656 | |||
| Opioid use (Yes vs. no) | 1.38 | (0.83–2.30) | 0.210 | |||
| Number of pre-docetaxel treatments | 1.31 | (1.09–1.57) | 0.005 | |||
| Time from diagnosis to docetaxel | 1.02 | (0.97–1.08) | 0.498 | |||
| Hemoglobin | 0.83 | (0.74–0.92) | <0.001 | |||
| Albumin | 0.39 | (0.23–0.66) | <0.001 | 0.58 | (0.35–0.97) | 0.037 |
| Log GGT | 1.06 | (0.85–1.34) | 0.597 | |||
| LDH (> UNL vs. ≤ ULN) | 1.79 | (1.16–2.79) | 0.009 | |||
| Log ALP | 1.53 | (1.21–1.93) | < 0.001 | |||
| CRP | 1.11 | (1.00–1.22) | 0.045 | |||
| Log PSA | 1.30 | (1.18–1.43) | < 0.001 | 1.26 | (1.14–1.40) | < 0.001 |
| Characteristic at Diagnosis | Tissue GGT Expression Status | p | |||||
|---|---|---|---|---|---|---|---|
| Negative to Weak (n = 6) | Moderate (n = 12) | Strong (n = 11) | |||||
| Age [years], median (IQR) | 76.2 | (65.2–79.6) | 69.6 | (67.0–72.4) | 70.5 | (64.6–78.2) | 0.438 * |
| Gleason score, median (IQR) | 9 | (9–9) | 9 | (9–9) | 9 | (9–9) | 0.772 * |
| Metastatic sites | 0.492 † | ||||||
| Lymph node only (M1a) | 0 | (0%) | 0 | (0%) | 0 | (0%) | |
| Bone/bone + lymph node (M1b) | 5 | (83%) | 9 | (82%) | 10 | (100%) | |
| Any visceral (M1c) | 1 | (17%) | 2 | (18%) | 0 | (0%) | |
| Serum GGT [U/L], median (IQR) | 15 | (10.5–33.3) | 33 | (23.5–53.3) | 64 | (50–74) | 0.018 * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Une, M.; Takemura, K.; Inamura, K.; Fukushima, H.; Ito, M.; Kobayashi, S.; Yuasa, T.; Yonese, J.; Board, P.G.; Koga, F. Impact of Serum γ-Glutamyltransferase on Overall Survival in Men with Metastatic Castration-Resistant Prostate Cancer Treated with Docetaxel. Cancers 2021, 13, 5587. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers13215587
Une M, Takemura K, Inamura K, Fukushima H, Ito M, Kobayashi S, Yuasa T, Yonese J, Board PG, Koga F. Impact of Serum γ-Glutamyltransferase on Overall Survival in Men with Metastatic Castration-Resistant Prostate Cancer Treated with Docetaxel. Cancers. 2021; 13(21):5587. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers13215587
Chicago/Turabian StyleUne, Minami, Kosuke Takemura, Kentaro Inamura, Hiroshi Fukushima, Masaya Ito, Shuichiro Kobayashi, Takeshi Yuasa, Junji Yonese, Philip G. Board, and Fumitaka Koga. 2021. "Impact of Serum γ-Glutamyltransferase on Overall Survival in Men with Metastatic Castration-Resistant Prostate Cancer Treated with Docetaxel" Cancers 13, no. 21: 5587. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers13215587