
Pathological Significance of GLUT-1 Expression in Breast Cancer Cells in Diabetic and Obese Patients: The French Guiana Study

 , and
, and 
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Definition of Clinical Groups
2.2. Definition of Molecular Types of Breast Carcinoma
2.3. GLUT-1 Immunohistochemistry Technique
2.4. Evaluation of GLUT-1 IHC Labeling
2.5. Exclusion Criteria
2.6. Statistical Analysis
2.7. Ethical Statement
3. Results
3.1. General Clinical and Histological Features of Breast Cancer in French Guiana
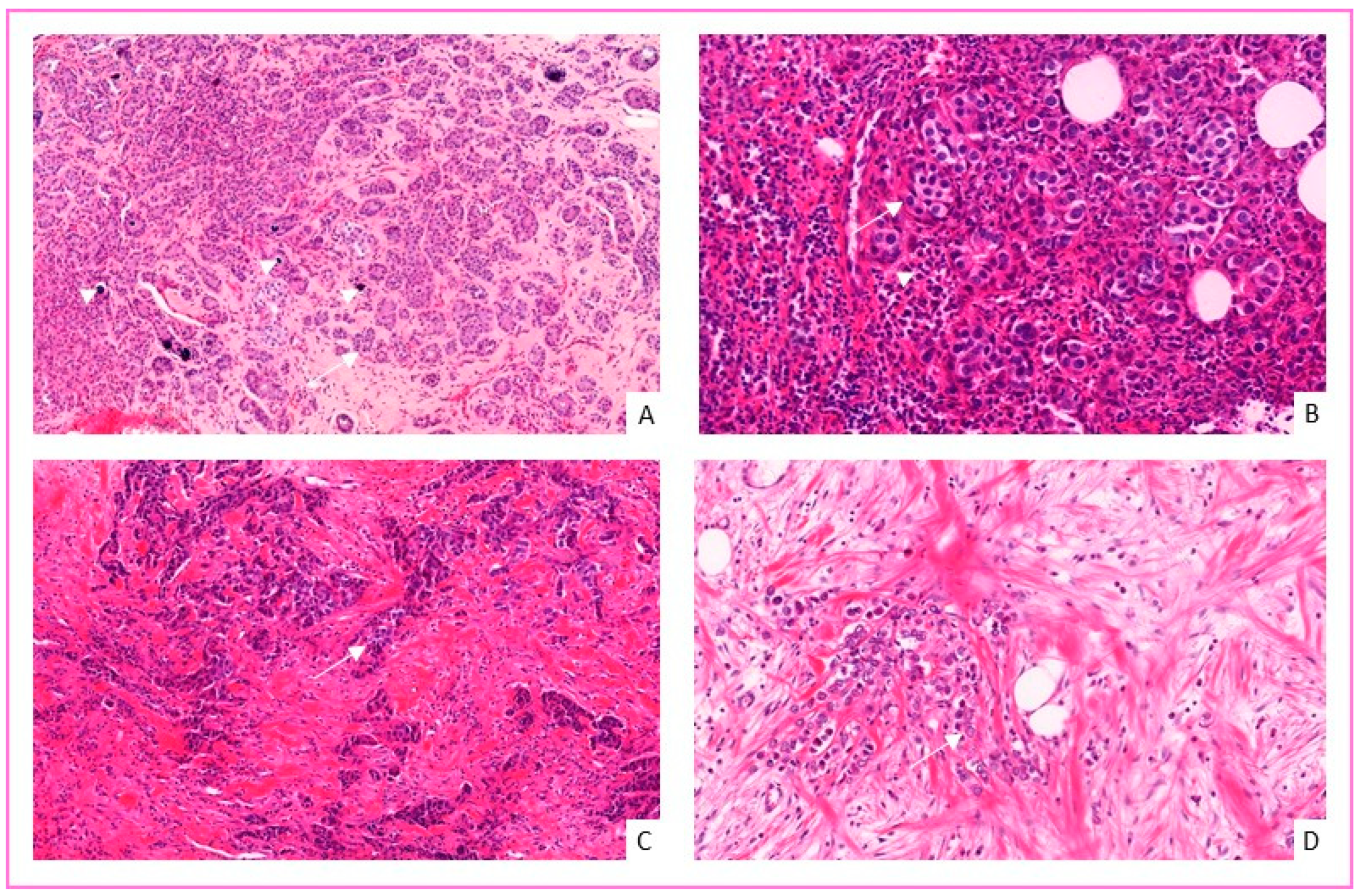
3.2. Histological and Prognostic Features of Breast Cancer in French Guiana
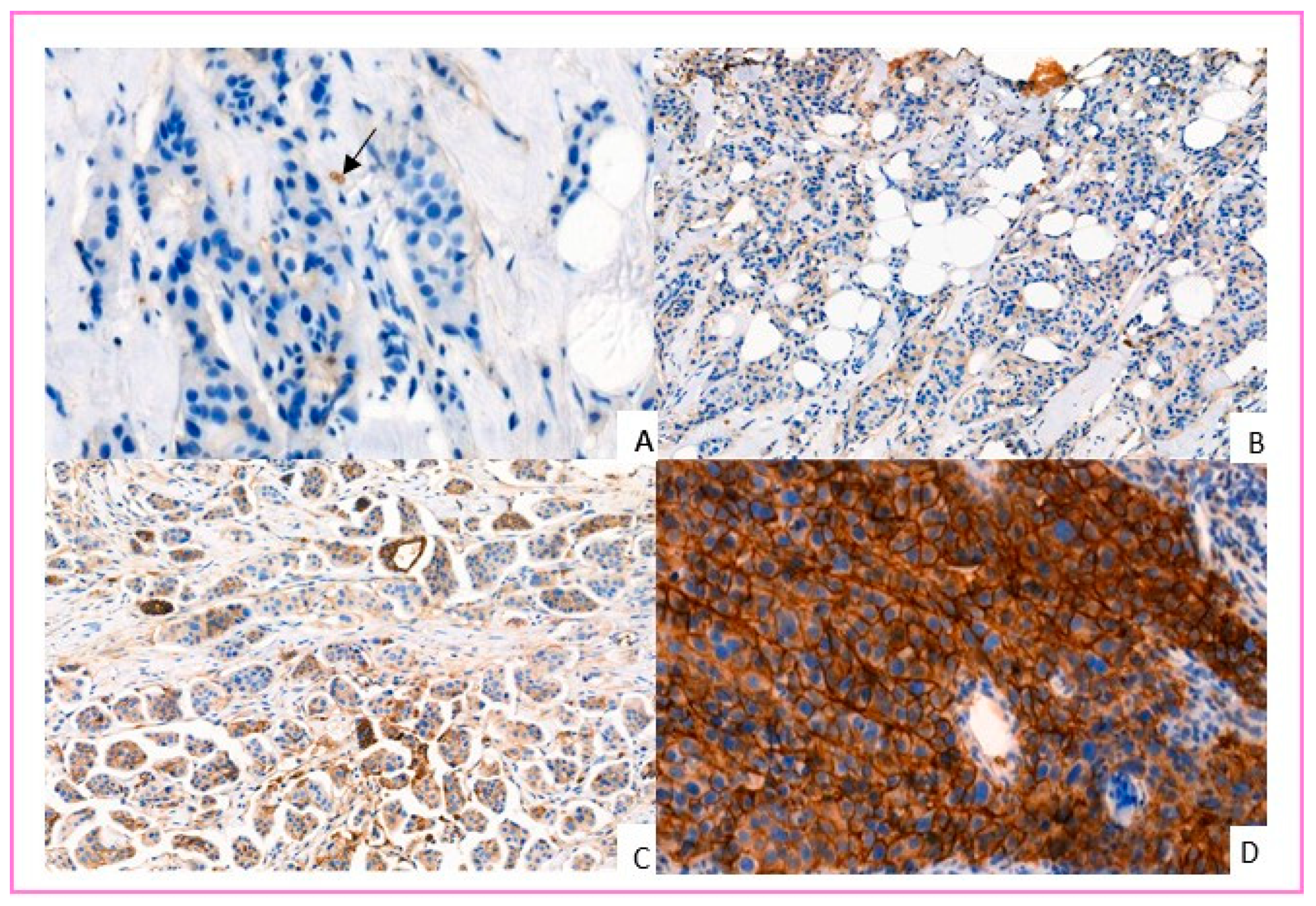
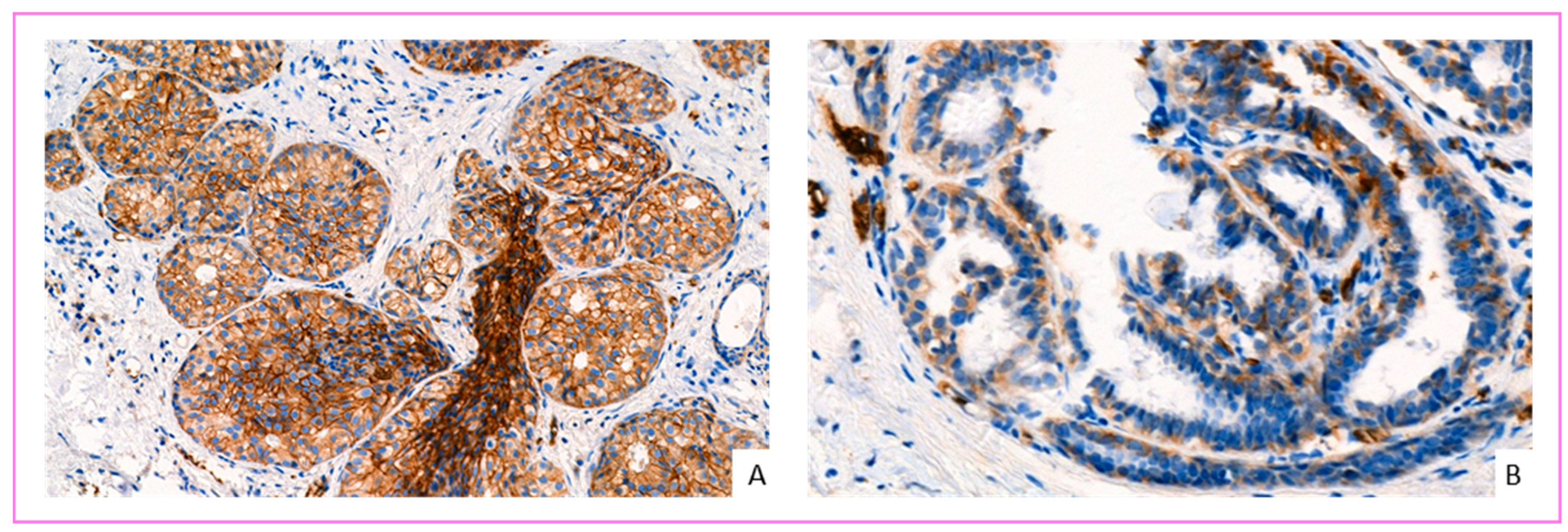
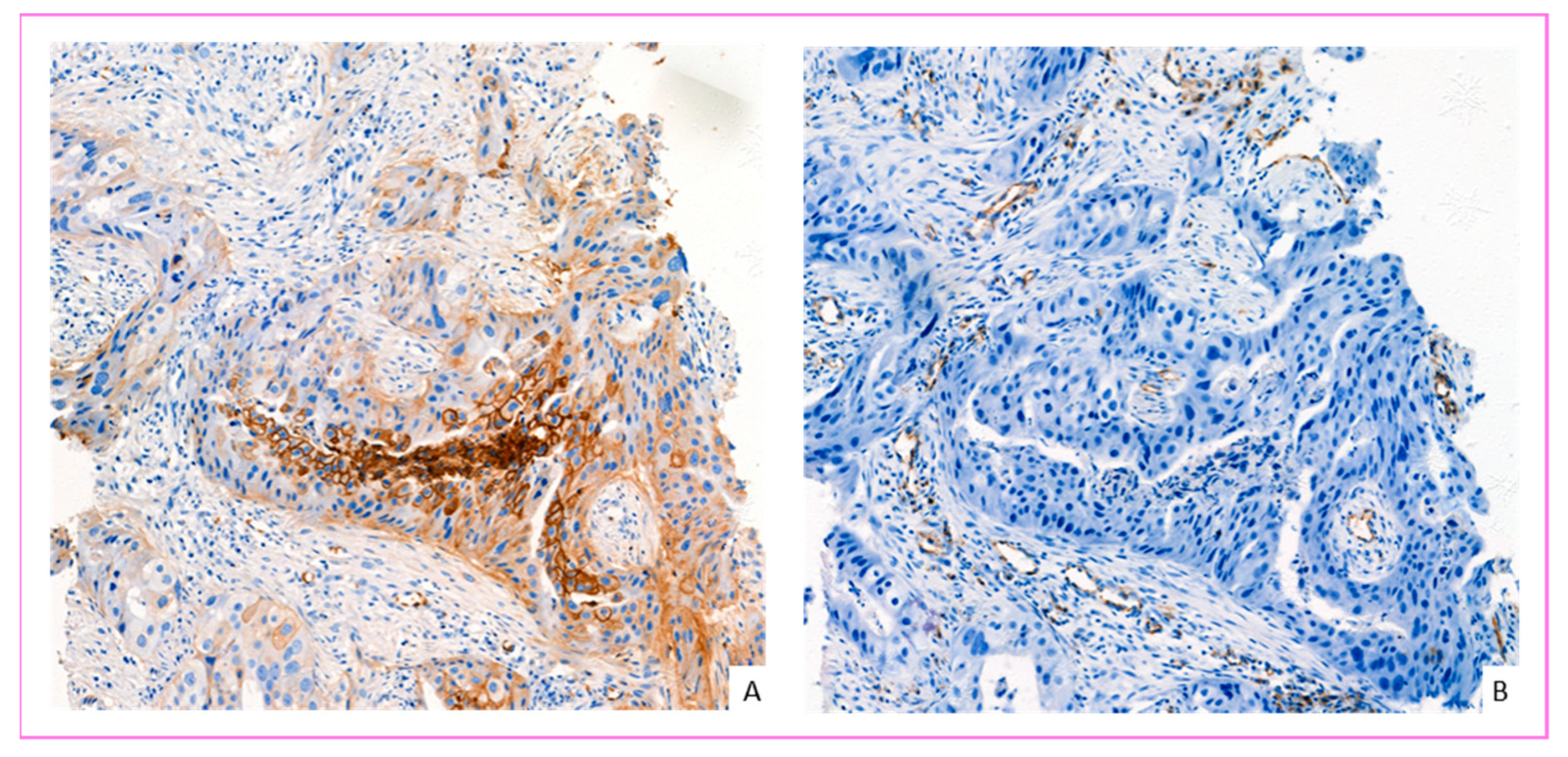
3.3. GLUT-1 Expression in Breast Cancer Cells
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- The GBD 2015 Obesity Collaborators. Health Effects of Overweight and Obesity in 195 Countries over 25 Years. N. Engl. J. Med. 2017, 377, 13–27. [Google Scholar] [CrossRef]
- Zheng, Y.; Ley, S.H.; Hu, F.B. Global aetiology and epidemiology of type 2 diabetes mellitus and its complications. Nat. Rev. Endocrinol. 2018, 14, 88–98. [Google Scholar] [CrossRef]
- Gallagher, E.J.; LeRoith, D. Hyperinsulinaemia in cancer. Nat. Cancer 2020, 20, 629–644. [Google Scholar] [CrossRef]
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–449. [Google Scholar] [CrossRef] [PubMed]
- Hanahan, D.; Weinberg, R.A. Hallmarks of Cancer: The Next Generation. Cell 2011, 144, 646–674. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Warburg, O.; Wind, F.; Negelein, E. The metabolism of tumors in the body. J. Gen. Physiol. 1927, 8, 519–530. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Warburg, O. On the Origin of Cancer Cells. Science 1956, 123, 309–314. [Google Scholar] [CrossRef]
- Kuo, M.-H.; Chang, W.-W.; Yeh, B.-W.; Chu, Y.-S.; Lee, Y.-C.; Lee, H.-T. Lee Glucose Transporter 3 Is Essential for the Survival of Breast Cancer Cells in the Brain. Cells 2019, 8, 1568. [Google Scholar] [CrossRef] [Green Version]
- Garrido, P.; Osorio, F.G.; Morán, J.; Cabello, E.; Alonso, A.; Freije, J.M.; González, C. Loss of GLUT4 Induces Metabolic Reprogramming and Impairs Viability of Breast Cancer Cells. J. Cell. Physiol. 2014, 230, 191–198. [Google Scholar] [CrossRef]
- Barbosa, A.M.; Martel, F. Targeting Glucose Transporters for Breast Cancer Therapy: The Effect of Natural and Synthetic Compounds. Cancers 2020, 12, 154. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Olson, A.L.; Pessin, J.E. Structure, function, and regulation of the mammalian facilitative glucose transporter gene family. Annu. Rev. Nutr. 1996, 16, 235–256. [Google Scholar] [CrossRef]
- Mueckler, M.; Caruso, C.; Baldwin, S.A.; Panico, M.; Blench, I.; Morris, H.R.; Allard, W.J.; Lienhard, G.E.; Lodish, H.F. Sequence and structure of a human glucose transporter. Science 1985, 229, 941–945. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Ye, C.; Chen, C.; Xiong, H.; Xie, B.; Zhou, J.; Chen, Y.; Zheng, S.; Wang, L. Glucose transporter GLUT1 expression and clinical outcome in solid tumors: A systematic review and meta-analysis. Oncotarget 2017, 8, 16875–16886. [Google Scholar] [CrossRef] [Green Version]
- Taha, C.; Liu, Z.; Jin, J.; Al-Hasani, H.; Sonenberg, N.; Klip, A. Opposite translational control of GLUT1 and GLUT4 glucose transporter mRNAs in response to insulin. Role of mammalian target of rapamycin, protein kinase b, and phosphatidylinositol 3-kinase in GLUT1 mRNA translation. J. Biol. Chem. 1999, 274, 33085–33091. [Google Scholar] [CrossRef] [Green Version]
- Cifuentes, M.; García, M.A.; Arrabal, P.M.; Martínez, F.; Yañez, M.J.; Jara, N.; Weil, B.; Domínguez, D.; Medina, R.A.; Nualart, F. Insulin regulates GLUT1-mediated glucose transport in MG-63 human osteosarcoma cells. J. Cell. Physiol. 2011, 226, 1425–1432. [Google Scholar] [CrossRef] [PubMed]
- Laybutt, D.R.; Thompson, A.L.; Cooney, G.J.; Kraegen, E.W. Selective chronic regulation of GLUT1 and GLUT4 content by insulin, glucose, and lipid in rat cardiac muscle in vivo. Am. J. Physiol. Content 1997, 273, H1309–H1316. [Google Scholar] [CrossRef] [PubMed]
- Silva, C.; Andrade, N.; Guimarães, J.T.; Patrício, E.; Martel, F. The in vitro effect of the diabetes-associated markers insulin, leptin and oxidative stress on cellular characteristics promoting breast cancer progression is GLUT1-dependent. Eur. J. Pharmacol. 2021, 898, 173980. [Google Scholar] [CrossRef] [PubMed]
- Kang, C.; LeRoith, D.; Gallagher, E.J. Diabetes, Obesity, and Breast Cancer. Endocrinology 2018, 159, 3801–3812. [Google Scholar] [CrossRef] [Green Version]
- Melstrom, L.G.; Salabat, M.R.; Ding, X.-Z.; Milam, B.M.; Strouch, M.; Pelling, J.C.; Bentrem, D.J. Apigenin Inhibits the GLUT-1 Glucose Transporter and the Phosphoinositide 3-Kinase/Akt Pathway in Human Pancreatic Cancer Cells. Pancreas 2008, 37, 426–431. [Google Scholar] [CrossRef]
- Gonnella, R.; Santarelli, R.; Farina, A.; Granato, M.; D’Orazi, G.; Faggioni, A.; Cirone, M. Kaposi sarcoma associated herpesvirus (KSHV) induces AKT hyperphosphorylation, bortezomib-resistance and GLUT-1 plasma membrane exposure in THP-1 monocytic cell line. J. Exp. Clin. Cancer Res. 2013, 32, 79. [Google Scholar] [CrossRef] [Green Version]
- Daigre, J.-L.; Atallah, A.; Boissin, J.-L.; Jean-Baptiste, G.; Kangambega, P.; Chevalier, H.; Balkau, B.; Smadja, D.; Inamo, J. The prevalence of overweight and obesity, and distribution of waist circumference, in adults and children in the French Overseas Territories: The PODIUM survey. Diabetes Metab. 2012, 38, 404–411. [Google Scholar] [CrossRef] [PubMed]
- Carvalho, L.; Belliardo, S.; Andrieu, A.; de Maria, F.; Chatignoux, É. Incidence et mortalité des cancers en Guyane, 2007–2014. Synthèse de l’état des connaissances/incidence and mortality of cancers in French Guiana, 2007–2014. Summary of the state of knowledge. Bull. Epidémiol. Hebd. 2020, 36–37, 730–736. [Google Scholar]
- Roué, T.; Fior, A.; Plenet, J.; Belliardo, S.; Nacher, M. The epidemiology of breast cancer in French Guiana 2003–2006. SpringerPlus 2013, 2, 471. [Google Scholar] [CrossRef]
- Roué, T.; Labbé, S.; Belliardo, S.; Plenet, J.; Douine, M.; Nacher, M. Predictive Factors of the Survival of Women With Invasive Breast Cancer in French Guiana: The Burden of Health Inequalities. Clin. Breast Cancer 2016, 16, e113–e118. [Google Scholar] [CrossRef]
- Elston, C.W.; Ellis, I.O. Pathological prognostic factors in breast cancer. I. The value of histological grade in breast cancer: Expe-rience from a large study with long-term follow-up. Histopathology 1991, 19, 403–410. [Google Scholar] [CrossRef]
- Available online: https://tumourclassification.iarc.who.int/welcome/ (accessed on 10 October 2021).
- Drouin, P.; Blickle, J.F.; Charbonnel, B.; Eschwege, E.; Guillausseau, P.J.; Plouin, P.F.; Daninos, J.M.; Balarac, N.; Sauvanet, J.P. Diagnostic et classification du diabete sucré les nouveaux criteres. Diabetes Metab. 1999, 25, 12. [Google Scholar]
- Cheang, M.C.; Martin, M.; Nielsen, T.O.; Prat, A.; Voduc, D.; Rodriguez-Lescure, A.; Ruiz, A.; Chia, S.; Shepherd, L.; Ruiz-Borrego, M.; et al. Defining Breast Cancer Intrinsic Subtypes by Quantitative Receptor Expression. Oncologist 2015, 20, 474–482. [Google Scholar] [CrossRef] [Green Version]
- Iwamoto, T.; Booser, D.; Valero, V.; Murray, J.L.; Koenig, K.; Esteva, F.; Ueno, N.T.; Zhang, J.; Shi, W.; Qi, Y.; et al. Estrogen Receptor (ER) mRNA and ER-Related Gene Expression in Breast Cancers That Are 1% to 10% ER-Positive by Immunohistochemistry. J. Clin. Oncol. 2012, 30, 729–734. [Google Scholar] [CrossRef]
- Wolff, A.C.; Hammond, M.E.H.; Allison, K.H.; Harvey, B.E.; Mangu, P.B.; Bartlett, J.M.S.; Bilous, M.; Ellis, L.O.; Fitzgibbons, P.; Hanna, W.; et al. Human Epidermal Growth Factor Receptor 2 Testing in Breast Cancer: American Society of Clinical Oncology/College of American Pathologists Clinical Practice Guideline Focused Update. J. Clin. Oncol. 2018, 36, 2105–2122. [Google Scholar] [CrossRef] [Green Version]
- Sakashita, M.; Aoyama, N.; Minami, R.; Maekawa, S.; Kuroda, K.; Shirasaka, D.; Ichihara, T.; Kuroda, Y.; Maeda, S.; Kasuga, M. Glut1 expression in T1 and T2 stage colorectal carcinomas: Its relationship to clinicopathological features. Eur. J. Cancer 2001, 37, 204–209. [Google Scholar] [CrossRef]
- BiostaTGV-Statistiques en Ligne. Institut Pierre Louis d’Epidémiologie, Santé Publique UMR S 1136, INSERM et Sorbonne Université (UPMC). Available online: https://biostatgv.sentiweb.fr/ (accessed on 15 October 2021).
- Joachim, C.; Véronique-Baudin, J.; Desroziers, L.; Chatignoux, É.; Belliardo, S.; Plenet, J.; Macni, J.; Ulric-Gervaise, S.; Peruvien, J.; Bhakkan-Mambir, B.; et al. Gynaecological cancer in Caribbean women: Data from the French population-based cancer registries of Martinique, Guadeloupe and French Guiana (2007–2014). BMC Cancer 2020, 20, 643. [Google Scholar] [CrossRef]
- Howlader, N.; Noone, A.; Krapcho, M.; Miller, D.; Brest, A.; Yu, M.; Ruhl, J.; Tatalovich, Z.; Mariotto, A.; Lewis, D.R.; et al. SEER Cancer Statistics Review, 1975–2016; National Cancer Institute: Bethesda, MD, USA, 2019. Available online: https://seer.cancer.gov/archive/csr/1975_2016/ (accessed on 15 October 2021).
- Al-thoubaity, F.K. Molecular classification of breast cancer: A retrospective cohort study. Ann. Med. Surg. 2020, 49, 44–48. [Google Scholar] [CrossRef] [PubMed]
- Yang, X.R.; Sherman, M.E.; Rimm, D.L.; Lissowska, J.; Brinton, L.A.; Peplonska, B.; Hewitt, S.; Anderson, W.F.; Szeszenia-Dąbrowska, N.; Bardin-Mikolajczak, A.; et al. Differences in Risk Factors for Breast Cancer Molecular Subtypes in a Population-Based Study. Cancer Epidemiol. Biomark. Prev. 2007, 16, 439–443. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Howlader, N.; Noone, A.; Krapcho, M.; Miller, D.; Bishop, K.; Altekruse, S.; Kosary, C.L.; Yu, M.; Ruhl, J.; Tatalovich, Z.; et al. SEER Cancer Statistics Review, 1975–2013; National Cancer Institute: Bethesda, MD, USA, 2016.
- Cortet, M.; Bertaut, A.; Molinie, F.; Bara, S.; Beltjens, F.; Coutant, C.; Arveux, P. Trends in molecular subtypes of breast cancer: Description of incidence rates between 2007 and 2012 from three French registries. BMC Cancer 2018, 18, 161. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hou, G.; Zhang, S.; Zhang, X.; Wang, P.; Hao, X.; Zhang, J. Clinical pathological characteristics and prognostic analysis of 1,013 breast cancer patients with diabetes. Breast Cancer Res. Treat. 2013, 137, 807–816. [Google Scholar] [CrossRef] [PubMed]
- Li, Z.; Luo, Y.; Gong, Y.; Liu, Y.; Qiu, W.; Tu, J. Clinical features and molecular phenotypes of breast cancer in patients with type-2 diabetes mellitus. Asian Pac. J. Cancer Prev. 2011, 12, 2183–2188. [Google Scholar]
- Bronsveld, H.K.; Jensen, V.; Vahl, P.; De Bruin, M.L.; Cornelissen, S.; Sanders, J.; Auvinen, A.; Haukka, J.; Andersen, M.; Vestergaard, P.; et al. Diabetes and Breast Cancer Subtypes. PLoS ONE 2017, 12, e0170084. [Google Scholar] [CrossRef] [PubMed]
- Turkoz, F.P.; Solak, M.; Petekkaya, I.; Keskin, O.; Kertmen, N.; Sarici, F.; Arik, Z.; Babacan, T.; Ozisik, Y.; Altundag, K. The prognostic impact of obesity on molecular subtypes of breast cancer in premenopausal women. J. BUON Off. J. Balk. Union Oncol. 2013, 18, 335–341. [Google Scholar]
- Nattenmüller, C.J.; Kriegsmann, M.; Sookthai, D.; Fortner, R.T.; Steffen, A.; Walter, B.; Johnson, T.; Kneisel, J.; Katzke, V.; Bergmann, M.; et al. Obesity as risk factor for subtypes of breast cancer: Results from a prospective cohort study. BMC Cancer 2018, 18, 616. [Google Scholar] [CrossRef]
- Uldry, M.; Thorens, B. The SLC2 family of facilitated hexose and polyol transporters. Pflüg. Arch. 2004, 447, 480–489. [Google Scholar] [CrossRef] [Green Version]
- Hussein, Y.R.; Bandyopadhyay, S.; Semaan, A.; Ahmed, Q.; Albashiti, B.; Jazaerly, T.; Nahleh, Z.; Ali-Fehmi, R. Glut-1 Expression Correlates with Basal-like Breast Cancer. Transl. Oncol. 2011, 4, 321–327. [Google Scholar] [CrossRef] [Green Version]
- Kuo, S.-J.; Wu, Y.-C.; Chen, C.-P.; Tseng, H.-S.; Chen, D.-R. Expression of Glucose Transporter-1 in Taiwanese Patients with Breast Carcinoma—A Preliminary Report. Kaohsiung J. Med. Sci. 2006, 22, 339–345. [Google Scholar] [CrossRef] [Green Version]
- Choi, J.; Kim, D.H.; Jung, W.H.; Koo, J.S. Metabolic interaction between cancer cells and stromal cells according to breast cancer molecular subtype. Breast Cancer Res. 2013, 15, R78. [Google Scholar] [CrossRef] [Green Version]
- Kang, S.S.; Chun, Y.K.; Hur, M.H.; Lee, H.K.; Kim, Y.J.; Hong, S.R.; Lee, J.H.; Lee, S.G.; Park, Y.K. Clinical Significance of Glucose Transporter 1 (GLUT1) Expression in Human Breast Carcinoma. Jpn. J. Cancer Res. 2002, 93, 1123–1128. [Google Scholar] [CrossRef]
- Jang, S.M.; Han, H.; Jang, K.-S.; Jun, Y.J.; Jang, S.-H.; Min, K.-W.; Chung, M.S.; Paik, S.S. The Glycolytic Phenotype is Correlated with Aggressiveness and Poor Prognosis in Invasive Ductal Carcinomas. J. Breast Cancer 2012, 15, 172–180. [Google Scholar] [CrossRef]
- Pinheiro, C.; Sousa, B.; Albergaria, A.; Paredes, J.; Dufloth, R.; Vieira, D.; Schmitt, F.; Baltazar, F. GLUT1 and CAIX expression profiles in breast cancer correlate with adverse prognostic factors and MCT1 overexpression. Histol. Histopathol. 2011, 26, 1279–1286. [Google Scholar] [PubMed]
- Deng, Y.; Zou, J.; Deng, T.; Liu, J. Clinicopathological and prognostic significance of GLUT1 in breast cancer: A meta-analysis. Medicine 2018, 97, e12961. [Google Scholar] [CrossRef] [PubMed]
- Rogers, S.; Macheda, M.; Docherty, S.E.; Carty, M.D.; Henderson, M.A.; Soeller, W.C.; Gibbs, E.M.; James, D.; Best, J. Identification of a novel glucose transporter-like protein—GLUT-12. Am. J. Physiol. Metab. 2002, 282, E733–E738. [Google Scholar] [CrossRef]
- Netea-Maier, R.T.; Smit, J.W.A.; Netea, M.G. Metabolic changes in tumor cells and tumor-associated macrophages: A mutual relationship. Cancer Lett. 2018, 413, 102–109. [Google Scholar] [CrossRef]
- Kim, J.; DeBerardinis, R.J. Mechanisms and Implications of Metabolic Heterogeneity in Cancer. Cell Metab. 2019, 30, 434–446. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.; Zhang, S.; Wang, X. The Metabolic Mechanisms of Breast Cancer Metastasis. Front. Oncol. 2021, 10, 602416. [Google Scholar] [CrossRef] [PubMed]
- Wellberg, E.A.; Johnson, S.; Finlay-Schultz, J.; Lewis, A.S.; Terrell, K.L.; Sartorius, C.A.; Abel, E.D.; Muller, W.J.; Anderson, S.M. The glucose transporter GLUT1 is required for ErbB2-induced mammary tumorigenesis. Breast Cancer Res. 2016, 18, 131. [Google Scholar] [CrossRef] [Green Version]
- Allred, D.C.; Clark, G.M.; Tandon, A.K.; Molina, R.; Tormey, D.C.; Osborne, C.K.; Gilchrist, K.W.; Mansour, E.G.; Abeloff, M.; Eudey, L. HER-2/neu in node-negative breast cancer: Prognostic significance of overexpression influenced by the presence of in situ carcinoma. J. Clin. Oncol. J. Am. Soc. Clin. Oncol. 1992, 10, 599–605. [Google Scholar] [CrossRef]
- de la Cruz-López, K.G.; Castro-Muñoz, L.J.; Reyes-Hernández, D.O.; García-Carrancá, A.; Manzo-Merino, J. Lactate in the Regulation of Tumor Microenvironment and Therapeutic Approaches. Front. Oncol. 2019, 9, 1143. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, C.-L.; Chu, J.-S.; Su, W.-C.; Huang, S.-C.; Lee, W.-Y. Hypoxia and metabolic phenotypes during breast carcinogenesis: Expression of HIF-1α, GLUT1, and CAIX. Virchows Arch. 2010, 457, 53–61. [Google Scholar] [CrossRef] [PubMed]
- Tirpe, A.A.; Gulei, D.; Ciortea, S.M.; Crivii, C.; Berindan-Neagoe, I. Hypoxia: Overview on Hypoxia-Mediated Mechanisms with a Focus on the Role of HIF Genes. Int. J. Mol. Sci. 2019, 20, 6140. [Google Scholar] [CrossRef] [Green Version]
- Mendez, L.E.; Manci, N.; Cantuaria, G.; Gomez-Marin, O.; Penalver, M.; Braunschweiger, P.; Nadji, M. Expression of Glucose Transporter-1 in Cervical Cancer and Its Precursors. Gynecol. Oncol. 2002, 86, 138–143. [Google Scholar] [CrossRef]
- Al Tameemi, W.; Dale, T.P.; Al-Jumaily, R.M.K.; Forsyth, N.R. Hypoxia-Modified Cancer Cell Metabolism. Front. Cell Dev. Biol. 2019, 7, 4. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ganapathy, V.; Thangaraju, M.; Prasad, P.D. Nutrient transporters in cancer: Relevance to Warburg hypothesis and beyond. Pharmacol. Ther. 2009, 121, 29–40. [Google Scholar] [CrossRef] [PubMed]
- Oh, S.; Kim, H.; Nam, K.; Shin, I. Glut1 promotes cell proliferation, migration and invasion by regulating epidermal growth factor receptor and integrin signaling in triple-negative breast cancer cells. BMB Rep. 2017, 50, 132–137. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Age (year) † (n = 190) | 53.5 [45.0;63.0] | Modified SBR (n = 187) | |
|---|---|---|---|
| BMI (kg/m2) † (n = 162) | 26.6 [23.1;30.5] | I | 18 (9.6%) |
| II | 117 (62.6%) | ||
| Tumor size (cm) † (n = 190) | 2.8 [1.6;4.1] | III | 52 (27.8%) |
| HR+ * (n = 189) | 131 (69.3%) | ||
| M+ * (n = 190) | 13 (6.8%) | ||
| N+ * (n = 190) | 57 (30.0%) | HER2+ * (n = 186) | 41 (22.0%) |
| Histological types (n = 190) | Ki67 † (n = 183) | 20 [10;40] | |
| NST | 172 (90.6%) | Molecular Groups * | |
| CLI | 11 (5.8%) | (n = 186) | |
| CPI | 4 (2.1%) | Luminal A | 108 (58.1%) |
| Tubular | 1 (0.5%) | Luminal B | 21 (11.3%) |
| Micro-papillary | 1 | HER2 enriched | 20 (10.7%) |
| Mucinous | 1 | TNBC | 37 (19.9%) |
| Age Groups (Years) | Nb. (%) |
|---|---|
| <35 | 10 (5.2) |
| 35–49 | 63 (33.2) |
| 50–64 | 71 (37.4) |
| 65–74 | 23 (12.1) |
| ≥75 | 23 (12.1) |
| Size (cm) | Nb. (%) |
|---|---|
| <2 cm | 40 (30.3%) |
| 2–5 cm | 66 (50%) |
| >5 cm | 26 (19.7%) |
| Category | BMI (kg/m2) | Nb. (%) |
|---|---|---|
| Thinness | <18.5 | 2 (1.2) |
| Normal weight | [18.5–24.9] | 55 (34.0) |
| Overweight | [25–29.9] | 61 (37.7) |
| Obesity including: | ≥30 | 44 (27.1) |
| Obesity class 1 | [30–34.9] | 27 (16.7) |
| Obesity class 2 | [35–39.9] | 12 (7.4) |
| Obesity class 3 | ≥40 | 5 (3.0) |
| Parameters | Total (n = 162) | Control (n = 100) | Diabetes (n = 36) | p Value | Obese (n = 26) | p Value |
|---|---|---|---|---|---|---|
| Tumor size (cm) † | 2.8 [1.8;4.5] (n = 129) | 2.8 [1.9;4.2] (n = 76) | 2.5 [1.5;4.0] (n = 32) | 0.370 | 3.6 [2.0;7.0] (n = 21) | 0.378 |
| M+ * | 0.067 | 0.632 | ||||
| Yes | 13 (8.0) | 5 (5.0) | 6 (16.7) | 2 (8.3) | ||
| No | 149 (92.0) | 95 (95.0) | 30 (83.3) | 24 (91.7) | ||
| N+ * | 0.157 | 0.161 | ||||
| Yes | 56 (34.6) | 35 (35.0) | 8 (22,2) | 13 (50.0) | ||
| No | 106 (65.4) | 65 (65.0) | 28 (77.8) | 13 (50.0) | ||
| SBR modified * | 0.246 | 0.329 | ||||
| I | 11 (6.9) | 6 (6.1) | 2 (5.6) | 3 (12.0) | ||
| II | 103 (64.3) | 69 (69.7) | 20 (55.5) | 14 (56.0) | ||
| III | 46 (28.8) | 24 (24.2) | 14 (38.9) | 8 (32.0) | ||
| RH * | 0.203 | 0.061 | ||||
| Positive | 112 (69.6) | 75 (75.0) | 23 (63.9) | 14 (56.0) | ||
| Negatives | 49 (30.4) | 25 (25.0) | 13 (36.1) | 11 (44.0) | ||
| HER2 * | 0.904 | 0.672 | ||||
| Positive | 38 (23.6) | 24 (24.0) | 9 (25.0) | 5 (20.0) | ||
| Negative | 123 (76.4) | 76 (76.0) | 27 (75.0) | 20 (80.0) | ||
| Ki67 † | 20 [20;40] (n= 156) | 20 [10;35] (n = 97) | 20 [10;40] (n = 35) | 0.666 | 27.5 [15;52] (n = 24) | 0.082 |
| Molecular Groups * (Molecular Groups) | 0.780 | 0.256 | ||||
| Luminal A | 90 (55.9) | 59 (59.0) | 19 (52.8) | 12 (48.0) | ||
| Luminal B | 23 (14.3) | 16 (16.0) | 5 (13.9) | 2 (8.0) | ||
| HER2 enriched | 16 (9.9) | 9 (9.0) | 4 (11.1) | 3 (12.0) | ||
| TNBC | 32 (19.9) | 16 (16.0) | 8 (22.2) | 8 (32.0) |
| Total Nb. (%) | Control Group Nb. (%) | Diabetes Nb. (%) | p Value | Obese Nb. (%) | p Value | |
|---|---|---|---|---|---|---|
| Overexpression of GLUT-1 | 0.732 | 0.833 | ||||
| Yes | 87 (60.4) | 56 (61.5) | 18 (58.1) | 13 (59.1) | ||
| No | 57 (39.6) | 35 (38.5) | 13 (41.9) | 9 (40.9) | ||
| Total | 144 (100) | 91 (63.2) | 31 (21.5) | 22 (15.3) |
| GLUT-1 Overexpressing | GLUT-1 Not Overexpressed | p Value | |
|---|---|---|---|
| Size (cm) † | 2.5 [2.0;4.6] (n = 69) | 3 [1.8;5.0] (n = 44) | 0.594 |
| M+ * | 0.344 | ||
| Yes | 5 (5.7) | 6 (10.5) | |
| No | 82 (94.3) | 51 (89.5) | |
| N+ * | 0.887 | ||
| Yes | 30 (34.5) | 19 (51.4) | |
| No | 57 (65.5) | 38 (48.6) | |
| Modified SBR | 0.000420 | ||
| I | 6 (7.0) | 4 (7.0) | |
| II | 49 (57.0) | 48 (84.2) | |
| III | 31 (36.0) | 5 (8.8) | |
| RH * | 0.000131 | ||
| Positive | 50 (57.5) | 52 (91.2) | |
| Negative | 37 (42.5) | 5 (8.8) | |
| HER2 * | 0.020 | ||
| Positive | 27 (31.0) | 8 (14.0) | |
| Negative | 60 (69.0) | 49 (86) | |
| Ki67 † | 28 [16;60] (n = 86) | 15 [10;20] (n = 54) | 4.51 × 10−6 |
| Molecular Groups * | 2.91 × 10−6 | ||
| Luminal A | 35 (40.2) | 47 (82.5) | |
| Luminal B | 16 (18.4) | 5 (8.8) | |
| HER2 enriched | 12 (13.8) | 3 (5.3) | |
| Triple negative | 24 (27.6) | 2 (3.4) |
| GLUT-1 Over. | Total (n = 144) | Control (n = 91) | Diabetes (n = 31) | Value of p | Obese (n = 22) | Value of p | |
|---|---|---|---|---|---|---|---|
| Tumor size (cm) † | |||||||
| Yes | 2.5 [2.0;4.6] (n = 69) | 2.8 [1.8;4.1] (n = 44) | 3.5 [1.7;4.1] (n = 15) | 0.780 | 5.2 [3.1;11.5] (n = 10) | 0.106 | |
| No | 3.0 [1.8;5.0] (n = 44) | 2.5 [1.9;5.0] (n = 25) | 2.4 [2.0;4.0] (n = 12) | 0.696 | 2.6 [2.3;4.9] (n = 10) | 0.855 | |
| M+ * | 1 | 1 | |||||
| Yes | 5 (45.4) | 2 (40.0) | 2 (50.0) | 1 (33.3) | |||
| No | 6 (54.6) | 3 (60.0) | 2 (50.0) | 2 (66.7) | |||
| N+ * | 0.677 | 0.735 | |||||
| Yes | 30 | 18 | 3 | 9 | |||
| No | 19 | 12 | 3 | 4 | |||
| Modified SBR | Yes | 0.270 | 0.125 | ||||
| I | 6 | 3 | 2 | 1 | |||
| II | 49 | 36 | 8 | 5 | |||
| III | 31 | 16 | 8 | 7 | |||
| No | 0.209 | 1 | |||||
| I | 4 | 3 | 0 | 1 | |||
| II | 48 | 30 | 10 | 8 | |||
| III | 5 | 2 | 3 | 0 | |||
| HR+ * | 0.574 | 0.254 | |||||
| Yes | 50 (49.0) | 37 (52,1) | 9 (45.0) | 9 (69.2) | |||
| No | 52 (51.0) | 34 (47.9) | 11 (55.0) | 4 (30.8) | |||
| HER2+ * | 1 | 1 | |||||
| Yes | 27 (49.0) | 17 (77.3) | 6 (75.0) | 4 (80.0) | |||
| No | 8 (22.9) | 5 (22.7) | 2 (25.0) | 1 (20.0) | |||
| Ki67 † | |||||||
| Yes | 28 [16;60] (n = 86) | 22 [15;54] (n = 55) | 35 [20;56] (n = 18) | 0.195 | 33 [25;65] (n = 13) | 0.144 | |
| No | 15 [10;20] (n = 54) | 15 [10;20] (n = 33) | 15 [10;18] (n = 13) | 0.641 | 19 [12;38] (n = 8) | 0.185 |
| Non-Obese Diabetics No. (%) | Rest of the Population No. (%) | Total No. (%) | p Value | |
|---|---|---|---|---|
| 0.718 | ||||
| GLUT-1 overexpressing | 9 (56.2) | 78 (60.9) | 87 (60.4) | |
| GLUT-1 not overexpressed | 7 (43.8) | 50 (39.1) | 57 (39.6) | |
| Total No. % | 16 (11.1) | 128 (88.9) | 144 (100) |
| Obese No. (%) | Non-Obese No. % | Total No. (%) | p Value | |
|---|---|---|---|---|
| 0.890 | ||||
| GLUT-1 overexpressing | 22 (59.5) | 65 (60.7) | 87 (60.4) | |
| GLUT-1 not overexpressed | 15 (40.5) | 42 (39.3) | 57 (39.6) | |
| Total No. % | 37 (25.7) | 107 (74.3) | 144 (100) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Suteau, V.; Bukasa-Kakamba, J.; Virjogh-Cenciu, B.; Adenis, A.; Sabbah, N.; Drak Alsibai, K. Pathological Significance of GLUT-1 Expression in Breast Cancer Cells in Diabetic and Obese Patients: The French Guiana Study. Cancers 2022, 14, 437. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers14020437
Suteau V, Bukasa-Kakamba J, Virjogh-Cenciu B, Adenis A, Sabbah N, Drak Alsibai K. Pathological Significance of GLUT-1 Expression in Breast Cancer Cells in Diabetic and Obese Patients: The French Guiana Study. Cancers. 2022; 14(2):437. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers14020437
Chicago/Turabian StyleSuteau, Valentin, John Bukasa-Kakamba, Beatrice Virjogh-Cenciu, Antoine Adenis, Nadia Sabbah, and Kinan Drak Alsibai. 2022. "Pathological Significance of GLUT-1 Expression in Breast Cancer Cells in Diabetic and Obese Patients: The French Guiana Study" Cancers 14, no. 2: 437. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers14020437