
Genomics of Plasma Cell Leukemia


1
Hematology Department, University Hospital of Salamanca, Institute of Biomedical Research of Salamanca (IBSAL), 37007 Salamanca, Spain
2
Cancer Research Center-Institute of Cancer Molecular and Cellular Biology (CIC-IBMCC) (USAL-CSIC), 37007 Salamanca, Spain
3
Centro de Investigación Biomédica en Red de Cáncer (CIBERONC), CB16/12/00233, 28029 Madrid, Spain
4
Grupo Español de Mieloma (GEM), 28040 Madrid, Spain
*
Author to whom correspondence should be addressed.
Cancers 2022, 14(6), 1594; https://0-doi-org.brum.beds.ac.uk/10.3390/cancers14061594
Submission received: 1 February 2022
/
Revised: 12 March 2022
/
Accepted: 16 March 2022
/
Published: 21 March 2022
(This article belongs to the Special Issue Genomics of Rare Hematologic Cancers)
Abstract
:Simple Summary
Plasma cell leukemia (PCL) is a very aggressive plasma cell disorder with a dismal prognosis, despite the therapeutic progress made in the last few years. The implementation of genomic high-throughput technologies in the clinical setting has revealed new insights into the genomic landscape of PCL, some of which may have an impact on the development of novel therapeutic approaches. The purpose of this review is to provide a comprehensive overview and update of the genomic studies carried out in PCL.
Abstract
Plasma cell leukemia (PCL) is a rare and highly aggressive plasma cell dyscrasia characterized by the presence of clonal circulating plasma cells in peripheral blood. PCL accounts for approximately 2–4% of all multiple myeloma (MM) cases. PCL can be classified in primary PCL (pPCL) when it appears de novo and in secondary PCL (sPCL) when it arises from a pre-existing relapsed/refractory MM. Despite the improvement in treatment modalities, the prognosis remains very poor. There is growing evidence that pPCL is a different clinicopathological entity as compared to MM, although the mechanisms underlying its pathogenesis are not fully elucidated. The development of new high-throughput technologies, such as microarrays and new generation sequencing (NGS), has contributed to a better understanding of the peculiar biological and clinical features of this disease. Relevant information is now available on cytogenetic alterations, genetic variants, transcriptome, methylation patterns, and non-coding RNA profiles. Additionally, attempts have been made to integrate genomic alterations with gene expression data. However, given the low frequency of PCL, most of the genetic information comes from retrospective studies with a small number of patients, sometimes leading to inconsistent results.
1. Introduction
Plasma cell leukemia (PCL) is an uncommon plasma cell dyscrasia with an aggressive course and poor prognosis. PCL represents less than 3% of all plasma cells neoplasms, and its incidence has been estimated at 0.04 cases per 100,000 persons/year [1,2].
Historically, PCL has been defined by the presence of more than 20% of circulating plasma cells (PCs) and an absolute number of ≥2 × 109/L of PCs in peripheral blood [3]. However, in some studies, only the presence of one of these criteria had been considered to define PCL. Moreover, recent studies have shown that much lower levels of circulating PC have the same adverse prognostic impact. Accordingly, the consensus recently published by the International Myeloma Working Group (IMWG) states that PCL is defined by the presence of 5% or more circulating plasma cells in peripheral blood [4].
PCL is classified as primary PCL (pPCL) when it occurs de novo so that the patient has no evidence of previous multiple myeloma (MM), and as secondary PCL (sPCL) when leukemic progression occurs in the context of pre-existing refractory or relapsing MM [5,6]. pPCL is more frequent than sPCL, representing about 60–70% of patients, [7] and occurs in patients significantly younger than sPCL. Nevertheless, the number of sPCL cases has been increasing in recent years, which is probably related to the increased survival of MM patients.
The clinical presentation of PCL is more aggressive than that observed in MM, including more severe cytopenias, hypercalcemia, and renal insufficiency. Higher tumor burden and proliferation activity of PCL are manifested by greater levels of B2-microglobulin and lactate dehydrogenase (LDH). Extramedullary involvement (lymph nodes, liver, spleen, pleura, and central nervous system) at diagnosis is more common in pPCL and sPCL than in MM, but osteolytic lesions are more frequent in sPCL and MM than in pPCL [8,9,10,11,12,13].
Various studies have analyzed the immunophenotype of PCL. The two common PCs markers, CD38 and CD138 antigens, are similarly expressed in MM and PCL. However, PCL displays a more immature phenotype than MM, expressing more frequently CD20, CD23, CD28, CD44, and CD45, and less frequently CD9, CD56, CD71, CD117, and HLA-DR antigens [14,15,16].
PCL patients are characterized by short remissions and early relapses. The 5-year survival rate from the diagnosis of PCL does not exceed 10%. Survival of sPCL patients is consistently shorter than pPCL [8]. The incorporation of new therapeutic agents has not achieved significant improvements in the survival of PCL, unlike what has been attained in MM. The low incidence of PCL makes it difficult to conduct studies aimed at exploring the efficacy of new drugs that would eventually help to establish an optimal therapeutic option. Thus, therapeutic recommendations are supported by small prospective and retrospective studies and sometimes by data extrapolated from clinical trials with MM patients. The therapeutic strategy usually followed in transplant-candidate patients generally includes an intensive induction with bortezomib-based regimens also containing lenalidomide and chemotherapeutic agents. After autologous stem cell transplantation (ASCT), there is increasing consensus on continuing a consolidation and maintenance therapy, although the therapeutic agents that should be included are not well established. A tandem transplant with an ASCT followed by reduced-intensity allogenic transplantation can also be considered. However, even using the most intensive therapeutic arsenal, the prognosis of PCL remains ominous. There is, therefore, a compelling need to advance in the search for new drugs with different mechanisms of action and more closely related to the genetic features of tumor PC. In this regard, the development of BCL2 inhibitors and the new immunotherapeutic approaches, such as chimeric antigen receptor T-cells (CAR-T cells) and monoclonal and bispecific antibodies, opens up new opportunities in the treatment of PCL patients.
Early cytogenetic studies performed in PCL had already revealed some differences between this entity and MM. Later on, the widespread use of fluorescence in situ hybridization (FISH) has increased our knowledge of genetic alterations. In recent years, the development of high-throughput genomic analysis tools has helped to better understand the genetic particularities of PCL. However, the robustness of the results is undermined by the limited number of patients included in the studies because of the low incidence of this disease. In this review, we mainly focus on the genomic characteristics of pPCL, although some data concerning sPCL are provided when considered of interest. A summary of the most relevant results provided by the main genomic studies carried out in PCL is shown in Table 1.
2. Cytogenetic Abnormalities
Early cytogenetic and DNA content studies carried out in PCL revealed that there was a predominance of non-hyperdiploid cases (more than 50% of pPCL) compared to that observed in MM [8,14,18]. These results were confirmed in subsequent studies using not only conventional karyotyping but also molecular cytogenetic techniques such as comparative genomic hybridization (CGH) and single nucleotide polymorphism (SNP)-arrays, which showed that pPCL had more DNA copy number changes with a predominance of chromosomal losses in contrast to MM [19,27]. As in MM, FISH has been routinely carried out to identify cytogenetic alterations present in pPCL at the time of diagnosis. Virtually all the studies reporting data provided by FISH analysis, sometimes in combination with other cytogenetic techniques, point out that the chromosomal abnormalities observed in pPCL are mostly the same recurrently found in MM, although many of them are present with greater frequency (Figure 1).
Monosomy and deletions of chromosome 13 (del(13q)) have been observed in approximately 85% of pPCL [8,22,35]. Abnormalities of chromosome 1 are also frequent in pPCL patients. Gain (3 copies) and amplification (≥4 copies) of chromosome arm 1q21 (gain/amp(1q)) have been reported in around 70% of pPCL cases [35,36]. Although the frequency of gain/amp(1q) does not reach such a high percentage in newly diagnosed MM patients, the incidence of this abnormality increases in relapsed/refractory MM up to 50–80% [22,43,44]. Likewise, most of the studies have shown greater frequency of deletion of 1p (del(1p)) in pPCL than in MM patients (24–33% vs. 9–18%, respectively) [22,41]. While the impact of abnormalities in chromosome 1, both gain/amp(1q) and del(1p), on the survival of patients with MM is well established [45,46], their effect on the prognosis of pPCL is still poorly substantiated. Only one study has reported that del(1p), but not gain/amp(1q), is associated with shorter survival of PCL patients, although the set of sPCL included in the study may be biasing the influence that this chromosomal alteration might have on pPCL considered as a separate entity [22]. Deletion of 17p (del(17p)), although uncommon in MM at the time of diagnosis, reaches frequencies of 50% in pPCL [8,22,27,32,37]. However, it seems to have no impact on the prognosis of pPCL, unlike in MM [8,22].
Taken together, all these results showing the increasing frequency of the aforementioned chromosome imbalances from MM to PCL support the multistep transformation model from monoclonal gammopathy of undetermined significance (MGUS) through smoldering multiple myeloma (SMM) and MM to PCL that leads to progressive accumulation of secondary genetic alterations.
The incidence of IGH translocations is significantly higher in pPCL than in MM. Several studies show that t(11;14) leading to CCND1 dysregulation are significantly more frequent in pPCL than in MM, reaching percentages as high as 45–70% in some series [8,17,18,21,22,23,24,27,40,41]; also noteworthy is the high proportion of t(14;16) detected in pPCL compared with MM (13–25% vs. 1–5%, respectively), which is supported by five studies [18,21,23,36,41]. Conversely, in most of the studies, t(4;14) has been found to be less frequent in pPCL than in MM [23,36,38].
The t(11;14) has largely been demonstrated to be a neutral prognostic factor for MM survival [47]. Although no influence of t(11;14) in the survival of pPCL patients was initially observed [8,22], it has recently been reported that pPCL patients bearing t(11;14) had a significantly longer OS than those without this abnormality [42]. On the contrary, t(4;14) has been associated with poor prognosis [22].
3. Gene Mutations
Before the availability of next-generation sequencing (NGS) technologies, the mutational status of RAS oncogenes (NRAS and KRAS), the two most prevalent mutated genes in MM, and of the tumor suppressor TP53, had been explored in pPCL using traditional DNA sequencing methodologies. Two studies demonstrated a high incidence of NRAS and KRAS activating mutations: one of them reported these mutations at codons 12, 13, or 61 in 27% of pPCL and 15% of sPCL cases [8], and in the other study NRAS and/or KRAS mutations were found in 50% of pPCL cases and in 55% of MM [20]. Strikingly, these findings were not confirmed in a subsequent study [27]. TP53 is one of the most frequently mutated genes in pPCL in all the published series, reaching frequencies of 25% [8,23,27]. The proportion of cases with biallelic inactivation of TP53 is also greater in pPCL than in MM (17–35% vs. 3–4%) [8,27]. TP53 coding mutations involving 5–8 exons were found, predicting all of them a non-functional p53 protein [8,27] (Figure 1).
The first whole-exome sequencing (WES) analysis of pPCL revealed a highly heterogeneous mutational profile [29]. Almost 2000 coding somatic non-silent variants on 1643 genes were described, with more than 160 variants per sample, although with hardly any recurrent mutations in two or more samples. Fourteen mutated genes mainly involved in cell cycle and apoptosis (CIDEC), RNA binding and degradation (DIS3, RPL17), and cell-matrix adhesion and membrane organization (SPTB, CELA1) were considered as potential cancer driver genes in pPCL. Other studies have confirmed that the number of nonsynonymous mutations per sample is higher in pPCL than in MM [36].
As in MM, activating N/KRAS mutations have been identified in pPCL using WES methodologies, although the proportions were significantly unequal between the two of the studies. The first study reported mutations of KRAS and NRAS only in two distinct samples (<10% of the pPCL). This study highlighted that KRAS and NRAS were three-fold less frequently mutated in pPCL compared to that observed in MM [29]. On the contrary, the second study also using WES methodology found that KRAS was the most frequently mutated gene in pPCL samples (around 39%), and mutations of NRAS were present in 13% of pPCL [36]. Using targeted NGS approaches, KRAS mutations were detected in 17% of pPCL, 18% of sPCL, and 33% of MM, and NRAS mutations in 4% of pPCL, 36% of sPCL, and 27% of MM [30]. Apparently, the MEK/ERK signaling pathway was less affected by mutation events in pPCL than in sPCL and MM [30].
Mutations of the BRAF gene have also been detected in pPCL samples. A low frequency and even absence of BRAF mutations in pPCL patients have been described using WES [29,36]. However, when targeted NGS was applied, the frequency of BRAF mutations detected in pPCL was higher (21% in pPCL and 9% in sPCL). It is worth highlighting the role that the different coverage levels among NGS studies and the small number of patients analyzed may be playing in the conflicting results.
TP53 gene has also been analyzed by NGS in pPCL [32,36,41], confirming the results previously observed using traditional DNA sequencing methodologies, namely, the high proportion of TP53 mutations in pPCL. Interestingly, the presence of TP53 mutations has been associated with significantly shorter survival in the study, including the largest number of patients with pPCL to date [41]. IRF4 mutations have recently been shown to be significantly more frequent in pPCL than in MM patients (11% vs. 4%) [41]. Other gene mutations commonly observed in MM have also been reported in pPCL but with different frequencies. Schinke et al. detected DIS3 and PRMD1 mutations in 5% and 13% of patients with pPCL, respectively, while Cifola et al. identified DIS3 mutations in 25% of cases and no variants in the PRMD1 gene. Both studies have described a similar incidence of FAM46C mutation (10–12%) in pPCL patients [29,36].
4. Transcriptome Characterization
Several studies have explored the gene expression profile (GEP) analyzed by microarrays in pPCL. All of them have identified a transcriptome signature characteristic of pPCL and different from that of MM. The first two reports identified a gene-specific signature that distinguished pPCL from MM cases, although the number of overlapped genes between both datasets containing the differentially expressed genes was only around 15%. The functional annotation analysis identified dysregulation of lipid metabolism, glucocorticoid receptor, and IL6 pathways in one study [25], and alterations of NF-kB pathway, FAS signaling, structural organization of the cell and migration processes in the other study [28]. A transcriptional signature including 27 genes has been associated with the overall survival of pPCL, despite the cytogenetic alterations. Interestingly, none of these genes had been selected in MM-high risk signatures [28].
More recently, the GEP of 41 pPCL patients has been compared to that of more than 700 newly diagnosed MM [36]. In pPCL, the analysis showed overexpression of genes previously related to MM biology or prognosis, such as PHF19 and TAGLN2, and underexpression of the adhesion molecules VCAM1 and CD163, which are highly expressed in MM and have been correlated with poor survival [51,52].
RNA-seq analysis of pPCL has also shown a specific transcriptional landscape of pPCL, as previously demonstrated by GEP using microarrays. Compared to MM, pPCL showed significantly higher expression of genes involved in G2M checkpoint and MYC target genes and lower expression of genes involved in p53 pathway, hypoxia, and TNF alpha signaling via NF-κB [41]. In this regard, significant overexpression of CDKN2A, CCND3, and CCND1 genes, using quantitative RT-PCR, has been reported in PCL compared to MM samples, indicating a marked cell cycle dysregulation in the transition from MM to PCL [53].
A comprehensive molecular analysis of pPCL integrating data from FISH, SNP-arrays, and GEP has revealed a strong correlation between chromosomal imbalances and transcriptional modulation. The gene dosage effect was particularly observed in those genes mapping 1q chromosome [27]. In addition, the analysis of upregulated and downregulated transcripts in the gained and lost chromosomal regions, respectively, found that protein transport, translation, and biosynthesis functional categories were upregulated in pPCL cases with gained chromosomal regions, whereas RNA splicing, protein catabolic process, and regulation of apoptosis were downregulated in pPCL cases with deleted regions.
Differences between the gene expression signature of pPCL and MM could be partly attributed to the dissimilar distribution of genetic abnormalities between the two diseases. This fact prompted us to compare the transcriptome of pPCL and MM patients using samples with del(17p) and a similar cytogenetic background [34]. This approach revealed that pPCL and MM were separated into two differentiated clusters despite the equivalent cytogenetic profile shared by both entities. Differentially expressed genes were mostly downregulated in pPCL, among which were genes associated with bone marrow microenvironment and bone diseases in MM, such as DKK1, KIT, NCAM1, and FRZB (Figure 1). Interestingly, the analysis focused on isoform expression showed that dysregulation of RNA splicing machinery may be a relevant molecular mechanism underlying the biological differences between the pPCL and MM.
A similar approach has been used to ascertain the differences in the transcriptome between pPCL and MM samples harboring t(11;14) [38]. In line with our results, this study shows that both plasma cell dyscrasias are clearly distinguishable based on the transcriptome profile despite sharing a uniform genetic background. pPCL with t(11;14) were positively associated with genes involved in IL2-STAT5 signaling but negatively associated with the regulation of cell and cell adhesion pathways. In any case, the most relevant finding of this study was that pPCL showed a different expression pattern of the BCL2 family genes and of the B-cell-associated genes, despite the presence of t(11;14) in both PCL and MM samples. These results suggest that the efficacy of venetoclax in pPCL and MM patients with t(11;14) may be associated with different molecular programs.
5. Non-Coding RNA Profile
Non-coding RNAs (ncRNAs) are classified as short (<200 nucleotides) and long (>200 nucleotides). The miRNAs are short ncRNAs of 19–22 nucleotides that regulate gene expression at the post-transcriptional level. Since their discovery, numerous studies have attributed a wide variety of functions for ncRNAs in the pathogenic mechanisms of MM [54,55,56].
There is only one study analyzing the expression pattern of miRNAs in pPCL [26]. The analysis of 18 pPCL identified 42 upregulated and 41 downregulated miRNAs in pPCL when compared with MM samples. Moreover, seven miRNAs were found to be differentially expressed depending on the type of IGH translocation. Three miRNAs (let-7e, miR-135a, and miR-148a) were overexpressed in PCL patients with t(4;14); three (miR-7, miR-7-1, and miR-454) underexpressed in PCL with t(14;16); and the miR-342-3p was underexpressed in PCL with t(11;14). Notably, four miRNAs, miR-22, miR-146a, miR-92a, and miR-330-3p, were found to have an impact on the survival of pPCL patients. The overexpression of miR-146a, which was associated with shorter progression-free survival (PFS) in pPCL cases, and miR-22, which was associated with longer PFS, showed a pro- and anti-survival effect, respectively, in myeloma cell lines [26]. Accordingly, one study has demonstrated that MM cells stimulate the overexpression of miR-146a in mesenchymal stromal cells, resulting in more cytokine secretion and enhancing cell viability of MM cells [57] (Figure 1).
Long non-coding RNAs (lncRNAs) are a group of very heterogeneous non-coding RNAs with a length of more than 200 nucleotides. They have a similar structure to mRNAs but are not translated to functional proteins. LncRNAs represent more than 50% of the non-coding RNAs, and their functions are related to the regulation of transcription, genome integrity, cell differentiation, X-chromosome inactivation, and development, among others [58].
LncRNAs expression profile has also been investigated in a large cohort of PC dyscrasias, including samples from MGUS, SMM, MM, and PCL together with NPC [31]. Differential expression of 160 lncRNAs between NPC and the four premalignant and malignant entities was detected. In particular, expression levels of 15 lncRNAs were progressively increased from NPC to PCL patients, while six lncRNAs showed a significant decrease in the transition from NPC and premalignant entities to more aggressive forms. LncRNAs involved in the progression from MM to PCL have recently been explored [39]. A total of 13 dysregulated lncRNAs was detected. A significant underexpression of lymphocyte antigen antisense RNA 1 (LY86-AS1) and VIM antisense RNA 1 (VIM-AS1) was observed in PCL compared to MM and further validated by qRT-PCR. However, their functions in MM to PCL progression remain unknown.
Differential expression of lncRNAs has also been detected between pPCL and MM samples with t(11;14) [38]. In particular, the lncRNA SNHG6, whose overexpression was associated with significantly inferior overall survival in MM patients from the CoMMpass dataset, was found to be upregulated in the pPCL patients.
6. Methylation Patterns
The analysis of global methylation patterns in pPCL using high-density arrays has identified a global hypomethylation profile in pPCL samples [33] (Figure 1). The comparison of methylation levels between pPCL, MM, MGUS, and NPC samples revealed that genes highly methylated in NPC underwent a progressive decrease in the levels of methylation as the aggressiveness of the disease increased from MGUS to MM and pPCL. Curiously, pPCL patients showed distinct methylation profiles depending on the presence of DIS3 gene mutations, t(11;14), and t(14;16). On the contrary, Walker et al. [59] had previously found gene-specific hypermethylation of almost 2000 genes in the transition from MM to PCL, although the number of PCL cases was quite small.
7. Concluding Remarks
Chromosomal, genetic, and genomic alterations found in pPCL are sufficiently different from those observed in MM to consider it a distinct clinicopathological entity and not merely a more aggressive form of MM. However, the low incidence of this disease makes it extremely difficult to gather enough pPCL cases to carry out genomic studies that provide consistent results. On the other hand, the paucity of clinical trials specifically designed for this disease precludes prospective studies. In this regard, proposals aimed at collecting hundreds of pPCL samples involving numerous centers in order to conduct biological studies could represent a breakthrough in identifying dysregulations of signaling pathways that could be therapeutically targeted.
Author Contributions
Conceptualization, N.C.G.; writing original draft, preparation, review, and editing, E.A.R. and N.C.G. All authors have read and agreed to the published version of the manuscript.
Funding
E.A.R. was supported by a fellowship from the Consejería de Educación de Castilla y León and FEDER funds. This study was funded by the Instituto de Salud Carlos III and co-financed by FEDER (PI16/01074 and PI19/00674); by the Asociación Española Contra el Cáncer (AECC) (Proyectos Estratégicos: PROYE20047GUTI); and by the Gerencia Regional de Salud, Junta de Castilla y León grants (GRS 2058/A/19 and GRS 2331/A/21).
Acknowledgments
The authors would like to thank Luzalba Sanoja-Flores for providing the image of flow cytometry.
Conflicts of Interest
E.A.R. declares no conflict of interest. N.C.G.: honoraria from Janssen.
References
- Gundesen, M.T.; Lund, T.; Moeller, H.E.H.; Abildgaard, N. Plasma Cell Leukemia: Definition, Presentation, and Treatment. Curr. Oncol. Rep. 2019, 21, 8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gonsalves, W.I.; Rajkumar, S.V.; Go, R.S.; Dispenzieri, A.; Gupta, V.; Singh, P.P.; Buadi, F.K.; Lacy, M.Q.; Kapoor, P.; Dingli, D.; et al. Trends in Survival of Patients with Primary Plasma Cell Leukemia: A Population-Based Analysis. Blood 2014, 124, 907–912. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fernández de Larrea, C.; Kyle, R.A.; Durie, B.G.M.; Ludwig, H.; Usmani, S.; Vesole, D.H.; Hajek, R.; San Miguel, J.F.; Sezer, O.; Sonneveld, P.; et al. Plasma Cell Leukemia: Consensus Statement on Diagnostic Requirements, Response Criteria and Treatment Recommendations by the International Myeloma Working Group. Leukemia 2013, 27, 780–791. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fernández de Larrea, C.; Kyle, R.; Rosiñol, L.; Paiva, B.; Engelhardt, M.; Usmani, S.; Caers, J.; Gonsalves, W.; Schjesvold, F.; Merlini, G.; et al. Primary Plasma Cell Leukemia: Consensus Definition by the International Myeloma Working Group According to Peripheral Blood Plasma Cell Percentage. Blood Cancer J. 2021, 11, 192. [Google Scholar] [CrossRef]
- Noel, P.; Kyle, R.A. Plasma Cell Leukemia: An Evaluation of Response to Therapy. Am. J. Med. 1987, 83, 1062–1068. [Google Scholar] [CrossRef]
- Albarracin, F.; Fonseca, R. Plasma Cell Leukemia. Blood Rev. 2011, 25, 107–112. [Google Scholar] [CrossRef] [Green Version]
- International Myeloma Working Group. Criteria for the Classification of Monoclonal Gammopathies, Multiple Myeloma and Related Disorders: A Report of the International Myeloma Working Group. Br. J. Haematol. 2003, 121, 749–757. [Google Scholar] [CrossRef] [Green Version]
- Tiedemann, R.E.; Gonzalez-Paz, N.; Kyle, R.A.; Santana-Davila, R.; Price-Troska, T.; Van Wier, S.A.; Chng, W.J.; Ketterling, R.P.; Gertz, M.A.; Henderson, K.; et al. Genetic Aberrations and Survival in Plasma Cell Leukemia. Leukemia 2008, 22, 1044–1052. [Google Scholar] [CrossRef] [Green Version]
- Chaulagain, C.P.; Diacovo, M.-J.; Van, A.; Martinez, F.; Fu, C.-L.; Jimenez Jimenez, A.M.; Ahmed, W.; Anwer, F. Management of Primary Plasma Cell Leukemia Remains Challenging Even in the Era of Novel Agents. Clin. Med. Insights Blood Disord. 2021, 14. [Google Scholar] [CrossRef]
- Mina, R.; D’Agostino, M.; Cerrato, C.; Gay, F.; Palumbo, A. Plasma Cell Leukemia: Update on Biology and Therapy. Leuk. Lymphoma 2017, 58, 1538–1547. [Google Scholar] [CrossRef]
- Jimenez-Zepeda, V.H.; Dominguez-Martinez, V.J. Plasma Cell Leukemia: A Highly Aggressive Monoclonal Gammopathy with a Very Poor Prognosis. Int. J. Hematol. 2009, 89, 259–268. [Google Scholar] [CrossRef] [PubMed]
- Jurczyszyn, A.; Radocha, J.; Davila, J.; Fiala, M.A.; Gozzetti, A.; Grząśko, N.; Robak, P.; Hus, I.; Waszczuk-Gajda, A.; Guzicka-Kazimierczak, R.; et al. Prognostic Indicators in Primary Plasma Cell Leukaemia: A Multicentre Retrospective Study of 117 Patients. Br. J. Haematol. 2018, 180, 831–839. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ramsingh, G.; Mehan, P.; Luo, J.; Vij, R.; Morgensztern, D. Primary Plasma Cell Leukemia: A Surveillance, Epidemiology, and End Results Database Analysis between 1973 and 2004. Cancer 2009, 115, 5734–5739. [Google Scholar] [CrossRef]
- García-Sanz, R.; Orfão, A.; González, M.; Tabernero, M.D.; Bladé, J.; Moro, M.J.; Fernández-Calvo, J.; Sanz, M.A.; Pérez-Simón, J.A.; Rasillo, A.; et al. Primary Plasma Cell Leukemia: Clinical, Immunophenotypic, DNA Ploidy, and Cytogenetic Characteristics. Blood 1999, 93, 1032–1037. [Google Scholar] [CrossRef]
- Kraj, M.; Pogłód, R.; Kopeć-Szlezak, J.; Sokołowska, U.; Woźniak, J.; Kruk, B. C-Kit Receptor (CD117) Expression on Plasma Cells in Monoclonal Gammopathies. Leuk. Lymphoma 2004, 45, 2281–2289. [Google Scholar] [CrossRef]
- Kraj, M.; Kopeć-Szlęzak, J.; Pogłód, R.; Kruk, B. Flow Cytometric Immunophenotypic Characteristics of 36 Cases of Plasma Cell Leukemia. Leuk. Res. 2011, 35, 169–176. [Google Scholar] [CrossRef] [PubMed]
- Avet-Loiseau, H.; Li, J.Y.; Facon, T.; Brigaudeau, C.; Morineau, N.; Maloisel, F.; Rapp, M.J.; Talmant, P.; Trimoreau, F.; Jaccard, A.; et al. High Incidence of Translocations t(11;14)(Q13;Q32) and t(4;14)(P16;Q32) in Patients with Plasma Cell Malignancies. Cancer Res. 1998, 58, 5640–5645. [Google Scholar] [PubMed]
- Avet-Loiseau, H.; Daviet, A.; Brigaudeau, C.; Callet-Bauchu, E.; Terré, C.; Lafage-Pochitaloff, M.; Désangles, F.; Ramond, S.; Talmant, P.; Bataille, R. Cytogenetic, Interphase, and Multicolor Fluorescence in Situ Hybridization Analyses in Primary Plasma Cell Leukemia: A Study of 40 Patients at Diagnosis, on Behalf of the Intergroupe Francophone Du Myélome and the Groupe Français de Cytogénétique Hématologique. Blood 2001, 97, 822–825. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gutiérrez, N.C.; Hernández, J.M.; García, J.L.; Cañizo, M.C.; González, M.; Hernández, J.; González, M.B.; Garciá-Marcos, M.A.; San Miguel, J.F. Differences in Genetic Changes between Multiple Myeloma and Plasma Cell Leukemia Demonstrated by Comparative Genomic Hybridization. Leukemia 2001, 15, 840–845. [Google Scholar] [CrossRef] [Green Version]
- Bezieau, S.; Devilder, M.C.; Avet-Loiseau, H.; Mellerin, M.P.; Puthier, D.; Pennarun, E.; Rapp, M.J.; Harousseau, J.L.; Moisan, J.P.; Bataille, R. High Incidence of N and K-Ras Activating Mutations in Multiple Myeloma and Primary Plasma Cell Leukemia at Diagnosis. Hum. Mutat. 2001, 18, 212–224. [Google Scholar] [CrossRef]
- Avet-Loiseau, H.; Facon, T.; Grosbois, B.; Magrangeas, F.; Rapp, M.-J.; Harousseau, J.-L.; Minvielle, S.; Bataille, R. Intergroupe Francophone du Myélome Oncogenesis of Multiple Myeloma: 14q32 and 13q Chromosomal Abnormalities Are Not Randomly Distributed, but Correlate with Natural History, Immunological Features, and Clinical Presentation. Blood 2002, 99, 2185–2191. [Google Scholar] [CrossRef] [PubMed]
- Chang, H.; Qi, X.; Yeung, J.; Reece, D.; Xu, W.; Patterson, B. Genetic Aberrations Including Chromosome 1 Abnormalities and Clinical Features of Plasma Cell Leukemia. Leuk. Res. 2009, 33, 259–262. [Google Scholar] [CrossRef] [PubMed]
- Chiecchio, L.; Dagrada, G.P.; White, H.E.; Towsend, M.R.; Protheroe, R.K.M.; Cheung, K.L.; Stockley, D.M.; Orchard, K.H.; Cross, N.C.P.; Harrison, C.J.; et al. Frequent Upregulation of MYC in Plasma Cell Leukemia. Genes Chromosomes Cancer 2009, 48, 624–636. [Google Scholar] [CrossRef]
- Pagano, L.; Valentini, C.G.; De Stefano, V.; Venditti, A.; Visani, G.; Petrucci, M.T.; Candoni, A.; Specchia, G.; Visco, C.; Pogliani, E.M.; et al. Primary Plasma Cell Leukemia: A Retrospective Multicenter Study of 73 Patients. Ann. Oncol. 2011, 22, 1628–1635. [Google Scholar] [CrossRef] [PubMed]
- Usmani, S.Z.; Nair, B.; Qu, P.; Hansen, E.; Zhang, Q.; Petty, N.; Waheed, S.; Shaughnessy, J.D.; Alsayed, Y.; Heuck, C.J.; et al. Primary Plasma Cell Leukemia: Clinical and Laboratory Presentation, Gene-Expression Profiling and Clinical Outcome with Total Therapy Protocols. Leukemia 2012, 26, 2398–2405. [Google Scholar] [CrossRef] [PubMed]
- Lionetti, M.; Musto, P.; Di Martino, M.T.; Fabris, S.; Agnelli, L.; Todoerti, K.; Tuana, G.; Mosca, L.; Gallo Cantafio, M.E.; Grieco, V.; et al. Biological and Clinical Relevance of MiRNA Expression Signatures in Primary Plasma Cell Leukemia. Clin. Cancer Res. 2013, 19, 3130–3142. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mosca, L.; Musto, P.; Todoerti, K.; Barbieri, M.; Agnelli, L.; Fabris, S.; Tuana, G.; Lionetti, M.; Bonaparte, E.; Sirchia, S.M.; et al. Genome-Wide Analysis of Primary Plasma Cell Leukemia Identifies Recurrent Imbalances Associated with Changes in Transcriptional Profiles. Am. J. Hematol. 2013, 88, 16–23. [Google Scholar] [CrossRef]
- Todoerti, K.; Agnelli, L.; Fabris, S.; Lionetti, M.; Tuana, G.; Mosca, L.; Lombardi, L.; Grieco, V.; Bianchino, G.; D’Auria, F.; et al. Transcriptional Characterization of a Prospective Series of Primary Plasma Cell Leukemia Revealed Signatures Associated with Tumor Progression and Poorer Outcome. Clin. Cancer Res. 2013, 19, 3247–3258. [Google Scholar] [CrossRef] [Green Version]
- Cifola, I.; Lionetti, M.; Pinatel, E.; Todoerti, K.; Mangano, E.; Pietrelli, A.; Fabris, S.; Mosca, L.; Simeon, V.; Petrucci, M.T.; et al. Whole-Exome Sequencing of Primary Plasma Cell Leukemia Discloses Heterogeneous Mutational Patterns. Oncotarget 2015, 6, 17543–17558. [Google Scholar] [CrossRef]
- Lionetti, M.; Barbieri, M.; Todoerti, K.; Agnelli, L.; Marzorati, S.; Fabris, S.; Ciceri, G.; Galletti, S.; Milesi, G.; Manzoni, M.; et al. Molecular Spectrum of BRAF, NRAS and KRAS Gene Mutations in Plasma Cell Dyscrasias: Implication for MEK-ERK Pathway Activation. Oncotarget 2015, 6, 24205–24217. [Google Scholar] [CrossRef] [Green Version]
- Ronchetti, D.; Agnelli, L.; Taiana, E.; Galletti, S.; Manzoni, M.; Todoerti, K.; Musto, P.; Strozzi, F.; Neri, A. Distinct LncRNA Transcriptional Fingerprints Characterize Progressive Stages of Multiple Myeloma. Oncotarget 2016, 7, 14814–14830. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lionetti, M.; Barbieri, M.; Manzoni, M.; Fabris, S.; Bandini, C.; Todoerti, K.; Nozza, F.; Rossi, D.; Musto, P.; Baldini, L.; et al. Molecular Spectrum of TP53 Mutations in Plasma Cell Dyscrasias by next Generation Sequencing: An Italian Cohort Study and Overview of the Literature. Oncotarget 2016, 7, 21353–21361. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Todoerti, K.; Calice, G.; Trino, S.; Simeon, V.; Lionetti, M.; Manzoni, M.; Fabris, S.; Barbieri, M.; Pompa, A.; Baldini, L.; et al. Global Methylation Patterns in Primary Plasma Cell Leukemia. Leuk. Res. 2018, 73, 95–102. [Google Scholar] [CrossRef]
- Rojas, E.A.; Corchete, L.A.; Mateos, M.V.; García-Sanz, R.; Misiewicz-Krzeminska, I.; Gutiérrez, N.C. Transcriptome Analysis Reveals Significant Differences between Primary Plasma Cell Leukemia and Multiple Myeloma Even When Sharing a Similar Genetic Background. Blood Cancer J. 2019, 9, 90. [Google Scholar] [CrossRef] [PubMed]
- Yu, T.; Xu, Y.; An, G.; Tai, Y.-T.; Ho, M.; Li, Z.; Deng, S.; Zou, D.; Yu, Z.; Hao, M.; et al. Primary Plasma Cell Leukemia: Real-World Retrospective Study of 46 Patients From a Single-Center Study in China. Clin. Lymphoma Myeloma Leuk. 2020, 20, e652–e659. [Google Scholar] [CrossRef] [PubMed]
- Schinke, C.; Boyle, E.M.; Ashby, C.; Wang, Y.; Lyzogubov, V.; Wardell, C.; Qu, P.; Hoering, A.; Deshpande, S.; Ryan, K.; et al. Genomic Analysis of Primary Plasma Cell Leukemia Reveals Complex Structural Alterations and High-Risk Mutational Patterns. Blood Cancer J. 2020, 10, 70. [Google Scholar] [CrossRef] [PubMed]
- Nandakumar, B.; Kumar, S.K.; Dispenzieri, A.; Buadi, F.K.; Dingli, D.; Lacy, M.Q.; Hayman, S.R.; Kapoor, P.; Leung, N.; Fonder, A.; et al. Clinical Characteristics and Outcomes of Patients With Primary Plasma Cell Leukemia in the Era of Novel Agent Therapy. Mayo Clin. Proc. 2021, 96, 677–687. [Google Scholar] [CrossRef]
- Todoerti, K.; Taiana, E.; Puccio, N.; Favasuli, V.; Lionetti, M.; Silvestris, I.; Gentile, M.; Musto, P.; Morabito, F.; Gianelli, U.; et al. Transcriptomic Analysis in Multiple Myeloma and Primary Plasma Cell Leukemia with t(11;14) Reveals Different Expression Patterns with Biological Implications in Venetoclax Sensitivity. Cancers (Basel) 2021, 13, 4898. [Google Scholar] [CrossRef]
- Bútová, R.; Vychytilová-Faltejsková, P.; Gregorová, J.; Radová, L.; Almáši, M.; Bezděková, R.; Brožová, L.; Jarkovský, J.; Knechtová, Z.; Štork, M.; et al. LncRNAs LY86-AS1 and VIM-AS1 Distinguish Plasma Cell Leukemia Patients from Multiple Myeloma Patients. Biomedicines 2021, 9, 1637. [Google Scholar] [CrossRef]
- Papadhimitriou, S.I.; Terpos, E.; Liapis, K.; Pavlidis, D.; Marinakis, T.; Kastritis, E.; Dimopoulos, M.-A.; Tsitsilonis, O.E.; Kostopoulos, I.V. The Cytogenetic Profile of Primary and Secondary Plasma Cell Leukemia: Etiopathogenetic Perspectives, Prognostic Impact and Clinical Relevance to Newly Diagnosed Multiple Myeloma with Differential Circulating Clonal Plasma Cells. Biomedicines 2022, 10, 209. [Google Scholar] [CrossRef]
- Cazaubiel, T.; Buisson, L.; Maheo, S.; Do Souto Ferreira, L.; Lannes, R.; Perrot, A.; Hulin, C.; Avet-Loiseau, H.; Corre, J. The Genomic and Transcriptomic Landscape of Plasma Cell Leukemia. Blood 2020, 136, 48–49. [Google Scholar] [CrossRef]
- Cazaubiel, T.; Leleu, X.; Perrot, A.; Manier, S.; Buisson, L.; Mahéo, S.; Do Souto Ferreira, L.; Lannes, R.; Pavageau, L.; Hulin, C.; et al. Primary Plasma Cell Leukemia Displaying t(11;14) Have Specific Genomic, Transcriptional and Clinical Feature. Blood 2021, in press. [Google Scholar] [CrossRef] [PubMed]
- Hanamura, I.; Stewart, J.P.; Huang, Y.; Zhan, F.; Santra, M.; Sawyer, J.R.; Hollmig, K.; Zangarri, M.; Pineda-Roman, M.; van Rhee, F.; et al. Frequent Gain of Chromosome Band 1q21 in Plasma-Cell Dyscrasias Detected by Fluorescence in Situ Hybridization: Incidence Increases from MGUS to Relapsed Myeloma and Is Related to Prognosis and Disease Progression Following Tandem Stem-Cell Transplantation. Blood 2006, 108, 1724–1732. [Google Scholar] [CrossRef]
- Hanamura, I. Gain/Amplification of Chromosome Arm 1q21 in Multiple Myeloma. Cancers (Basel) 2021, 13, 256. [Google Scholar] [CrossRef]
- Chang, H.; Qi, X.; Jiang, A.; Xu, W.; Young, T.; Reece, D. 1p21 Deletions Are Strongly Associated with 1q21 Gains and Are an Independent Adverse Prognostic Factor for the Outcome of High-Dose Chemotherapy in Patients with Multiple Myeloma. Bone Marrow Transpl. 2010, 45, 117–121. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chang, H.; Qi, C.; Jiang, A.; Xu, W.; Trieu, Y.; Reece, D.E. Loss of Chromosome 1p21 Band Is Associated with Disease Progression and Poor Survival in Multiple Myeloma Patients Undergoing Autologous Stem Cell Transplantation. Blood 2008, 112, 1702. [Google Scholar] [CrossRef]
- Rajkumar, S.V.; Dimopoulos, M.A.; Palumbo, A.; Blade, J.; Merlini, G.; Mateos, M.-V.; Kumar, S.; Hillengass, J.; Kastritis, E.; Richardson, P.; et al. International Myeloma Working Group Updated Criteria for the Diagnosis of Multiple Myeloma. Lancet Oncol. 2014, 15, e538–e548. [Google Scholar] [CrossRef]
- Avet-Loiseau, H.; Gerson, F.; Magrangeas, F.; Minvielle, S.; Harousseau, J.L.; Bataille, R. Intergroupe Francophone du Myélome Rearrangements of the C-Myc Oncogene Are Present in 15% of Primary Human Multiple Myeloma Tumors. Blood 2001, 98, 3082–3086. [Google Scholar] [CrossRef] [Green Version]
- Jonveaux, P.; Berger, R. Chromosome Studies in Plasma Cell Leukemia and Multiple Myeloma in Transformation. Genes Chromosomes Cancer 1992, 4, 321–325. [Google Scholar] [CrossRef]
- Dimopoulos, M.A.; Palumbo, A.; Delasalle, K.B.; Alexanian, R. Primary Plasma Cell Leukaemia. Br. J. Haematol. 1994, 88, 754–759. [Google Scholar] [CrossRef]
- Andersen, M.N.; Abildgaard, N.; Maniecki, M.B.; Møller, H.J.; Andersen, N.F. Monocyte/Macrophage-Derived Soluble CD163: A Novel Biomarker in Multiple Myeloma. Eur. J. Haematol. 2014, 93, 41–47. [Google Scholar] [CrossRef] [PubMed]
- Terpos, E.; Migkou, M.; Christoulas, D.; Gavriatopoulou, M.; Eleutherakis-Papaiakovou, E.; Kanellias, N.; Iakovaki, M.; Panagiotidis, I.; Ziogas, D.C.; Fotiou, D.; et al. Increased Circulating VCAM-1 Correlates with Advanced Disease and Poor Survival in Patients with Multiple Myeloma: Reduction by Post-Bortezomib and Lenalidomide Treatment. Blood Cancer J. 2016, 6, e428. [Google Scholar] [CrossRef] [PubMed]
- Kryukov, F.; Dementyeva, E.; Kubiczkova, L.; Jarkovsky, J.; Brozova, L.; Petrik, J.; Nemec, P.; Sevcikova, S.; Minarik, J.; Stefanikova, Z.; et al. Cell Cycle Genes Co-Expression in Multiple Myeloma and Plasma Cell Leukemia. Genomics 2013, 102, 243–249. [Google Scholar] [CrossRef] [PubMed]
- Chen, D.; Yang, X.; Liu, M.; Zhang, Z.; Xing, E. Roles of MiRNA Dysregulation in the Pathogenesis of Multiple Myeloma. Cancer Gene Ther. 2021, 28, 1256–1268. [Google Scholar] [CrossRef] [PubMed]
- Carrasco-Leon, A.; Ezponda, T.; Meydan, C.; Valcárcel, L.V.; Ordoñez, R.; Kulis, M.; Garate, L.; Miranda, E.; Segura, V.; Guruceaga, E.; et al. Characterization of Complete LncRNAs Transcriptome Reveals the Functional and Clinical Impact of LncRNAs in Multiple Myeloma. Leukemia 2021, 35, 1438–1450. [Google Scholar] [CrossRef]
- Misiewicz-Krzeminska, I.; Krzeminski, P.; Corchete, L.A.; Quwaider, D.; Rojas, E.A.; Herrero, A.B.; Gutiérrez, N.C. Factors Regulating MicroRNA Expression and Function in Multiple Myeloma. Noncoding RNA 2019, 5, 9. [Google Scholar] [CrossRef] [Green Version]
- De Veirman, K.; Wang, J.; Xu, S.; Leleu, X.; Himpe, E.; Maes, K.; De Bruyne, E.; Van Valckenborgh, E.; Vanderkerken, K.; Menu, E.; et al. Induction of MiR-146a by Multiple Myeloma Cells in Mesenchymal Stromal Cells Stimulates Their pro-Tumoral Activity. Cancer Lett. 2016, 377, 17–24. [Google Scholar] [CrossRef]
- Statello, L.; Guo, C.-J.; Chen, L.-L.; Huarte, M. Gene Regulation by Long Non-Coding RNAs and Its Biological Functions. Nat. Rev. Mol. Cell Biol. 2021, 22, 96–118. [Google Scholar] [CrossRef]
- Walker, B.A.; Wardell, C.P.; Chiecchio, L.; Smith, E.M.; Boyd, K.D.; Neri, A.; Davies, F.E.; Ross, F.M.; Morgan, G.J. Aberrant Global Methylation Patterns Affect the Molecular Pathogenesis and Prognosis of Multiple Myeloma. Blood 2011, 117, 553–562. [Google Scholar] [CrossRef]
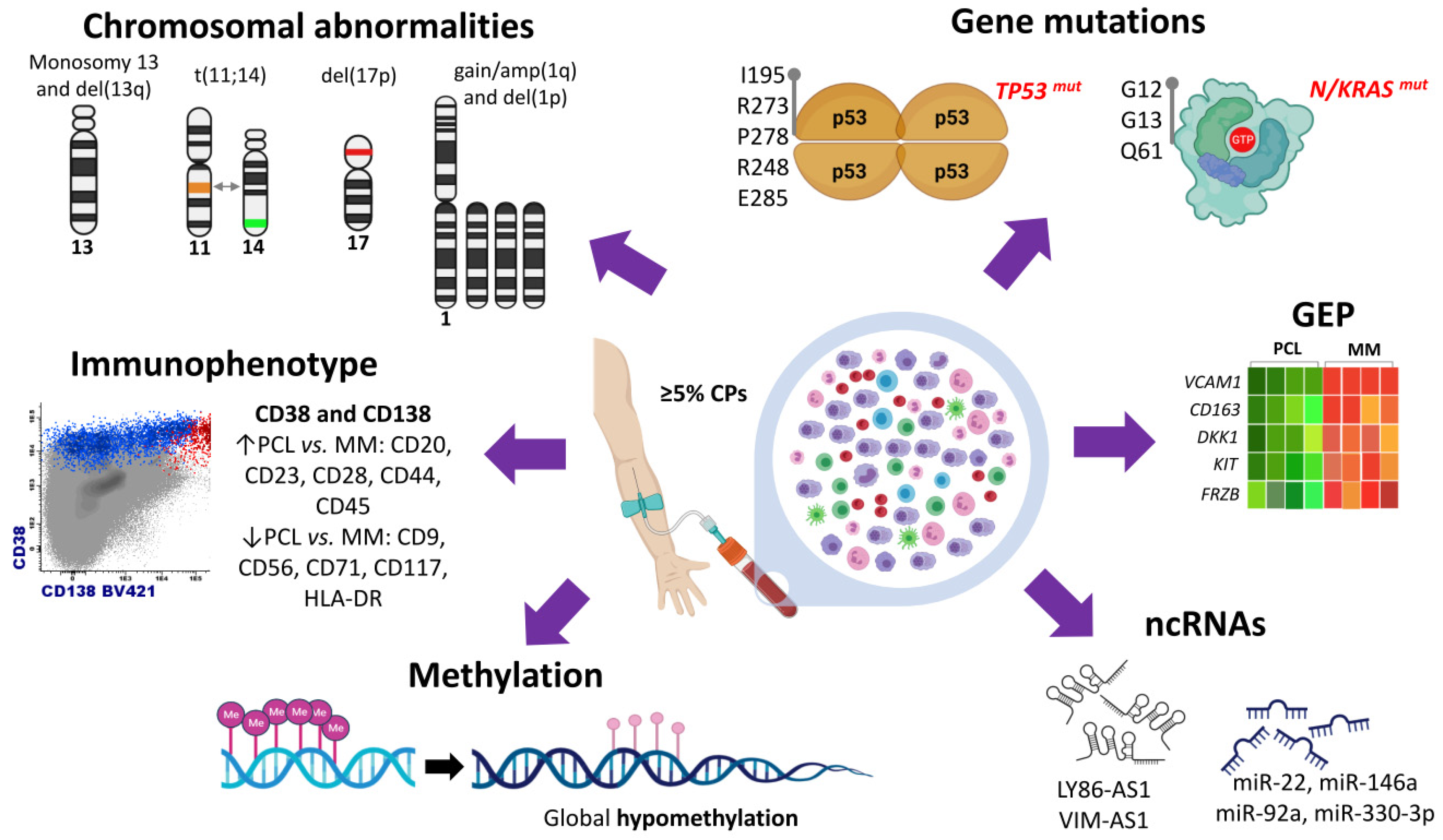
Figure 1.
Genomic abnormalities of primary plasma cell leukemia (pPCL). The updated consensus of the IMWG defines pPCL by the presence of 5% or more circulating plasma cells in peripheral blood. Cytogenetic studies by FISH show predominance of monosomy and deletions of chromosome 13, t(11;14), del(17p), gain/amp(1q) and del(1p). Mutation studies by conventional DNA sequencing, WES, and targeted NGS detect a high frequency of mutations in TP53 and K/NRAS genes. The amino acids most frequently mutated in TP53 are I195, R273, P278, R248, and E285. Activating mutations of K/NRAS most frequently found in pPCL patients affect codons 12, 13, and 61 (G12, G13, and Q61). Immunophenotyping of plasma cells reveals expression of CD38 and CD138 in both pPCL and MM, although higher expression of CD20, CD23, CD28, CD44, and CD45 and lower expression of CD9, CD56, CD71, CD117, and HLA-DR may be found in pPCL compared to MM. Gene expression profiling in pPCL has shown downregulation of genes associated with bone marrow microenvironment and bone diseases in MM, such as DKK1, KIT, and NCAM1 genes. A global hypomethylation profile has been found in pPCL samples. Non-coding RNAs (miRNAs and lncRNAs) are dysregulated in pPCL, and some of them are associated with survival of patients (as shown in the figure).
Figure 1.
Genomic abnormalities of primary plasma cell leukemia (pPCL). The updated consensus of the IMWG defines pPCL by the presence of 5% or more circulating plasma cells in peripheral blood. Cytogenetic studies by FISH show predominance of monosomy and deletions of chromosome 13, t(11;14), del(17p), gain/amp(1q) and del(1p). Mutation studies by conventional DNA sequencing, WES, and targeted NGS detect a high frequency of mutations in TP53 and K/NRAS genes. The amino acids most frequently mutated in TP53 are I195, R273, P278, R248, and E285. Activating mutations of K/NRAS most frequently found in pPCL patients affect codons 12, 13, and 61 (G12, G13, and Q61). Immunophenotyping of plasma cells reveals expression of CD38 and CD138 in both pPCL and MM, although higher expression of CD20, CD23, CD28, CD44, and CD45 and lower expression of CD9, CD56, CD71, CD117, and HLA-DR may be found in pPCL compared to MM. Gene expression profiling in pPCL has shown downregulation of genes associated with bone marrow microenvironment and bone diseases in MM, such as DKK1, KIT, and NCAM1 genes. A global hypomethylation profile has been found in pPCL samples. Non-coding RNAs (miRNAs and lncRNAs) are dysregulated in pPCL, and some of them are associated with survival of patients (as shown in the figure).


{kind=link}
Table 1.
Summary of the most relevant genomic studies carried out in PCL.
| Study/Reference | Number of Patients | Methodologies | Summary of Results * |
|---|---|---|---|
| Avet-Loiseau et al., 1998 [17] | 14 pPCL/127 MM | FISH | IGH translocations in 71% pPCL. |
| García-Sanz et al., 1999 [14] | 26 pPCL/664 MM | Cell DNA content, immunophenotypic studies, FISH | Numeric abnormalities in 92% pPCL. DNA content: diploid in 85% pPCL. |
| Avet-Loiseau et al., 2001 [18] | 40 pPCL/247 MM | FISH, conventional karyotyping | Higher proportion of t(11;14), t(14;16), and hypodiploid karyotype in pPCL. |
| Gutiérrez et al., 2001 [19] | 5 pPCL/25 MM | CGH | Losses of chromosomal material significantly more frequent in pPCL. |
| Bezieau et al., 2001 [20] | 10 pPCL/3 sPCL/33 MM/6 MGUS/2 SMM/11 MM at relapse | Allele-specific PCR amplification and K/NRAS direct sequencing | K/NRAS mutations in 55% MM at diagnosis, 81% MM at relapse, and 50% pPCL. KRAS mutations were always more frequent than NRAS. |
| Avet-Loiseauet al., 2002 [21] | 46 pPCL/147 MGUS/39 SMM/669 MM | FISH | Higher proportion of t(11;14), t(14;16), and 13q deletions in pPCL. |
| Tiedemann et al., 2008 [8] | 41 pPCL/39 sPCL/439 MM | FISH, conventional karyotyping, methylation-sensitive PCR, TP53, and N/K-RAS DNA sequencing | t(11;14) significantly more frequent in pPCL than in sPCL. High proportion of del(17p), TP53 mutation, and biallelic inactivation in pPCL and sPCL. |
| Chang et al., 2009 [22] | 15 pPCL/26 sPCL/220 MM | cIg-FISH, FISH | del(13q), del (17p), t(4;14), 1q21 amplification and del(1p21) significantly more common in PCL than in MM. t(4;14) and del(1p21) associated with shorter OS. In multivariant analysis, t(4;14) remained a significant predictor for adverse OS in PCL. |
| Chiecchio et al., 2009 [23] | 10 pPCL/2 sPCL/861 MM | FISH, conventional karyotyping, aCGH, qRT-PCR | t(11;14) and t(14;16) significantly more frequent in PCL. Structural and numerical abnormalities frequently involve 8q24. MYC upregulation in PCL. |
| Paganoet al., 2011 [24] | 73 pPCL (41 FISH), 53 sPCL | Conventional karyotyping (n = 28), FISH (n = 23) | Unfavorable cytogenetics: 56%. |
| Usmani et al., 2012 [25] | 13 pPCL/19 sPCL/1018 MM | GEP, FISH | GEP analyses distinguished pPCL from MM based on 203 gene probes. |
| Lionetti et al., 2013 [26] | 18 pPCL | FISH, GEP, SNP arrays, miRNA microarrays | 83 deregulated miRNAs in pPCL compared to MM. Expression levels of miR-497, miR-106b, miR-181a, and miR-181b correlated with treatment response, and of miR-92a, miR-330-3p, miR-22, and miR-146a correlated with clinical outcome. |
| Mosca et al., 2013 [27] | 23 pPCL | FISH, SNP array, and GEP | Predominance of t(11;14) (40%) and t(14;16) (30%) Absence of activating mutations of N/KRAS in pPCL. GEP analysis revealed deregulated genes involved in metabolic processes. |
| Todoerti et al., 2013 [28] | 21 pPCL/55 MM | GEP | 503-gene transcriptional signature distinguishes pPCL from MM. Underexpression of YIPF6, EDEM3, and CYB5D2 associated with nonresponder pPCL. 27-gene model identifies pPCL patients with shorter OS. |
| Cifolaet al., 2015 [29] | 12 pPCL | WES | First study of mutational pattern in pPCL patients using WES. Identification of 14 candidate cancer driver genes, mainly involved in cell cycle, genome stability, RNA metabolism, and protein folding. |
| Lionetti et al., 2015 [30] | 24 pPCL/11 sPCL/132 MM | Targeted NGS for BRAF (exons 11 and 15), NRAS (exons 2 and 3) and KRAS (exons 2–4) | MAPK pathway affected in 42% pPCL, 64% sPCL, and 60% MM. BRAF mutations in 21% pPCL, 9% sPCL and 11% MM. |
| Ronchettiet al., 2016 [31] | 24 pPCL/12 sPCL/170 MM/33 SMM/20 MGUS/9 NPC | lncRNA expression profiling by arrays | 15 lncRNAs progressively increased, and six decreased from normal PCs to MGUS, SMM, MM, and PCL samples. |
| Lionetti et al., 2016 [32] | 12 pPCL/10 sPCL/129 MM | Targeted NGS for TP53 (exons 4–9) | TP53 mutations in 25% pPCL, 20% sPCL and 3% MM. del(17p) in 29% pPCL, 44% sPCL, and 5% MM. TP53 mutations and del(17p) are markers of progression. |
| Todoerti et al., 2018 [33] | 14 pPCL/60 MM/5 MGUS | Global methylation patterns by high-density arrays | Global hypomethylation profile in pPCL. Decreasing methylation levels from MGUS to MM and pPCL. |
| Rojas et al., 2019 [34] | 9 pPCL/ 10 MM | Transcriptome arrays | Different transcriptome profiles between pPCL and MM carrying del(17p). RNA splicing machinery was one of the most deregulated processes in pPCL. |
| Yu et al., 2020 [35] | 46 pPCL | Conventional karyotyping (n = 34) and FISH (n = 37) | Predominance of del(13q) (38%), 1q gains (30%), del(17p) (27%), and t(11;14) (24%). t(4;14): not found. |
| Schinke et al., 2020 [36] | 23 pPCL/1273 MM | FISH, WES, and GEP | Predominance of complex structural changes and high-risk mutational patterns in pPCL. Driver genes with more mutations in pPCL than in MM: KRAS, TP53, EGR1, LTB, PRDM1, EP300, NF1, PIK3CA, and ZFP36L1. |
| Nandakumar et al., 2021 [37] | 68 pPCL (defined by ≥5% of clonal circulating PC) | FISH (n = 58) | Predominance of t(11;14) (47%), del(17p) (28%) and t(14;16) (12%). |
| Todoerti et al., 2021 [38] | 15 pPCL/50 MM | GEP, FISH | Different transcriptome profiles between pPCL and MM carrying t(11;14). |
| Bútová et al., 2021 [39] | 12 pPCL/11 sPCL/34 MM | lncRNA expression profile by NGS. Validation with qRT-PCR | 13 deregulated lncRNAs between PCL and MM. Downregulation of LY86-AS1 and VIM-AS1 in PCL compared to MM. |
| Papadhimitriou et al., 2022 [40] | 25 pPCL/19 sPCL/965 MM | FISH and NGF | Distinct cytogenetic profile between pPCL and sPCL, predominantly more del(13q) (95%) and del(17p) (68%) in sPCL than in pPCL, but t(11;14) only detected in pPCL and MM cases, and significantly higher incidence of 8q24 rearrangements in pPCL (40%) compared to sPCL (26%) and MM (9%). |
| Cazaubiel et al., 2020 [41] and Cazaubiel et al., 2022 [42] | 96 pPCL/907 MM | Targeted NGS, RNA-seq, and FISH | TP53 and IRF4 mutations significantly more frequent in pPCL. Increased proportion of double hit profiles in pPCL. Different transcriptome profiles between pPCL with and without t(11;14). |
FISH—fluorescence in situ hybridization; CGH—comparative genomic hybridization; aCGH—comparative genome hybridization arrays; NGS—next-generation sequencing; WES—whole-exome sequencing; SNP—single nucleotide polymorphism; GEP—gene expression profiling by microarrays; cIg-FISH—Cytoplasm light chain immunofluorescence with simultaneous interphase fluorescence in situ hybridization; qRT-PCR—quantitative real-time PCR; OS—overall survival; NGF—next-generation flow cytometry. * Only results related to genetic/genomic alterations are summarized.
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Rojas, E.A.; Gutiérrez, N.C. Genomics of Plasma Cell Leukemia. Cancers 2022, 14, 1594. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers14061594
AMA Style
Rojas EA, Gutiérrez NC. Genomics of Plasma Cell Leukemia. Cancers. 2022; 14(6):1594. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers14061594
Chicago/Turabian StyleRojas, Elizabeta A., and Norma C. Gutiérrez. 2022. "Genomics of Plasma Cell Leukemia" Cancers 14, no. 6: 1594. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers14061594
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.