
Liquid Biopsies: Applications for Cancer Diagnosis and Monitoring

 , , , ,
, , , ,
Abstract
:1. Introduction
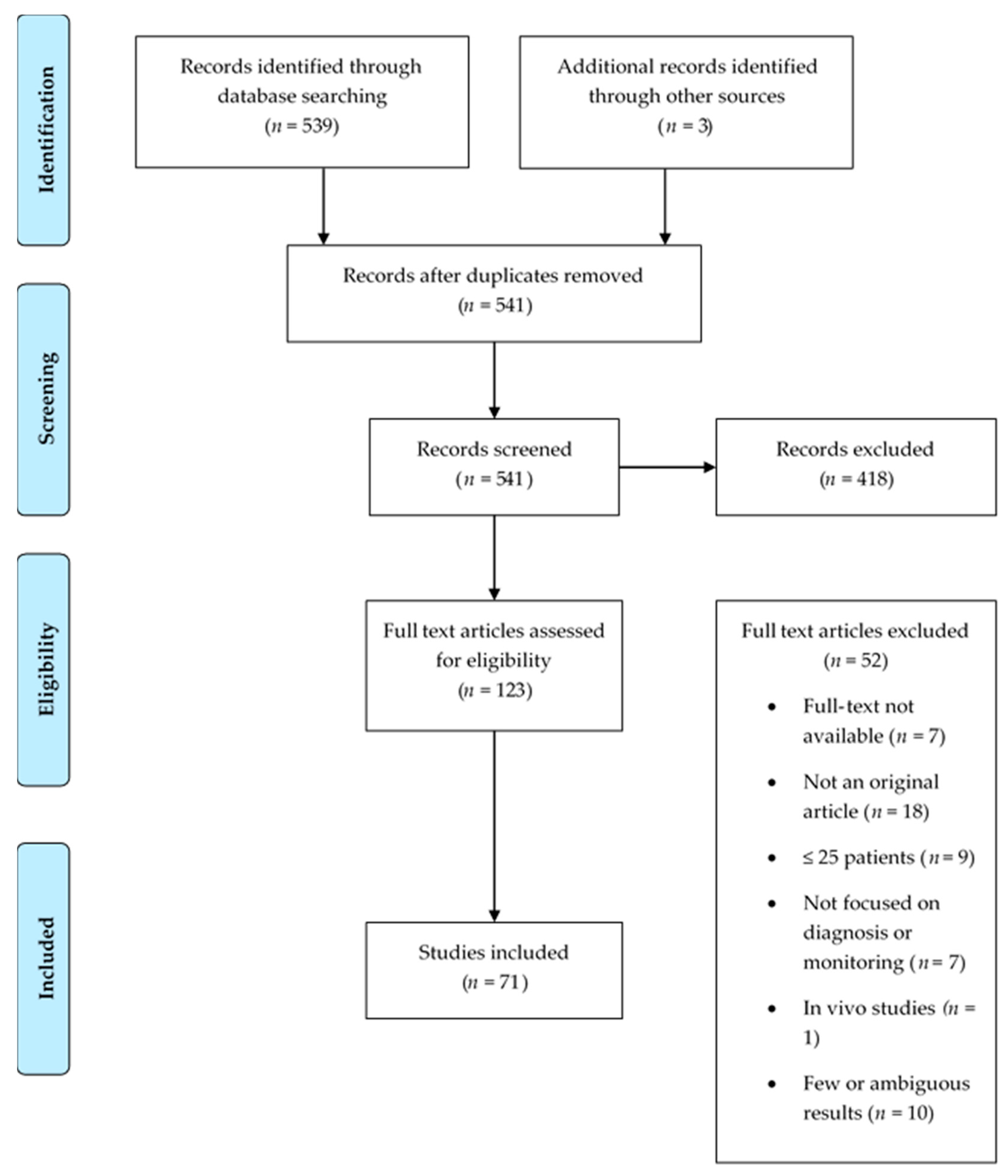
2. Materials and Methods
2.1. Search Strategy
2.2. Eligibility Criteria
3. Results
4. Discussion
4.1. Liquid Biopsies for Diagnosis and Tumor Profiling
4.2. Liquid Biopsies for the Follow-up of Cancer Patients
4.3. Liquid Biopsies in the Immuno-Oncology Field
4.4. Advantages and Disadvantages of Liquid Biopsies
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- The global challenge of cancer. Nat. Rev. Cancer 2020, 1, 1–2. [CrossRef] [Green Version]
- Mattox, A.K.; Bettegowda, C.; Zhou, S.; Papadopoulos, N.; Kinzler, K.W.; Vogelstein, B. Applications of liquid biopsies for cancer. Sci. Transl. Med. 2019, 11, eaay1984. [Google Scholar] [CrossRef] [Green Version]
- Thomsen, C.B.; Hansen, T.F.; Andersen, R.F.; Lindebjerg, J.; Jensen, L.H.; Jakobsen, A. Monitoring the effect of first line treatment in RAS/RAF mutated metastatic colorectal cancer by serial analysis of tumor specific DNA in plasma. J. Exp. Clin. Cancer Res. 2018, 37, 55. [Google Scholar] [CrossRef] [Green Version]
- Malczewska, A.; Oberg, K.; Bodei, L.; Aslanian, H.; Lewczuk, A.; Filosso, P.L.; Wójcik-Giertuga, M.; Rydel, M.; Zielińska-Leś, I.; Walter, A.; et al. NETest liquid biopsy is diagnostic of lung neuroendocrine tumors and identifies progressive disease. Neuroendocrinology 2019, 108, 219–231. [Google Scholar] [CrossRef] [PubMed]
- Aaltonen, K.E.; Novosadova, V.; Bendahl, P.-O.; Graffman, C.; Larsson, A.-M.; Rydén, L. Molecular characterization of circulating tumor cells from patients with metastatic breast cancer reflects evolutionary changes in gene expression under the pressure of systemic therapy. Oncotarget 2017, 8, 45544–45565. [Google Scholar] [CrossRef]
- Shoda, K.; Ichikawa, D.; Fujita, Y.; Masuda, K.; Hiramoto, H.; Hamada, J.; Arita, T.; Konishi, H.; Komatsu, S.; Shiozaki, A.; et al. Monitoring the HER2 copy number status in circulating tumor DNA by droplet digital PCR in patients with gastric cancer. Gastric Cancer 2016, 20, 126–135. [Google Scholar] [CrossRef] [Green Version]
- Xie, F.; Li, P.; Gong, J.; Tan, H.; Ma, J. Urinary cell-free DNA as a prognostic marker for KRAS-positive advanced-stage NSCLC. Clin. Transl. Oncol. 2018, 20, 591–598. [Google Scholar] [CrossRef] [PubMed]
- Qi, L.-N.; Xiang, B.-D.; Wu, F.-X.; Ye, J.-Z.; Zhong, J.-H.; Wang, Y.-Y.; Chen, Y.-Y.; Chen, Z.-S.; Ma, L.; Chen, J.; et al. Circulating tumor cells undergoing EMT provide a metric for diagnosis and prognosis of patients with hepatocellular carcinoma. Cancer Res. 2018, 78, 4731–4744. [Google Scholar] [CrossRef] [Green Version]
- Insua, Y.V.; De la Cámara, J.; Vázquez, E.B.; Fernández, A.; Rivera, F.V.; Silva, M.J.V.; Barbazán, J.; Muinelo-Romay, L.; Folgar, S.C.; Abalo, A.; et al. Predicting outcome and therapy response in mCRC patients using an indirect method for CTCs detection by a multigene expression panel: A multicentric prospective validation study. Int. J. Mol. Sci. 2017, 18, 1265. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Keup, C.; Mach, P.; Aktas, B.; Tewes, M.; Kolberg, H.-C.; Hauch, S.; Sprenger-Haussels, M.; Kimmig, R.; Kasimir-Bauer, S. RNA profiles of circulating tumor cells and extracellular vesicles for therapy stratification of metastatic breast cancer patients. Clin. Chem. 2018, 64, 1054–1062. [Google Scholar] [CrossRef]
- Gorges, T.M.; Riethdorf, S.; Von Ahsen, O.; Nastały, P.; Röck, K.; Boede, M.; Peine, S.; Kuske, A.; Schmid, E.; Kneip, C.; et al. Heterogeneous PSMA expression on circulating tumor cells—A potential basis for stratification and monitoring of PSMA-directed therapies in prostate cancer. Oncotarget 2016, 7, 34930–34941. [Google Scholar] [CrossRef] [Green Version]
- He, J.; Tan, W.; Ma, J. Circulating tumor cells and DNA for real-time EGFR detection and monitoring of non-small-cell lung cancer. Futur. Oncol. 2017, 13, 787–797. [Google Scholar] [CrossRef]
- Guibert, N.; Delaunay, M.; Lusque, A.; Boubekeur, N.; Rouquette, I.; Clermont, E.; Mourlanette, J.; Gouin, S.; Dormoy, I.; Favre, G.; et al. PD-L1 expression in circulating tumor cells of advanced non-small cell lung cancer patients treated with nivolumab. Lung Cancer 2018, 120, 108–112. [Google Scholar] [CrossRef]
- Hong, X.; Sullivan, R.J.; Kalinich, M.; Kwan, T.T.; Giobbie-Hurder, A.; Pan, S.; Licausi, J.A.; Milner, J.D.; Nieman, L.T.; Wittner, B.S.; et al. Molecular signatures of circulating melanoma cells for monitoring early response to immune checkpoint therapy. Proc. Natl. Acad. Sci. USA 2018, 115, 2467–2472. [Google Scholar] [CrossRef] [Green Version]
- Gao, W.; Huang, T.; Yuan, H.; Yang, J.; Jin, Q.; Jia, C.; Mao, G.; Zhao, J. Highly sensitive detection and mutational analysis of lung cancer circulating tumor cells using integrated combined immunomagnetic beads with a droplet digital PCR chip. Talanta 2018, 185, 229–236. [Google Scholar] [CrossRef]
- Mastoraki, S.; Strati, A.; Tzanikou, E.; Chimonidou, M.; Politaki, E.; Voutsina, A.; Psyrri, A.; Georgoulias, V.; Lianidou, E.S. ESR1 Methylation: A Liquid biopsy–based epigenetic assay for the follow-up of patients with metastatic breast cancer receiving endocrine treatment. Clin. Cancer Res. 2017, 24, 1500–1510. [Google Scholar] [CrossRef] [Green Version]
- Balaji, S.A.; Shanmugam, A.; Chougule, A.; Sridharan, S.; Prabhash, K.; Arya, A.; Chaubey, A.; Hariharan, A.; Kolekar, P.; Sen, M.; et al. Analysis of solid tumor mutation profiles in liquid biopsy. Cancer Med. 2018, 7, 5439–5447. [Google Scholar] [CrossRef]
- Yang, Y.-C.; Wang, D.; Jin, L.; Yao, H.-W.; Zhang, J.-H.; Wang, J.; Zhao, X.-M.; Shen, C.-Y.; Chen, W.; Wang, X.-L.; et al. Circulating tumor DNA detectable in early- and late-stage colorectal cancer patients. Biosci. Rep. 2018, 38. [Google Scholar] [CrossRef] [Green Version]
- Schwaederle, M.; Husain, H.; Fanta, P.T.; Piccioni, D.E.; Kesari, S.; Schwab, R.B.; Banks, K.C.; Lanman, R.B.; Talasaz, A.; Parker, B.A.; et al. Detection rate of actionable mutations in diverse cancers using a biopsy-free (blood) circulating tumor cell DNA assay. Oncotarget 2016, 7, 9707–9717. [Google Scholar] [CrossRef]
- Chung, T.K.; Cheung, T.H.; Yim, S.F.; Yu, M.Y.; Chiu, R.W.; Lo, K.W.; Lee, I.P.; Wong, R.R.; Lau, K.K.; Wang, V.W.; et al. Liquid biopsy of PIK3CA mutations in cervical cancer in Hong Kong Chinese women. Gynecol. Oncol. 2017, 146, 334–339. [Google Scholar] [CrossRef]
- Salvianti, F.; Giuliani, C.; Petrone, L.; Mancini, I.; Vezzosi, V.; Pupilli, C.; Pinzani, P. Integrity and quantity of total cell-free dna in the diagnosis of thyroid cancer: Correlation with cytological classification. Int. J. Mol. Sci. 2017, 18, 1350. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Braig, D.; Becherer, C.; Bickert, C.; Braig, M.; Claus, R.; Eisenhardt, A.E.; Heinz, J.; Scholber, J.; Herget, G.W.; Bronsert, P.; et al. Genotyping of circulating cell-free DNA enables noninvasive tumor detection in myxoid liposarcomas. Int. J. Cancer 2019, 145, 1148–1161. [Google Scholar] [CrossRef]
- Avogbe, P.H.; Manel, A.; Vian, E.; Durand, G.; Forey, N.; Voegele, C.; Zvereva, M.; Hosen, I.; Meziani, S.; De Tilly, B.; et al. Urinary TERT promoter mutations as non-invasive biomarkers for the comprehensive detection of urothelial cancer. EBioMedicine 2019, 44, 431–438. [Google Scholar] [CrossRef] [Green Version]
- Cote, G.J.; Evers, C.; Hu, M.I.; Grubbs, E.G.; Williams, M.D.; Hai, T.; Duose, D.Y.; Houston, M.R.; Bui, J.H.; Mehrotra, M.; et al. Prognostic significance of circulating RET M918T mutated tumor DNA in Patients with advanced medullary thyroid carcinoma. J. Clin. Endocrinol. Metab. 2017, 102, 3591–3599. [Google Scholar] [CrossRef]
- Shoda, K.; Masuda, K.; Ichikawa, D.; Arita, T.; Miyakami, Y.; Watanabe, M.; Konishi, H.; Imoto, I.; Otsuji, E. HER2 amplification detected in the circulating DNA of patients with gastric cancer: A retrospective pilot study. Gastric Cancer 2014, 18, 698–710. [Google Scholar] [CrossRef]
- Sinha, S.; Brown, H.; Tabak, J.; Fang, Z.; Du Tertre, M.C.; McNamara, S.; Gambaro, K.; Batist, G.; Buell, J.F. Multiplexed real-time polymerase chain reaction cell-free DNA assay as a potential method to monitor stage IV colorectal cancer. Surgery 2019, 166, 534–539. [Google Scholar] [CrossRef]
- Tian, J.; Geng, Y.; Lv, D.; Li, P.; Cordova, M.; Liao, Y.; Tian, X.; Zhang, X.; Zhang, Q.; Zou, K.; et al. Using plasma cell-free DNA to monitor the chemoradiotherapy course of cervical cancer. Int. J. Cancer 2019, 145, 2547–2557. [Google Scholar] [CrossRef]
- Wang, X.; Meng, Q.; Wang, C.; Li, F.; Zhu, Z.; Liu, S.; Shi, Y.; Huang, J.; Chen, S.; Li, C. Investigation of transrenal KRAS mutation in late stage NSCLC patients correlates to disease progression. Biomarkers 2016, 22, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Akamatsu, H.; Koh, Y.; Okamoto, I.; Fujimoto, D.; Bessho, A.; Azuma, K.; Morita, S.; Yamamoto, N.; Nakagawa, K. Clinical significance of monitoring EGFR mutation in plasma using multiplexed digital PCR in EGFR mutated patients treated with afatinib (West Japan Oncology Group 8114LTR study). Lung Cancer 2019, 131, 128–133. [Google Scholar] [CrossRef] [Green Version]
- Fernandez-Garcia, D.; Hills, A.; Page, K.; Hastings, R.K.; Toghill, B.; Goddard, K.S.; Ion, C.; Ogle, O.; Boydell, A.R.; Gleason, K.; et al. Plasma cell-free DNA (cfDNA) as a predictive and prognostic marker in patients with metastatic breast cancer. Breast Cancer Res. 2019, 21, 1–13. [Google Scholar] [CrossRef]
- Almodovar, K.; Iams, W.T.; Meador, C.B.; Zhao, Z.; York, S.; Horn, L.; Yan, Y.; Hernandez, J.; Chen, H.; Shyr, Y.; et al. Longitudinal Cell-Free DNA Analysis in patients with small cell lung cancer reveals dynamic insights into treatment efficacy and disease relapse. J. Thorac. Oncol. 2018, 13, 112–123. [Google Scholar] [CrossRef] [Green Version]
- Bernard, V.; Kim, D.U.; Lucas, F.A.S.; Castillo, J.; Allenson, K.; Mulu, F.C.; Stephens, B.M.; Huang, J.; Semaan, A.; Guerrero, P.A.; et al. Circulating nucleic acids are associated with outcomes of patients with pancreatic cancer. Gastroenterology 2019, 156, 108–118.e4. [Google Scholar] [CrossRef] [Green Version]
- Benešová, L.; Hálková, T.; Ptáčková, R.; Semyakina, A.; Menclová, K.; Pudil, J.; Ryska, M.; Levý, M.; Šimša, J.; Pazdírek, F.; et al. Significance of postoperative follow-up of patients with metastatic colorectal cancer using circulating tumor DNA. World J. Gastroenterol. 2019, 25, 6939–6948. [Google Scholar] [CrossRef]
- Kodahl, A.R.; Ehmsen, S.; Pallisgaard, N.; Jylling, A.M.B.; Jensen, J.D.; Laenkholm, A.-V.; Knoop, A.S.; Ditzel, H.J. Correlation between circulating cell-free PIK 3 CA tumor DNA levels and treatment response in patients with PIK 3 CA -mutated metastatic breast cancer. Mol. Oncol. 2018, 12, 925–935. [Google Scholar] [CrossRef] [Green Version]
- Schøler, L.V.; Reinert, T.; Ørntoft, M.-B.W.; Kassentoft, C.G.; Árnadóttir, S.S.; Vang, S.; Nordentoft, I.; Knudsen, M.; Lamy, P.; Andreasen, D.; et al. Clinical implications of monitoring circulating tumor DNA in patients with colorectal cancer. Clin. Cancer Res. 2017, 23, 5437–5445. [Google Scholar] [CrossRef] [Green Version]
- García-Saenz, J.A.; Ayllón, P.; Laig, M.; Acosta-Eyzaguirre, D.; García-Esquinas, M.; Montes, M.; Sanz, J.; Barquín, M.; Moreno, F.; Garcia-Barberan, V.; et al. Tumor burden monitoring using cell-free tumor DNA could be limited by tumor heterogeneity in advanced breast cancer and should be evaluated together with radiographic imaging. BMC Cancer 2017, 17, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Christensen, E.; Birkenkamp-Demtröder, K.; Nordentoft, I.; Høyer, S.; Van der Keur, K.; Van Kessel, K.; Zwarthoff, E.; Agerbæk, M.; Ørntoft, T.F.; Jensen, J.B.; et al. Liquid biopsy analysis of FGFR3 and PIK3CA hotspot mutations for disease surveillance in bladder cancer. Eur. Urol. 2017, 71, 961–969. [Google Scholar] [CrossRef]
- Lv, J.; Chen, Y.; Zhou, G.; Qi, Z.; Tan, K.R.L.; Wang, H.; Lin, L.; Chen, F.; Zhang, L.; Huang, X.; et al. Liquid biopsy tracking during sequential chemo-radiotherapy identifies distinct prognostic phenotypes in nasopharyngeal carcinoma. Nat. Commun. 2019, 10, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Song, T.; Mao, F.; Shi, L.; Xu, X.; Wu, Z.; Zhou, J.; Xiao, M. Urinary measurement of circulating tumor DNA for treatment monitoring and prognosis of metastatic colorectal cancer patients. Clin. Chem. Lab. Med. 2018, 57, 268–275. [Google Scholar] [CrossRef]
- Cheng, J.; Cao, Y.; MacLeay, A.; Lennerz, J.K.; Baig, A.; Frazier, R.P.; Lee, J.; Hu, K.; Pacula, M.; Meneses, E.; et al. Clinical validation of a Cell-Free DNA Gene Panel. J. Mol. Diagn. 2019, 21, 632–645. [Google Scholar] [CrossRef]
- Iwama, E.; Sakai, K.; Azuma, K.; Harada, T.; Harada, D.; Nosaki, K.; Hotta, K.; Ohyanagi, F.; Kurata, T.; Fukuhara, T.; et al. Monitoring of somatic mutations in circulating cell-free DNA by digital PCR and next-generation sequencing during afatinib treatment in patients with lung adenocarcinoma positive for EGFR activating mutations. Ann. Oncol. 2016, 28, 136–141. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.Y.; Qing, X.; Xiumin, W.; Yali, B.; Keunchil, P.; Bak, S.H.; Lee, H.Y.; Sun, J.-M.; Lee, S.-H.; Ahn, J.S.; et al. Longitudinal monitoring of EGFR mutations in plasma predicts outcomes of NSCLC patients treated with EGFR TKIs: Korean Lung cancer consortium (KLCC-12-02). Oncotarget 2016, 7, 6984–6993. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, D.-S.; Liu, Z.-X.; Lu, Y.-X.; Bao, H.; Wu, X.; Zeng, Z.-L.; Liu, Z.; Zhao, Q.; He, C.-Y.; Lu, J.-H.; et al. Liquid biopsies to track trastuzumab resistance in metastatic HER2-positive gastric cancer. Gut 2019, 68, 1152–1161. [Google Scholar] [CrossRef]
- Khan, K.H.; Cunningham, D.; Werner, B.; Vlachogiannis, G.; Spiteri, I.; Heide, T.; Mateos, J.F.; Vatsiou, A.; Lampis, A.; Damavandi, M.D.; et al. Longitudinal liquid biopsy and mathematical modeling of clonal evolution forecast time to treatment failure in the PROSPECT-C Phase II colorectal cancer clinical trial. Cancer Discov. 2018, 8, 1270–1285. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Iwama, E.; Sakai, K.; Hidaka, N.; Inoue, K.; Fujii, A.; Nakagaki, N.; Ota, K.; Toyozawa, R.; Azuma, K.; Nakatomi, K.; et al. Longitudinal monitoring of somatic genetic alterations in circulating cell-free DNA during treatment with epidermal growth factor receptor–tyrosine kinase inhibitors. Cancer 2020, 126, 219–227. [Google Scholar] [CrossRef]
- Bordi, P.; Del Re, M.; Minari, R.; Rofi, E.; Buti, S.; Restante, G.; Squadrilli, A.; Crucitta, S.; Casartelli, C.; Gnetti, L.; et al. From the beginning to resistance: Study of plasma monitoring and resistance mechanisms in a cohort of patients treated with osimertinib for advanced T790M-positive NSCLC. Lung Cancer 2019, 131, 78–85. [Google Scholar] [CrossRef]
- Chen, S.; Zhao, J.; Cui, L.; Liu, Y. Urinary circulating DNA detection for dynamic tracking of EGFR mutations for NSCLC patients treated with EGFR-TKIs. Clin. Transl. Oncol. 2016, 19, 332–340. [Google Scholar] [CrossRef]
- Egyud, M.; Tejani, M.; Pennathur, A.; Luketich, J.; Sridhar, P.; Yamada, E.; Ståhlberg, A.; Filges, S.; Krzyzanowski, P.; Jackson, J.; et al. Detection of circulating tumor DNA in Plasma: A potential biomarker for esophageal adenocarcinoma. Ann. Thorac. Surg. 2019, 108, 343–349. [Google Scholar] [CrossRef]
- Francaviglia, I.; Magliacane, G.; Lazzari, C.; Grassini, G.; Brunetto, E.; Cin, E.D.; Girlando, S.; Medicina, D.; Smart, C.E.; Bulotta, A.; et al. Identification and monitoring of somatic mutations in circulating cell-free tumor DNA in lung cancer patients. Lung Cancer 2019, 134, 225–232. [Google Scholar] [CrossRef]
- Vidal, J.; Muinelo, L.; Dalmases, A.; Jones, F.; Edelstein, D.; Iglesias, M.; Orrillo, M.; Abalo, A.; Rodríguez, C.; Brozos, E.; et al. Plasma ctDNA RAS mutation analysis for the diagnosis and treatment monitoring of metastatic colorectal cancer patients. Ann. Oncol. 2017, 28, 1325–1332. [Google Scholar] [CrossRef]
- Shoda, K.; Ichikawa, D.; Fujita, Y.; Masuda, K.; Hiramoto, H.; Hamada, J.; Arita, T.; Konishi, H.; Kosuga, T.; Komatsu, S.; et al. Clinical utility of circulating cell-free Epstein-Barr virus DNA in patients with gastric cancer. Oncotarget 2017, 8, 28796–28804. [Google Scholar] [CrossRef] [PubMed]
- Yu, H.; Han, L.; Yuan, J.; Sun, Y. Circulating tumor cell free DNA from plasma and urine in the clinical management of colorectal cancer. Cancer Biomark. 2019, 27, 29–37. [Google Scholar] [CrossRef] [PubMed]
- Bohers, E.; Viailly, P.-J.; Becker, S.; Marchand, V.; Ruminy, P.; Maingonnat, C.; Bertrand, P.; Etancelin, P.; Picquenot, J.-M.; Camus, V.; et al. Non-invasive monitoring of diffuse large B-cell lymphoma by cell-free DNA high-throughput targeted sequencing: Analysis of a prospective cohort. Blood Cancer J. 2018, 8, 1–13. [Google Scholar] [CrossRef] [Green Version]
- Pizzi, M.P.; Bartelli, T.F.; Pelosof, A.G.; Freitas, H.C.; Begnami, M.D.; De Abrantes, L.L.S.; Sztokfisz, C.; Valieris, R.; Knebel, F.H.; Coelho, L.G.V.; et al. Identification of DNA mutations in gastric washes from gastric adenocarcinoma patients: Possible implications for liquid biopsies and patient follow-up. Int. J. Cancer 2019, 145, 1090–1098. [Google Scholar] [CrossRef] [PubMed]
- Herrmann, S.; Zhan, T.; Betge, J.; Rauscher, B.; Belle, S.; Gutting, T.; Schulte, N.; Jesenofsky, R.; Härtel, N.; Gaiser, T.; et al. Detection of mutational patterns in cell-free DNA of colorectal cancer by custom amplicon sequencing. Mol. Oncol. 2019, 13, 1669–1683. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jensen, T.J.; Goodman, A.M.; Kato, S.; Ellison, C.K.; Daniels, G.A.; Kim, L.; Nakashe, P.; McCarthy, E.; Mazloom, A.R.; McLennan, G.; et al. Genome-Wide sequencing of cell-free dna identifies copy-number alterations that can be used for monitoring response to immunotherapy in cancer patients. Mol. Cancer Ther. 2019, 18, 448–458. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xu, R.-H.; Wei, W.; Krawczyk, M.; Wang, W.; Luo, H.; Flagg, K.; Yi, S.; Shi, W.; Quan, Q.; Li, K.; et al. Circulating tumour DNA methylation markers for diagnosis and prognosis of hepatocellular carcinoma. Nat. Mater. 2017, 16, 1155–1161. [Google Scholar] [CrossRef] [PubMed]
- Cheng, T.H.; Jiang, P.; Teoh, J.Y.; Heung, M.M.; Tam, J.C.; Sun, X.; Lee, W.-S.; Ni, M.; Chan, R.C.; Ng, C.-F.; et al. Noninvasive detection of bladder cancer by shallow-depth genome-wide bisulfite sequencing of urinary cell-free dna for methylation and copy number profiling. Clin. Chem. 2019, 65, 927–936. [Google Scholar] [CrossRef] [PubMed]
- Barault, L.; Amatu, A.; Siravegna, G.; Ponzetti, A.; Moran, S.; Cassingena, A.; Mussolin, B.; Falcomatà, C.; Binder, A.M.; Cristiano, C.; et al. Discovery of methylated circulating DNA biomarkers for comprehensive non-invasive monitoring of treatment response in metastatic colorectal cancer. Gut 2017, 67, 1995–2005. [Google Scholar] [CrossRef] [PubMed]
- Miller, A.M.; Shah, R.H.; Pentsova, E.I.; Pourmaleki, M.; Briggs, S.; Distefano, N.; Zheng, Y.; Skakodub, A.; Mehta, S.A.; Campos, C.; et al. Tracking tumour evolution in glioma through liquid biopsies of cerebrospinal fluid. Nat. Cell Biol. 2019, 565, 654–658. [Google Scholar] [CrossRef]
- Endzeliņš, E.; Berger, A.; Melne, V.; Bajo-Santos, C.; Soboļevska, K.; Ābols, A.; Rodriguez, M.; Šantare, D.; Rudņickiha, A.; Lietuvietis, V.; et al. Detection of circulating miRNAs: Comparative analysis of extracellular vesicle-incorporated miRNAs and cell-free miRNAs in whole plasma of prostate cancer patients. BMC Cancer 2017, 17, 1–13. [Google Scholar] [CrossRef]
- Malentacchi, F.; Vinci, S.; Della Melina, A.; Kuncová, J.; Villari, D.; Nesi, G.; Selli, C.; Orlando, C.; Pazzagli, M.; Pinzani, P. Urinary carbonic anhydrase IX splicing messenger RNA variants in urogenital cancers. Urol. Oncol. Semin. Orig. Investig. 2016, 34, 292.e9–292.e16. [Google Scholar] [CrossRef]
- Zedan, A.H.; Hansen, T.F.; Assenholt, J.; Madsen, J.S.; Osther, P.J.S. Circulating miRNAs in localized/locally advanced prostate cancer patients after radical prostatectomy and radiotherapy. Prostate 2018, 79, 425–432. [Google Scholar] [CrossRef] [Green Version]
- Okajima, W.; Komatsu, S.; Ichikawa, D.; Miyamae, M.; Kawaguchi, T.; Hirajima, S.; Ohashi, T.; Imamura, T.; Kiuchi, J.; Arita, T.; et al. Circulating microRNA profiles in plasma: Identification of miR-224 as a novel diagnostic biomarker in hepatocellular carcinoma independent of hepatic function. Oncotarget 2016, 7, 53820–53836. [Google Scholar] [CrossRef] [Green Version]
- Sestini, S.; Boeri, M.; Marchiano, A.; Pelosi, G.; Galeone, C.; Verri, C.; Suatoni, P.; Sverzellati, N.; La Vecchia, C.; Sozzi, G.; et al. Circulating microRNA signature as liquid-biopsy to monitor lung cancer in low-dose computed tomography screening. Oncotarget 2015, 6, 32868–32877. [Google Scholar] [CrossRef] [Green Version]
- Willms, A.; Müller, C.; Julich, H.; Klein, N.; Schwab, R.; Güsgen, C.; Richardsen, I.; Schaaf, S.; Krawczyk, M.; Krawczyk, M.; et al. Tumour-associated circulating microparticles: A novel liquid biopsy tool for screening and therapy monitoring of colorectal carcinoma and other epithelial neoplasia. Oncotarget 2016, 7, 30867–30875. [Google Scholar] [CrossRef] [Green Version]
- Ogle, L.F.; Orr, J.G.; Willoughby, C.E.; Hutton, C.; McPherson, S.; Plummer, R.; Boddy, A.V.; Curtin, N.J.; Jamieson, D.; Reeves, H.L. Imagestream detection and characterisation of circulating tumour cells—A liquid biopsy for hepatocellular carcinoma? J. Hepatol. 2016, 65, 305–313. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Von Felden, J.; Garcia-Lezana, T.; Schulze, K.; Losic, B.; Villanueva, A. Liquid biopsy in the clinical management of hepatocellular carcinoma. Gut 2020, 69, 2025–2034. [Google Scholar] [CrossRef]
- Ou, S.-H.I.; Nagasaka, M.; Zhu, V.W. Liquid biopsy to identify actionable genomic alterations. Am. Soc. Clin. Oncol. Educ. Book 2018, 38, 978–997. [Google Scholar] [CrossRef]
- Roy, D.; Tiirikainen, M. Diagnostic power of DNA methylation classifiers for early detection of cancer. Trends Cancer 2020, 6, 78–81. [Google Scholar] [CrossRef]
- Roy, D.; Taggart, D.; Zheng, L.; Liu, D.; Li, G.; Li, M.; Zhang, K.; Van Etten, R.A. Abstract 837: Circulating cell-free DNA methylation assay: Towards early detection of multiple cancer types. Mol. Cell. Biol. 2019, 79, 837. [Google Scholar] [CrossRef]
- Zhou, B.; Xu, K.; Zheng, X.; Chen, T.; Wang, J.; Song, Y.; Shao, Y.; Zheng, S. Application of exosomes as liquid biopsy in clinical diagnosis. Signal Transduct. Target. Ther. 2020, 5, 1–14. [Google Scholar] [CrossRef]
- Boffa, D.J.; Graf, R.P.; Salazar, M.C.; Hoag, J.; Lu, D.; Krupa, R.; Louw, J.; Dugan, L.; Wang, Y.; Landers, M.; et al. Cellular expression of PD-L1 in the peripheral blood of lung cancer patients is associated with worse survival. Cancer Epidemiol. Biomark. Prev. 2017, 26, 1139–1145. [Google Scholar] [CrossRef] [Green Version]
- Grimm, M.; Kraut, W.; Hoefert, S.; Krimmel, M.; Biegner, T.; Teriete, P.; Cetindis, M.; Polligkeit, J.; Kluba, S.; Munz, A.; et al. Evaluation of a biomarker based blood test for monitoring surgical resection of oral squamous cell carcinomas. Clin. Oral Investig. 2015, 20, 329–338. [Google Scholar] [CrossRef] [PubMed]
- Girotti, M.R.; Gremel, G.; Lee, R.; Galvani, E.; Rothwell, D.; Viros, A.; Mandal, A.K.; Lim, K.H.J.; Saturno, G.; Furney, S.J.; et al. Application of sequencing, liquid biopsies, and patient-derived xenografts for personalized medicine in melanoma. Cancer Discov. 2016, 6, 286–299. [Google Scholar] [CrossRef] [Green Version]
- Tjon-Kon-Fat, L.-A.; Lundholm, M.; Schröder, M.; Wurdinger, T.; Thellenberg-Karlsson, C.; Widmark, A.; Wikström, P.; Nilsson, R.J.A. Platelets harbor prostate cancer biomarkers and the ability to predict therapeutic response to abiraterone in castration resistant patients. Prostate 2018, 78, 48–53. [Google Scholar] [CrossRef] [PubMed]
- Xue, L.; Xie, L.; Song, X.; Song, X. Identification of potential tumor-educated platelets RNA biomarkers in non-small-cell lung cancer by integrated bioinformatical analysis. J. Clin. Lab. Anal. 2018, 32, e22450. [Google Scholar] [CrossRef] [PubMed]
- Mantini, G.; Meijer, L.L.; Glogovitis, I.; In‘t Veld, S.G.; Paleckyte, R.; Capula, M.; Le Large, T.; Morelli, L.; Pham, T.V.; Piersma, S.R.; et al. Tumor-educated platelet RNA for the detection and (Pseudo)progression monitoring of glioblastoma. Cell Rep. Med. 2020, 1, 100101. [Google Scholar] [CrossRef]
- Pisetsky, D.S.; Fairhurst, A.-M. The origin of extracellular DNA during the clearance of dead and dying cells. Autoimmunity 2007, 40, 281–284. [Google Scholar] [CrossRef] [PubMed]
- U.S. Food and Drug Administration. Cobas EGFR Mutation Test v2. Available online: https://www.fda.gov/drugs/resources-information-approved-drugs/cobas-egfr-mutation-test-v2 (accessed on 31 January 2021).
- U.S. Food and Drug Administration. FDA Approves Liquid Biopsy Next-Generation Sequencing Companion Diagnostic Test. Available online: https://www.fda.gov/drugs/drug-approvals-and-databases/fda-approves-liquid-biopsy-next-generation-sequencing-companion-diagnostic-test (accessed on 31 January 2021).
- Lamb, Y.N.; Dhillon, S. Epi proColon® 2.0 CE: A blood-based screening test for colorectal cancer. Mol. Diagn. Ther. 2017, 21, 225–232. [Google Scholar] [CrossRef]
- Sheridan, C. Investors keep the faith in cancer liquid biopsies. Nat. Biotechnol. 2019, 37, 972–974. [Google Scholar] [CrossRef]
- Poulet, G.; Massias, J.; Taly, V. Liquid biopsy: General concepts. Acta Cytol. 2019, 63, 449–455. [Google Scholar] [CrossRef]
- Thierry, A.R.; El Messaoudi, S.; Gahan, P.B.; Anker, P.; Stroun, M. Origins, structures, and functions of circulating DNA in oncology. Cancer Metastasis Rev. 2016, 35, 347–376. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lo, Y.M.D.; Zhang, J.; Leung, T.N.; Lau, T.K.; Chang, A.M.; Hjelm, N.M. Rapid clearance of fetal DNA from maternal plasma. Am. J. Hum. Genet. 1999, 64, 218–224. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yao, W.; Mei, C.; Nan, X.; Hui, L. Evaluation and comparison of in vitro degradation kinetics of DNA in serum, urine and saliva: A qualitative study. Gene 2016, 590, 142–148. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.; Ju, S.; Wang, X.; Cong, H. Advances in liquid biopsy using circulating tumor cells and circulating cell-free tumor DNA for detection and monitoring of breast cancer. Clin. Exp. Med. 2019, 19, 271–279. [Google Scholar] [CrossRef]
- Yan, W.-T.; Cui, X.; Chen, Q.; Li, Y.-F.; Cui, Y.-H.; Wang, Y.; Jiang, J. Circulating tumor cell status monitors the treatment responses in breast cancer patients: A meta-analysis. Sci. Rep. 2017, 7, srep43464. [Google Scholar] [CrossRef] [Green Version]
- Vogl, T.J.; Riegelbauer, L.J.; Oppermann, E.; Kostantin, M.; Ackermann, H.; Trzmiel, A.; Stein, S.; Eichler, K.; Zharov, V.P.; Roy, D.; et al. Early dynamic changes in circulating tumor cells and prognostic relevance following interventional radiological treatments in patients with hepatocellular carcinoma. PLoS ONE 2021, 16, e0246527. [Google Scholar] [CrossRef]
- Aceto, N. Fluctuating numbers of circulating tumor cells in cancer patients and the meaning of zero counts. Oncotarget 2019, 10, 2658–2659. [Google Scholar] [CrossRef]
- Ammerlaan, W.; Betsou, F. Biospecimen Science of Blood for cfDNA Genetic Analyses. Curr. Pathobiol. Rep. 2019, 7, 9–15. [Google Scholar] [CrossRef] [Green Version]
- Fernando, M.R.; Norton, S.E.; Luna, K.K.; Lechner, J.M.; Qin, J. Stabilization of cell-free RNA in blood samples using a new collection device. Clin. Biochem. 2012, 45, 1497–1502. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cohen, J.D.; Li, L.; Wang, Y.; Thoburn, C.; Afsari, B.; Danilova, L.; Douville, C.; Javed, A.A.; Wong, F.; Mattox, A.; et al. Detection and localization of surgically resectable cancers with a multi-analyte blood test. Science 2018, 359, 926–930. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khalaf, N.; Wolpin, B.M. Metabolic alterations as a signpost to early pancreatic cancer. Gastroenterology 2019, 156, 1560–1563. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cowling, T.; Loshak, H. An overview of liquid biopsy for screening and early detection of cancer. In CADTH Issues in Emerging Health Technologies; Canadian Agency for Drugs and Technologies in Health: Ottawa, ON, USA, 2016; pp. 1–13. [Google Scholar]


{kind=link}
| Author, Year (Trial Code, If Applicable) | Number of Patients and Type of Cancer | Type of Biofluid and Analyte | Main Findings |
|---|---|---|---|
| Schwaederle, M. et al., 2015 [19] | 171 patients, including lung (n = 40) and breast (n = 40) cancers, glioblastoma (n = 33), and others | Plasma circulating tumor DNA (ctDNA) | ctDNA alterations, most of which were potentially targetable by approved drugs, were detectable in 65% of various cancers and in 27% of glioblastomas. |
| Shoda, K. et al., 2015 [25] | 77 gastric cancer patients | Plasma ctDNA | HER2 amplification can be detected in plasma which might have utility in predicting treatment efficacy in gastric cancer. |
| Sestini, S et al., 2015 [65] | 84 lung cancer patients | Plasma micro-RNA (miRNA) | The studied 24 plasma miRNA signature seems to have utility as a prognostic and monitoring tool in lung cancer. |
| Girotti, M.R. et al., 2015 [75] | 214 melanoma patients | Blood circulating tumor cells (CTCs) and plasma ctDNA | Longitudinal ctDNA analysis can be used to monitor treatment response and to identify mechanisms of resistance in melanoma patients. CTC–derived xenografts can be used as a complement to improve personalized treatment selection. |
| Ogle, L.F. et al., 2016 [67] | 69 hepatocellular carcinoma (HCC) patients | Blood CTCs | Multiparametric analysis, using flow cytometry, size, morphology and the investigation of DNA improved the detection of CTCs, which have predictive potential in HCC. |
| Wang, X. et al., 20167 [28] | 200 non-small cell lung cancer (NSCLC) patients | Urine ctDNA | The KRAS mutational profile is highly concordant in urine and in corresponding tumor tissues. The longitudinal monitoring of mutations in transrenal DNA is helpful to stratify NSCLC patients according to predicted outcomes. |
| Okajima, W. et al., 2016 [64] | 107 HCC patients | Plasma miRNA | Plasma miRNA-224 could be a sensitive biomarker to screen, monitor, and evaluate treatment in HCC. |
| Grimm, M. et al., 2016 [74] | 92 oral squamous cell carcinoma (OSCC) patients | Blood Apo10 and transketolase like 1 (TKTL1) epitopes in monocytes | The significant decrease in epitope detection in monocytes (EDIM)-Apo10 and EDIM-TKTL1 scores after surgery suggest that these could be used as biomarkers to evaluate surgical resection and to monitor OSCC. |
| Malentacchi, F. et al., 2016 [62] | 138 patients, including bladder (n = 93) and renal (n = 25) cancers, and prostate adenocarcinoma (n = 25) | Urinary carbonic anhydrase IX (CAIX) messenger RNA (mRNA) | The relative percentage of the full-length isoform CAIX mRNA in urine sediments could be used as a surrogate marker of CAIX expression in tumor tissues for kidney, prostate and bladder cancer diagnosis. |
| Lee, J.Y. et al., 2016 [42] | 81 NSCLC patients | Plasma ctDNA | Analysis of EGFR mutations in plasma ctDNA is useful to monitor response and to promptly detect resistance in NSCLC patients treated with EGFR tyrosine kinase inhibitors (TKIs). |
| Gorges, T.M. et al., 2016 [11] | 29 metastatic prostate cancer (PCa) patients | Blood CTCs | The detection of prostate specific membrane antigen (PSMA)-expressing CTCs could identify PCa patients that might benefit from targeted therapies and allow their monitorization. |
| Willms, A. et al., 2016 [66] | 103 patients, including colorectal cancer (CRC) (n = 52), NSCLC (n = 40) and pancreas carcinoma (n = 11) | Serum tumor-associated microparticles (taMPS) | taMPs expressing epithelial cell adhesion molecule (EpCAM) and CD147 could be a promising biomarker for the diagnosis and monitoring of several neoplasias. |
| Endzeliņš, E. et al., 2017 [61] | 50 PCa patients | Plasma circulating miRNAs and extracellular vesicle (EV)-associated miRNAs | miRNA profiles recovered from whole plasma and plasma extracellular vesicles (EVs) of PCa patients are different and have distinct diagnostic value. |
| Salvianti, F. et al., 2017 [21] | 97 thyroid cancer patients | Plasma cell-free DNA (cfDNA) | The cfDNA integrity index [180/67 base pairs (bp)] is a promising biomarker for the diagnosis of thyroid carcinoma. |
| Xu, R-H. et al., 2017 [57] | 1098 HCC patients | Plasma ctDNA | ctDNA methylation markers have utility for diagnosis, prognosis, and monitoring of HCC. |
| Cote, G.J. et al., 2017 [24] | 75 medullary thyroid carcinoma patients | Plasma ctDNA | The detection of RET M918T mutations in plasma is highly specific but lacks sensitivity. The allelic fraction of ctDNA correlated with overall survival (OS) in thyroid carcinoma. |
| Insua, Y.V. et al., 2017 [9] | 94 metastatic colorectal cancer (mCRC) patients | Blood CTCs | The gene expression panel used to detect CTCs was able to assess early treatment response, with improved efficiency in comparison to computed tomography (CT) scans in mCRC patients. |
| Xie, F. et al., 2018 [7] | 150 NSCLC patients | Urine ctDNA | Urinary ctDNA informs about the tumor profile and serial monitoring could be used for prognosis of NSCLC. |
| Shoda, K. et al., 2017 [6] | 60 gastric cancer patients | Plasma ctDNA | The copy number status of HER2 is useful to monitor treatment efficacy in HER2(+) gastric cancer patients and to guide treatment decisions in patients showing a positive conversion of HER2 status with recurrence. |
| Schøler, L.V. et al., 2017 [35] | 45 CRC patients | Plasma ctDNA | Postoperative ctDNA is able to detect residual disease and early relapse in CRC. |
| Aaltonen, K.E. et al., 2017 [5] | 36 metastatic breast cancer (mBC) patients | Blood CTCs | Gene expression alterations in CTCs could be related with treatment resistance and the characterization of these cells over time could help in treatment selection in mBC. |
| Barault, L. et al., 2018 [59] | 182 mCRC patients | Plasma ctDNA | Methylation panels for ctDNA analysis can be used to monitor disease burden in mCRC patients. |
| Mastoraki, S. et al., 2018 [16] | 122 mBC patients | Blood CTCs and plasma ctDNA | ESR1 methylation status is highly concordant in CTCs and plasma ctDNA. ESR1 methylation in CTCs was associated with lack of response to treatment in mBC patients. |
| Tjon-Kon-Fat, L-A. et al., 2018 [76] | 50 castration resistant prostate cancer (CRPC) patients | Blood platelets | It is possible to find tumor-derived transcripts in platelets of CRPC patients that provide predictive information on treatment response and outcome. |
| Iwama, E. et al., 2017 [41] | 35 lung adenocarcinoma patients | Plasma ctDNA | ctDNA analysis using droplet digital Polymerase Chain Reaction (ddPCR) is useful to predict treatment efficacy, while Next Generation Sequencing (NGS) can inform about resistance mechanisms in adenocarcinoma patients treated with afatinib. |
| Chen, S. et al., 2017 [47] | 150 NSCLC patients | Urine ctDNA | Urinay cfDNA might be used as an alternative to tissue biopsies to determine EGFR status for diagnosis, prognosis and monitoring of NSCLC patients. |
| Shoda, K. et al., 2017 [51] | 153 gastric cancer patients | Plasma circulating cell-free Epstein-Barr virus (cfEBV) DNA | Plasma cfEBV DNA might be useful to detect Epstein-Barr virus-associated gastric carcinoma (EBVaGC) and to monitor treatment response or disease progression in real-time. |
| He, J. et al., 2017 [12] | 120 NSCLC patients | Blood CTCs and plasma ctDNA | CTCs and ctDNA capture the dynamic tumor profile during treatment and could complement current strategies for NSCLC management. |
| Chung, T.K.H. et al., 2017 [20] | 117 cervical cancer patients | Plasma cfDNA | PIK3CA analysis in liquid biopsies shows promise to help in risk stratification of cervical cancer patients and to make informed treatment decisions. |
| García-Saenz, J.A. et al., 2017 [36] | 49 breast cancer (BC) patients | Plasma ctDNA | Plasma ctDNA quantification has potential to monitor treatment outcomes, however, it might be limited by tumor heterogeneity and should be evaluated together with imaging data. |
Christensen, E. et al., 2017 [37] | 831 bladder cancer patients | Plasma and urine ctDNA | Monitoring FGFR3 and PIK3CA mutations in urine and plasma samples of bladder cancer patients might be useful to monitor disease progression and recurrence. |
| Vidal, J. et al., 2017 [50] | 115 mCRC patients | Plasma ctDNA | High concordance rates of RAS mutations in tumor tissue and ctDNA supports the use of liquid biopsies as a viable alternative to tissue biopsies for baseline diagnosis and to select candidates for anti-EGFR therapy. |
| Balaji, S.A. et al., 2018 [17] | 180 patients, including lung (n = 9), breast (n = 42), colorectal (n = 22) and other cancers | Plasma ctDNA | ctDNA is a reliable marker in a large number of cancers and seems to have prognostic value at baseline. |
| Yang, Y-C. et al., 2018 [18] | 47 CRC patients | Plasma ctDNA | Analysis of ctDNA provides additional clinical information regarding the tumor profile and could aid in early diagnosis and prognosis of CRC patients. |
| Qi, L-N. et al., 2018 [8] | 112 HCC patients | Blood CTCs | CTCs are markers for early diagnosis and predictors of early recurrence. Epithelial-to-mesenchymal transition (EMT) and CTC release seem to be related to the overexpression of BCAT1. |
| Keup, C. et al. 2018 [10] | 35 mBC patients | Blood CTCs and plasma EVs | EVs and CTCs display different mRNA profiles and might have potential to monitor therapy in mBC patients. |
| Almodovar, K. et al., 2018 [31] | 27 small-cell lung cancer (SCLC) patients | Plasma ctDNA | ctDNA is a useful tool to monitor disease during treatment and to detect relapse prior to conventional imaging in SCLC. |
| Kodahl, A.R. et al., 2018 [34] | 66 mBC patients | Serum ctDNA | The detection of PIK3CA mutations in tumor tissue and serum ctDNA is highly concordant. Detection of ctDNA PIK3CA mutations might complement imaging methods to follow treatment response in mBC. |
| Thomsen, C.B. et al. 2018 [3] | 138 mCRC patients | Plasma ctDNA | Changes in ctDNA levels are related to progression risk during first line chemotherapy in RAS/RAF mutated mCRC patients. |
| Song, T. et al., 2018 [39] | 150 mCRC patients | Urine cfDNA | There is a good concordance in DNA profiles of urine and tumor tissues. Monitoring total urine cfDNA levels could be used as a complement to mutation profiling, allowing to predict early treatment response and to identify mCRC patients at high risk. |
| Wang, D-S. et al., 2019 [43] | 78 gastric cancer patients | Plasma ctDNA | Longitudinal sequencing of ctDNA is useful to monitor treatment of HER2(+) gastric cancer patients and to detect alterations driving resistance. |
| Khan, K.H. et al., 2018 (NCT02994888) [44] | 47 CRC patients | Plasma ctDNA | cfDNA analysis is able to detect RAS pathway alterations in CRC patients that are classified as wildtype according to tumor tissues. Combining serial analysis of cfDNA and mathematical modeling allows to quantitatively predict the time needed for progression. |
| Bohers, E. et al., 2018 (NCT02339805) [53] | 30 diffuse large B-cell lymphoma (DLBCL) patients | Plasma ctDNA | Liquid biopsies allow to correctly genotype DLBCL. cfDNA analysis could be used for follow-up as a complement to Positron Emission Tomography (PET) scan imaging. |
| Gao, W. et al., 2018 [15] | 143 lung cancer patients | Blood CTCs | The combined use of immunomagnetic beads and ddPCR allows to sensitively detect CTCs, which have diagnostic value and potential for prognosis and monitoring of lung cancer patients. |
| Guibert, N. et al., 2018 (NCT02827344) [13] | 96 NSCLC patients | Blood CTCs | It is possible to detect programmed death ligand 1 (PD-L1) expression in CTCs of NSCLC patients. CTCs were more frequently PD-L1(+) than tumor tissues and PD-L1(+) CTCs were found in all patients at progression. |
| Boffa, D.J. et al., 2017 (NCT01830426) [73] | 112 NSCLC patients | Blood CTCs | PD-L1 expression in peripheral blood cells of NSCLC patients is associated with worse survival. |
| Jensen, T.J. et al., 2019 [56] | 44 patients, including NSCLC (n = 8), melanoma (n = 8), breast cancer (n = 4), and others | Plasma ctDNA | The evaluation of dynamic copy number variations (CNVs) in cfDNA could serve as an early indicator of immunotherapy response or progression in various cancers. |
| Hong, X. et al., 2018 [14] | 49 melanoma patients | Blood CTCs | RNA-based scoring of CTCs allows to serially monitor melanoma patients treated with immune checkpoint inhibitors (ICIs) and is predictive of clinical outcome. |
| Xue, L. et al., 2018 [77] | 402 NSCLC patients | Blood tumor educated platelets (TEPs) | TEP RNA biomarkers could help NSCLC diagnosis and facilitate early detection. |
| Avogbe, P.H. et al., 2019 [23] | 143 urothelial cancer patients | Plasma and urine ctDNA, and DNA from urinary exfoliated cells | The identification of TERT promoter mutations in urinary DNA is a highly sensitive and specific method for urothelial cancer detection, exceeding the performance of urine cytology for the detection of low-grade cancer. |
| Cheng, T.H.T. et al., 2019 [58] | 46 bladder cancer patients | Urine ctDNA | Methylation and copy number analysis of urinary cfDNA allows to detect bladder cancer, which could be valuable for diagnosis and monitoring of tumor burden. |
| Sinha, S. et al., 2019 [26] | 39 CRC patients | Plasma cfDNA | cfDNA quantity and integrity index (265/80 bp) is able to distinguish stage IV mCRC patients from healthy controls and might be useful for treatment monitoring. |
| Tian, J. et al., 2019 [27] | 57 cervical cancer patients | Plasma ctDNA | Targeted deep sequencing of cfDNA is useful to monitor treatment response and to predict progression in cervical cancer. |
| Akamatsu, H. et al., 2019 (WJOG8114LTR) [29] | 57 NSCLC patients | Plasma ctDNA | Liquid biopsies are able to predict treatment efficacy and progression in part of EGFR-mutated NSCLC patients. |
| Fernandez-Garcia, D. et al., 2019 [30] | 194 mBC patients | Plasma cfDNA and blood CTCs | Total cfDNA levels and CTC number are predictors of disease response and outcomes in mBC. |
| Bernard, V. et al., 2019 [32] | 194 pancreatic adenocarcinoma patients | Plasma ctDNA and DNA in exosomes (exoDNA) | Longitudinal monitorization of ctDNA and exoDNA provides prognostic information, which could be useful for therapeutic stratification of adenocarcinoma patients. |
| Benešová, L. et al., 2019 [33] | 47 mCRC patients | Plasma ctDNA | ctDNA is useful for the early detection of recurrence and to confirm surgery extent in mCRC. |
| Zedan, A.H. et al., 2019 [63] | 149 PCa patients | Plasma miRNAs | The changing levels of miRNA-93 and miRNA-221 during follow-up reveal their potential role for PCa monitoring. |
| Lv, J. et al., 2019 [38] | 673 nasopharyngeal carcinoma patients | Plasma cfEBV DNA | Longitudinal quantification of cfEBV DNA in nasopharyngeal carcinoma during treatment adds prognostic value and may be helpful to adapt treatments according to risk. |
| Braig, D. et al., 2019 [22] | 64 soft tissue sarcoma (STS) patients | Plasma cfDNA | Quantification and fragmentation analysis of cfDNA can distinguish patients with myxoid sarcomas from patients in complete remission or healthy individuals. Genotyping of ctDNA has potential to monitor myxoid sarcoma patients and to detect minimal residual disease and recurrence. |
| Cheng, J. et al., 2019 [40] | 40 NSCLC | Plasma ctDNA | ctDNA analysis using a gene panel to study commonly mutated genes in NSCLC advanced tumors allowed to detect mutations at diagnosis, to monitor response to treatment, and to find resistance mutations. |
| Bordi, R. et al., 2019 (NCT02474335) [46] | 38 NSCLC | Plasma ctDNA | The analysis of ctDNA EGFR mutations plays a crucial role in prognosis of NSCLC. |
| Egyud, M. et al., 2019 [48] | 38 esophageal carcinoma patients | Plasma ctDNA | Plasma ctDNA is detectable and correlates with disease burden in esophageal carcinoma. ctDNA could be used to monitor treatment response and recurrence. |
| Francaviglia, I. et al., 2019 [49] | 100 NSCLC patients | Plasma ctDNA | ctDNA is useful to identify therapeutic targets, to monitor therapy and to find mechanisms of resistance in NSCLC. |
| Malczewska, A. et al., 2019 [4] | 99 bronchopulmonary carcinoid tumor (BPC) patients and 101 patients with other lung neoplasias | Blood mRNA | Increased levels of target transcripts are indicative of lung neuroendocrine neoplasia. Gene expression was concordant in blood and matched tumor tissues and allowed to identify disease progression accurately. |
| Pizzi, M.P. et a., 2019 [54] | 46 gastric adenocarcinoma patients | Plasma and gastric wash ctDNA | Gastric washes are a source of ctDNA and could be used to track mutations in gastric adenocarcinoma patients. Combined analysis of gastric washes and plasma increased sensitivity of ctDNA detection. |
| Herrmann, S. et al., 2019 [55] | 34 CRC patients | Plasma ctDNA | The use of custom amplicon panels allows to detect relevant sets of ctDNA mutations and to monitor treatment response and development of resistance in CRC. |
| Miller, A.M. et al., 2019 [60] | 85 glioma patients | Cerebrospinal fluid (CSF) ctDNA | ctDNA from CSF collected from glioma patients is able to represent the tumor profile and could be used to track tumor evolution. |
| Iwama, E. et al., 2020 [45] | 100 NSCLC patients | Plasma ctDNA | The analysis of mutations in cfDNA is useful to predict efficacy and to monitor clonal evolution during EGFR TKI treatment in NSCLC. |
| Yu, H. et al., 2020 [52] | 150 mCRC patients | Plasma and urine ctDNA | Both plasma and urine ctDNA genotyping might have clinical utility in mCRC, namely for monitoring and risk stratification. |
| Sol, N. et al., 2020 [78] | 89 primary glioblastoma patients and 126 patients with one or multiple brain metastases [primary tumors include: NSCLC (n = 85); BC (n = 15); melanoma (n = 15); renal cell carcinoma (n = 7); and others] | Blood TEPs | TEP-spliced RNA profiles enable high-accuracy classification compared with TEP-spliced RNA profiles from asymptomatic healthy controls and patients with neuro-inflammatory or other (neuro)oncological conditions. TEPs profiles are dynamic, indicating that TEPs can be employed for blood-based therapy monitoring. |
| Liquid Biopsy Analytes | Clinical Applications | Limitations | |||||
|---|---|---|---|---|---|---|---|
| Aid Diagnosis | Tumor Profiling | Prognosis | Monitoring Treatment Response | Early Identification of Resistance Mechanisms | Early Detection of Relapse or Residual Disease | ||
| Cell-free DNA (cfDNA) | [17,21,22,26,39,47,52] | [6,17,29,32,35,40,42,43,44,50,52,53,57] | [3,17,28,31,33,35,37,41,42,44,45,48,49,50,55,75] | [3,6,29,31,34,37,38,39,41,42,45,46,48,49,51,53,59] | [28,29,43,47,50] | [3,31,33,35,38,42,48,50,51,75] | Low concentrations and low sensitivity of detection [12,41,44,92] |
| Lack of standardized preanalytical protocols [92] | |||||||
| Circulating Tumor Cells (CTCs) | [8,15] | [8,12,13,16,30] | [14,15,67,73] | [9,10,11,14,30,75] | [5,12,75] | [8] | Rare in circulation [5,12,16] |
| Difficult and costly isolation [5,12,16,30] | |||||||
| Circulating RNAs | [4,62,64,65] | [4,61,64,65] | [65] | [4,63,64,65] | [4,64] | Techniques in early development [93] | |
| RNA instability [93] | |||||||
| Difficult to detect low abundance RNAs [93] | |||||||
| Extracellular Vesicles (EVs) and Tumor-Associated Microparticles (taMPs) | [61,66] | [32] | [10,61,66] | Lack of standardized preanalytical protocols [61,92] | |||
| Tumor Educated Platelets (TEPs) | [77] | [78] | [76] | [78] | Techniques in early development [42,78] | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Martins, I.; Ribeiro, I.P.; Jorge, J.; Gonçalves, A.C.; Sarmento-Ribeiro, A.B.; Melo, J.B.; Carreira, I.M. Liquid Biopsies: Applications for Cancer Diagnosis and Monitoring. Genes 2021, 12, 349. https://0-doi-org.brum.beds.ac.uk/10.3390/genes12030349
Martins I, Ribeiro IP, Jorge J, Gonçalves AC, Sarmento-Ribeiro AB, Melo JB, Carreira IM. Liquid Biopsies: Applications for Cancer Diagnosis and Monitoring. Genes. 2021; 12(3):349. https://0-doi-org.brum.beds.ac.uk/10.3390/genes12030349
Chicago/Turabian StyleMartins, Ivana, Ilda Patrícia Ribeiro, Joana Jorge, Ana Cristina Gonçalves, Ana Bela Sarmento-Ribeiro, Joana Barbosa Melo, and Isabel Marques Carreira. 2021. "Liquid Biopsies: Applications for Cancer Diagnosis and Monitoring" Genes 12, no. 3: 349. https://0-doi-org.brum.beds.ac.uk/10.3390/genes12030349