
The Role of the Reanalysis of Genetic Test Results in the Diagnosis of Dysmorphic Syndrome Caused by Inherited Xq24 Deletion including the UBE2A and CXorf56 Genes

 , , and
, , and {kind=link}
{kind=link}
Abstract
:1. Clinical Report
2. Genetic Results
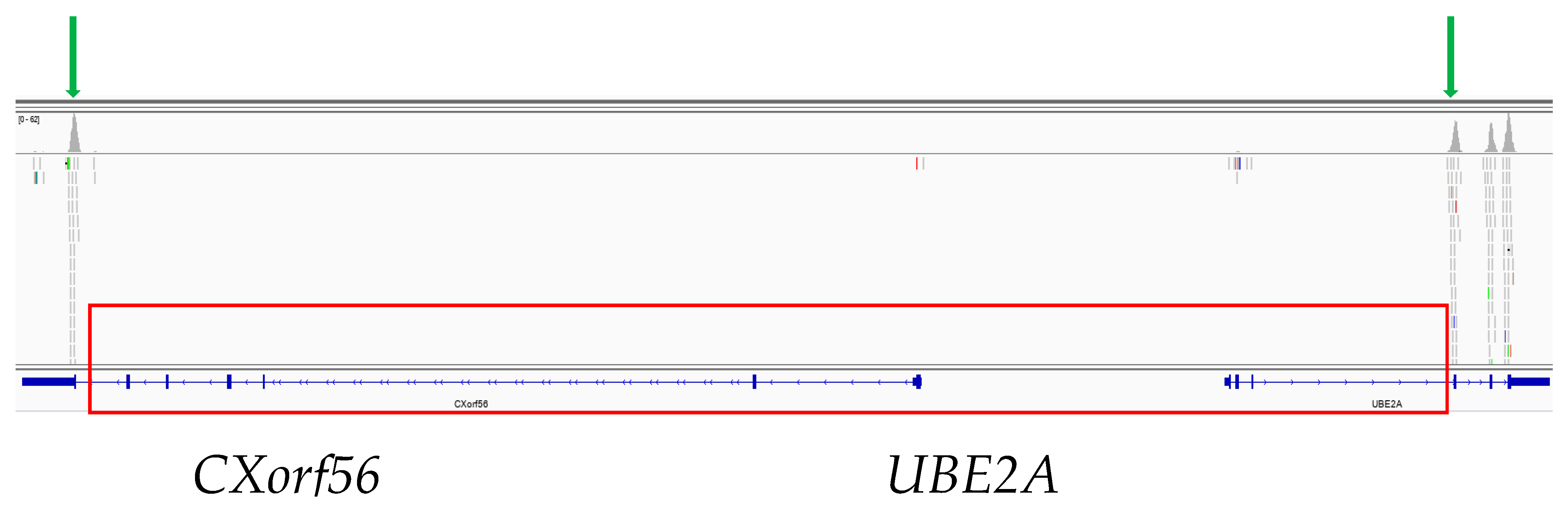
WES Study
3. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Rydzanicz, M.; Wachowska, M.; Cook, E.C.; Lisowski, P.; Kuźniewska, B.; Szymańska, K.; Diecke, S.; Prigione, A.; Szczałuba, K.; Szybińska, A.; et al. Novel calcineurin A (PPP3CA) variant associated with epilepsy, constitutive enzyme activation and downregulation of protein expression. Eur. J. Hum. Genet. 2019, 27, 61–69. [Google Scholar] [CrossRef] [PubMed]
- Integrative Genomics Viewer. Available online: http://software.broadinstitute.org/software/igv/ (accessed on 3 January 2021).
- The Genome Aggregation Database. Available online: https://gnomad.broadinstitute.org/ (accessed on 20 August 2020).
- Hennekam, R.C.M.; Krantz, I.D.; Allanson, J.E. Gorlin’s Syndromes of Head and Neck, 5th ed.; Oxford University Press: New York, NY, USA, 2010. [Google Scholar]
- Aase, J.M. Diagnostic Dysmorphology; Plenum Medical Book Company: New York, NY, USA; London, UK, 1990. [Google Scholar]
- Beaudet, A.L. The Utility of Chromosomal Microarray Analysis in Developmental and Behavioral Pediatrics. Child Dev. 2013, 84, 121–132. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hennekam, R.C.; Biesecker, L.G. Next-generation sequencing demands next-generation phenotyping. Hum. Mutat. 2012, 33, 884–886. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thunstrom, S.; Sodermark, L.; Ivarsson, L.; Samuelsson, L.; Stefanova, M. UBE2A Deficiency Syndrome: A Report of Two Unrelated Cases with Large Xq24 Deletions Encompassing UBE2A Gene. Am. J. Med. Genet. Part A 2014, 167A, 204–210. [Google Scholar] [PubMed]
- Tsurusaki, Y.; Ohashi, I.; Enomoto, Y.; Naruto, T.; Mitsui, J.; Aida, N.; Kurosawa, K. A novel UBE2A mutation causes X-linked intellectual disability type Nascimento. Hum. Genome Var. 2017, 4, hgv201719. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Verkerk, A.; Zeidler, S.; Breedveld, G.; Overbeek, L.; Huigh, D.; Koster, L.; van der Linde, H.; de Esch, C.; Severijnen, L.A.; de Vries, B. CXorf56, a dendritic neuronal protein, identified as a new candidategene for X-linked intellectual disability. Eur. J. Hum. Genet. 2018, 26, 552–560. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Budny, B.; Badura-Stronka, M.; Materna-Kiryluk, A.; Tzschach, A.; Raynaud, M.; Latos-Bielenska, A.; Ropers, H.H. Novel missense mutationsin the ubiquitination-related gene UBE2A cause a recognizable X-linked mental retardation syndrome. Clin. Genet. 2010, 77, 541–551. [Google Scholar] [CrossRef] [PubMed]
- De Leeuw, N.; Bulk, S.; Green, A.; Jaeckle-Santos, L.; Baker, L.A.; Zinn, A.R.; Kleefstra, T.; van der Smagt, J.J.; Vianne Morgante, A.M.; de Vries, B.B.; et al. UBE2A Deficiency Syndrome: Mild to Severe Intellectual Disability Ac-companied by Seizures, Absent Speech, Urogenital, and Skin Anomalies in Male Patients. Am. J. Med. Genet. Part A 2010, 152A, 3084–3090. [Google Scholar] [CrossRef] [PubMed]
- Czeschik, J.C.; Bauer, P.; Buiting, K.; Dufke, C.; Guillén-Navarro, E.; Johnson, D.S.; Koehler, U.; López-González, V.; Lüdecke, H.-J.; Male, A.; et al. X-linked intellectual disability type Nascimento is a clinically distinct, probably underdiagnosed entity. Orphanet. J. Rare Dis. 2013, 8, 146. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Honda, S.; Orii, K.; Kobayashi, J.; Hayashi, S.; Imamura, A.; Imoto, I.; Nakagawa, E.; Goto, Y.-I.; Inazawa, J. Novel deletion at Xq24 including the UBE2A gene in a patient with X-linked mental retardation. J. Hum. Genet. 2010, 55, 244–247. [Google Scholar] [CrossRef] [PubMed]
- Miller, D.T.; Adam, M.P.; Aradhya, S.; Biesecker, L.G.; Brothman, A.R.; Carter, N.P.; Church, D.M.; Crolla, J.A.; Eichler, E.E.; Epstein, C.J.; et al. Consensus Statement: Chromosomal Microarray Is a First-Tier Clinical Diagnostic Test for Individuals with Developmental Disabilities or Congenital Anomalies. Am. J. Hum. Genet. 2010, 86, 749–764. [Google Scholar] [CrossRef] [PubMed]
- Boycott, K.M.; Vanstone, M.R.; Bulman, D.E.; MacKenzie, A.E. Rare-disease genetics in the era of next-generation sequencing: Discovery to translation. Nat. Rev. Genet. 2013, 14, 681–691. [Google Scholar] [CrossRef] [PubMed]
- Bamshad, M.J.; Ng, S.B.; Bigham, A.W.; Tabor, H.K.; Emond, M.J.; Nickerson, D.A.; Shendure, J. Exome sequencing as a tool for Mendelian disease gene discovery. Nat. Rev. Genet. 2011, 12, 745–755. [Google Scholar] [CrossRef] [PubMed]
- Murcia Pienkowski, V.; Kucharczyk, M.; Rydzanicz, M.; Poszewiecka, B.; Pachota, K.; Młynek, M.; Stawiński, P.; Pollak, A.; Kosińska, J.; Wojciechowska, K.; et al. Breakpoint Mapping of Symptomatic Balanced Translocations Links the EPHA6, KLF13 and UBR3 Genes to Novel Disease Phenotype. J. Clin. Med. 2020, 25, 1245. [Google Scholar] [CrossRef] [PubMed]
- Douzgou, S.; Panel, T.D.E.; Clayton-Smith, J.; Gardner, S.; Day, R.; Griffiths, P.; Strong, K.; Amiel, J.; Baraitser, M.; Brueton, L.; et al. Dysmorphology at a distance: Results of a web-based diagnostic service. Eur. J. Hum. Genet. 2013, 22, 327–332. [Google Scholar] [CrossRef] [PubMed] [Green Version]


Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wolańska, E.; Pollak, A.; Rydzanicz, M.; Pesz, K.; Kłaniewska, M.; Rozensztrauch, A.; Skiba, P.; Stawiński, P.; Płoski, R.; Śmigiel, R. The Role of the Reanalysis of Genetic Test Results in the Diagnosis of Dysmorphic Syndrome Caused by Inherited Xq24 Deletion including the UBE2A and CXorf56 Genes. Genes 2021, 12, 350. https://0-doi-org.brum.beds.ac.uk/10.3390/genes12030350
Wolańska E, Pollak A, Rydzanicz M, Pesz K, Kłaniewska M, Rozensztrauch A, Skiba P, Stawiński P, Płoski R, Śmigiel R. The Role of the Reanalysis of Genetic Test Results in the Diagnosis of Dysmorphic Syndrome Caused by Inherited Xq24 Deletion including the UBE2A and CXorf56 Genes. Genes. 2021; 12(3):350. https://0-doi-org.brum.beds.ac.uk/10.3390/genes12030350
Chicago/Turabian StyleWolańska, Ewelina, Agnieszka Pollak, Małgorzata Rydzanicz, Karolina Pesz, Magdalena Kłaniewska, Anna Rozensztrauch, Paweł Skiba, Piotr Stawiński, Rafał Płoski, and Robert Śmigiel. 2021. "The Role of the Reanalysis of Genetic Test Results in the Diagnosis of Dysmorphic Syndrome Caused by Inherited Xq24 Deletion including the UBE2A and CXorf56 Genes" Genes 12, no. 3: 350. https://0-doi-org.brum.beds.ac.uk/10.3390/genes12030350