
CT-Based Risk Stratification for Intensive Care Need and Survival in COVID-19 Patients—A Simple Solution

 ,
,
Abstract
:1. Introduction
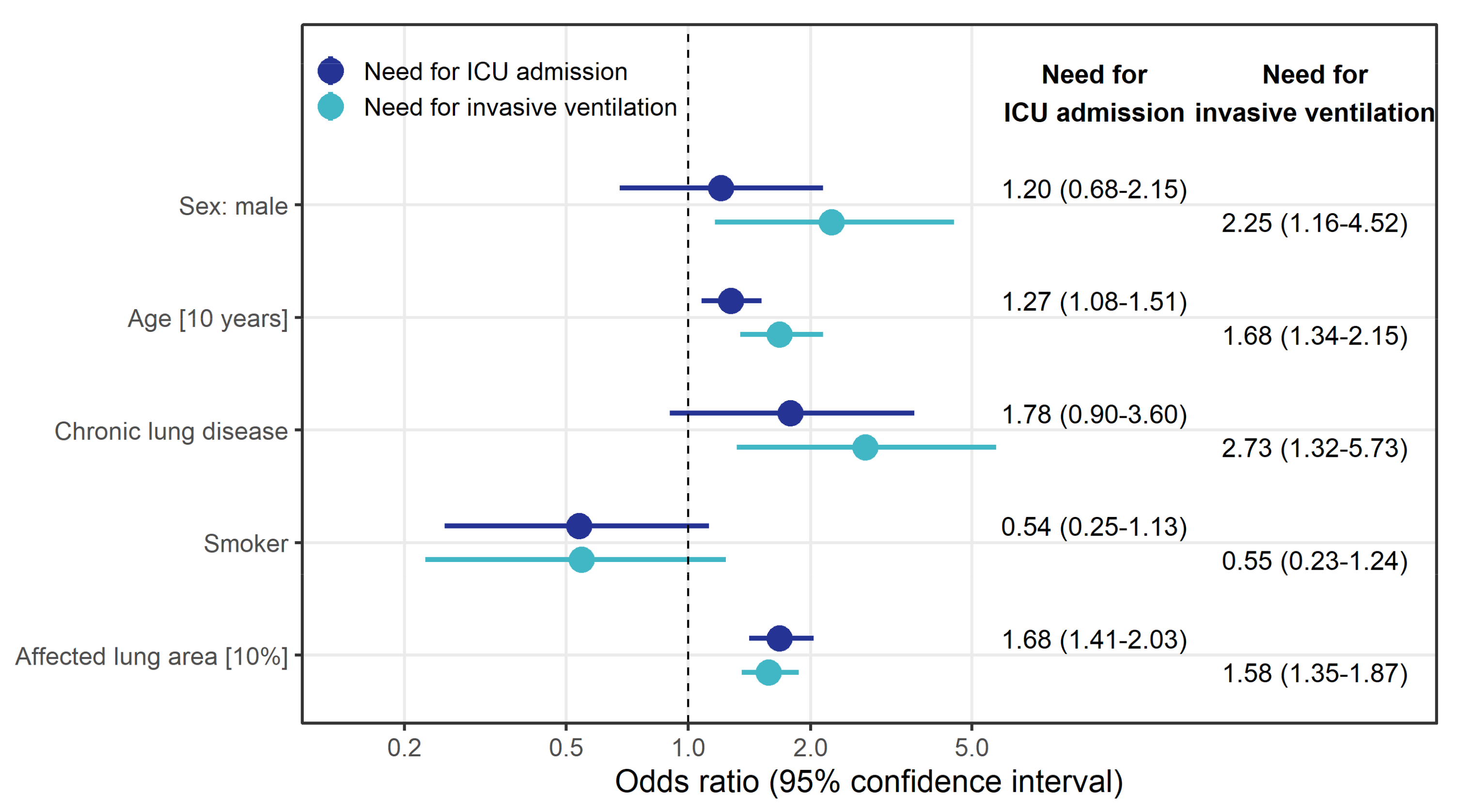
- With the SSQ method, a 10% increase in affected lung area increased the risk for need of ICU treatment with an OR of 1.68 (95% CI: 1.41–2.03) and for invasive ventilation with an OR of 1.58 (95% CI: 1.35–1.87).
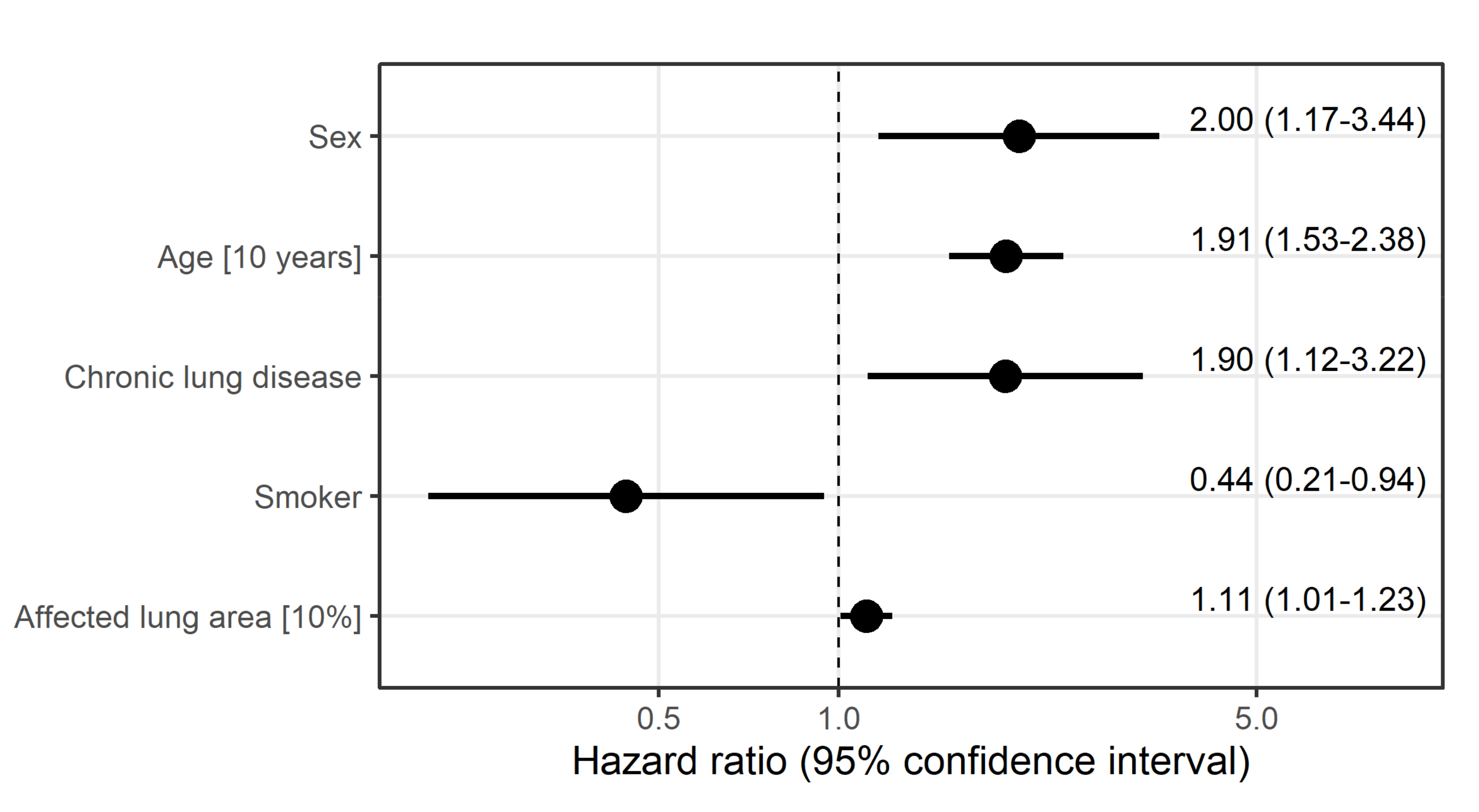
- A larger total affected lung area increased the cause-specific instantaneous risk of dying (HR 1.11 (95% CI: 1.01–1.23) independently of other risk factors.
- SSQ assessment of lung involvement in the first available CT scans of COVID-19 patients may support early identification of those in need for ICU treatment and invasive ventilation, yet well-trained radiologists achieve comparable results.
2. Materials and Methods
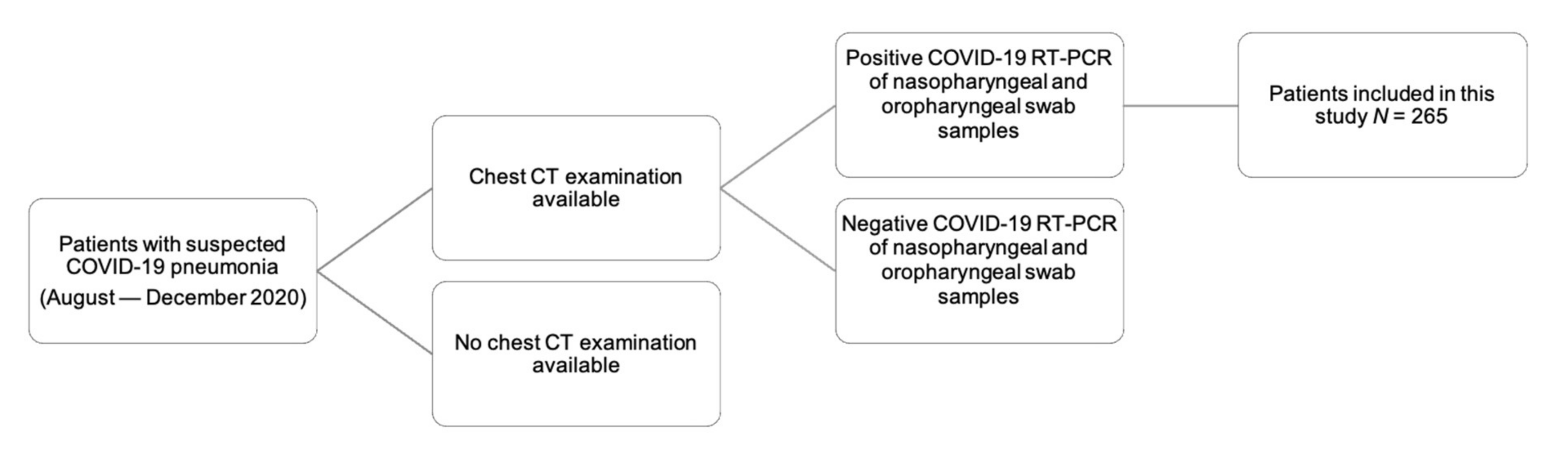
2.1. Study Design and Patient Population
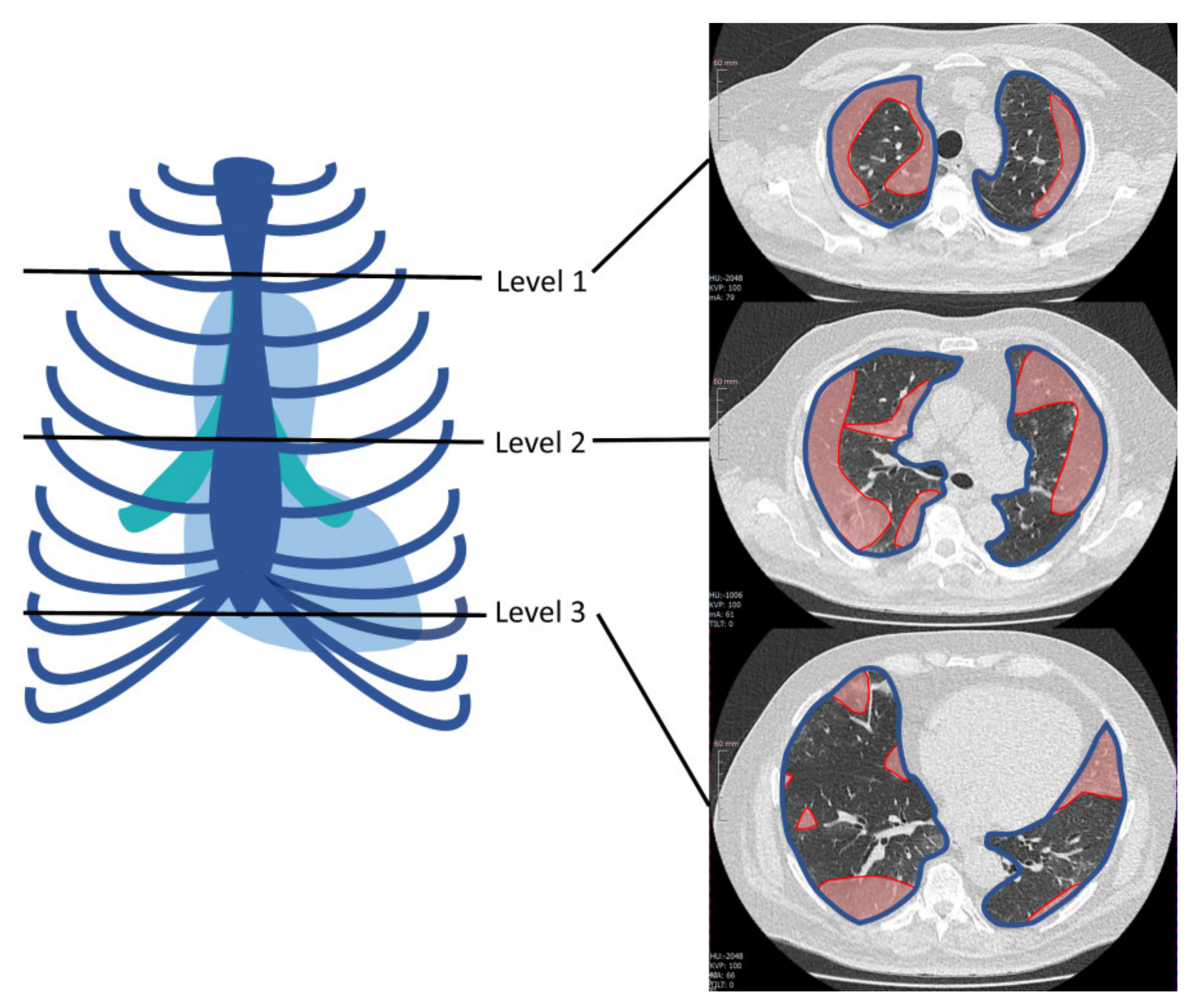
2.2. Subjective and SSQ Assessment of CT Scans
2.3. CT Scan Parameters
2.4. Statistical Evaluation
3. Results
3.1. Epidemiologic Patient Data
3.2. Subjective CT Assessment
3.3. SSQ Assessment of CT Scans
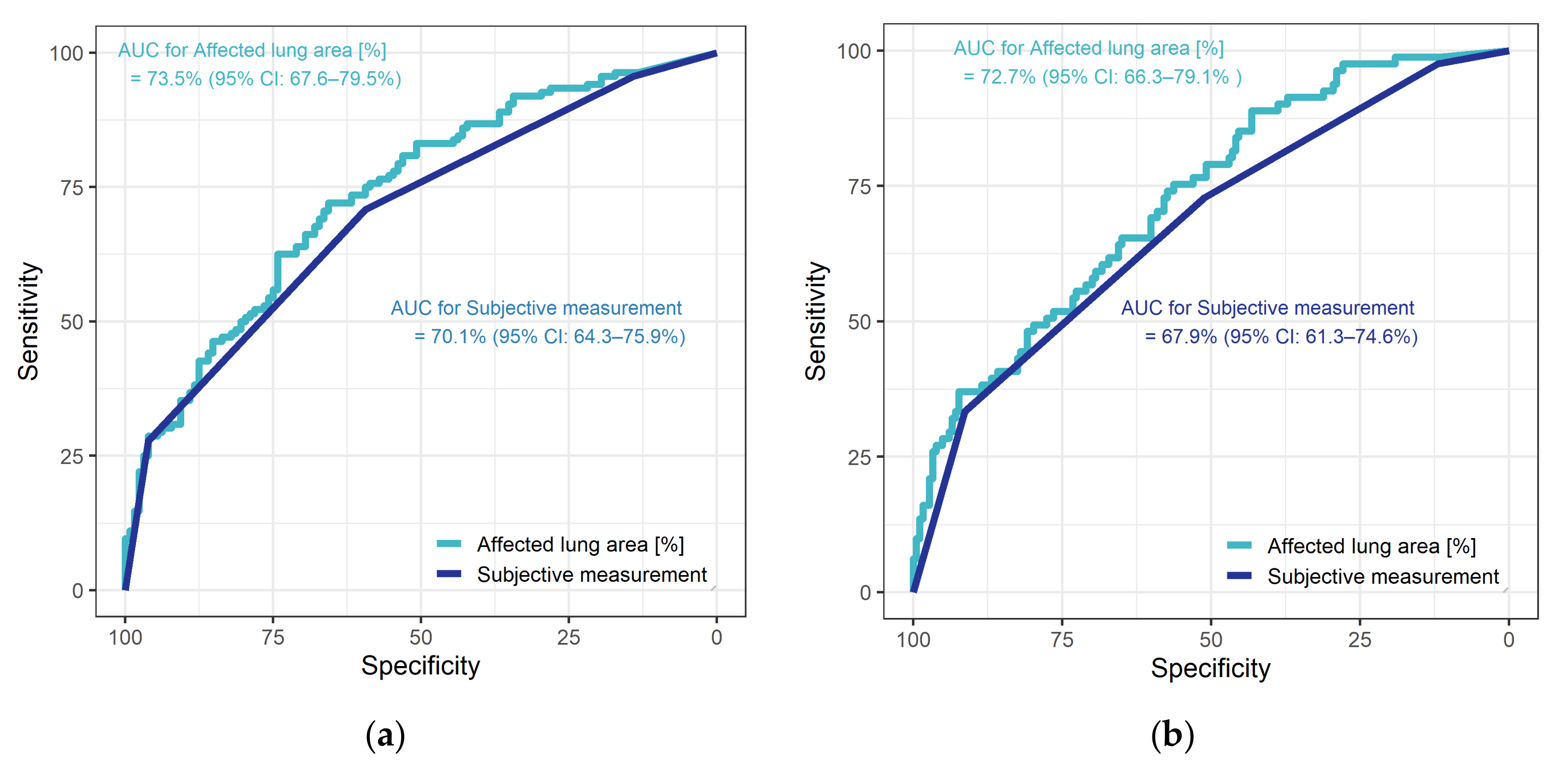
3.4. Diagnostic Performance
3.5. Risk Stratification
3.6. Survival Analysis
4. Discussion
4.1. Epidemiologic Patient Data
4.2. Subjective CT Assessment
4.3. Diagnostic Performance
4.4. Risk Stratification
4.5. Survival Analysis
4.6. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Zhou, P.; Yang, X.-L.; Wang, X.-G.; Hu, B.; Zhang, L.; Zhang, W.; Si, H.-R.; Zhu, Y.; Li, B.; Huang, C.-L.; et al. A pneumonia outbreak associated with a new coronavirus of probable bat origin. Nature 2020, 579, 270–273. [Google Scholar] [CrossRef] [Green Version]
- Wu, F.; Zhao, S.; Yu, B.; Chen, Y.-M.; Wang, W.; Song, Z.-G.; Hu, Y.; Tao, Z.-W.; Tian, J.-H.; Pei, Y.-Y.; et al. A new coronavirus associated with human respiratory disease in China. Nature 2020, 579, 265–269. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- W.W.H. Organization. WHO Coronavirus (COVID-19) Dashboard. WHO Health Emergency Dashboard. 2020. Available online: https://covid19.who.int/ (accessed on 5 May 2021).
- Wu, Y.-C.; Chen, C.-S.; Chan, Y.-J. The outbreak of COVID-19: An overview. J. Chin. Med. Assoc. 2020, 83, 217–220. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez-Morales, A.J.; Cardona-Ospina, J.A.; Gutiérrez-Ocampo, E.; Villamizar-Peña, R.; Holguin-Rivera, Y.; Escalera-Antezana, J.P.; Alvarado-Arnez, L.E.; Bonilla-Aldana, D.K.; Franco-Paredes, C.; Henao-Martinez, A.F.; et al. Clinical, laboratory and imaging features of COVID-19: A systematic review and meta-analysis. Travel Med. Infect. Dis. 2020, 34, 101623. [Google Scholar] [CrossRef]
- Karagiannidis, C.; Mostert, C.; Hentschker, C.; Voshaar, T.; Malzahn, J.; Schillinger, G.; Klauber, J.; Janssens, U.; Marx, G.; Weber-Carstens, S.; et al. Case characteristics, resource use, and outcomes of 10,021 patients with COVID-19 admitted to 920 German hospitals: An observational study. Lancet Respir. Med. 2020, 8, 853–862. [Google Scholar] [CrossRef]
- Robert Koch Institut. SARS-CoV-2 Steckbrief zur Coronavirus-Krankheit-2019 (COVID-19). 2020. Available online: https://www.rki.de/DE/Content/InfAZ/N/Neuartiges_Coronavirus/Steckbrief.html#doc13776792bodyText1 (accessed on 19 May 2021).
- Phua, J.; Weng, L.; Ling, L.; Egi, M.; Lim, C.-M.; Divatia, J.V.; Shrestha, B.R.; Arabi, Y.M.; Ng, J.; Gomersall, C.D.; et al. Intensive care management of coronavirus disease 2019 (COVID-19): Challenges and recommendations. Lancet Respir. Med. 2020, 8, 506–517. [Google Scholar] [CrossRef]
- Rubin, G.D.; Ryerson, C.J.; Haramati, L.B.; Sverzellati, N.; Kanne, J.P.; Raoof, S.; Schluger, N.W.; Volpi, A.; Yim, J.J.; Martin, I.B.K.; et al. The Role of Chest Imaging in Patient Management during the COVID-19 Pandemic: A Multinational Consensus Statement from the Fleischner Society. Radiology 2020, 296, 172–180. [Google Scholar] [CrossRef] [Green Version]
- Chen, Z.; Fan, H.; Cai, J.; Li, Y.; Wu, B.; Hou, Y.; Xu, S.; Zhou, F.; Liu, Y.; Xuan, W.; et al. High-resolution computed tomography manifestations of COVID-19 infections in patients of different ages. Eur. J. Radiol. 2020, 126, 108972. [Google Scholar] [CrossRef] [Green Version]
- Colombi, D.; Bodini, F.C.; Petrini, M.; Maffi, G.; Morelli, N.; Milanese, G.; Silva, M.; Sverzellati, N.; Michieletti, E. Well-aerated Lung on Admitting Chest CT to Predict Adverse Outcome in COVID-19 Pneumonia. Radiology 2020, 296, e86–e96. [Google Scholar] [CrossRef] [Green Version]
- Hamper, C.M.; Fleckenstein, F.N.; Büttner, L.; Hamm, B.; Thieme, N.; Thiess, H.M.; Scholz, O.; Döllinger, F.; Böning, G. Submillisievert chest CT in patients with COVID-19—Experiences of a German Level-I center. Eur. J. Radiol. Open 2020, 7, 100283. [Google Scholar] [CrossRef]
- Lee, E.H.; Zheng, J.; Colak, E.; Mohammadzadeh, M.; Houshmand, G.; Bevins, N.; Kitamura, F.; Altinmakas, E.; Reis, E.P.; Kim, J.-K.; et al. Deep COVID DeteCT: An international experience on COVID-19 lung detection and prognosis using chest CT. NPJ Digit. Med. 2021, 4, 11. [Google Scholar] [CrossRef] [PubMed]
- Bong, C.-L.; Brasher, C.; Chikumba, E.; McDougall, R.; Mellin-Olsen, J.; Enright, A. The COVID-19 Pandemic: Effects on Low- and Middle-Income Countries. Anesth. Analg. 2020, 131, 86–92. [Google Scholar] [CrossRef]
- Kanne, J.P.; Bai, H.; Bernheim, A.; Chung, M.; Haramati, L.B.; Kallmes, D.F.; Little, B.P.; Rubin, G.; Sverzellati, N. COVID-19 Imaging: What We Know Now and What Remains Unknown. Radiology 2021, 299, e262–e279. [Google Scholar] [CrossRef]
- Büttner, L.; Aigner, A.; Fleckenstein, F.N.; Hamper, C.M.; Jonczyk, M.; Hamm, B.; Scholz, O.; Böning, G. Diagnostic Value of Initial Chest CT Findings for the Need of ICU Treatment/Intubation in Patients with COVID-19. Diagnostics 2020, 10, 929. [Google Scholar] [CrossRef]
- Kluge, S.; Janssens, U.; Welte, T.; Weber-Carstens, S.; Schälte, G.; Salzberger, B.; Gastmeier, P.; Langer, F.; Wepler, M.; Westhoff, M.; et al. German recommendations for treatment of critically ill patients with COVID-19-version 3. Pneumologe 2020, 1–12. [Google Scholar] [CrossRef]
- RC Team. R: A Language and Environment for Statistical Computing. R Foundation for Statistical Computing. 2019. Available online: https://www.R-project.org/ (accessed on 25 April 2020).
- Huang, L.; Han, R.; Ai, T.; Yu, P.; Kang, H.; Tao, Q.; Xia, L. Serial Quantitative Chest CT Assessment of COVID-19: A Deep Learning Approach. Radiol. Cardiothorac. Imaging 2020, 2, e200075. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gresser, E.; Rueckel, J.; Puhr-Westerheide, D.; Schwarze, V.; Fink, N.; Kunz, W.G.; Wassilowsky, D.; Irlbeck, M.; Ricke, J.; Ingrisch, M.; et al. Prognostic Value of Admission Chest CT Findings for Invasive Ventilation Therapy in COVID-19 Pneumonia. Diagnostics 2020, 10, 1108. [Google Scholar] [CrossRef]
- Komolafe, T.E.; Agbo, J.; Olaniyi, E.O.; Komolafe, K.; Yang, X. Prevalence of COVID-19 Diagnostic Output with Chest Computed Tomography: A Systematic Review and Meta-Analysis. Diagnostics 2020, 10, 1023. [Google Scholar] [CrossRef] [PubMed]
- Giagulli, V.A.; Guastamacchia, E.; Magrone, T.; Jirillo, E.; Lisco, G.; De Pergola, G.; Triggiani, V. Worse progression of COVID-19 in men: Is testosterone a key factor? Andrology 2021, 9, 53–64. [Google Scholar] [CrossRef]
- Douglas, G.C.; O’Bryan, M.K.; Hedger, M.P.; Lee, D.K.; Yarski, M.A.; Smith, A.I.; Lew, R.A. The novel angiotensin-converting enzyme (ACE) homolog, ACE2, is selectively expressed by adult Leydig cells of the testis. Endocrinology 2004, 145, 4703–4711. [Google Scholar] [CrossRef] [Green Version]
- Pozzilli, P.; Lenzi, A. Commentary: Testosterone, a key hormone in the context of COVID-19 pandemic. Metabolism 2020, 108, 154252. [Google Scholar] [CrossRef]
- Kwee, T.C.; Kwee, R.M. Chest CT in COVID-19: What the Radiologist Needs to Know. Radiographics 2020, 40, 1848–1865. [Google Scholar] [CrossRef] [PubMed]
- Takahashi, T.; Ellingson, M.K.; Wong, P.; Israelow, B.; Lucas, C.; Klein, J.; Silva, J.; Mao, T.; Oh, J.E.; Tokuyama, M.; et al. Sex differences in immune responses that underlie COVID-19 disease outcomes. Nature 2020, 588, 315–320. [Google Scholar] [CrossRef] [PubMed]
- Zhou, F.; Yu, T.; Du, R.; Fan, G.; Liu, Y.; Liu, Z.; Xiang, J.; Wang, Y.; Song, B.; Gu, X.; et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: A retrospective cohort study. Lancet 2020, 395, 1054–1062. [Google Scholar] [CrossRef]
- Di Castelnuovo, A.; Costanzo, S.; Antinori, A.; Berselli, N.; Blandi, L.; Bonaccio, M.; Bruno, R.; Cauda, R.; Gialluisi, A.; Guaraldi, G.; et al. Lopinavir/Ritonavir and Darunavir/Cobicistat in Hospitalized COVID-19 Patients: Findings From the Multicenter Italian CORIST Study. Front. Med. 2021, 8, 639970. [Google Scholar] [CrossRef]
- Di Castelnuovo, A.; Costanzo, S.; Antinori, A.; Berselli, N.; Blandi, L.; Bonaccio, M.; Cauda, R.; Guaraldi, G.; Menicanti, L.; Mennuni, M.; et al. Heparin in COVID-19 Patients Is Associated with Reduced In-Hospital Mortality: The Multicenter Italian CORIST Study. Thromb. Haemost. 2021, 121, 1054–1065. [Google Scholar] [CrossRef]
- Wu, L.; O’Kane, A.M.; Peng, H.; Bi, Y.; Motriuk-Smith, D.; Ren, J. SARS-CoV-2 and cardiovascular complications: From molecular mechanisms to pharmaceutical management. Biochem. Pharm. 2020, 178, 114114. [Google Scholar] [CrossRef]
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X.; et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef] [Green Version]
- Oudit, G.Y.; Kassiri, Z.; Jiang, C.; Liu, P.P.; Poutanen, S.M.; Penninger, J.M.; Butany, J. SARS-coronavirus modulation of myocardial ACE2 expression and inflammation in patients with SARS. Eur. J. Clin. Investig. 2009, 39, 618–625. [Google Scholar] [CrossRef] [PubMed]
- Lichtenstein, D.A. BLUE-protocol and FALLS-protocol: Two applications of lung ultrasound in the critically ill. Chest 2015, 147, 1659–1670. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Volpicelli, G.; Elbarbary, M.; Blaivas, M.; Lichtenstein, D.A.; Mathis, G.; Kirkpatrick, A.W.; Melniker, L.; Gargani, L.; Noble, V.E.; Via, G.; et al. International evidence-based recommendations for point-of-care lung ultrasound. Intensive Care Med. 2012, 38, 577–591. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mongodi, S.; Bouhemad, B.; Orlando, A.; Stella, A.; Tavazzi, G.; Via, G.; Iotti, G.A.; Braschi, A.; Mojoli, F. Modified Lung Ultrasound Score for Assessing and Monitoring Pulmonary Aeration. Ultraschall Med. 2017, 38, 530–537. [Google Scholar] [CrossRef]
- Lerchbaumer, M.H.; Lauryn, J.H.; Bachmann, U.; Enghard, P.; Fischer, T.; Grune, J.; Hegemann, N.; Khadzhynov, D.; Kruse, J.M.; Lehner, L.J.; et al. Point-of-care lung ultrasound in COVID-19 patients: Inter- and intra-observer agreement in a prospective observational study. Sci. Rep. 2021, 11, 10678. [Google Scholar] [CrossRef]
- Ruch, Y.; Kaeuffer, C.; Ohana, M.; Labani, A.; Fabacher, T.; Bilbault, P.; Kepka, S.; Solis, M.; Greigert, V.; Lefebvre, N.; et al. CT lung lesions as predictors of early death or ICU admission in COVID-19 patients. Clin. Microbiol. Infect. 2020, 26, 1417.e5–1417.e8. [Google Scholar] [CrossRef] [PubMed]
- Vardavas, C.I.; Nikitara, K. COVID-19 and smoking: A systematic review of the evidence. Tob. Induc. Dis. 2020, 18, 20. [Google Scholar] [CrossRef]
- Adams, H.J.A.; Kwee, T.C.; Yakar, D.; Hope, M.D.; Kwee, R.M. Chest CT Imaging Signature of Coronavirus Disease 2019 Infection: In Pursuit of the Scientific Evidence. Chest 2020, 158, 1885–1895. [Google Scholar] [CrossRef]
- Ding, X.; Xu, J.; Zhou, J.; Long, Q. Chest CT findings of COVID-19 pneumonia by duration of symptoms. Eur. J. Radiol. 2020, 127, 109009. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Dong, C.; Hu, Y.; Li, C.; Ren, Q.; Zhang, X.; Shi, H.; Zhou, M. Temporal Changes of CT Findings in 90 Patients with COVID-19 Pneumonia: A Longitudinal Study. Radiology 2020, 296, e55–e64. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bernheim, A.; Mei, X.; Huang, M.; Yang, Y.; Fayad, Z.A.; Zhang, N.; Diao, K.; Lin, B.; Zhu, X.; Li, K.; et al. Chest CT Findings in Coronavirus Disease-19 (COVID-19): Relationship to Duration of Infection. Radiology 2020, 295, 200463. [Google Scholar] [CrossRef] [Green Version]
- Inui, S.; Fujikawa, A.; Jitsu, M.; Kunishima, N.; Watanabe, S.; Suzuki, Y.; Umeda, S.; Uwabe, Y. Chest CT Findings in Cases from the Cruise Ship Diamond Princess with Coronavirus Disease (COVID-19). Radiol. Cardiothorac. Imaging 2020, 2, e200110. [Google Scholar] [CrossRef] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| No Need for Invasive Ventilation (n = 184) | Need for Invasive Ventilation (n = 81) | No Need for ICU Treatment (n = 128) | Need for ICU Treatment (n = 137) | Total (n = 265) | |
|---|---|---|---|---|---|
| Sex and Age | |||||
| Female | 75 (40.8%) | 27 (33.3%) | 50 (39.1%) | 52 (38.0%) | 102 (38.5%) |
| Male | 109 (59.2%) | 54 (66.7%) | 78 (60.9%) | 85 (62.0%) | 163 (61.5%) |
| Age (median (IQR)) | 65 (53–77) | 75 (65–84) | 65 (51–79) | 70 (59–80) | 68 (56–79) |
| Comorbidities | |||||
| Alcohol abuse | 9 (4.9%) | 0 (0.0%) | 8 (6.2%) | 1 (0.7%) | 9 (3.4%) |
| CAD | 49 (26.6%) | 43 (53.1%) | 31 (24.2%) | 61 (44.5%) | 92 (34.7%) |
| Chronic lung disease | 31 (16.8%) | 25 (31.2%) | 22 (17.2%) | 34 (25.0%) | 56 (21.2%) |
| Bronchiectasis | 10 (5.4%) | 26 (32.1%) | 5 (3.9%) | 31 (22.6%) | 36 (13.6%) |
| Emphysema and fibrosis | 16 (8.8%) | 25 (31.2%) | 10 (7.9%) | 31 (23.0%) | 41 (15.7%) |
| Diabetes mellitus | 42 (22.8%) | 25 (30.9%) | 26 (20.3%) | 41 (29.9%) | 67 (25.3%) |
| Hypertension | 106 (57.9%) | 50 (61.7%) | 65 (51.2%) | 91 (66.4%) | 156 (59.1%) |
| Obesity | 45 (24.9%) | 12 (15.0%) | 27 (21.3%) | 30 (22.4%) | 57 (21.8%) |
| Smoker | 33 (17.9%) | 12 (15.0%) | 25 (19.5%) | 20 (14.7%) | 45 (17.0%) |
| Symptoms | |||||
| Abdominal symptoms 1 | 42 (22.8%) | 8 (9.9%) | 27 (21.1%) | 23 (16.8%) | 50 (18.9%) |
| Cardiac symptoms 2 | 29 (15.8%) | 6 (7.4%) | 21 (16.4%) | 14 (10.2%) | 35 (13.2%) |
| Cough | 99 (53.8%) | 37 (45.7%) | 67 (52.3%) | 69 (50.4%) | 136 (51.3%) |
| Dyspnea | 128 (69.6%) | 68 (84.0%) | 76 (59.4%) | 120 (87.6%) | 196 (74.0%) |
| Fever | 122 (66.7%) | 49 (60.5%) | 84 (66.1%) | 87 (63.5%) | 171 (64.8%) |
| Limb pain | 33 (17.9%) | 5 (6.2%) | 24 (18.8%) | 14 (10.2%) | 38 (14.3%) |
| Weakness | 117 (63.6%) | 54 (66.7%) | 83 (64.8%) | 88 (64.2%) | 171 (64.5%) |
| Ventilation | |||||
| None | 56 (30.8%) | 0 (0.0%) | 54 (42.5%) | 2 (1.5%) | 56 (21.4%) |
| Nasal Oxygen | 87 (47.8%) | 25 (31.2%) | 67 (52.8%) | 45 (33.3%) | 112 (42.7%) |
| Noninvasive | 39 (21.4%) | 10 (12.5%) | 6 (4.7%) | 43 (31.9%) | 49 (18.7%) |
| Invasive | 0 (0.0%) | 34 (42.5%) | 0 (0.0%) | 34 (25.2%) | 34 (13.0%) |
| ECMO | 0 (0.0%) | 11 (13.8%) | 0 (0.0%) | 11 (8.1%) | 11 (4.2%) |
| No Need for Invasive Ventilation (n = 184) | Need for Invasive Ventilation (n = 81) | No Need for ICU Treatment (n = 128) | Need for ICU Treatment (n = 137) | Total (n = 265) | |
|---|---|---|---|---|---|
| Subjective Classification of Pulmonary Involvement | |||||
| None | 22 (12.0%) | 2 (2.5%) | 18 (14.1%) | 6 (4.4%) | 24 (9.1%) |
| Minor | 72 (39.1%) | 20 (24.7%) | 58 (45.3%) | 34 (24.8%) | 92 (34.7%) |
| Moderate | 74 (40.2%) | 32 (39.5%) | 47 (36.7%) | 59 (43.1%) | 106 (40.0%) |
| Major | 16 (8.7%) | 27 (33.3%) | 5 (3.9%) | 38 (27.7%) | 43 (16.2%) |
| Consolidations | |||||
| None | 61 (33.2%) | 7 (8.6%) | 46 (35.9%) | 22 (16.1%) | 68 (25.7%) |
| Minor 1 | 85 (46.2%) | 38 (46.9%) | 64 (50.0%) | 59 (43.1%) | 123 (46.4%) |
| Moderate 1 | 28 (15.2%) | 25 (30.9%) | 15 (11.7%) | 38 (27.7%) | 53 (20.0%) |
| Major 1 | 10 (5.4%) | 11 (13.6%) | 3 (2.3%) | 18 (13.1%) | 21 (7.9%) |
| Ground-Glass Opacities (GGOs) | |||||
| No | 24 (13.0%) | 5 (6.2%) | 17 (13.3.%) | 12 (8.8%) | 29 (10.9%) |
| Minor 1 | 65 (35.3%) | 19 (23.5%) | 47 (36.7%) | 37 (27.0%) | 84 (31.7%) |
| Moderate 1 | 72 (39.1%) | 29 (35.8%) | 50 (39,1%) | 52 (37.2%) | 101 (38.1%) |
| Major 1 | 23 (12.5%) | 28 (34.6%) | 14 (10.9%) | 37 (27.0%) | 51 (19.2%) |
| Effusions | |||||
| No | 165 (89.7%) | 59 (72.8%) | 117 (91.4%) | 107 (78.1%) | 224 (84.8%) |
| Minor | 15 (8.2%) | 19 (23.5%) | 10 (7.8%) | 24 (17.5%) | 34 (12.8%) |
| Moderate | 3 (1.6%) | 3 (3.7%) | 1 (0.8%) | 5 (3.6%) | 6 (2.3%) |
| Major | 1 (0.5%) | 0 (0%) | 0 (0%) | 1 (0.7%) | 1 (0.4%) |
| Lymphadenopathy | 35 (19.0%) | 21 (25.9%) | 21 (16.4%) | 35 (25.5%) | 56 (21.1%) |
| Distribution | |||||
| Central | 3 (1.6%) | 3 (3.7%) | 3 (2.3%) | 3 (2.2%) | 6 (2.3%) |
| Diffuse | 13 (7.1%) | 27 (33.3%) | 5 (3.9%) | 35 (25.5%) | 40 (15.1%) |
| No pattern | 21 (11.4%) | 2 (2.5%) | 17 (13.3%) | 6 (4.4.%) | 23 (8.7%) |
| Peribronchial | 72 (39.1%) | 21 (25.9%) | 52 (40.6%) | 41 (29.9%) | 93 (35.1%) |
| Peripheral | 75 (40.8%) | 28 (34.6%) | 51 (39.8%) | 52 (38.9%) | 103 (38.9%) |
| Predominant Localization | |||||
| Apical | 18 (9.7%) | 6 (7.4%) | 11 (8.6%) | 13 (9.5%) | 23 (8.7%) |
| Basal | 82 (44.6%) | 33 (40.7%) | 59 (46.1%) | 56 (40.9%) | 115 (43.4%) |
| Medial | (9 (4.9%) | 6 (7.4%) | 7 (5.5%) | 8 (5.8%) | 15 (5.7%) |
| No pattern | 21 (11.4%) | 5 (6.2%) | 17 (13.3%) | 9 (6.6%) | 26 (9.8%) |
| Posterolateral | 54 (29.3%) | 31 (38.3%) | 34 (26.6%) | 51 (37.2%) | 85 (32.1%) |
| No Need for Invasive Ventilation (n = 184) | Need for Invasive Ventilation (n = 81) | No Need for ICU Treatment (n = 128) | Need for ICU Treatment (n = 137) | Total (n = 265) | |
|---|---|---|---|---|---|
| Aortic arch (% of lung area affected) | 5.4 (0.0–19.7) | 20.3 (7.9–42.8) | 2.7 (0.0–11.5) | 19.6 (5.8–37.6) | 9.9 (0.7–25.2) |
| Tracheal bifurcation (% of lung area affected)) | 10.6 (1.7–21.3) | 24.0 (9.8–51.3) | 6.2 (0.5–16.0) | 20.1 (9.7–44.1) | 12.8 (3.7–31.6) |
| Inferior end of xiphoid (% of lung area affected)) | 14.6 (4.8–27.8) | 32.8 (14.5–57.9) | 12.0 (4.4–24.1) | 24.7 (13.2–49.5) | 18.8 (7.3–37.5) |
| Total affected lung area (%) | 11.7 (4.7–24.4) | 25.5 (14.5–52.3) | 8.2 (3.6–19.6) | 22.6 (12.0–43.3) | 15.3 (6.5–31.1) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hosse, C.; Büttner, L.; Fleckenstein, F.N.; Hamper, C.M.; Jonczyk, M.; Scholz, O.; Aigner, A.; Böning, G. CT-Based Risk Stratification for Intensive Care Need and Survival in COVID-19 Patients—A Simple Solution. Diagnostics 2021, 11, 1616. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics11091616
Hosse C, Büttner L, Fleckenstein FN, Hamper CM, Jonczyk M, Scholz O, Aigner A, Böning G. CT-Based Risk Stratification for Intensive Care Need and Survival in COVID-19 Patients—A Simple Solution. Diagnostics. 2021; 11(9):1616. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics11091616
Chicago/Turabian StyleHosse, Clarissa, Laura Büttner, Florian Nima Fleckenstein, Christina Maria Hamper, Martin Jonczyk, Oriane Scholz, Annette Aigner, and Georg Böning. 2021. "CT-Based Risk Stratification for Intensive Care Need and Survival in COVID-19 Patients—A Simple Solution" Diagnostics 11, no. 9: 1616. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics11091616