
Dental Disorders and Salivary Changes in Patients with Laryngopharyngeal Reflux

 ,
,  , and
, and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Collection
2.2. Clinical Examination
2.3. Qualitative and Quantitative Examination of Saliva
2.4. Statistical Analysis
3. Results
3.1. Intraoral Manifestations
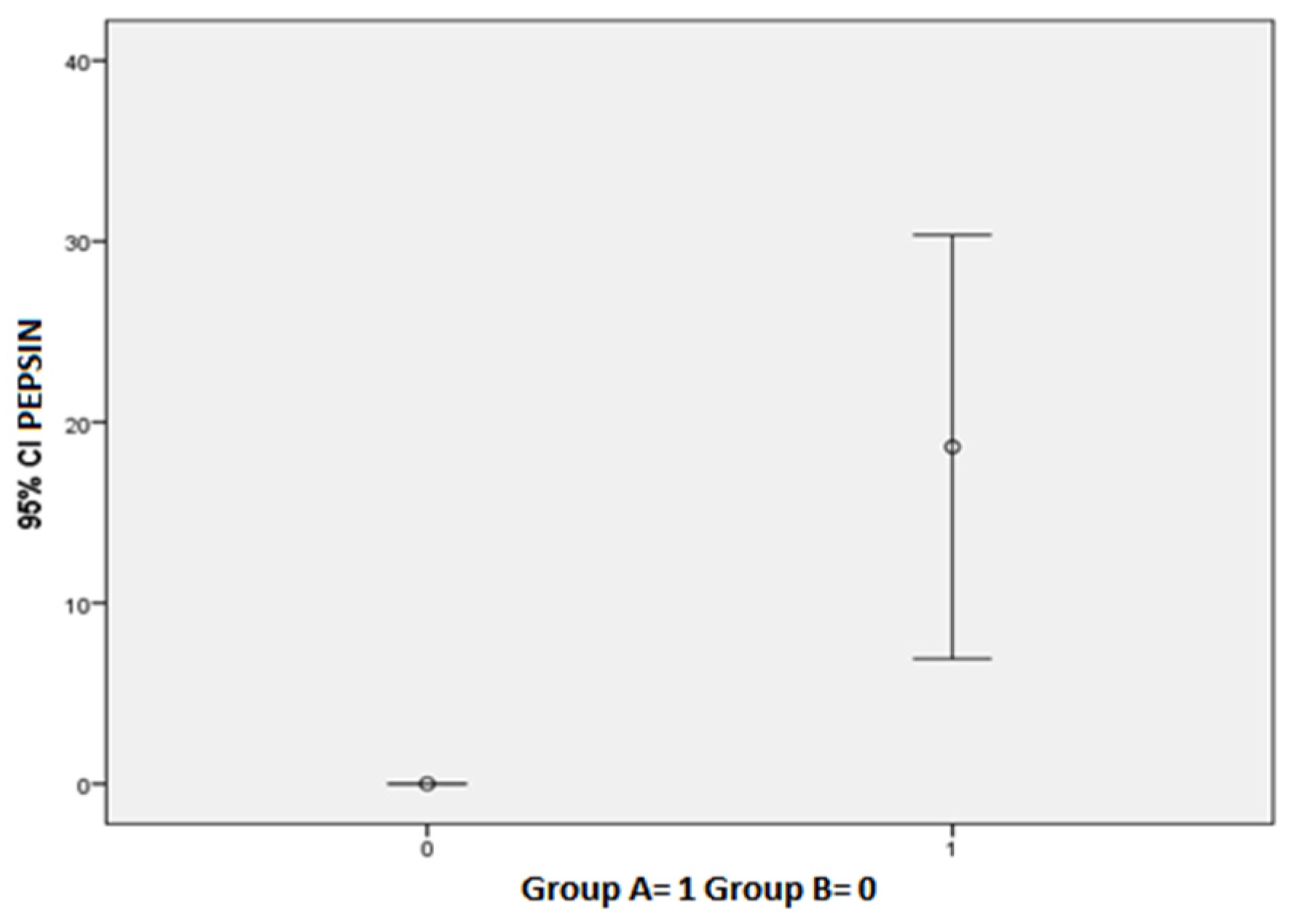
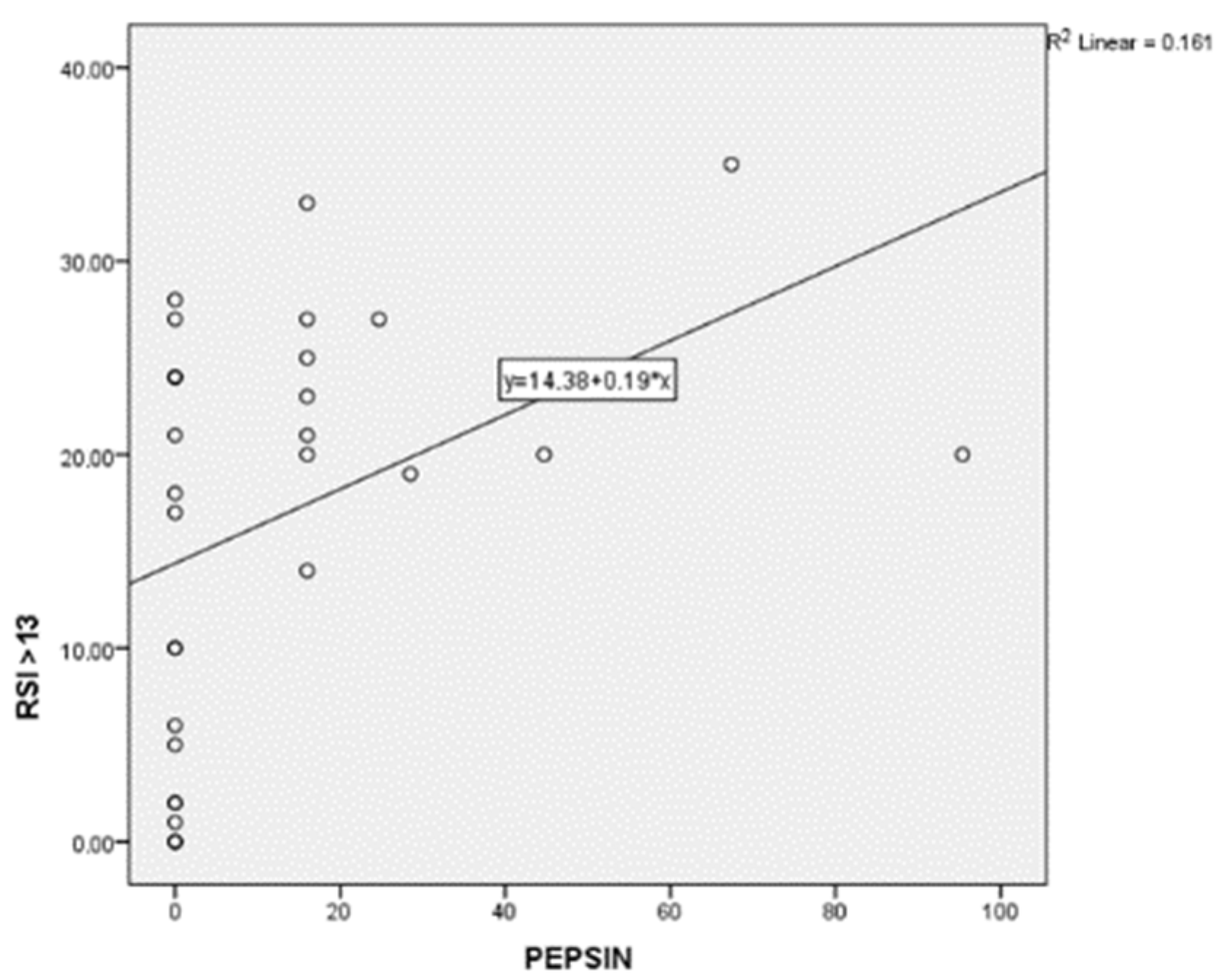
3.2. Salivary Pepsin Levels and Related Symptoms
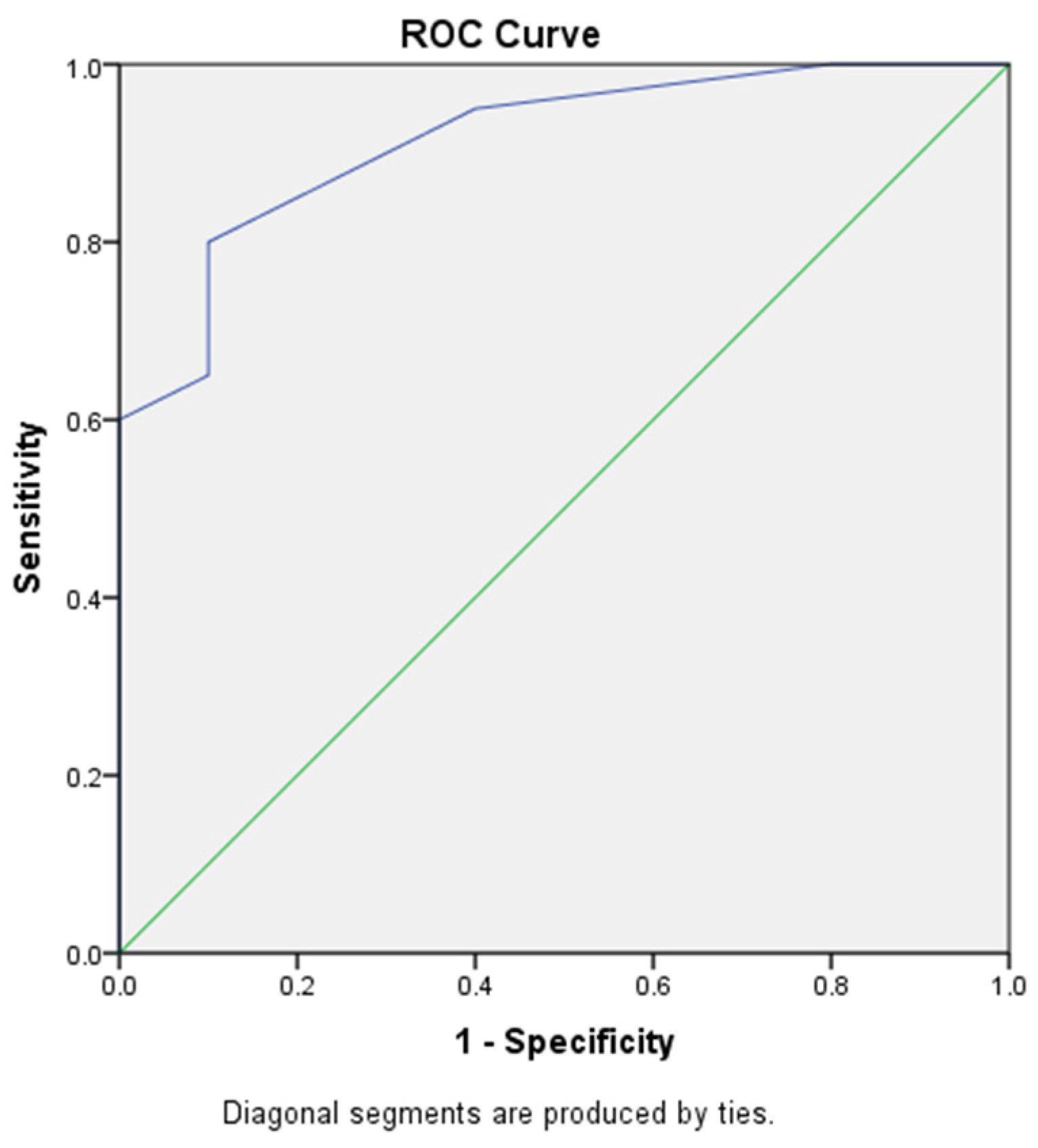
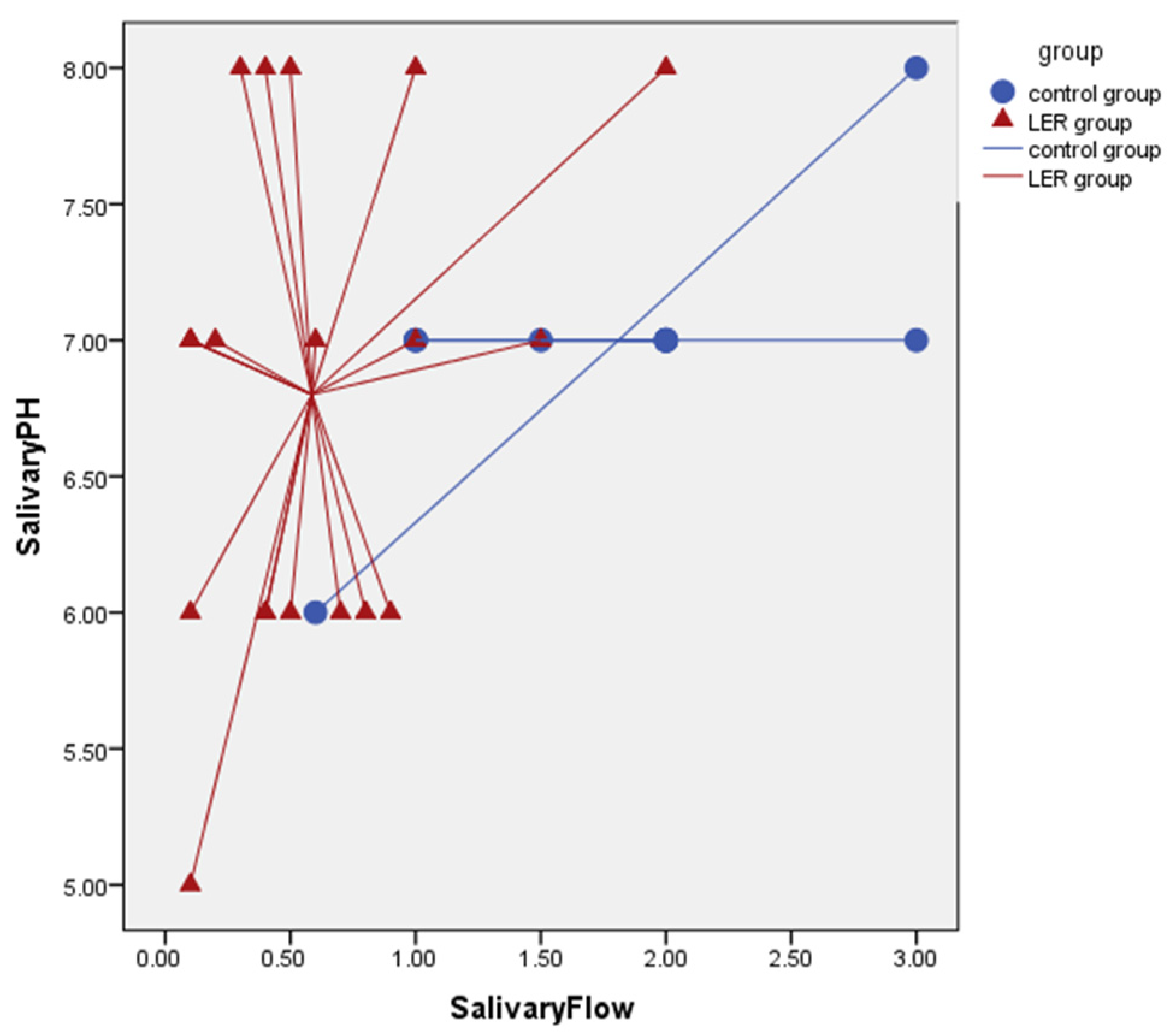
3.3. Salivary Flow Rate Results
4. Discussion
4.1. The Correlation between GER and Dental Disorders
4.2. The Role of LPR in the Development of Dental Disorders
4.3. Preventive Measures for Dental Disorders
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Lechien, J.R.; Akst, L.M.; Hamdan, A.L.; Schindler, A.; Karkos, P.D.; Barillari, M.R.; Calvo-Henriquez, C.; Crevier-Buchman, L.; Finck, C.; Eun, Y.-G.; et al. Evaluation and Management of Laryngopharyngeal Reflux Disease: State of the Art Review. Otolaryngol. Head Neck Surg. 2019, 160, 762–782. [Google Scholar] [CrossRef] [PubMed]
- Morice, D.; Elhassan, H.; Myint-Wilks, L.; Barnett, R.; Rasheed, A.; Collins, H.; Owen, A.; Hughes, K.; Mcleod, R. Laryngopharyngeal reflux: Is laparoscopic fundoplication an effective treatment? Ann. R. Coll. Surg. Engl. 2021. [Google Scholar] [CrossRef] [PubMed]
- Tseng, W.-H.; Hsu, W.-C.; Hsiao, T.-Y.; Wu, J.-F.; Lee, H.-C.; Wang, H.-P.; Wu, M.-S.; Tseng, P.-H. Anatomical and physiological characteristics in patients with Laryngopharyngeal Reflux Symptoms: A case-control study utilizing high-resolution impedance manometry. J. Formos. Med. Assoc. 2021. [Google Scholar] [CrossRef] [PubMed]
- Horvath, L.; Hagmann, P.; Burri, E.; Kraft, M. A novel scoring system for evaluating laryngopharyngeal reflux. Clin. Otolaryngol. 2021, 46, 594–601. [Google Scholar] [CrossRef]
- Bozzani, A.; Grattagliano, I.; Pellegatta, G.; Furnari, M.; Galeone, C.; Savarino, V.; Savarino, E.; De Bastiani, R. Usefulness of Pep-Test for Laryngo-Pharyngeal Reflux: A Pilot Study in Primary Care. Korean J. Fam. Med. 2020, 41, 250–255. [Google Scholar] [CrossRef]
- Masthan, K.; Vinesh, E.; Kumar, M.S.; Jeyapriya, S.M.; Babu, A.; Thinakaran, M. A Clinicopathologic Study of Oral Changes in Gastroesophageal Reflux Disease, Gastritis, and Ulcerative Colitis. J. Contemp. Dent. Pract. 2016, 17, 943–947. [Google Scholar] [CrossRef]
- Gelardi, M.; Ciprandi, G. Focus on gastroesophageal reflux (GER) and laryngopharyngeal reflux (LPR): New pragmatic insights in clinical practice. J. Biol. Regul. Homeost. Agents 2018, 32, 41–47. [Google Scholar]
- Wu, J.-F.; Hsu, W.-C.; Tsai, I.-J.; Tong, T.-W.; Lin, Y.-C.; Yang, C.-H.; Tseng, P.-H. Bolus transit of upper esophageal sphincter on high-resolution impedance manometry study correlate with the laryngopharyngeal reflux symptoms. Sci. Rep. 2021, 11, 20392. [Google Scholar] [CrossRef]
- Rocha, M.O.C.; Cruz, A.A.C.F.; Santos, D.O.; Douglas-De-Oliveira, D.W.; Flecha, O.D.; Gonçalves, P.F. Sensitivity and specificity of assessment scales of dentin hypersensitivity—An accuracy study. Braz. Oral Res. 2020, 34, e043. [Google Scholar] [CrossRef]
- Giraudeau, N.; Camman, P.; Pourreyron, L.; Inquimbert, C.; Lefebvre, P. The contribution of teledentistry in detecting tooth erosion in patients with eating disorders. Digit. Health 2021, 7, 20552076211019250. [Google Scholar] [CrossRef]
- Aránguiz, V.; Lara, J.S.; Marró, M.L.; O’Toole, S.; Ramirez, V.; Bartlett, D. Recommendations and guidelines for dentists using the basic erosive wear examination index (BEWE). Br. Dent. J. 2020, 228, 153. [Google Scholar] [CrossRef] [Green Version]
- Said, O.B.; Razumova, S.; Velichko, E.; Tikhonova, S.; Barakat, H. Evaluation of the Changes of Salivary pH among Dental Students Depending on Their Anxiety Level. Eur. J. Dent. 2020, 14, 605–612. [Google Scholar] [CrossRef] [PubMed]
- Islas-Granillo, H.; Borges-Yáñez, S.A.; Fernández-Barrera, M.; Ávila-Burgos, L.; Patiño-Marín, N.; Márquez-Corona, M.D.L.; Mendoza-Rodríguez, M.; Medina-Solís, C.E. Relationship of hyposalivation and xerostomia in Mexican elderly with socioeconomic, sociodemographic and dental factors. Sci. Rep. 2017, 7, 40686. [Google Scholar] [CrossRef] [PubMed]
- Villa, A.; Connell, C.L.; Abati, S. Diagnosis and management of xerostomia and hyposalivation. Ther. Clin. Risk Manag. 2015, 11, 45. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Iannella, G.; Vicini, C.; Polimeni, A.; Greco, A.; Gobbi, R.; Montevecchi, F.; De Vito, A.; Meccariello, G.; Cammaroto, G.; D’Agostino, G.; et al. Laryngopharyngeal Reflux Diagnosis in Obstructive Sleep Apnea Patients Using the Pepsin Salivary Test. Int. J. Environ. Res. Public Health 2019, 16, 2056. [Google Scholar] [CrossRef] [Green Version]
- Vance, D.; Alnouri, G.; Shah, P.; Ferster, A.P.O.; Lyons, K.; Ross, J.; Sataloff, R.T. The Validity and Reliability of the Reflux Finding Score. J. Voice 2020, 111, 1313–1317. [Google Scholar] [CrossRef]
- Lechien, J.-R.; Mouawad, F.; Bobin, F.; Bartaire, E.; Crevier-Buchman, L.; Saussez, S. Review of management of laryngopharyngeal reflux disease. Eur. Ann. Otorhinolaryngol. Head Neck Dis. 2021, 138, 257–267. [Google Scholar] [CrossRef]
- Wlodarczyk, E.; Domeracka-Kolodziej, A.; Miaskiewicz, B.; Skarzynski, H.; Skarzynski, P.H. A simple qualitative scale for diagnosis of laryngopharyngeal reflux: High correlations with pH measurements and disease severity. The usefulness of the Warsaw Scale in LPR diagnostics compared to other diagnostic tools. Eur. Arch. Oto-Rhino-Laryngol. 2021, 278, 4883–4892. [Google Scholar] [CrossRef]
- Dundar, A.; Sengun, A. Dental approach to erosive tooth wear in gastroesophageal reflux disease. Afr. Health Sci. 2014, 14, 481–486. [Google Scholar] [CrossRef] [Green Version]
- Lechien, J.R.; Chiesa-Estomba, C.M.; Henriquez, C.C.; Mouawad, F.; Ristagno, C.; Barillari, M.R.; Schindler, A.; Nacci, A.; Bouland, C.; Laino, L.; et al. Laryngopharyngeal reflux, gastroesophageal reflux and dental disorders: A systematic review. PLoS ONE 2020, 15, e0237581. [Google Scholar] [CrossRef]
- Stabenau, K.; Johnston, N. How I Approach Laryngopharyngoesophageal Reflux (LPR). Curr. Gastroenterol. Rep. 2021, 23, 27. [Google Scholar] [CrossRef] [PubMed]
- Borysenko, A.; Timokhina, T.; Kononova, O. Indicators of Local Immunity in the Comorbid Course of Caries and Gastroesophageal Reflux Disease. Georgian Med. News 2021, 310, 48–54. [Google Scholar]
- Corrêa, M.C.C.S.F.; Lerco, M.M.; Cunha, M.D.L.R.D.S.D.; Henry, M.A.C.D.A. Salivary parameters and teeth erosions in patients with gastroesophageal reflux disease. Arq. Gastroenterol. 2012, 49, 214–218. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yoshikawa, H.; Furuta, K.; Ueno, M.; Egawa, M.; Yoshino, A.; Kondo, S.; Nariai, Y.; Ishibashi, H.; Kinoshita, Y.; Sekine, J. Oral symptoms including dental erosion in gastroesophageal reflux disease are associated with decreased salivary flow volume and swallowing function. J. Gastroenterol. 2012, 47, 412–420. [Google Scholar] [CrossRef]
- Ciprandi, G.; Passali, D.; Damiani, V.; Mezzedimi, C.; Bellussi, L.M.; Passali, G.C.; Laryngopharyngeal Reflux Study Group. Laryngopharyngeal reflux management in clinical practice. J. Biol. Regul. Homeost. Agents 2021, 35, 55–59. [Google Scholar] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Reflux Symptom Index (RSI) | ||||||
|---|---|---|---|---|---|---|
| Within the last month, how did the following problem affect you? | 0 = No problem to 5 = Severe problem | |||||
| 1. Hoarseness or a problem with your voice | 0 | 1 | 2 | 3 | 4 | 5 |
| 2. Clearing your throat | 0 | 1 | 2 | 3 | 4 | 5 |
| 3. Excess throat mucous or postnasal drip | 0 | 1 | 2 | 3 | 4 | 5 |
| 4. Difficulty swallowing food, liquids, or pills | 0 | 1 | 2 | 3 | 4 | 5 |
| 5. Coughing after you ate or after lying down | 0 | 1 | 2 | 3 | 4 | 5 |
| 6. Breathing difficulties or choking episodes | 0 | 1 | 2 | 3 | 4 | 5 |
| 7. Troublesome or annoying cough | 0 | 1 | 2 | 3 | 4 | 5 |
| 8. Sensations of something sticking in your throat or a lump in your throat | 0 | 1 | 2 | 3 | 4 | 5 |
| 9. Heartburn, chest pain, indigestion, or stomach acid coming up | 0 | 1 | 2 | 3 | 4 | 5 |
| Group A (N = 20) M ± DS or n (%) | Group B (N = 10) M ± DS or n (%) | p Value | |
|---|---|---|---|
| Sex, M | 5 (25) | 1 (10) | 0.326 |
| Age | 44.90 ± 0.34 | 31.90 ± 17.11 | 0.061 |
| RSI | 23.35 ± 5.20 | 3.60 ± 0.34 | 0.0001 |
| Salivary pH | 6.80 ± 0.89 | 7.00 ± 0.47 | 0.515 |
| uSFR | 0.580 ± 0.50 | 1.81 ± 0.80 | 0.001 |
| Pepsin | 18.63 ± 25.03 | 0.00 ± 0.00 | 0.027 |
| SISS | 1.25 ± 0.91 | 0.30 ± 0.48 | 0.001 |
| BEWE | 1.60 ± 0.99 | 0.10 ± 0.31 | 0.0001 |
| DMFT | 8.70 ± 3.73 | 6.00 ± 3.97 | 0.091 |
| VAS | 3.45 ± 2.64 | 0.00 ± 0.00 | 0.0001 |
| Burning mouth | 4 (20) | 0 (0) | 0.177 |
| Xerostomia | 14 (70) | 2 (20) | 0.013 |
| Sialorrhea | 5 (25) | 0 (0) | 0.104 |
| Halitosis | 11 (55) | 1 (10) | 0.021 |
| Dysgeusia | 8 (40) | 0 (0) | 0.022 |
| Hyperesthesia | 15 (75) | 2 (20) | 0.006 |
| Aphthosis | 4 (20) | 0 (0) | 0.177 |
| Soft palate erythema | 5 (25) | 0 (0) | 0.109 |
| Glossitis | 6 (30) | 0 (0) | 0.065 |
| Group A PEP + (N = 12) M ± DS or n (%) | Group A PEP − (N = 8) M ± DS or n (%) | p Value | |
|---|---|---|---|
| Sex, M | 3 (25) | 2 (25) | 0.693 |
| Age | 40.58 ± 17.34 | 51.38 ± 11.25 | 0.139 |
| RSI | 23.67 ± 6.05 | 22.87± 3.94 | 0.727 |
| Salivary pH | 6.58 ± 0.90 | 7.12 ± 0.83 | 0.187 |
| uSFR | 0.60 ± 0.40 | 0.55 ± 0.66 | 0.827 |
| SISS | 1.42 ± 0.90 | 1.00 ± 0.92 | 0.335 |
| BEWE | 1.67± 1.07 | 1.50 ± 0.92 | 0.716 |
| DMFT | 7.50 ± 3.00 | 10.50 ± 4.17 | 0.106 |
| VAS | 3.67 ± 2.77 | 3.13 ± 2.58 | 0.542 |
| Burning mouth | 3 (25) | 1(12.5) | 0.465 |
| Xerostomia | 8 (66.7) | 6 (75.5) | 0.545 |
| Sialorrhea | 4 (33.3) | 1(12.5) | 0.307 |
| Halitosis | 8 (66.7) | 3 (37.5) | 0.205 |
| Dysgeusia | 6 (50.0) | 2 (25.0) | 0.260 |
| Hyperesthesia | 10 (83.3) | 5 (62.5) | 0.295 |
| Aphthosis | 4 (33.3) | 0 (0) | 0.102 |
| Soft palate erythema | 5 (41.7) | 0 (0) | 0.050 |
| Glossitis | 4 (33.3) | 2 (25.0) | 0.545 |
| Sensitivity | Specificity | PPV | NPV | |
|---|---|---|---|---|
| Cutoff < 0.1 | 25.00% | 100.00% | 100.00% | 40.00% |
| ODD | CI 95% | p Value | |
|---|---|---|---|
| Salivary Flow | 0.072 | 0.012–0.472 | 0.004 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Casciaro, S.; Gelardi, M.; Giancaspro, R.; Quaranta, V.N.; Porro, G.; Sterlicchio, B.; Abbinante, A.; Corsalini, M. Dental Disorders and Salivary Changes in Patients with Laryngopharyngeal Reflux. Diagnostics 2022, 12, 153. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics12010153
Casciaro S, Gelardi M, Giancaspro R, Quaranta VN, Porro G, Sterlicchio B, Abbinante A, Corsalini M. Dental Disorders and Salivary Changes in Patients with Laryngopharyngeal Reflux. Diagnostics. 2022; 12(1):153. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics12010153
Chicago/Turabian StyleCasciaro, Sabrina, Matteo Gelardi, Rossana Giancaspro, Vitaliano Nicola Quaranta, Giuseppe Porro, Brigida Sterlicchio, Antonia Abbinante, and Massimo Corsalini. 2022. "Dental Disorders and Salivary Changes in Patients with Laryngopharyngeal Reflux" Diagnostics 12, no. 1: 153. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics12010153