
Impact of Maximum Tongue Pressure in Patients with Jaw Deformities Who Underwent Orthognathic Surgery

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. MTP Measurements
2.3. Statistical Analysis
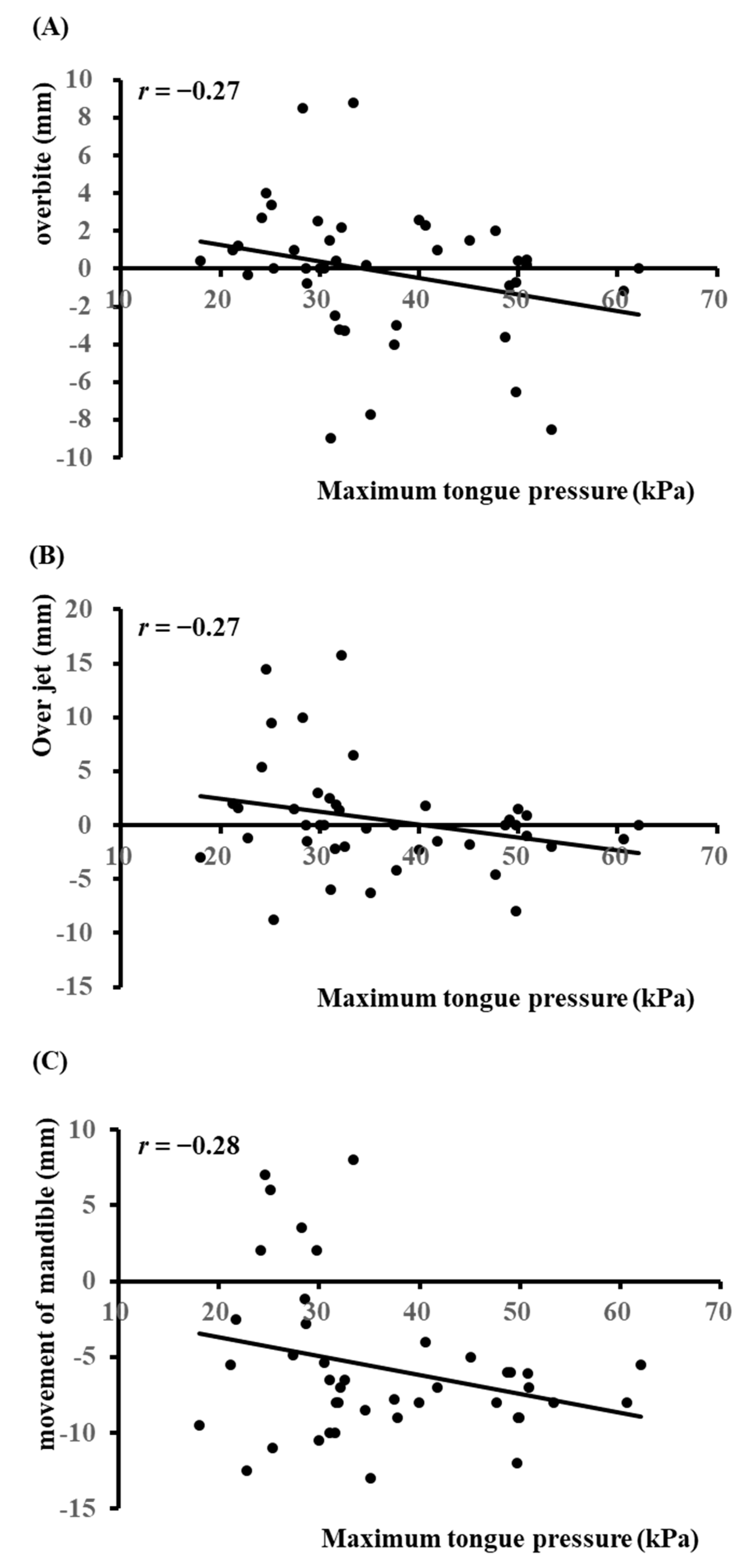
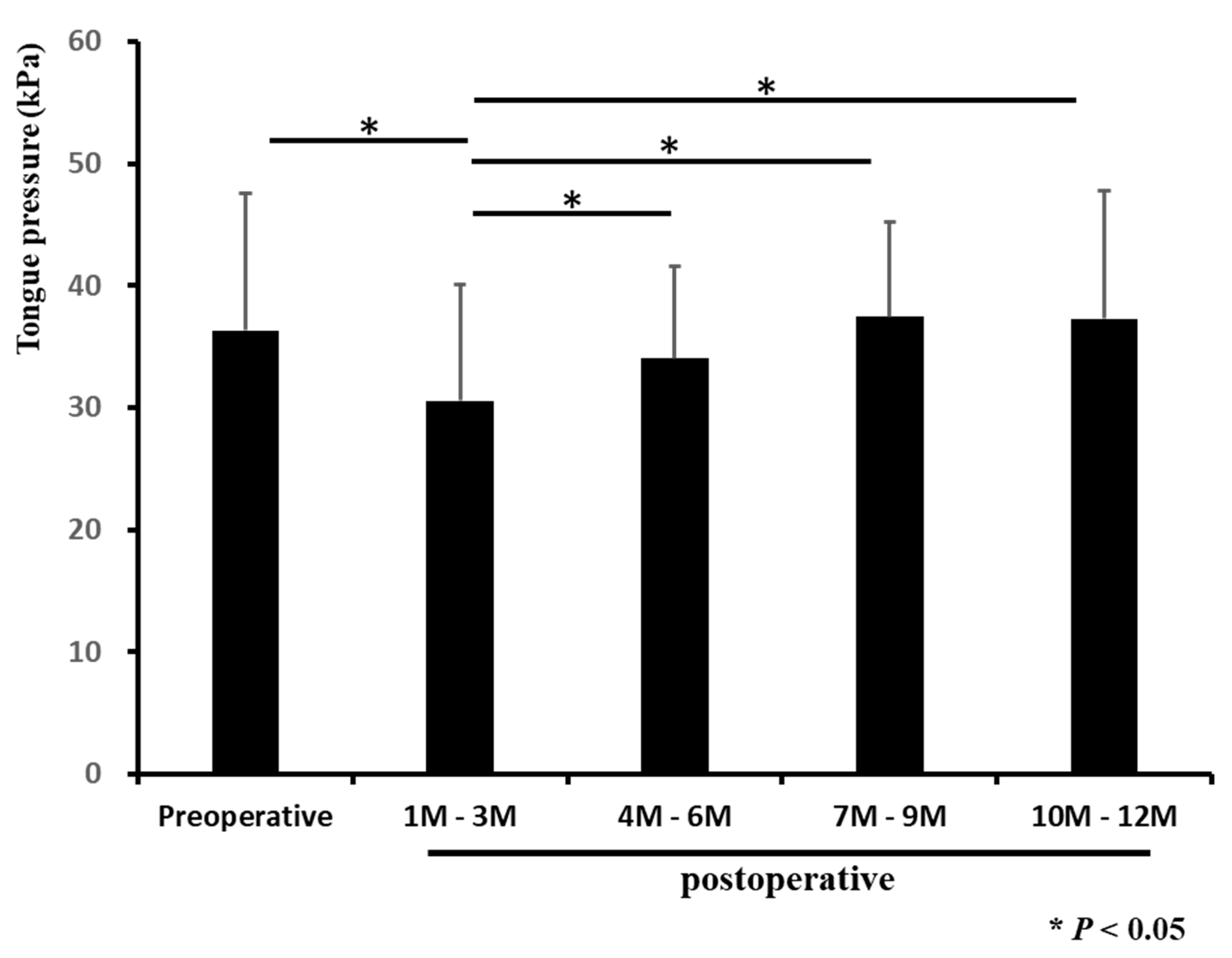
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kobayashi, T.; Honma, K.; Shingaki, S.; Nakajima, T. Changes in masticatory function after orthognathic treatment in patients with mandibular prognathism. Br. J. Oral Maxillofac. Surg. 2001, 39, 260–265. [Google Scholar] [CrossRef] [PubMed]
- Ohkura, K.; Harada, K.; Morishima, S.; Enomoto, S. Changes in bite force and occlusal contact area after orthognathic surgery for correction of mandibular prognathism. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2001, 91, 141–145. [Google Scholar] [CrossRef] [PubMed]
- Ueki, K.; Marukawa, K.; Moroi, A.; Sotobori, M.; Ishihara, Y.; Iguchi, R.; Kohsaka, A.; Nakano, Y.; Higuchi, M.; Nakazawa, R.; et al. The time-course change in the lip closing force in Class III malocclusion after orthognathic surgery. J. Craniomaxillofac. Surg. 2014, 42, 896–900. [Google Scholar] [CrossRef]
- Simpson, W. The results of surgery for mandibular prognathism. Br. J. Oral Surg. 1974, 12, 166–176. [Google Scholar] [CrossRef]
- Howe, G.L. The future of dentistry in the British Isles. Some personal thoughts. Br. Dent. J. 1969, 127, 208–213. [Google Scholar]
- Kobayashi, T.; Watanabe, I.; Ueda, K.; Nakajima, T. Stability of the mandible after sagittal ramus osteotomy for correction of prognathism. J. Oral Maxillofac. Surg. 1986, 44, 693–697. [Google Scholar] [CrossRef]
- Hoppenreijs, T.J.; van der Linden, F.P.; Freihofer, H.P.; van’t Hof, M.A.; Tuinzing, D.B.; Voorsmit, R.A.; Stoelinga, P.J. Occlusal and functional conditions after surgical correction of anterior open bite deformities. Int. J. Adult Orthodon. Orthognath. Surg. 1996, 11, 29–39. [Google Scholar]
- Mizuno, R.; Yamada, K.; Murakami, M.; Kaede, K.; Masuda, Y. Relationship between frontal craniofacial morphology and horizontal balance of lip-closing forces during lip pursing. J. Oral Rehab. 2014, 41, 659–666. [Google Scholar] [CrossRef]
- Kagawa, H.; Kaku, M.; Yamamoto, T.; Yashima, Y.; Sumi, H.; Kamiya, T.; Yamamoto, I.; Tanimoto, K. Changes in tongue-palatal contact during swallowing in patients with skeletal mandibular prognathism after orthognathic surgery. PLoS ONE 2021, 16, e0251759. [Google Scholar] [CrossRef]
- Wickwire, N.A.; White, R.P., Jr.; Proffit, W.R. The effect of mandibular osteotomy on tongue position. J. Oral Surg. 1972, 30, 184–190. [Google Scholar]
- Przygoński, A.; Arkuszewski, P. Evaluation of tongue pressure on the inferior dental arch in patients with mandibular prognathism. Ann. Acad. Med. Stetin. 2006, 52 (Suppl. S3), 131–133. [Google Scholar] [PubMed]
- Sueishi, K.; Yamaguchi, H.; Sebata, M.; Takahashi, S. Changes in oral functions before and after surgical-orthodontic treatment by means of video. Shikwa Gakuho 1988, 88, 905–917. [Google Scholar] [PubMed]
- Shaker, R.; Cook, I.J.; Dodds, W.J.; Hogan, W.J. Pressure-flow dynamics of the oral phase of swallowing. Dysphagia 1988, 3, 79–84. [Google Scholar] [CrossRef] [PubMed]
- Utanohara, Y.; Hayashi, R.; Yoshikawa, M.; Yoshida, M.; Tsuga, K.; Akagawa, Y. Standard values of maximum tongue pressure taken using newly developed disposable tongue pressure measurement device. Dysphagia 2008, 23, 286–290. [Google Scholar] [CrossRef]
- Tsuga, T. The relationship between oral frailty and tongue pressure testing. J. Jpn. Soc. Stomatognath. Funct. 2020, 26, 79–83. [Google Scholar] [CrossRef]
- Sakaue, K.; Fukui, T.; Sasakura, C.; Hori, K.; Ono, T.; Saito, I. Tongue pressure production during swallowing in patients with mandibular prognathism. J. Oral Rehabil. 2016, 43, 348–355. [Google Scholar] [CrossRef]
- Tomita, S.; Takamori, H.; Kobayashi, R.; Karube, K.; Itoh, S.; Mishiro, F.; Katsui, T.; Kumazawa, Y.; Sonoyama, N.; Taniguchi, I.; et al. Tongue pressure and relapse after surgical correction in mandibular prognathism. Jpn. J. Oral Maxillofac. Surg. 1986, 32, 1173–1191. [Google Scholar] [CrossRef] [Green Version]
- Ishikawa, K. Changes of lip and tongue pressures before and after surgical orthodontic correction and their effect on postoperative stability. Tsurumi Shigaku 1988, 14, 449–481. [Google Scholar]
- Dal Pont, G. Retromolar osteotomy for the correction of prognathism. J. Oral Surg. Anesth. Hosp. Dent. Serv. 1961, 19, 42–47. [Google Scholar]
- González-Ulloa, M.; Stevens, E. The role of chin correction in profileplasty. Plast. Reconstr. Surg. 1968, 41, 477–486. [Google Scholar] [CrossRef]
- Yoshikawa, M.; Fukuoka, T.; Mori, T.; Hiraoka, A.; Higa, C.; Kuroki, A.; Takeda, C.; Maruyama, M.; Yoshida, M.; Tsuga, K. Comparison of the Iowa Oral Performance Instrument and JMS tongue pressure measurement device. J. Dent. Sci. 2021, 16, 214–219. [Google Scholar] [CrossRef] [PubMed]
- Minakuchi, S.; Tsuga, K.; Ikebe, K.; Ueda, T.; Tamura, F.; Nagao, K.; Furuya, J.; Matsuo, K.; Yamamoto, K.; Kanazawa, M.; et al. Oral hypofunction in the older population: Position paper of the Japanese Society of Gerodontology in 2016. Gerodontology 2018, 35, 317–324. [Google Scholar] [CrossRef] [PubMed]
- Lambrechts, H.; De Baets, E.; Fieuws, S.; Willems, G. Lip and tongue pressure in orthodontic patients. Eur. J. Orthod. 2010, 32, 466–471. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kieser, J.A.; Farland, M.G.; Jack, H.; Farella, M.; Wang, Y.; Rohrle, O. The role of oral soft tissues in swallowing function: What can tongue pressure tell us? Aust. Dent. J. 2014, 59 (Suppl. S1), 155–161. [Google Scholar] [CrossRef]
- Alexander, C.D. Open bite, dental alveolar protrusion, class I malocclusion: A successful treatment result. Am. J. Orthod. Dentofacial. Orthop. 1999, 116, 494–500. [Google Scholar] [CrossRef]
- Sasakura, C.; Fukui, T.; Saito, I. A Feature of the Deglutition Muscle Activity Form in Patients with Mandibular Prognathism. Jpn. J. Jaw Deformit. 2010, 20, 283–291. [Google Scholar] [CrossRef] [Green Version]
- Cho, H.W.; Kim, I.K.; Cho, H.Y.; Seo, J.H.; Lee, D.H.; Park, S.H. Retrospective study of changes in pharyngeal airway space and position of hyoid bone after mandibular setback surgery by cephalometric analysis. Maxillofac. Plast. Reconstr. Surg. 2015, 37, 38. [Google Scholar] [CrossRef] [Green Version]
- Mark, A.M. Why does my jaw hurt? J. Am. Dent. Assoc. 2019, 150, 12. [Google Scholar] [CrossRef] [Green Version]
- Khosravani, M.R. Mechanical behavior of restorative dental composites under various loading conditions. J. Mech. Behav. Biomed. Mater. 2019, 93. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Total (n = 42) | Low Tongue Pressure b (n = 15) | High Tongue Pressure c (n = 27) | p Value (Low vs. High) | |
|---|---|---|---|---|
| Age (years), median (QRT) | 20 (18, 28.3) | 25 (17.5, 33.5) | 20 (18, 21.5) | 0.1 |
| Gender a (Male/Female) | 12/30 | 5/12 | 7/18 | 0.92 |
| Body mass index (kg/mm2), median (QRT) | 20.6 (19.3, 22.1) | 20.7 (19.4, 21.8) | 20.6 (18.7, 22.7) | 0.94 |
| Over jet (mm), median (QRT) | 0.3 (−2.2, 1.9) | 1.8 (−1.43, 6.23) | −0.65 (−2.15, 0.8) | 0.04 * |
| Overbite (mm), median (QRT) | 0 (−2.0, 1.9) | 1.1 (0, 3.23) | −0.35 (−3.28, 0.88) | 0.01 * |
| Amount of movement d (mm), median (QRT) | −7 (−8.9, −4.9) | −2.75 (−9.5, 2) | −8.5 (−8, −6.1) | 0.03 * |
| Surgical method (cases) | ||||
| SSRO | 42 | |||
| LeFort I | 17 | |||
| tongue reduction | 2 | |||
| Preoperative tongue pressure (kPa), median (QRT) | 32.3 (28.5, 48.0) | 27.2 (23.1, 30.9) | 42.1 (34.3, 50) | <0.001 |
| Postoperative tongue pressure (kPa), median (QRT) | ||||
| 1M–3M (n = 35) | 29.6 (23.2, 37.4) | 23 (17.3, 32.2) | 32.9 (28.3, 40.6) | 0.008 * |
| 4M–6M (n = 21) | 33.4 (30.8, 37.7) | 33.1 (30.4, 36.8) | 37.4 (32.3, 42.2) | 0.07 |
| 7M–9M (n = 17) | 40.1 (32.4, 44.1) | 34.7 (23.3, 41.9) | 41.4 (34.5, 44.1) | 0.15 |
| 10M–12M (n = 22) | 36.8 (31.5, 44.0) | 31.9 (24.6, 36.2) | 42 (35.7, 49.2) | 0.009 * |
| Cephalometric analysis | ||||
| gonial angle (degree), median (QRT) | 127 (122, 134) | 126 (117, 135) | 127 (123, 133) | 0.52 |
| SNA (degree), median (QRT) | 81 (79, 83) | 81.8 (80, 84.5) | 79.9 (78.3, 82.2) | 0.04 * |
| SNB (degree), median (QRT) | 82 (76, 84) | 80.6 (74.6, 83) | 81.7 (77.2, 85.1) | 0.29 |
| ANB (degree), median (QRT) | −0.2 (−2.8, 2.2) | 1.15 (−2.35, 8.08) | −0.8 (−2.75, 0.7) | 0.03 * |
| Interincisal angle (degree), median (QRT) | 128 (117, 136) | 120 (109, 138) | 132 (118, 136) | 0.37 |
| U1 to SN (degree), median (QRT) | 105(99, 111) | 105 (97, 110) | 105 (101, 112) | 0.64 |
| U1 to FH (degree), median (QRT) | 115 (111, 121) | 115 (107, 125) | 115 (112, 119) | 0.8 |
| FMA (degree), median (QRT) | 31 (27, 35) | 31.3 (25.8, 37) | 30.5 (26.8, 33.8) | 0.71 |
| IMPA (degree), median (QRT) | 84 (79, 90) | 85 (75.5, 92.5) | 83.3 (79.8, 89.6) | 1 |
| FMIA (degree), median (QRT) | 63 (58, 70) | 63.2 (49.2, 66.1) | 64.3 (59, 74.9) | 0.24 |
| Preoperative | 1–3M | 4–6M | 7–9M | 10–12M | |
|---|---|---|---|---|---|
| Preoperative | <0.01 | 0.65 | 0.78 | 0.12 | |
| 1–3M | <0.01 | <0.01 | <0.01 | ||
| 4–6M | 0.97 | 0.08 | |||
| 7–9M | 0.38 | ||||
| 10–12M |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Koizumi, K.; Shintani, T.; Yoshimi, Y.; Higaki, M.; Kunimatsu, R.; Yoshioka, Y.; Tsuga, K.; Tanimoto, K.; Shiba, H.; Toratani, S. Impact of Maximum Tongue Pressure in Patients with Jaw Deformities Who Underwent Orthognathic Surgery. Diagnostics 2022, 12, 404. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics12020404
Koizumi K, Shintani T, Yoshimi Y, Higaki M, Kunimatsu R, Yoshioka Y, Tsuga K, Tanimoto K, Shiba H, Toratani S. Impact of Maximum Tongue Pressure in Patients with Jaw Deformities Who Underwent Orthognathic Surgery. Diagnostics. 2022; 12(2):404. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics12020404
Chicago/Turabian StyleKoizumi, Koichi, Tomoaki Shintani, Yuki Yoshimi, Mirai Higaki, Ryo Kunimatsu, Yukio Yoshioka, Kazuhiro Tsuga, Kotaro Tanimoto, Hideki Shiba, and Shigeaki Toratani. 2022. "Impact of Maximum Tongue Pressure in Patients with Jaw Deformities Who Underwent Orthognathic Surgery" Diagnostics 12, no. 2: 404. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics12020404