
Altered TIMP-3 Levels in the Cerebrospinal Fluid and Plasma of Patients with Alzheimer’s Disease


 ,
,
Abstract
:1. Introduction
2. Material & Methods
2.1. Human Blood Samples
2.2. CSF Sampling
2.3. Cell Cultures
2.4. Animals
2.5. Antibodies and Reagents
2.6. Measurement of Blood Proteins by ELISA
2.7. Western Blotting
2.8. Real-Time Reverse Transcription Polymerase Chain Reaction
2.9. Immunofluorescence Assay
2.10. Statistical Analyses
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Mudher, A.; Lovestone, S. Alzheimer’s Disease–Do tauists and baptists finally shake hands? Trends Neurosci. 2002, 25, 22–26. [Google Scholar] [CrossRef]
- Selkoe, D.J. Alzheimer’s disease: Genes, proteins, and therapy. Physiol. Rev. 2001, 81, 741–766. [Google Scholar] [CrossRef] [PubMed]
- Prince, M. Alzheimer’s disease facts and figures. Alzheimers Dement 2018, 14, 367–429. [Google Scholar]
- Lorenzl, S.; Albers, D.S.; Relkin, N.; Ngyuen, T.; Hilgenberg, S.L.; Chirichigno, J.; Cudkowicz, M.E.; Beal, M.F. Increased plasma levels of matrix metalloproteinase-9 in patients with Alzheimer’s disease. Neurochem. Int. 2003, 43, 191–196. [Google Scholar] [CrossRef]
- Jiang, T.; Chang, R.C.-C.; Rosenmann, H.; Yu, J.-T. Advances in Alzheimer’s disease: From bench to bedside. BioMed Res. Int. 2015, 2015, 202676. [Google Scholar] [CrossRef] [PubMed]
- Kojro, E.; Fahrenholz, F. The non-amyloidogenic pathway: Structure and function of α-secretases. Alzheimer’s Dis. 2005, 38, 105–127. [Google Scholar]
- Vatanabe, I.P.; Peron, R.; Grigoli, M.M.; Pelucchi, S.; De Cesare, G.; Magalhães, T.; Manzine, P.; Balthazar, M.F.; Di Luca, M.; Marcello, E.; et al. ADAM10 Plasma and CSF Levels Are Increased in Mild Alzheimer’s Disease. Int. J. Mol. Sci. 2021, 22, 2416. [Google Scholar] [CrossRef]
- Lorenzl, S.; Buerger, K.; Hampel, H.; Beal, M.F. Profiles of matrix metalloproteinases and their inhibitors in plasma of patients with dementia. Int. Psychogeriatr. 2008, 20, 67–76. [Google Scholar] [CrossRef]
- Backstrom, J.R.; Lim, G.P.; Cullen, M.J.; Tokes, Z.A. Matrix metalloproteinase-9 (MMP-9) is synthesized in neurons of the human hippocampus and is capable of degrading the amyloid-beta peptide (1–40). J. Neurosci. 1996, 16, 7910–7919. [Google Scholar] [CrossRef] [Green Version]
- Arpino, V.; Brock, M.; Gill, S.E. The role of TIMPs in regulation of extracellular matrix proteolysis. Matrix Biol. 2015, 44, 247–254. [Google Scholar] [CrossRef]
- Köhrmann, A.; Kammerer, U.; Kapp, M.; Dietl, J.; Anacker, J. Expression of matrix metalloproteinases (MMPs) in primary human breast cancer and breast cancer cell lines: New findings and review of the literature. BMC Cancer 2009, 9, 188. [Google Scholar] [CrossRef] [Green Version]
- Bauer, Y.; White, E.S.; de Bernard, S.; Cornelisse, P.; Leconte, I.; Morganti, A.; Roux, S.; Nayler, O. MMP-7 is a predictive biomarker of disease progression in patients with idiopathic pulmonary fibrosis. ERJ Open Res. 2017, 3, 00074-2016. [Google Scholar] [CrossRef] [Green Version]
- Halade, G.V.; Jin, Y.-F.; Lindsey, M.L. Matrix metalloproteinase (MMP)-9: A proximal biomarker for cardiac remodeling and a distal biomarker for inflammation. Pharmacol. Ther. 2013, 139, 32–40. [Google Scholar] [CrossRef] [Green Version]
- Kelly, P.J.; Morrow, J.D.; Ning, M.; Koroshetz, W.; Lo, E.H.; Terry, E.; Milne, G.L.; Hubbard, J.; Lee, H.; Stevenson, E. Oxidative stress and matrix metalloproteinase-9 in acute ischemic stroke: The Biomarker Evaluation for Antioxidant Therapies in Stroke (BEAT-Stroke) study. Stroke 2008, 39, 100–104. [Google Scholar] [CrossRef] [Green Version]
- Su, C.-W.; Lin, C.-W.; Yang, W.-E.; Yang, S.-F. TIMP-3 as a therapeutic target for cancer. Ther. Adv. Med. Oncol. 2019, 11, 1758835919864247. [Google Scholar] [CrossRef] [Green Version]
- Lorenzl, S.; Albers, D.; LeWitt, P.; Chirichigno, J.; Hilgenberg, S.; Cudkowicz, M.; Beal, M. Tissue inhibitors of matrix metalloproteinases are elevated in cerebrospinal fluid of neurodegenerative diseases. J. Neurol. Sci. 2003, 207, 71–76. [Google Scholar] [CrossRef]
- Walker, E.J.; Rosenberg, G.A. TIMP-3 and MMP-3 contribute to delayed inflammation and hippocampal neuronal death following global ischemia. Exp. Neurol. 2009, 216, 122–131. [Google Scholar] [CrossRef] [Green Version]
- Bjerke, M.; Zetterberg, H.; Edman, A.; Blennow, K.; Wallin, A.; Andreasson, U. Cerebrospinal fluid matrix metalloproteinases and tissue inhibitor of metalloproteinases in combination with subcortical and cortical biomarkers in vascular dementia and Alzheimer’s disease. J. Alzheimer’s Dis. 2011, 27, 665–676. [Google Scholar] [CrossRef]
- Tuna, G.; Yener, G.G.; Oktay, G.; Işlekel, G.H.; Kİrkalİ, F.G. Evaluation of Matrix Metalloproteinase-2 (MMP-2) and -9 (MMP-9) and Their Tissue Inhibitors (TIMP-1 and TIMP-2) in Plasma from Patients with Neurodegenerative Dementia. J. Alzheimer’s Dis. 2018, 66, 1265–1273. [Google Scholar] [CrossRef]
- Basu, R.; Fan, D.; Kandalam, V.; Lee, J.; Das, S.K.; Wang, X.; Baldwin, T.A.; Oudit, G.Y.; Kassiri, Z. Loss of Timp3 gene leads to abdominal aortic aneurysm formation in response to angiotensin II. J. Biol. Chem. 2012, 287, 44083–44096. [Google Scholar] [CrossRef] [Green Version]
- Gooz, M. ADAM-17: The enzyme that does it all. Crit. Rev. Biochem. Mol. Biol. 2010, 45, 146–169. [Google Scholar] [CrossRef] [Green Version]
- Dewing, J.M.; Carare, R.O.; Lotery, A.J.; Ratnayaka, J.A. The Diverse Roles of TIMP-3: Insights into degenerative diseases of the senescent retina and brain. Cells 2019, 9, 39. [Google Scholar] [CrossRef] [Green Version]
- Hoe, H.-S.; Cooper, M.J.; Burns, M.P.; Lewis, P.; Van Der Brug, M.; Chakraborty, G.; Cartagena, C.M.; Pak, D.T.S.; Cookson, M.R.; Rebeck, G.W. The metalloprotease inhibitor TIMP-3 regulates amyloid precursor protein and apolipoprotein E receptor proteolysis. J. Neurosci. 2007, 27, 10895–10905. [Google Scholar] [CrossRef] [Green Version]
- Manousopoulou, A.; Gatherer, M.; Smith, C.; Nicoll, J.; Woelk, C.H.; Johnson, M.; Kalaria, R.; Attems, J.; Garbis, S.; Carare, R.O. Systems proteomic analysis reveals that clusterin and tissue inhibitor of metalloproteinases 3 increase in leptomeningeal arteries affected by cerebral amyloid angiopathy. Neuropathol. Appl. Neurobiol. 2017, 43, 492–504. [Google Scholar] [CrossRef]
- Cho, S.-J.; Park, M.H.; Han, C.; Yoon, K.; Koh, Y.H. VEGFR2 alteration in Alzheimer′s disease. Sci. Rep. 2017, 7, 17713. [Google Scholar] [CrossRef] [Green Version]
- Qi, J.H.; Ebrahem, Q.; Moore, N.; Murphy, G.; Claesson-Welsh, L.; Bond, M.; Baker, A.; Anand-Apte, B. A novel function for tissue inhibitor of metalloproteinases-3 (TIMP3): Inhibition of angiogenesis by blockage of VEGF binding to VEGF receptor-2. Nat. Med. 2003, 9, 407–415. [Google Scholar] [CrossRef]
- Petersen, R.C.; Smith, G.E.; Waring, S.C.; Ivnik, R.J.; Tangalos, E.G.; Kokmen, E. Mild cognitive impairment: Clinical characterization and outcome. Arch. Neurol. 1999, 56, 303–308. [Google Scholar] [CrossRef]
- Han, C.; Jo, S.A.; Kim, N.H.; Jo, I.; Park, M.H. Study design and methods of the Ansan Geriatric Study (AGE study). BMC Neurol. 2009, 9, 10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sun, Q.; Hampel, H.; Blennow, K.; Lista, S.; Levey, A.; Tang, B.; Li, R.; Shen, Y. Increased plasma TACE activity in subjects with mild cognitive impairment and patients with Alzheimer’s disease. J. Alzheimer’s Dis. 2014, 41, 877–886. [Google Scholar] [CrossRef] [Green Version]
- McKhann, G.; Drachman, D.; Folstein, M.; Katzman, R.; Price, D.; Stadlan, E.M. Clinical diagnosis of Alzheimer’s disease: Report of the NINCDS-ADRDA Work Group* under the auspices of Department of Health and Human Services Task Force on Alzheimer’s Disease. Neurology 1984, 34, 939. [Google Scholar] [CrossRef] [Green Version]
- Lee, J.H.; Lee, K.U.; Lee, D.Y.; Kim, K.W.; Jhoo, J.H.; Kim, J.H.; Lee, K.H.; Kim, S.Y.; Han, S.H.; Woo, J.I. Development of the Korean version of the Consortium to Establish a Registry for Alzheimer’s Disease Assessment Packet (CERAD-K): Clinical and neuropsychological assessment batteries. J. Gerontol. 2002, 57, 47–53. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jang, B.G.; Yun, S.-M.; Ahn, K.; Song, J.H.; Jo, S.A.; Kim, Y.-Y.; Kim, D.K.; Park, M.H.; Han, C.; Koh, Y.H. Plasma carbonic anhydrase II protein is elevated in Alzheimer’s disease. J. Alzheimer’s Dis. 2010, 21, 939–945. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.; Park, M.H.; Kim, E.; Han, C.; Jo, S.A.; Jo, I. Plasma homocysteine is associated with the risk of mild cognitive impairment in an elderly Korean population. J. Nutr. 2007, 137, 2093–2097. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jung, N.-Y.; Kim, E.S.; Kim, H.-S.; Jeon, S.; Lee, M.J.; Pak, K.; Lee, J.-H.; Lee, Y.M.; Lee, K.; Shin, J.-H.; et al. Comparison of diagnostic performances between cerebrospinal fluid biomarkers and amyloid PET in a clinical setting. J. Alzheimer’s Dis. 2020, 74, 473–490. [Google Scholar] [CrossRef]
- Kang, Y.; Na, D.; Hahn, S. Seoul Neuropsychological Screening Battery; Human Brain Research & Consulting Co.: Incheon, Korea, 2003. [Google Scholar]
- Albert, M.S.; DeKosky, S.T.; Dickson, D.; Dubois, B.; Feldman, H.H.; Fox, N.C.; Gamst, A.; Holtzman, D.M.; Jagust, W.J.; Petersen, R.C.; et al. The diagnosis of mild cognitive impairment due to Alzheimer’s disease: Recommendations from the National Institute on Aging-Alzheimer’s Association workgroups on diagnostic guidelines for Alzheimer’s disease. Alzheimer’s Dement. 2011, 7, 270–279. [Google Scholar] [CrossRef] [Green Version]
- McKhann, G.M.; Knopman, D.S.; Chertkow, H.; Hyman, B.T.; Jack, J.C.R.; Kawas, C.H.; Klunk, W.E.; Koroshetz, W.J.; Manly, J.J.; Mayeux, R. The diagnosis of dementia due to Alzheimer’s disease: Recommendations from the National Institute on Aging-Alzheimer’s Association workgroups on diagnostic guidelines for Alzheimer’s disease. Alzheimer’s Dement. 2011, 7, 263–269. [Google Scholar] [CrossRef] [Green Version]
- Cho, S.-J.; Yun, S.-M.; Jo, C.; Lee, D.-h.; Choi, K.J.; Song, J.C.; Park, S.I.; Kim, Y.-J.; Koh, Y.H. SUMO1 promotes Aβ production via the modulation of autophagy. Autophagy 2014, 11, 100–112. [Google Scholar] [CrossRef] [Green Version]
- Ylisirnio, S.; Hoyhtya, M.; Turpeenniemi-Hujanen, T. Serum matrix metalloproteinases -2, -9 and tissue inhibitors of metalloproteinases -1, -2 in lung cancer--TIMP-1 as a prognostic marker. Anticancer. Res. 2000, 20, 1311–1316. [Google Scholar]
- Wu, Z.-S.; Wu, Q.; Yang, J.-H.; Wang, H.-Q.; Ding, X.-D.; Yang, F.; Xu, X.-C. Prognostic significance of MMP-9 and TIMP-1 serum and tissue expression in breast cancer. Int. J. Cancer 2008, 122, 2050–2056. [Google Scholar] [CrossRef]
- Cuadrado, E.; Rosell, A.; Penalba, A.; Slevin, M.; Alvarez-Sabin, J.; Ortega-Aznar, A.; Montaner, J. Vascular MMP-9/TIMP-2 and neuronal MMP-10 up-regulation in human brain after stroke: A combined laser microdissection and protein array study. J. Proteome Res. 2009, 8, 3191–3197. [Google Scholar] [CrossRef]
- Jaroslav, P.; Christian, R.; Stefan, O.; Alexander, Z.; Zepper, P.; Holger, P.; Hans-Henning, E. Evaluation of serum biomarkers for patients at increased risk of stroke. Int. J. Vasc. Med. 2012, 2012, 1–6. [Google Scholar] [CrossRef] [Green Version]
- Su, C.-W.; Su, B.-F.; Chiang, W.-L.; Yang, S.-F.; Chen, M.-K.; Lin, C.-W. Plasma levels of the tissue inhibitor matrix metalloproteinase-3 as a potential biomarker in oral cancer progression. Int. J. Med. Sci. 2017, 14, 37–44. [Google Scholar] [CrossRef] [Green Version]
- Hendrickson, C.M.; Gibb, S.L.; Miyazawa, B.Y.; Keating, S.; Ross, E.; Conroy, A.S.; Calfee, C.S.; Pati, S.; Cohen, M.J. Elevated plasma levels of TIMP-3 are associated with a higher risk of acute respiratory distress syndrome and death following severe isolated traumatic brain injury. Trauma Surg. Acute Care Open 2018, 3, e000171. [Google Scholar] [CrossRef]
- Cymbaluk-Płoska, A.; Chudecka-Głaz, A.; Pius-Sadowska, E.; Machaliński, B.; Menkiszak, J.; Sompolska-Rzechuła, A. Suitability assessment of baseline concentration of MMP3, TIMP3, HE4 and CA125 in the serum of patients with ovarian cancer. J. Ovarian Res. 2018, 11, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Stomrud, E.; Björkqvist, M.; Janciauskiene, S.; Minthon, L.; Hansson, O. Alterations of matrix metalloproteinases in the healthy elderly with increased risk of prodromal Alzheimer’s disease. Alzheimer’s Res. Ther. 2010, 2, 20. [Google Scholar] [CrossRef] [Green Version]
- Allinson, T.M.J.; Parkin, E.; Condon, T.P.; Schwager, S.L.U.; Sturrock, E.D.; Turner, A.J.; Hooper, N.M. The role of ADAM10 and ADAM17 in the ectodomain shedding of angiotensin converting enzyme and the amyloid precursor protein. JBIC J. Biol. Inorg. Chem. 2004, 271, 2539–2547. [Google Scholar] [CrossRef]
- Skovronsky, D.M.; Fath, S.; Lee, V.M.-Y.; Milla, M.E. Neuronal localization of the TNF? converting enzyme (TACE) in brain tissue and its correlation to amyloid plaques. J. Neurobiol. 2001, 49, 40–46. [Google Scholar] [CrossRef]
- Attems, J.; Lauda, F.; A Jellinger, K. Unexpectedly low prevalence of intracerebral hemorrhages in sporadic cerebral amyloid angiopathy. J. Neurol. 2008, 255, 70–76. [Google Scholar] [CrossRef]
- Mandybur, T.I. The incidence of cerebral amyloid angiopathy in Alzheimer’s disease. Neurology 1975, 25, 120-6. [Google Scholar] [CrossRef]
- Zarow, C.; Zaias, B.; A Lyness, S.; Chui, H. Cerebral amyloid angiopathy in Alzheimer disease is associated with apolipoprotein E4 and cortical neuron loss. Alzheimer Dis. Assoc. Disord. 1999, 13, 1–8. [Google Scholar] [CrossRef]
- Monet-Leprêtre, M.; Haddad, I.; Baron-Menguy, C.; Fouillot-Panchal, M.; Riani, M.; Domenga-Denier, V.; Dussaule, C.; Cognat, E.; Vinh, J.; Joutel, A. Abnormal recruitment of extracellular matrix proteins by excess Notch3ECD: A new pathomechanism in CADASIL. Brain 2013, 136, 1830–1845. [Google Scholar] [CrossRef] [Green Version]
- Zellner, A.; Scharrer, E.; Arzberger, T.; Oka, C.; Domenga-Denier, V.; Joutel, A.; Lichtenthaler, S.F.; Müller, S.A.; Dichgans, M.; Haffner, C. CADASIL brain vessels show a HTRA1 loss-of-function profile. Acta Neuropathol. 2018, 136, 111–125. [Google Scholar] [CrossRef]
- Jäkel, L.; Kuiperij, H.B.; Gerding, L.P.; Custers, E.E.M.; Berg, E.V.D.; Jolink, W.M.T.; Schreuder, F.H.B.M.; Küsters, B.; Klijn, C.J.M.; Verbeek, M.M. Disturbed balance in the expression of MMP9 and TIMP3 in cerebral amyloid angiopathy-related intracerebral haemorrhage. Acta Neuropathol. Commun. 2020, 8, 1–14. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Features | Control | MCI | Dementia | p-Value |
|---|---|---|---|---|
| N (Male/Female) | 115 (48/67) | 71 (29/42) | 65 (16/49) | |
| Age (years) | 71.9 ± 0.43 | 73.05 ± 0.54 | 75.1 ± 0.75 | 0.001 |
| Education | 9.12 ± 0.47 | 6.18 ± 0.57 | 3.56 ± 0.55 | <0.001 |
| MMSE | 27.21 ± 0.2 | 24.96 ± 0.35 | 16.0 ± 0.73 | <0.001 |
| CDR | 0.043 ± 0.01 | 0.26 ± 0.02 | 1.12 ± 0.09 | <0.001 |
| Total CHOL | 195.6 ± 3.2 | 190.3 ± 4.1 | 201.4 ± 4.5 | 0.306 |
| TG | 137.4 ± 7.2 | 127.9 ± 7.7 | 152.6 ± 11.5 | 0.287 |
| HDL | 43.4 ± 0.89 | 43.1 ± 1.46 | 44.5 ± 1.2 | 0.371 |
| LDL | 124.7 ± 3.0 | 121.5 ± 3.4 | 126.4 ± 3.8 | 0.599 |
| Platelet | 253.3 ± 6.6 | 268.0 ± 7.2 | 266.2 ± 11.3 | 0.229 |
| Glucose | 101.4 ± 2.0 | 102.3 ± 2.5 | 107.5 ± 5.1 | 0.483 |
| vitB12 | 790.6 ± 57.3 | 699.2 ± 31.6 | 717.1 ± 41.3 | 0.903 |
| TIMP-3 (ng/mL) | 0.61 ± 0.06 | 0.40 ± 0.04 | 0.39 ± 0.05 a | 0.065 |
| Features | TIMP-3 | |
|---|---|---|
| Rho | p-Value | |
| Age | −0.112 | 0.075 |
| Education | 0.094 | 0.14 |
| MMSE | 0.104 | 0.099 |
| CDR | −0.153 | 0.015 |
| Total CHOL | −0.105 | 0.096 |
| Tg | 0.008 | 0.902 |
| HDL | −0.049 | 0.442 |
| LDL | −0.142 | 0.025 |
| Platelet | 0.038 | 0.55 |
| Glucose | −0.127 | 0.046 |
| VitB12 | 0.079 | 0.21 |
| Features | Control | MCI | ADD | p-Value |
|---|---|---|---|---|
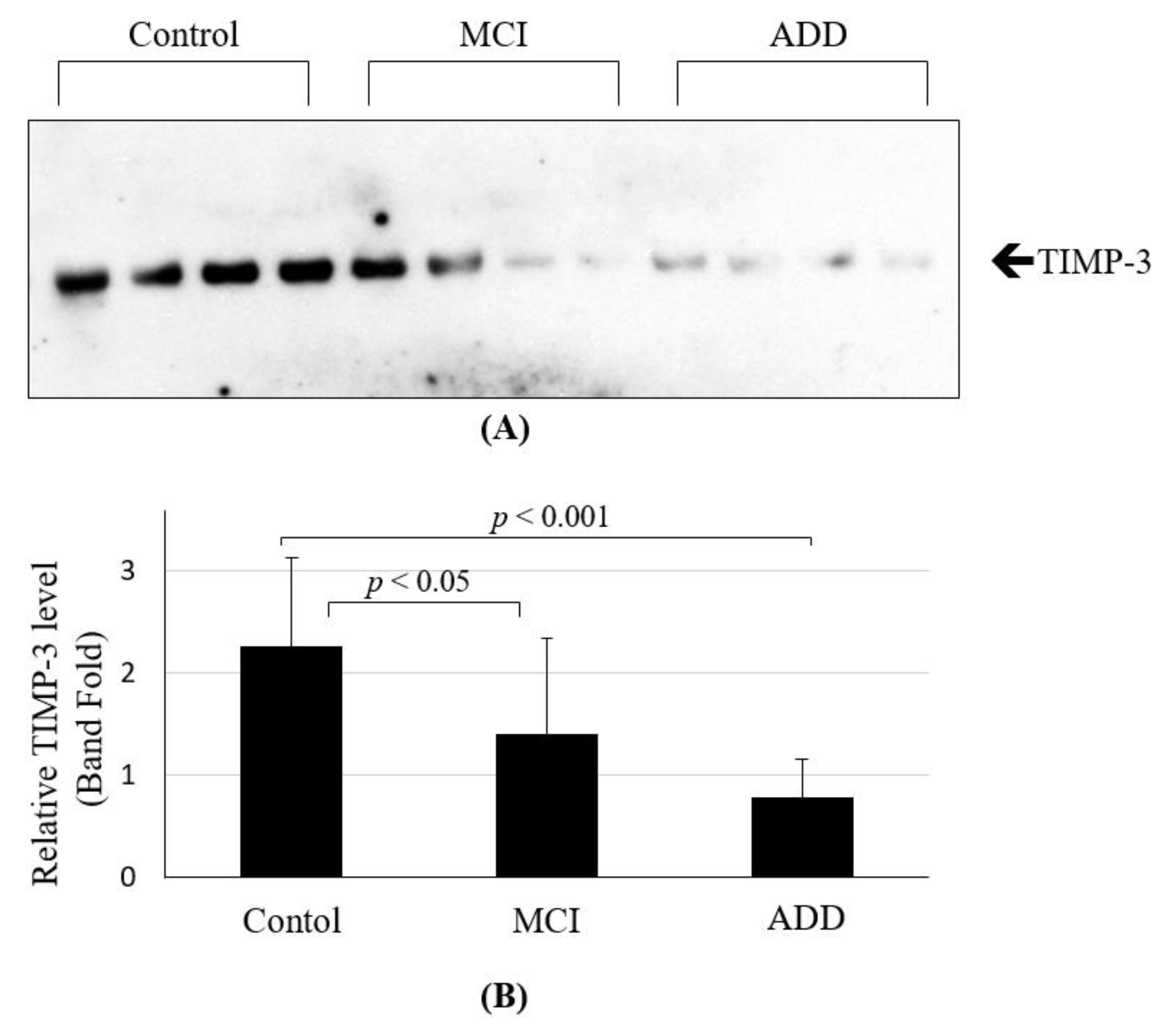
| TIMP-3 | 2.26 ± 0.26 | 1.40 ± 0.29 1 | 0.77 ± 0.11 | 0.004 |
| Aβ1-42 (pg/mL) | 1030.1 ± 32.6 | 766.3 ± 70.9 2 | 401.3 ± 27.4 3 | <0.001 |
| Total Tau (pg/mL) | 224.3 ± 25.6 | 328.9 ± 69.5 | 480.8 ± 100.7 | 0.092 |
| pTau (pg/mL) | 50.3 ± 2.4 | 41.2 ± 4.5 | 81.5 ± 9.3 4 | 0.001 |
| Features | TIMP-3 | |
|---|---|---|
| Rho | p-Value | |
| Age | −0.25 | 0.17 |
| Aβ1-42 | 0.515 | 0.004 |
| Total Tau | −0.337 | 0.069 |
| pTau | −0.372 | 0.047 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Park, J.H.; Cho, S.-J.; Jo, C.; Park, M.H.; Han, C.; Kim, E.-J.; Huh, G.Y.; Koh, Y.H. Altered TIMP-3 Levels in the Cerebrospinal Fluid and Plasma of Patients with Alzheimer’s Disease. J. Pers. Med. 2022, 12, 827. https://0-doi-org.brum.beds.ac.uk/10.3390/jpm12050827
Park JH, Cho S-J, Jo C, Park MH, Han C, Kim E-J, Huh GY, Koh YH. Altered TIMP-3 Levels in the Cerebrospinal Fluid and Plasma of Patients with Alzheimer’s Disease. Journal of Personalized Medicine. 2022; 12(5):827. https://0-doi-org.brum.beds.ac.uk/10.3390/jpm12050827
Chicago/Turabian StylePark, Jung Hyun, Sun-Jung Cho, Chulman Jo, Moon Ho Park, Changsu Han, Eun-Joo Kim, Gi Yeong Huh, and Young Ho Koh. 2022. "Altered TIMP-3 Levels in the Cerebrospinal Fluid and Plasma of Patients with Alzheimer’s Disease" Journal of Personalized Medicine 12, no. 5: 827. https://0-doi-org.brum.beds.ac.uk/10.3390/jpm12050827