Thermophysiological Comfort of Surgeons and Patient in an Operating Room Based on PMV-PPD and PHS Indexes


1
Department of Textiles, Technical University of Sofia, 1000 Sofia, Bulgaria
2
Department of Hydroaerodynamics and Hydraulic Machines, Technical University of Sofia, 1000 Sofia, Bulgaria
*
Author to whom correspondence should be addressed.
Appl. Sci. 2020, 10(5), 1801; https://0-doi-org.brum.beds.ac.uk/10.3390/app10051801
Submission received: 14 January 2020
/
Revised: 17 February 2020
/
Accepted: 2 March 2020
/
Published: 5 March 2020
(This article belongs to the Special Issue Thermal Comfort and Indoor Air Quality in the 2021 Built Environment)
Abstract
:There are different actors in an operating room (OR), who have controversial requirements for the indoor thermal environment. While the patient is at risk of perioperative hypothermia, the surgeons are in a state of thermophysiological discomfort. The study presents an analysis of the thermophysiological comfort of both patient and surgeons in an OR. Surgical clothing ensembles with three values of clothing insulation are simulated. Different indoor environment conditions (air temperature and relative humidity) are tested. The analysis is based on the calculation of predicted mean vote and predicted percentage of dissatisfied (PMV-PPD) indexes and assessment of the climatic conditions categories. Discussion of the predicted heat strain is also presented. The simulated results and their analysis show considerable discrepancies between the thermophysiological comfort of the patient and the surgeons, even when dressed in a light protective ensemble, in the same indoor environment.
1. Introduction
The indoor environmental conditions in an operating room (OR) are usually designed to satisfy the patients’ comfort and health [1]. The International Standard ISO 7730 [2], which deals with the specification of the conditions for thermal comfort, does not make a difference between types of indoor spaces in terms of thermal comfort. Therefore, any OR has to meet the requirements of this standard, similar to office premises or a theatre hall.
The thermophysiological comfort of people in the indoor environment depends on three groups of factors [3]:
- Environmental factors: air temperature, mean radiant temperature, relative air humidity, air movement (air velocity);
- Factors related to the state of the human body: thermoregulation mechanism, central nervous system, cardiovascular system, respiratory system, skeletal-muscular system, digestive system;
- Factors related to clothing/textiles as a barrier between the body and the environment: insulating ability (resistance to heat transfer), air permeability, water vapour permeability, water repellency, drying rate.
The patient in the OR stays together with the medical staff, which involves different actors: surgeons, anaesthetists, nurses, assistants. The thermophysiological comfort of everyone has to be satisfied in order to assure their high-quality performance during the operation (for the staff) or their health (for the patient). Though the staff and the patient occupy the same indoor environment, all three groups of factors that define their thermophysiological comfort differ.
The most significant difference between the staff and the patient is the clothing: the patient is usually necked and covered with a surgical drape, while the medical staff wears protective clothing. The original function of surgical clothing was to protect the patient in the OR from a possible impact of the surgical team. Later on, having the results from the studies on the dangers associated with blood-borne pathogens, the role of the surgical clothing changed: the need to protect the surgeons from the patient was added to the need to protect the surgeons from the patient himself [3]. Furthermore, the clothing of the surgeons and the surgical nurses differs from the clothing of the anaesthetists and the technicians who may handle specific medical equipment in the OR.
The factors related to the state of the human body are also different. Тhe patient is lying down under anaesthesia, his/her thermoregulatory mechanism is inhibited with increased risk for perioperative hypothermia, the body is under stress and internal organs and body tissues are exposed to the environment with possible blood losses. At the same time, behavioural responses to thermal discomfort are impossible. Meanwhile, the medical staff are standing; the surgeons work stationarily around the operating table, while the nurses and the anesthesiologist can move slightly. The mental load and physical stress for the staff are also different, being most heavy for the surgeons [4,5].
The environmental factors in the OR also differ: it was found that in the area just below the operating lamps, due to the radiation heat, the air temperature is higher on average by 3 °C than the rest of the OR [6].
Obviously, there is a conflict in the requirements for the thermal environment in the OR. Even though the heating, ventilation and air-conditioning system in the OR provides standard comfort conditions (20–22 °C, 65% relative humidity) [2], it is likely that only nurses and anaesthetists will be able to determine the thermal environment as comfortable. In cases where there is no individual system or device (blanket) for warming the patient, the air temperature in the OR should not be below 23 °C [4] or even higher than 24 °C [7]. At the same time, the air temperature for the surgeons in heavy protective gowns during extended operations is suggested to be lower than 18 °C [7].
The technical standards for the indoor environmental in an OR were summarized in [5]. It was found that significant discrepancies exist between the HVAC (Heating, Ventilation and Air Conditioning) standards and the actual thermophysiological comfort of both the surgical team and the patient. Several studies dedicated to the topic [4,5,7,8,9,10] have found that it might be difficult to find out a general solution for the problem, having in mind the current design of HVAC systems and the thermal requirements of the different players in the OR.
The predicted mean vote (PMV), developed by Fanger in 1972 [11], is the most used model for predicting thermal comfort in enclosures. Other models used in the literature are the wet bulb globe temperature (WBGT) [12,13], effective temperature (ET) [14] and thermal acceptance ratio (TAR) [12]. Details about the indexes for the evaluation of thermal comfort and hot stress can be found in review works [15,16].
According to the PMV model, the thermophysiological comfort of a person is assessed based on the body’s heat balance, mean skin temperature and sweat rate. The determination of the PMV index requires several input variables and its computation, which requires several iterations, might be done using different programs, including black box [17] and white box [18] software.
The PMV index allows the number of the occupants of the indoor premises who are not satisfied with the provided thermal conditions (feel cold or warm) to be predicted. This feeling stays at the bottom of the determination of the predicted percentage of dissatisfied (PPD) index [11]. It allows the assessment of how many of the occupants will feel uncomfortable in a particular thermal indoor environment.
Predicted heat strain (PHS) is evaluated on the basis of the ISO 7933 international standard [19], and the following stress/strain criteria are taken into account: the maximum sweat rate and maximum skin wettedness. Two strain criteria are also assessed: the maximum water loss and maximum rectal temperature, which is used as equivalent to the core body temperature.
The present paper aims to perform an analysis of thermophysiological comfort in an OR from the point of view of both the patient and the surgeons during an operation. Different surgical clothing ensembles are tested. A computational program for the prediction of the heat strain, following ISO 7933:2004 [16], was applied to calculate the PMV-PPD indexes, according to the model developed by [20]. Interpretations in terms of the predicted heat strain are also made.
2. Methodology: Computational Data
2.1. Environmental Factors
According to ASHRAE standard 170–2013 [21], the air temperature of an OR (Class B and C) should be 20–24 °C. The air temperature of the operating zone around the operating table is 3 °C higher than the air temperature of the rest of the room [6].
The calculations involve a temperature interval from 16 to 32 °C (with a step of 1 °C), changing the relative humidity from 30% to 60% with a step of 10% (see Table 1).
2.2. Factors Related to Human Body Status
Two steady-state activities were considered [19]: sleeping (40 W/m2) for the patient and moderate activity (145 W/m2) for the surgeons.
To assess the thermophysiological comfort of the surgeon and patient, the same data for the physical characteristics of the human body were used for both the surgeon and the patient: height 175, weight 80 kg.
2.3. Factors Related to Clothing
The study in [22] showed that the thermal insulation of the clothing ensembles of surgeons is between 0.54 ± 0.01 clo and 0.95 ± 0.01 clo. It was measured in [23] that the thermal insulation of clothing ensembles was higher than 1 clo. Three clothing ensembles were considered in this study with the following descriptions [23]:
- 0.96 clo: surgical polyester ensemble with coal fibrеs and multiple-use barrier surgical polyester gown with carbon fibres and liquid proof fabric of higher resistance on sleeves and front;
- 1.01 clo: surgical polyester ensemble with coal fibres and multiple-use polyester surgical gown with polytetrafluorethylene protective sleeves and front and carbon fibres on the back;
- 1.05 clo: surgical polyester ensemble with coal fibres and single-use cotton surgical gown.
In addition, a surgical cotton/polyester (33/67%) drape for the patient of 0.15 clo was selected [3].
Table 1 presents the simulated conditions for different clothing insulation, human activity and thermal environment. Forty cases were simulated for the patient in the OR and 180 cases for the surgeons, or 220 cases altogether.
3. Results and Discussion
The PMV index vary from −3 to +3 and the thermal sense scale is shown in Table 2.
The PPD index obtains values from 0% to 100% and is a quantitative measure for the perceived comfort of the inhabitants of a particular thermal environment.
The PHS index is calculated only in a hot environment and is expressed in terms of sweat rate, total sweat loss and rise of the core body temperature.
According to the results for the indexes, the thermal conditions are assessed, following the ISO standard 15265 [24]. The climatic conditions categories, as defined in [20], are summarised in Table 3.
3.1. Thermophysiological Comfort of the Patient
The predicted PMV index for the patient, lying under anaesthesia on the operating table, is shown in Figure 1. The predicted percentage of dissatisfied (PPD) is presented in Figure 2. According to the results, the thermal conditions are assessed, following the ISO standard 15265 [24]. The categories for the climatic conditions are shown in Figure 3.
The simulated temperature interval in which the thermophysiological comfort of the patient was predicted and assessed was between 23 and 32 °C. Calculations for temperatures below 23 °C were meaningless, as, after 25 °C, the PMV index was −3 and the PPD index was 100% dissatisfied. High OR temperatures were tested (31 °C and 32 °C) aiming to reach a climatic conditions category higher than 5 (slight warm discomfort)—Figure 4.
For moderate thermal environments ISO 7730 [2] suggest the limits −0.5 < PMV < 0.5 and the PPD index is below 10%. In the current predictions these values are obtained for the interval from 29 °C, 60% RH (PMV = −0.42) to 31 °C, 30% RH (PMV = +0.44). The comfort temperature interval for the patient is far away from the prescribed comfort indoor environmental temperature (20–22 °C) [2]. The low insulation ability of the standard surgical drape and the low metabolic activity of the patient are the two reasons for the need for very high temperatures in the OR to reach a comfortable environment for the patient. This result confirms the findings in [10], which suggest that the temperature in the OR should be even higher than 24 °C to ensure the thermophysiological comfort of the patient.
The risk for perioperative hypothermia and its effect on the patient’s health, e.g., influence on the blood loss during an operation and special transfusion requirements, are well recognised [25,26]. The administration of 1 dm3 fluid intravenously with a temperature equal to room air temperature (21 °C) decreases the temperature of the core body by 0.25 °C [25]. Such an effect is not even foreseen when calculating the PMV index. Therefore, special methods and devices for warming the patient have been developed and have to be used in the OR in any cases of operations under anaesthesia to assure the thermophysiological comfort of the patient and to protect him/her from perioperative hypothermia. According to the review in [27], these could be intravenous fluid warmers, which are widely applied during surgical operations or body warming devices, like water-filled mattresses, electric blankets, heating pads, carbon fibre items, etc.
3.2. Thermophysiological Comfort of the Surgeon
Figure 4 summarizes the results for the PMV index, computed for a surgeon, working in the OR.
The three clothing ensembles are compared and four different graphs for the relative humidity values in the range 30%–60% are shown. The simulated temperatures were between 16 and 30 °C, different from the temperature range used in the predictions for the thermophysiological comfort of the patient (23–32 °C). The temperatures went below 23 °C to reach climatic conditions category 5 of the indoor environment and to discover at which temperature it turns to climatic conditions category 4.
Figure 5 presents the results for the PPD index and Figure 6 the climatic conditions of the OR from the point of view of the surgeon.
The predicted values for the PMV and PPD show that the thermophysiological comfort of the surgeon, dressed in different clothing ensembles is assured in the following intervals:
- For clothing ensemble with 0.96 clo: from 18 °C, 30% RH (PMV = −0.48) to 23 °C, 40% RH (PMV = +0.48).
- For clothing ensemble with 1.01 clo: from 17 °C, 60% RH (PMV = −0.49) to 23 °C, 30% RH (PMV = +0.47).
- For clothing ensemble with 1.05 clo: from 17 °C, 40% RH (PMV = −0.49) to 22 °C, 60% RH (PMV = +0.49).
The comfort temperature interval for the surgeon is much closer to the prescribed comfort indoor environmental temperature (20–22 °C) [2], compared to the comfort temperature interval for the patient. The results confirm the suggestions in [10], the temperature in the OR to be lower than 18 °C to assure the comfort of the surgeons in heavy protective gowns.
The results in Figure 5 and Figure 6 confirm the conclusions from the prediction of PMV index for the surgeons. The graphs in Figure 6 allow the comfortable environment for the surgeons to be quickly assessed, using the studied protective clothing: all combinations between air temperature and relative humidity, where the climatic category is computed as “5: comfortable, no health risk” (Table 3).
3.3. The Thermophysiological Comfort of the Patient vs. the Thermophysiological Comfort of the Surgeon
The comparison between the PMV index for the patient and the surgeon in the concurrent temperature interval (23–30 °C) is presented in Figure 7. The comparison is made for two values of the relative humidity of the air (30% and 60%) and 0.96 clo thermal insulation of the clothing ensemble of the surgeon, assuming that this is the closest value to the thermal insulation of the patient under anaesthesia.
Figure 8 presents the comparison for the PPD index for the same conditions and Figure 9 for the category of the climatic conditions.
The results obtained show that within the concurrent temperature interval (23–30 °C) there is no combination between air temperature and relative humidity values that can assure the thermophysiological comfort for both the surgeon and the patient. The most favourable PPD index for the surgeon and the patient simultaneously is for 28 °C, 30% RH (Figure 8a), where the PPD for the patient is 48% and for the surgeon is 44%. The next favourable PPD index is for 28 °C, 60% RH (Figure 8b): 29% for the patient and 56% for the surgeon.
Obviously, the thermal discrepancies between the thermophysiological comfort of the patient and the surgeon can provoke thermal stress for one or the other, even for short-time interventions in the OR. If the surgeon stays dressed in heavier operating suits (with clothing insulation higher than 0.96 clo) the discrepancies between him/her and the patient increase.
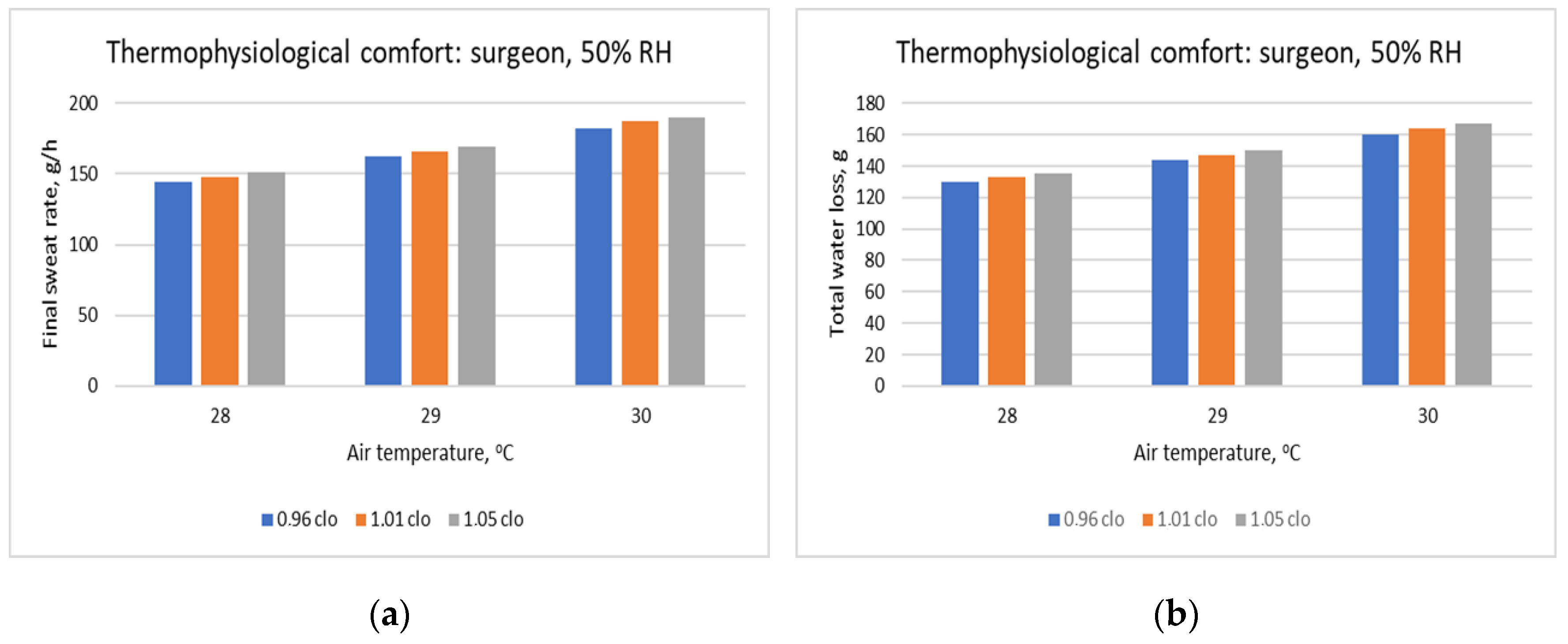
Figure 10 shows exemplary results for the thermal stress of the surgeon, dressed in the studied clothing ensembles. In cases where the climatic conditions category is equal to 7 (severe warm discomfort without health risk, Table 3) or higher, thermal stress due to the hot environment appears in the body. The stress results mainly in increased sweating of the body, which can be expressed by the final sweat rate and the total water loss (calculated here for 60 min). The results are presented for 50% RH in the OR.
The joint increment of the air temperature and the clothing insulation of the surgical gowns provokes the rise of both the sweat rate and the water losses through the skin. The sweat rate increment aims to compensate for the heat gained by the environmental air as well as the impeded heat and fluid transfer through the clothing ensemble with higher clothing insulation.
3.4. Research Strengths and Limitations
The performed calculations are done on the basis of the real clothing insulation of both the surgeons and patient. The study is not spread among other players in the OR (anaesthetists, nurses, assistants), concentrating on the thermophysiological comfort of the subjects that share one and the same thermal environment. The calculations of the PMV/PPD indexes for different clothing insulation, metabolism, temperature, and relative humidity are fast, reliable, and confirm once again the need for special HVAC design or other measures that could guarantee the thermophysiological comfort of all persons in the OR.
The limitations of the study are related to the fact that the PMV/PPD model is developed for healthy people and its application for a patient under anaesthesia might not be correct, as the thermophysiological reactions could be different. Another limitation of the predictions is that the OR is taken as a standard one, while different OR exists (orthopedic, cardiac, etc.).
4. Conclusions
The use of different textiles and clothing ensembles, coupled with different metabolic activity, puts the patient and the surgeon in opposed thermal conditions in the operating room. Even a surgical gown with the lowest possible insulation requires the temperature in the OR to be much lower than is healthy for the patient under anaesthesia. It was found that within the studied environmental, metabolic and clothing conditions, only the temperature of 28 °C can partly satisfy the thermophysiological comfort of both the patient and the surgeon. However, it cannot be recommended, as it provokes thermal stress for the surgeon.
The recommendations of future research should involve the development of a database for the clothing insulation of surgical clothes, surgical gowns and drapes. It would be interesting to evaluate the effect of the stress of the surgeons on their thermophysiological reaction during operations, as well as the impact of the duration of the operation on surgeons’ thermophysiological comfort.
Author Contributions
Conceptualization and original draft preparation, R.A.A.; data curation and editing, R.V.; visualization, R.A.A. All authors have read and agreed to the published version of the manuscript.
Funding
The authors would like to thank the Research and Development Sector at the Technical University of Sofia for the financial support for the publishing of the present research.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Uścinowicz, P.; Chludzińska, M.; Bogdan, A. Thermal environment conditions in Polish operating rooms. Build. Environ. 2015, 94, 296–304. [Google Scholar] [CrossRef]
- International Organization for Standardization. ISO 7730: Moderate Thermal Environments-Determination of the PMV and PPD Indices and Specification of the Conditions for Thermal Comfort; ISO: Geneva, Switzerland, 2005. [Google Scholar]
- Angelova, R.A. Textiles and Human Thermophysiological Comfort in the Indoor Environment; CRC Press: Boca Raton, FL, USA, 2015. [Google Scholar]
- Khodakarami, J.; Nasrollahi, N. Thermal comfort in hospitals–A literature review. Renew. Sustain. Energy Rev. 2012, 16, 4071–4077. [Google Scholar] [CrossRef]
- Van Gaever, R.; Jacobs, V.A.; Diltoer, M.; Peeters, L.; Vanlanduit, S. Thermal comfort of the surgical staff in the operating room. Build. Environ. 2014, 81, 37–41. [Google Scholar] [CrossRef]
- Chow, T.T.; Kwan, A.; Lin, Z.; Bai, W. Conversion of operating theatre from positive to negative pressure environment. J. Hosp. Infect. 2006, 64, 371–378. [Google Scholar] [CrossRef] [PubMed]
- Patania, F.; Gagliano, A.; Nocera, F.; Galesi, A. Thermal comfort in operating rooms: A case study. WIT Trans. Biomed. Health 2011, 15, 105–114. [Google Scholar]
- Sadrizadeh, S.; Loomans, M.G.L.C. Thermal comfort in hospital and healthcare facilities: A literature review. In Proceedings of the 9th International Conference on Indoor Air Quality Ventilation & Energy Conservation in Buildings, Seoul, Korea, 23–26 October 2016; pp. 1–12. [Google Scholar]
- Zwolińska, M.; Bogdan, A. Thermal sensations of surgeons during work in surgical gowns. Int. J. Occup. Saf. Ergon. 2013, 19, 443–453. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Balaras, C.A.; Dascalaki, E.; Gaglia, A. HVAC and indoor thermal conditions in hospital operating rooms. Energy Build. 2007, 39, 454–470. [Google Scholar] [CrossRef]
- Fanger, P.O. Thermal Comfort Analysis and Applications in Environmental Engineering; McGraw-Hill: New York, NY, USA, 1972. [Google Scholar]
- Moran, D.S.; Pandolf, K.B.; Shapiro, Y.; Heled, Y.; Shani, Y.; Mathew, W.T.; Gonzalez, R.R. An environmental stress index (ESI) as a substitute for the wet bulb globe temperature (WBGT). J. Therm. Biol. 2001, 26, 427–431. [Google Scholar] [CrossRef]
- D’Ambrosio Alfano, F.R.; Malchaire, J.; Palella, B.I.; Riccio, G. WBGT index revisited after 60 years of use. Ann. Occup. Hyg. 2014, 58, 955–970. [Google Scholar] [PubMed] [Green Version]
- Yaglou, C.P. Temperature, humidity, and air movement in industries: The effective temperature index. J. Ind. Hyg. 1927, 9, 297–309. [Google Scholar]
- Taleghani, M.; Tenpierik, M.; Kurvers, S.; Van Den Dobbelsteen, A. A review into thermal comfort in buildings. Renew. Sustain. Energy Rev. 2013, 26, 201–215. [Google Scholar] [CrossRef]
- Epstein, Y.; Moran, D.S. Thermal comfort and the heat stress indices. Ind. Health 2006, 44, 388–398. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Atthajariyakul, S.; Leephakpreeda, T. Real-time determination of optimal indoor-air condition for thermal comfort, air quality and efficient energy usage. Energy Build. 2004, 36, 720–733. [Google Scholar] [CrossRef]
- Homod, R.Z.; Sahari, K.S.M.; Almurib, H.A.; Nagi, F.H. RLF and TS fuzzy model identification of indoor thermal comfort based on PMV/PPD. Build. Environ. 2012, 49, 141–153. [Google Scholar] [CrossRef]
- ISO. Ergonomics of the Thermal Environment-Analytical Determination and Interpretation of Heat Stress Using Calculation of the Predicted Heat Strain; International Standardisation Organisation: Geneva, Germany, 2004. [Google Scholar]
- Malchaire, J.B. Evaluation of natural wet bulb and wet globe thermometers. The Annals of occupational hygiene 1976, 19, 251–258. [Google Scholar]
- ASHRAE Standard 170-2013. Ventilation of Health Care Facilities; ASHRAE: Atlanta, GA, USA, 2013.
- Konarska, M.; Soltynski, K.; Sudol-Szo-pinska, I.; Chojnacka, A. Comparative evaluation of clothing thermal insulation measured on a thermal manikin and on volunteers. Fibres Text. East. Eur. 2007, 15, 79–85. [Google Scholar]
- Bogdan, A.; Sudoł-Szopińska, I.; Szopiński, T. Assessment of textiles for use in operating theatres with respect to the thermal comfort of surgeons. Fibres Text. East. Eur. 2011, 19, 65–69. [Google Scholar]
- ISO. 15265:2004 Ergonomics of the Thermal Environment-Risk Assessment Strategy for the Prevention of Stress or Discomfort in Thermal Working Conditions; ISO: Geneva, Switzerland, 2004. [Google Scholar]
- Sessler, D.I. Mild perioperative hypothermia. New Engl. J. Med. 1997, 336, 1730–1737. [Google Scholar] [CrossRef] [PubMed]
- Rajagopalan, S.; Mascha, E.; Na, J.; Sessler, D.I. The effects of mild perioperative hypothermia on blood loss and transfusion requirement. Anesthesiol. J. Am. Soc. Anesthesiol. 2008, 108, 71–77. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- John, M.; Ford, J.; Harper, M. Peri-Operative warming devices: Performance and clinical application. Anaesthesia 2014, 69, 623–638. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Predicted mean vote (PMV) index for the patient under anaesthesia.

Figure 2.
Predicted percentage of dissatisfied (PPD) index for the patient under anaesthesia.

Figure 3.
Category of the climatic conditions for the patient under anaesthesia.

Figure 4.
PMV index for the surgeon, dressed in three clothing ensembles with different clothing insulation: (a) relative humidity (RH) of the air 30%; (b) RH 40%; (c) RH 50%; (d) RH 60%.
Figure 4.
PMV index for the surgeon, dressed in three clothing ensembles with different clothing insulation: (a) relative humidity (RH) of the air 30%; (b) RH 40%; (c) RH 50%; (d) RH 60%.

Figure 5.
PPD index for the surgeon, dressed in three clothing ensembles with different clothing insulation: (a) relative humidity (RH) of the air 30%; (b) RH 40%; (c) RH 50%; (d) RH 60%.
Figure 5.
PPD index for the surgeon, dressed in three clothing ensembles with different clothing insulation: (a) relative humidity (RH) of the air 30%; (b) RH 40%; (c) RH 50%; (d) RH 60%.

Figure 6.
Climatic conditions category for the surgeon, dressed in three clothing ensembles with different clothing insulation: (a) relative humidity (RH) of the air 30%; (b) RH 40%; (c) RH 50%; (d) RH 60%.
Figure 6.
Climatic conditions category for the surgeon, dressed in three clothing ensembles with different clothing insulation: (a) relative humidity (RH) of the air 30%; (b) RH 40%; (c) RH 50%; (d) RH 60%.

Figure 7.
PMV index for the patient (0.15 clo) and the surgeon (0.96 clo): (a) relative humidity (RH) of the air 30%; (b) RH 60%.
Figure 7.
PMV index for the patient (0.15 clo) and the surgeon (0.96 clo): (a) relative humidity (RH) of the air 30%; (b) RH 60%.

Figure 8.
PPD index for the patient (0.15 clo) and the surgeon (0.96 clo): (a) relative humidity (RH) of the air 30%; (b) RH 60%.
Figure 8.
PPD index for the patient (0.15 clo) and the surgeon (0.96 clo): (a) relative humidity (RH) of the air 30%; (b) RH 60%.

Figure 9.
Climatic conditions category for the patient (0.15 clo) and the surgeon (0.96 clo): (a) relative humidity (RH) of the air 30%; (b) RH 60%.
Figure 9.
Climatic conditions category for the patient (0.15 clo) and the surgeon (0.96 clo): (a) relative humidity (RH) of the air 30%; (b) RH 60%.

Figure 10.
Thermophysiological comfort of the surgeon (50% RH): (a) final sweat rate; (b) total water loss for 60 min.
Figure 10.
Thermophysiological comfort of the surgeon (50% RH): (a) final sweat rate; (b) total water loss for 60 min.


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Table 1.
Simulated conditions.
| Clothing Insulation | Temperature | Humidity | Metabolism |
|---|---|---|---|
| 0.15 clo | 23–32 °C | 30–60% | 40 W/m2 |
| 0.96 clo | 16–30 °C | 30–60% | 145 W/m2 |
| 1.01 clo | 16–30 °C | 30–60% | 145 W/m2 |
| 1.05 clo | 16–30 °C | 30–60% | 145 W/m2 |
Table 2.
PMV index sense scale.
| Value | Thermal Sense |
|---|---|
| −3 | cold |
| −2 | cool |
| −1 | slightly cool |
| 0 | neutral |
| +1 | slightly warm |
| +2 | warm |
| +3 | hot |
Table 3.
Climatic conditions category.
| Category | Comfort Related to the Climatic Conditions |
|---|---|
| 3 | Severe discomfort without health risk |
| 4 | Slight cold discomfort without health risk |
| 5 | Comfort, no health risk |
| 6 | Slight warm discomfort without health risk |
| 7 | Severe warm discomfort without health risk |
| 8 | Long-term constraint: discomfort and dehydration after several hours of exposure |
| 9 | Short-term constraint: health risk after 30–120 min of exposure |
| 10 | Immediate constraint: health risk even for exposures of very short duration (less than 30 min) several hours of exposure |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Angelova, R.A.; Velichkova, R. Thermophysiological Comfort of Surgeons and Patient in an Operating Room Based on PMV-PPD and PHS Indexes. Appl. Sci. 2020, 10, 1801. https://0-doi-org.brum.beds.ac.uk/10.3390/app10051801
AMA Style
Angelova RA, Velichkova R. Thermophysiological Comfort of Surgeons and Patient in an Operating Room Based on PMV-PPD and PHS Indexes. Applied Sciences. 2020; 10(5):1801. https://0-doi-org.brum.beds.ac.uk/10.3390/app10051801
Chicago/Turabian StyleAngelova, Radostina A., and Rositsa Velichkova. 2020. "Thermophysiological Comfort of Surgeons and Patient in an Operating Room Based on PMV-PPD and PHS Indexes" Applied Sciences 10, no. 5: 1801. https://0-doi-org.brum.beds.ac.uk/10.3390/app10051801
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.