Control System Applied to the Microinjection of Artificial Tears for Severe Dry Eye Treatment

 , , and
, , and
Abstract
:
1. Introduction
2. Foundations
2.1. Hagen–Poiseuille Flow
2.2. Theoretical Determination of Power
3. Materials and Methods
3.1. Electronic Components and Accessories
3.2. Mechatronic V VDI 2206 Methodology
4. Tears Microinjector Design and Assembly
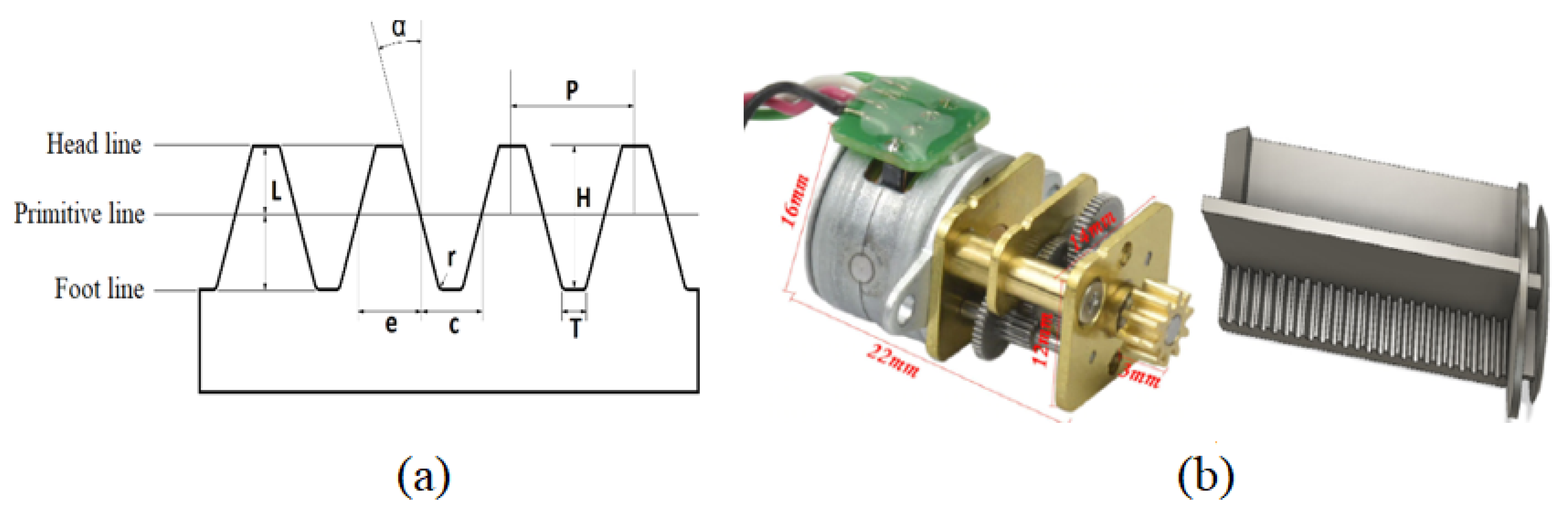
4.1. Engine–Plunger Coupling and Mechanical Design
4.2. Electronic Design and Assembly
4.3. Control of the Microinjection System
5. User Configuration
- Turn on the device by pressing on the start button.
- To connect his/her Android-based cell phone via Wi-Fi with the ESP8266EX microcontroller web server. The name and password of the network must be previously assigned when programming the microcontroller. Easy to remember names are suggested, like “Dry Eye” for the network’s name.
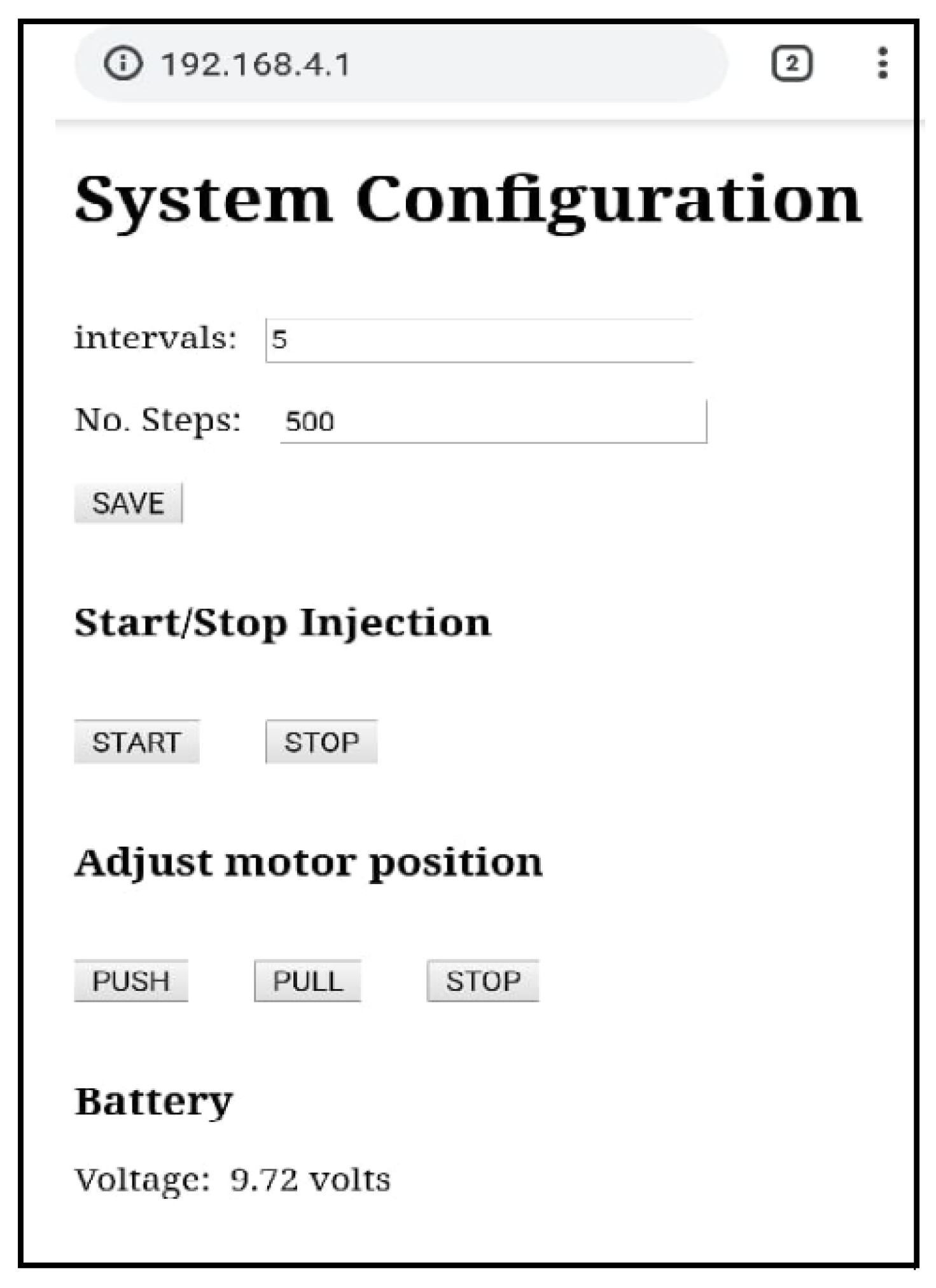
- Once connected, a web browser opens at the IP address of the server, and the user-friendly interface shown in Figure 9 is displayed. This interface is controlled by the Algorithm A1, it has enter and touch buttons to perform every possible action offered by the microinjector and to introduce input values.
- Intervals: waiting time between consecutive injections, (number in s).
- No. Steps: number of steps to be rotated by the engine, n.
- SAVE: Saves input parameters.
- START: Starts injection.
- STOP: Stops/pause injection.
- Refill/Empty tears reservoir
- PUSH: Moves the plunger forward at maximum engine power. This option may be used to empty the reservoir.
- PULL: Moves the plunger backwards at maximum engine power. This option is used to refill the reservoir.
- STOP: stops movement of the plunger.
- Battery indicator
- Voltage: Indicates the current voltage of the battery, this value is updated every 10 s automatically.
6. Results of Functionality and Performance Tests
7. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A
| Algorithm A1 Microinjector sequence control. |
| 1: Start |
| 2: Read_EEPROM(No_Steps, Time_interval |
| 3: Initialize_Variables (No_Steps, Time_interval) |
| 4: Start_Server() |
| 5: Set_Ports_I/O() |
| 6: Continuous_Cycle() |
| 7: if Web_Client_Request then |
| 8: if Save_Button then |
| 9: Read_Web_Page (No_Steps, Time_interval) |
| 10: Save_in_EEPROM (No_Steps, Time_interval ) |
| 11: Initialize_Variables (No_Steps, Time_interval ) |
| 12: if Pull_Button then |
| 13: Rotate_Motor_Right () |
| 14: if push_Button then |
| 15: Rotate_Motor_Left () |
| 16: if Stop_Button then |
| 17: stop_Motor() |
| 18: if Start_Button then |
| 19: Flag_Active_Start |
| 20: if Finish_Button then |
| 21: Flag_Inactive_Start |
| 22: if Active_Time > 10 Seconds then |
| 23: Update_Battery_voltage() |
| 24: if Flag_Active_Start then |
| 25: if Interval >= Elapsed_time then |
| 26: Move_Motor (Number_Steps) |
| 27: Save_Data_in_EEPROM (Number_Steps) |
| 28: if Number_Steps >= Steps_MAX then |
| 29: Flag_Inactive_Start |
| 30: if Flag_Inactive_Start then |
| 31: Stop_Motor; |
| 32: Save_Steps_in_EEPROM; |
| 33: Finish |
References
- Barabino, S.; Labetoulle, M.; Rolando, M.; Messmer, E.M. Understanding symptoms and quality of life in patients with dry eye syndrome. Ocul. Surf. 2016, 14, 365–376. [Google Scholar] [CrossRef] [PubMed]
- Zheng, Y.; Wu, X.; Lin, X.; Lin, H. The prevalence of depression and depressive symptoms among eye disease patients: A systematic review and meta-analysis. Sci. Rep. 2017, 7, 46453. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Onwubiko, S.N.; Eze, B.I.; Udeh, N.N.; Arinze, O.C.; Onwasigwe, E.N.; Umeh, R.E. Dry eye disease: Prevalence, distribution and determinants in a hospital-based population. Contact Lens Anterior Eye 2014, 37, 157–161. [Google Scholar] [CrossRef] [PubMed]
- Clegg, J.P.; Guest, J.F.; Lehman, A.; Smith, A.F. The annual cost of dry eye syndrome in France, Germany, Italy, Spain, Sweden and the United Kingdom among patients managed by ophthalmologists. Ophthalmic Epidemiol. 2006, 13, 263–274. [Google Scholar] [CrossRef] [PubMed]
- Schaumberg, D.A.; Sullivan, D.A.; Buring, J.E.; Dana, M.R. Prevalence of dry eye syndrome among US women. Am. J. Ophthalmol. 2003, 136, 318–326. [Google Scholar] [CrossRef]
- Schaumberg, D.A.; Dana, R.; Buring, J.E.; Sullivan, D.A. Prevalence of dry eye disease among US men: Estimates from the Physicians’ Health Studies. Arch. Ophthalmol. 2009, 127, 763–768. [Google Scholar] [CrossRef] [Green Version]
- Osae, A.; Gehlsen, U.; Horstmann, J.; Siebelmann, S.; Stern, M.; Kumah, D.; Steven, P. Epidemiology of dry eye disease in Africa: The sparse information, gaps and opportunities. Ocul. Surf. 2017, 15, 159–168. [Google Scholar] [CrossRef]
- Song, P.; Xia, W.; Wang, M.; Chang, X.; Wang, J.; Jin, S.; Wang, J.; Wei, W.; Rudan, I. Variations of dry eye disease prevalence by age, sex and geographic characteristics in China: A systematic review and meta-analysis. J. Glob. Health 2018, 8, 020503. [Google Scholar] [CrossRef]
- Donthineni, P.R.; Kammari, P.; Shanbhag, S.S.; Singh, V.; Das, A.V.; Basu, S. Incidence, demographics, types and risk factors of dry eye disease in India: Electronic medical records driven big data analytics report I. Ocul. Surf. 2019, 17, 250–256. [Google Scholar] [CrossRef]
- Andrade, F.N.V.; Flores, T.E.M.; Barzola, C.V.R.; Mestanza, P.M.G. Sindrome de ojo seco asociado al computador, manifestaciones clínicas y factores de riesgo. Sinerg. Educ. 2020, E, 1–9. [Google Scholar]
- Doughty, M.J.; Fonn, D.; Richter, D.; Simpson, T.; Caffery, B.; Gordon, K. A patient questionnaire approach to estimating the prevalence of dry eye symptoms in patients presenting to optometric practices across Canada. Optom. Vis. Sci. Off. Publ. Am. Acad. Optom. 1997, 74, 624–631. [Google Scholar] [CrossRef] [PubMed]
- Shimmura, S.; Shimazaki, J.; Tsubota, K. Results of a population-based questionnaire on the symptoms and lifestyles associated with dry eye. Cornea 1999, 18, 408–411. [Google Scholar] [CrossRef] [PubMed]
- Yazdani, C.; McLaughlin, T.; Smeeding, J.E.; Walt, J. Prevalence of treated dry eye disease in a managed care population. Clin. Ther. 2001, 23, 1672–1682. [Google Scholar] [CrossRef]
- Stapleton, F.; Alves, M.; Bunya, V.Y.; Jalbert, I.; Lekhanont, K.; Malet, F.; Na, K.S.; Schaumberg, D.; Uchino, M.; Vehof, J.; et al. Tfos dews ii epidemiology report. Ocul. Surf. 2017, 15, 334–365. [Google Scholar] [CrossRef] [PubMed]
- O’Neil, E.C.; Henderson, M.; Massaro-Giordano, M.; Bunya, V.Y. Advances in dry eye disease treatment. Curr. Opin. Ophthalmol. 2019, 30, 166–178. [Google Scholar] [CrossRef]
- Fezza, J.P. Cross-linked hyaluronic acid gel occlusive device for the treatment of dry eye syndrome. Clin. Ophthalmol. 2018, 12, 2277. [Google Scholar] [CrossRef] [Green Version]
- Barta, Z.; Czompa, L.; Rentka, A.; Zold, E.; Remenyik, J.; Biro, A.; Gesztelyi, R.; Zsuga, J.; Szodoray, P.; Kemeny-Beke, A. Evaluation of Objective Signs and Subjective Symptoms of Dry Eye Disease in Patients with Inflammatory Bowel Disease. BioMed Res. Int. 2019, 2019, 8310583. [Google Scholar] [CrossRef] [Green Version]
- German, E.J.; Hurst, M.A.; Wood, D. Reliability of drop size from multi-dose eye drop bottles: Is it cause for concern? Eye 1999, 13, 93. [Google Scholar] [CrossRef] [Green Version]
- Surya, V.; Srutartha, B.; Shreya Kulkarni, K.D. Ocular Drug Delivery System Using Open-Source Syringe Pump. Asian J. Pharm. Clin. Res. 2018, 11, 152–157. [Google Scholar]
- Mishima, S.; Gasset, A.; Klyce, S.; Baum, J. Determination of tear volume and tear flow. Investig. Ophthalmol. Vis. Sci. 1966, 5, 264–276. [Google Scholar]
- Cerretani, C.F.; Radke, C. Tear dynamics in healthy and dry eyes. Curr. Eye Res. 2014, 39, 580–595. [Google Scholar] [CrossRef] [PubMed]
- Li, S.; Kim, Y.H.; Li, W.; Lin, M.C.; Radke, C.J. Human lacrimal production rates from modified Schirmer-tear test. Optom. Vis. Sci. 2018, 95, 343–348. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ousler, G.W., III; Hagberg, K.W.; Schindelar, M.; Welch, D.; Abelson, M.B. The ocular protection index. Cornea 2008, 27, 509–513. [Google Scholar] [CrossRef] [PubMed]
- Jones, L.T. Anatomy of the tear system. Int. Ophthalmol. Clin. 1973, 13, 3–22. [Google Scholar] [CrossRef] [PubMed]
- Chan, T.C.; Chow, S.S.; Wan, K.H.; Yuen, H.K. Update on the association between dry eye disease and meibomian gland dysfunction. Hong Kong Med. J. 2019, 25, 38–47. [Google Scholar] [CrossRef] [Green Version]
- Murube, J.; Murube, E.; ChenZhuo, L.; Rivas, L. Subcutaneous abdominal artificial tears pump-reservoir for severe dry eye. Orbit 2003, 22, 29–40. [Google Scholar] [CrossRef]
- Pillay, V.; Choonara, Y.E.; du Toit, L.C. Intraocular drug delivery technologies: Advancing treatment of posterior segment disorders of the eye. In Nano-Biomaterials for Ophthalmic Drug Delivery; Springer: Berlin, Germany, 2016; pp. 407–460. [Google Scholar]
- Tiffany, J.M. The viscosity of human tears. Int. Ophthalmol. 1991, 15, 371–376. [Google Scholar] [CrossRef]
- Andres, S.; Garcia, M.; Espina, M.; Valero, J.; Valls, O. Tear pH, air pollution, and contact lenses. Am. J. Optom. Physiol. Opt. 1988, 65, 627–631. [Google Scholar] [CrossRef]
- Tiffany, J.M. Composition and biophysical properties of the tear film: Knowledge and uncertainty. In Lacrimal Gland, Tear Film, and Dry Eye Syndromes; Springer: Berlin, Germany, 1994; pp. 231–238. [Google Scholar]
- Versura, P.; Profazio, V.; Campos, E. Performance of tear osmolarity compared to previous diagnostic tests for dry eye diseases. Curr. Eye Res. 2010, 35, 553–564. [Google Scholar] [CrossRef]
- Bhojwani, R.; Cellesi, F.; Maino, A.; Jalil, A.; Haider, D.; Noble, B. Treatment of dry eye: An analysis of the British Sjögren’s Syndrome Association comparing substitute tear viscosity and subjective efficacy. Contact Lens Anterior Eye 2011, 34, 269–273. [Google Scholar] [CrossRef]
- Kirby, B.J. Micro-And Nanoscale Fluid Mechanics: Transport in Microfluidic Devices; Cambridge University Press: Cambridge, UK, 2010. [Google Scholar]
- Pisano, A. From Tubes and Catheters to the Basis of Hemodynamics: The Hagen–Poiseuille Equation. In Physics for Anesthesiologists; Springer: Berlin, Germany, 2017; pp. 55–61. [Google Scholar]
- Lievens, C.; Berdy, G.; Douglass, D.; Montaquila, S.; Lin, H.; Simmons, P.; Carlisle-Wilcox, C.; Vehige, J.; Haque, S. Evaluation of an enhanced viscosity artificial tear for moderate to severe dry eye disease: A multicenter, double-masked, randomized 30-day study. Contact Lens Anterior Eye 2019, 42, 443–449. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Milner, M.S.; Beckman, K.A.; Luchs, J.I.; Allen, Q.B.; Awdeh, R.M.; Berdahl, J.; Boland, T.S.; Buznego, C.; Gira, J.P.; Goldberg, D.F.; et al. Dysfunctional tear syndrome: Dry eye disease and associated tear film disorders–new strategies for diagnosis and treatment. Curr. Opin. Ophthalmol. 2017, 28, 3. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sianoudis, I.; Drakaki, E. An approach to Poiseuille’s law in an undergraduate laboratory experiment. Eur. J. Phys. 2008, 29, 489. [Google Scholar] [CrossRef]
- Poiseuille, J. Recherches expérimentales sur le mouvement des liquides dans les tubes de très petits diamètres [Experimental research on the movement of liquids in capillary of very small diameters]. Comptes Rendus Hebdomadaires Des SÉances de L’Académie des Sciences 1840, 11, 1041–1048. [Google Scholar]
- Hagen, G. Ueber die Bewegung des Wassers in engen cylindrischen Röhren. Ann. Phys. 1839, 122, 423–442. [Google Scholar] [CrossRef] [Green Version]
- Entwicklungsmethodik für Mechatronische Systeme. Design Methodology for Mechatronic Systems: VDI 2206, VDI-Richtlinien; Beuth Verlag GmbH: Berlin, Germany, 2004; Volume 2206. [Google Scholar]
- Ruben, M.O.; Trodd, C.H. Constant perfusion for dry eyes and sockets. Br. J. Ophthalmol. 1978, 62, 268–270. [Google Scholar] [CrossRef] [Green Version]












{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Programmed Volume (μL) | Programmed Time (h-m-s) | Obtained Volume (μL) | Air | Distilled Water | Lagricel Ofteno (Ophthalmic Solution 0.4%) | |||
|---|---|---|---|---|---|---|---|---|
| Real Time (h-m-s) | Time Error (%) | Real Time (h-m-s) | Time Error (%) | Real Time (h-m-s) | Time Error (%) | |||
| 1000 | 16-20-00 | 1000 | 16-20-00 | 0.000 | 16-21-03 | 0.100 | 16-21-30 | 0.153 |
| 960 | 16-00-00 | 960 | 16-00-00 | 0.000 | 16-00-43 | 0.070 | 16-01-31 | 0.157 |
| 780 | 13-00-00 | 780 | 13-00-00 | 0.000 | 13-00-37 | 0.070 | 13-01-16 | 0.162 |
| 600 | 10-00-00 | 600 | 10-00-00 | 0.000 | 10-00-29 | 0.080 | 10-01-07 | 0.186 |
| 360 | 06-00-00 | 360 | 06-00-01 | 0.004 | 06-00-32 | 0.140 | 06-00-51 | 0.236 |
| 120 | 02-00-00 | 120 | 02-00-04 | 0.055 | 02-00-07 | 0.090 | 02-00-18 | 0.249 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Meni-Babakidi, N.; Viramontes-Gamboa, G.; Ibarra-Bracamontes, L.A.; Luna-Reyes, I. Control System Applied to the Microinjection of Artificial Tears for Severe Dry Eye Treatment. Appl. Sci. 2020, 10, 1883. https://0-doi-org.brum.beds.ac.uk/10.3390/app10051883
Meni-Babakidi N, Viramontes-Gamboa G, Ibarra-Bracamontes LA, Luna-Reyes I. Control System Applied to the Microinjection of Artificial Tears for Severe Dry Eye Treatment. Applied Sciences. 2020; 10(5):1883. https://0-doi-org.brum.beds.ac.uk/10.3390/app10051883
Chicago/Turabian StyleMeni-Babakidi, Narcisse, Gonzalo Viramontes-Gamboa, Laura Alicia Ibarra-Bracamontes, and Israel Luna-Reyes. 2020. "Control System Applied to the Microinjection of Artificial Tears for Severe Dry Eye Treatment" Applied Sciences 10, no. 5: 1883. https://0-doi-org.brum.beds.ac.uk/10.3390/app10051883