
The Anatomy, Features and Sex Correlations (Dimorphism) of Tubero–Palato–Pterygoid Region among Adult Population—Single Center Study Based on 3D Printed Models

 , ,
, ,  ,
,  , ,
, ,  ,
,  and
and
Abstract
:1. Introduction
2. Materials and Methods
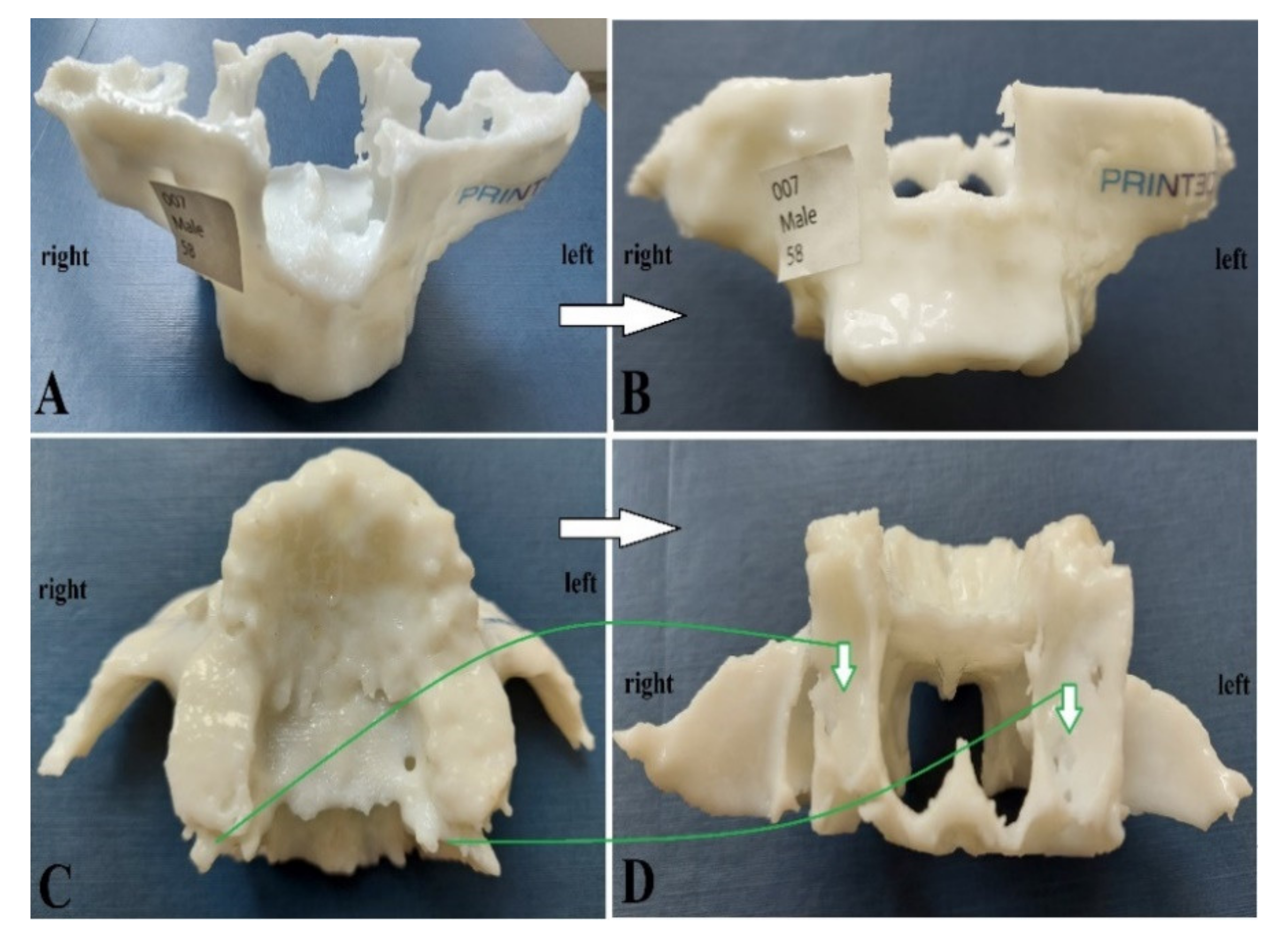
2.1. Study Group and Printed Models of Maxilla (CT)
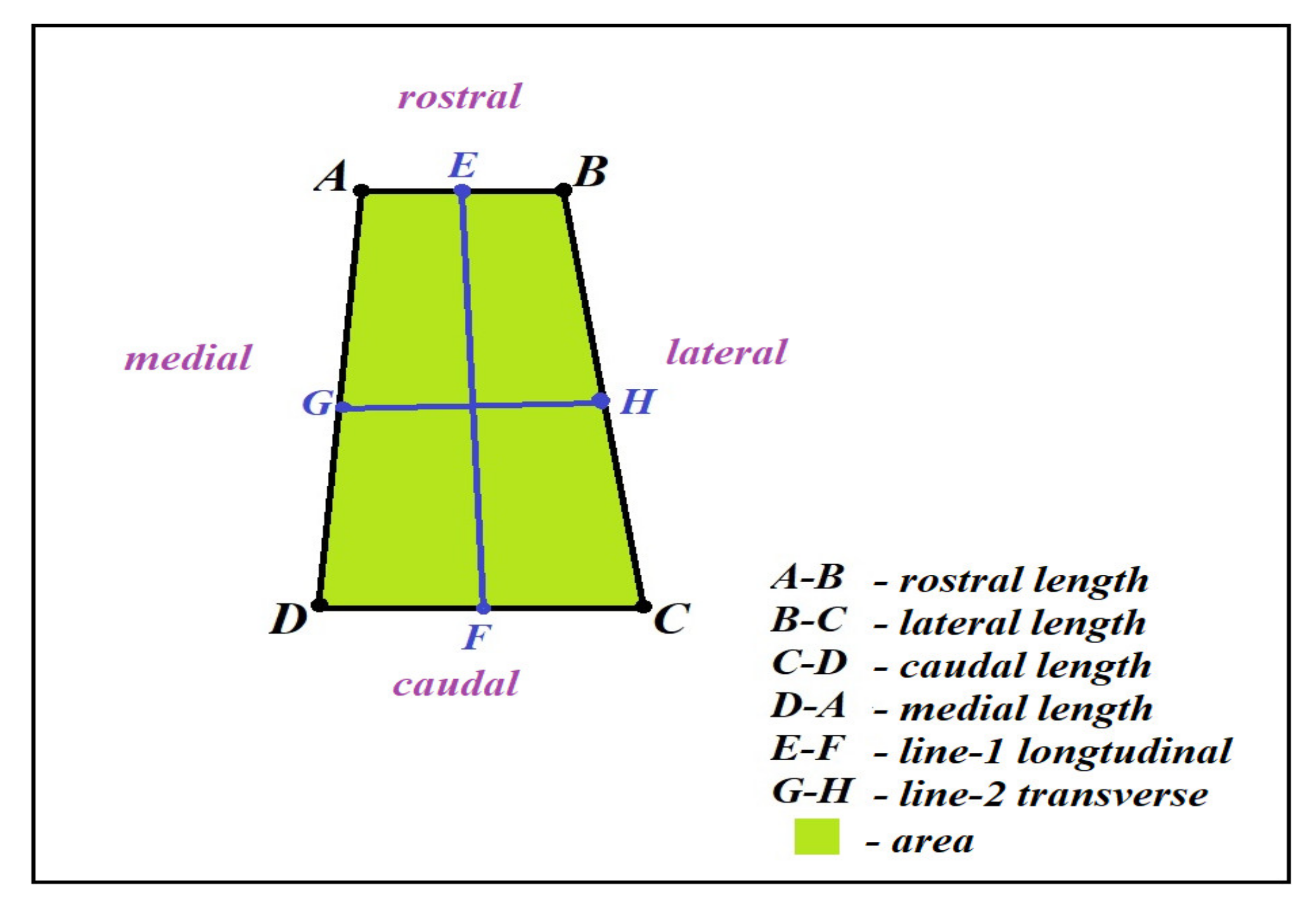
2.2. Measurements
2.3. Statistical Analysis
3. Results
3.1. Descriptive Analysis
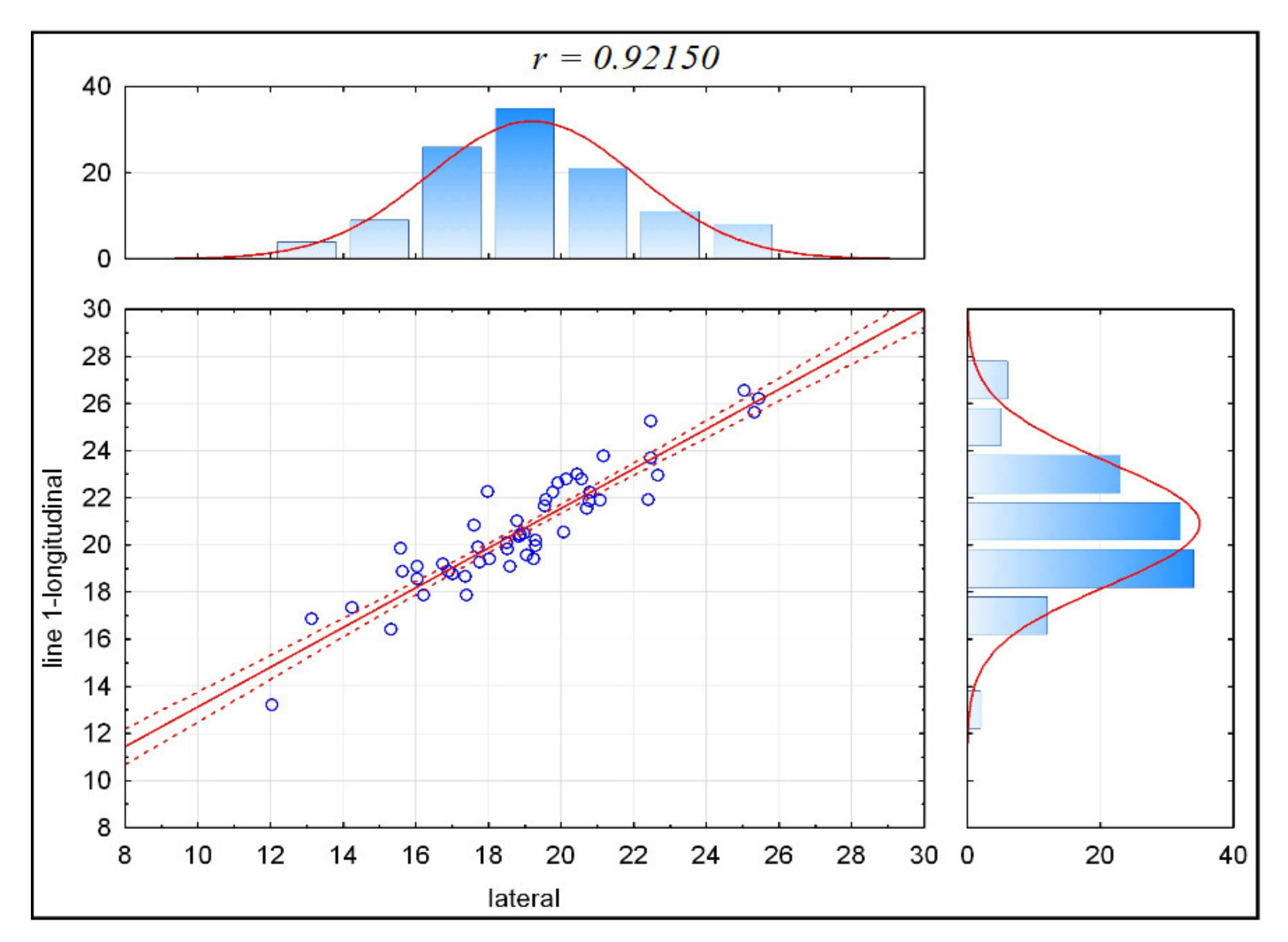
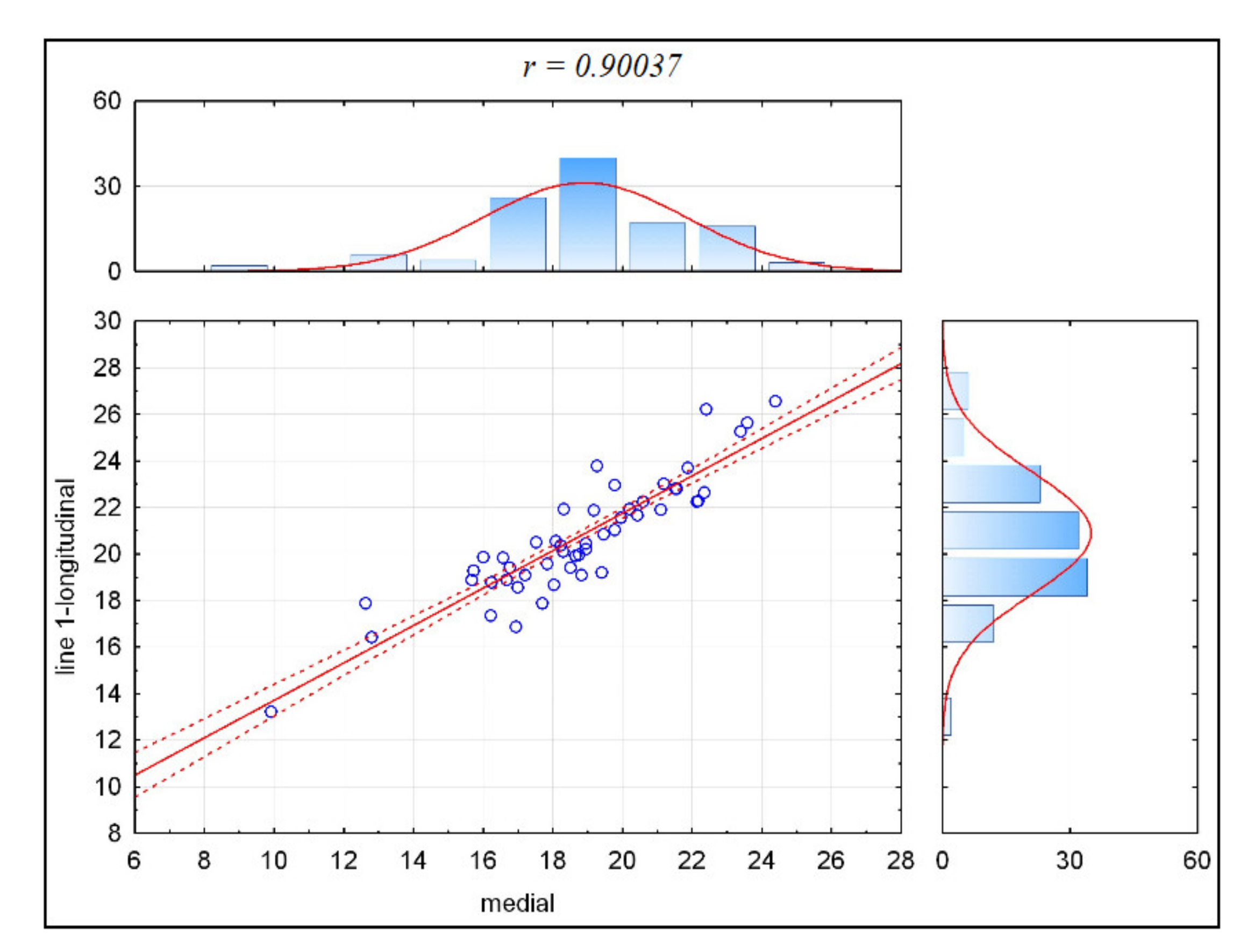
3.2. Correlations
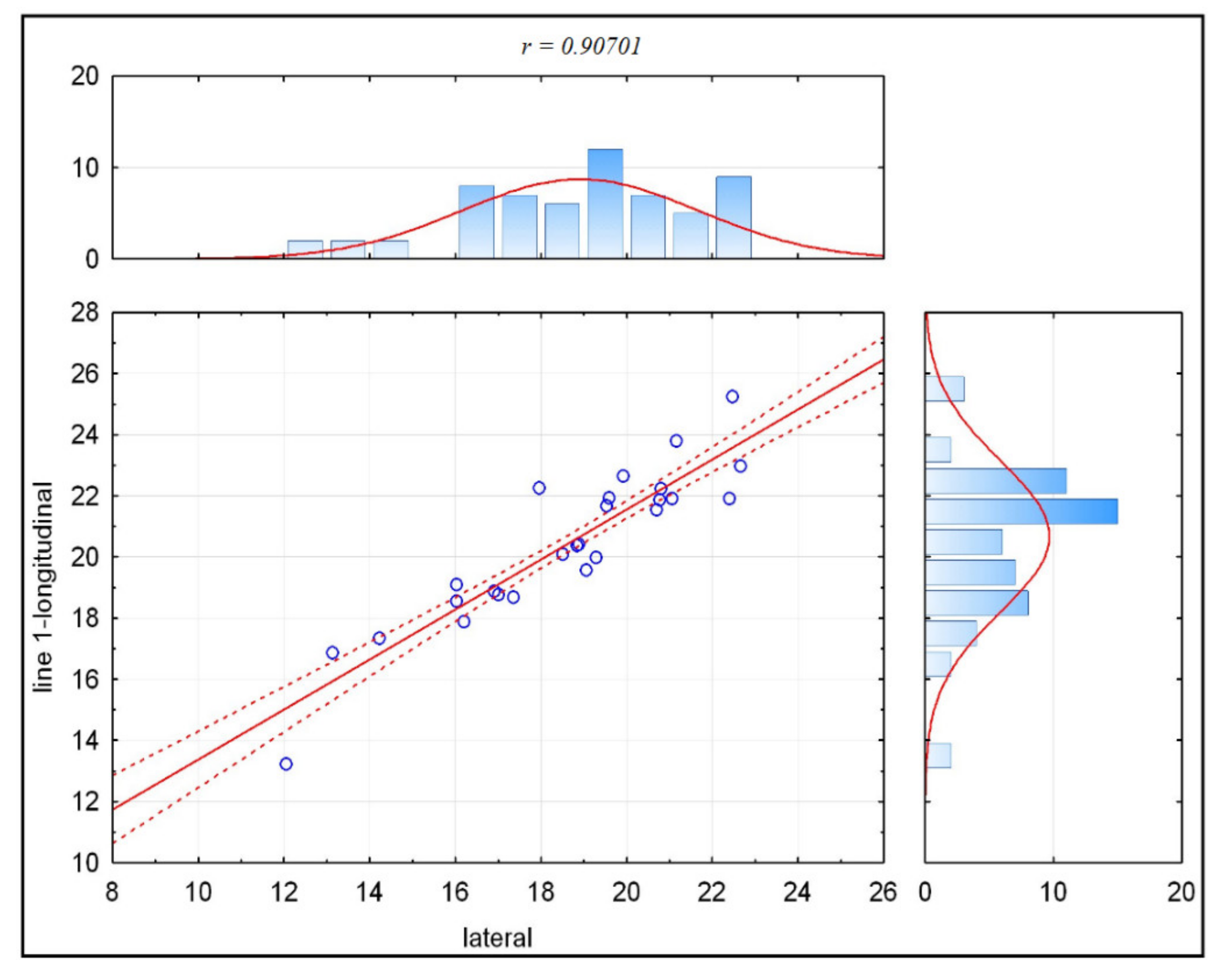
3.2.1. Whole Population Correlation
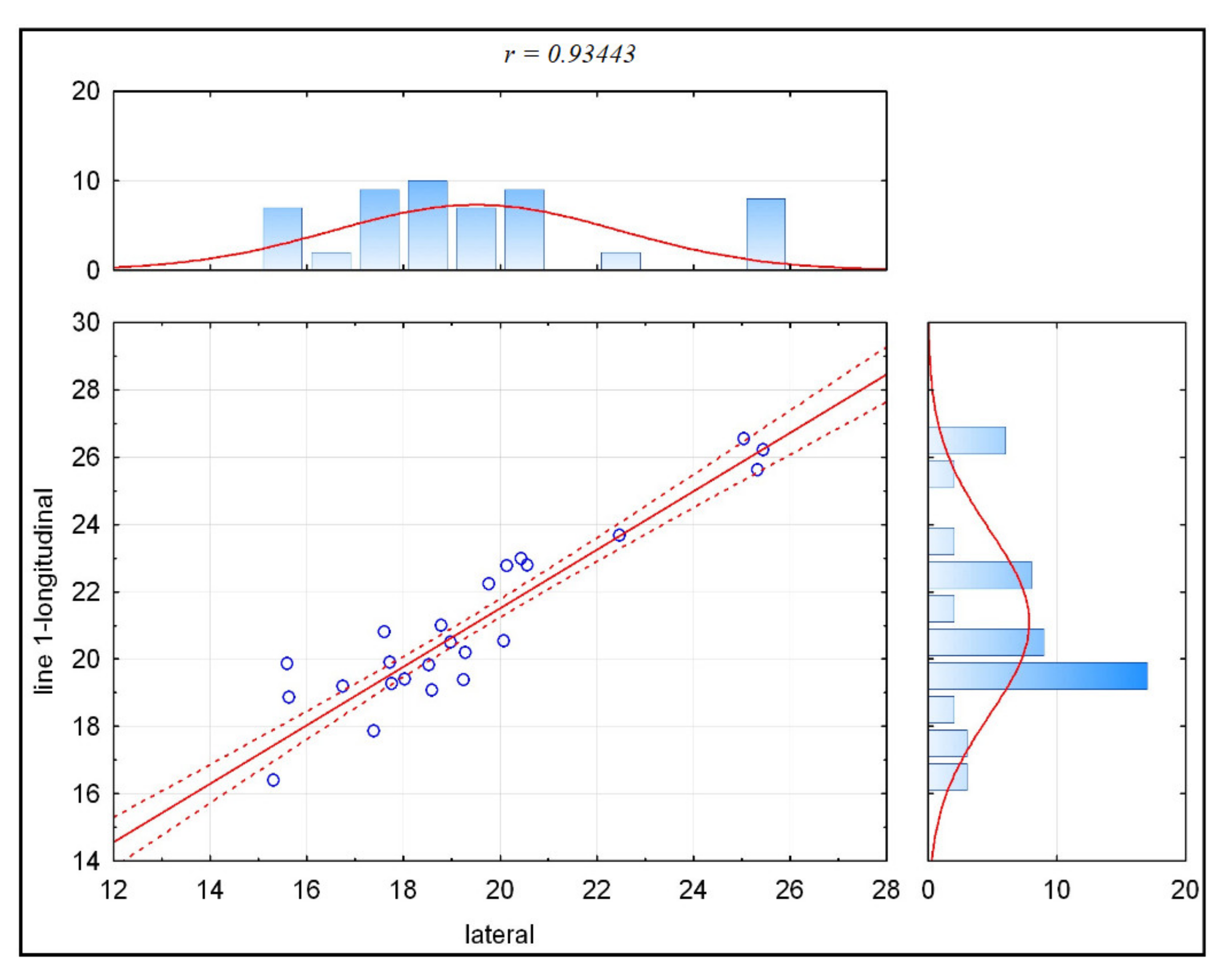
3.2.2. Female Group Correlation
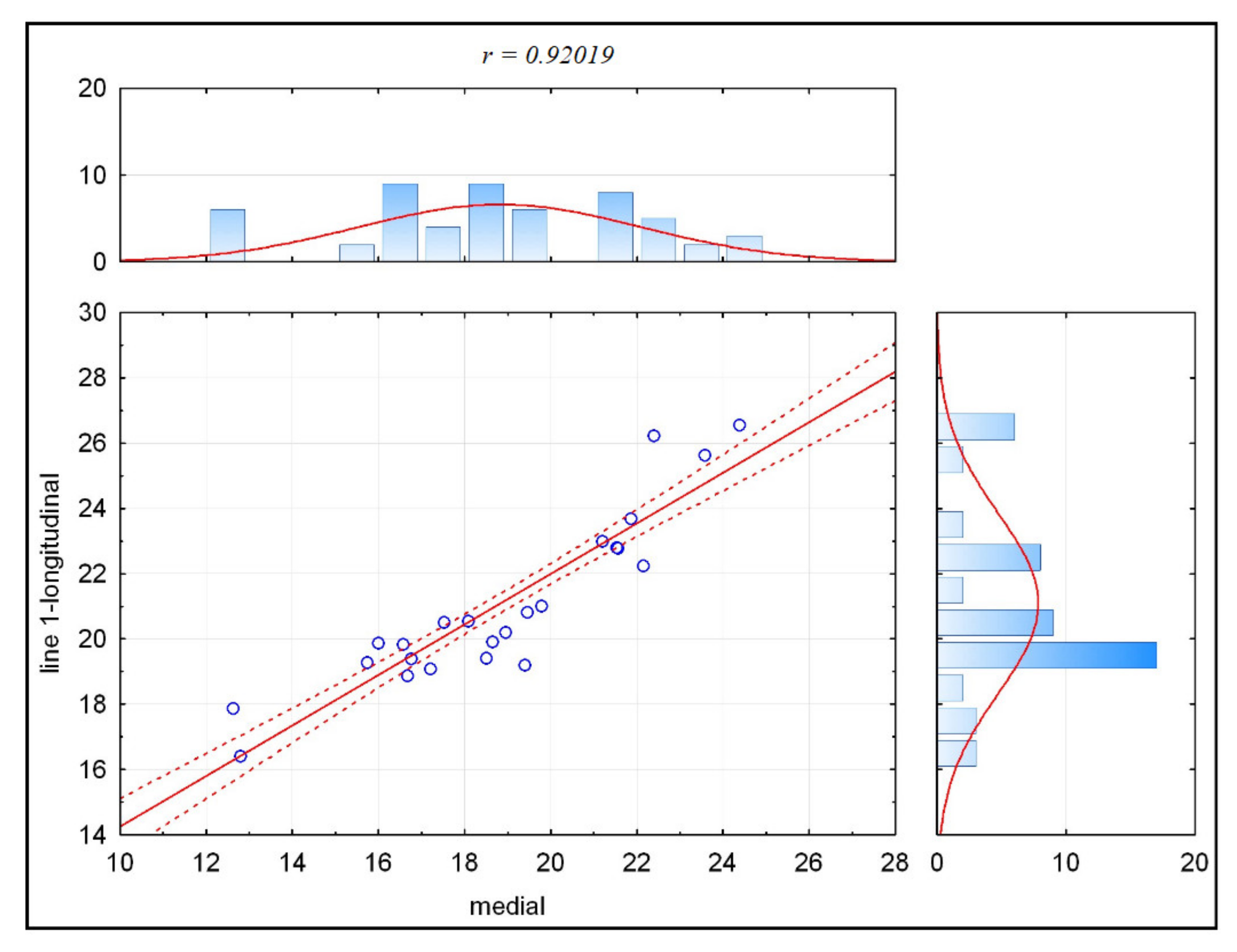
3.2.3. Male Group Correlation
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Wentges, R.T. Surgical anatomy of the pterygopalatine fossa. Laryngology meeting. R. Soc. Med. 1974, 89, 35–45. [Google Scholar]
- Hwang, K.; Lee, D.K.; Chung, I.H.; Lee, S.I. Le Fort I osteotomy with sparing fracture of lateral pterygoid plate. J. Craniofac. Surg. 2001, 12, 48–52. [Google Scholar] [CrossRef] [PubMed]
- Chin, Y.P.; Leno, M.B.; Dumrongwongsiri, S.; Chung, K.H.; Lin, H.H.; Lo, L.J. The pterygomaxillary junction: An imaging study for surgical information of LeFort I osteotomy. Sci. Rep. 2017, 7, 9953. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nish, I.; Pynn, B.; Holmes, H.; Young, E. Maxillary nerve block: A case report and review of the intraoral technique. J. Can. Assoc. 1995, 61, 305–310. [Google Scholar]
- Icen, M.; Orhan, K. Cone-beam computed tomography evaluation of the pterygomaxillary fissure and pterygopalatine fossa using 3D rendering programs. Surg. Radiol. Anat. 2019, 41, 513–522. [Google Scholar] [CrossRef] [PubMed]
- Puche-Torres, M.; Blasco-Serra, A.; Campos-Peláez, A.; Valverde-Navarro, A.A. Radiological anatomy assessment of the fissura pterygomaxillaris for a surgical approach to ganglion pterygopalatinum. J. Anat. 2017, 231, 961–969. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Melsen, B.; Melsen, F. The postnatal development of the palatomaxillary region studied on human autopsy material. Am. J. Orthod. 1982, 82, 329–342. [Google Scholar] [CrossRef]
- Kanazawa, T.; Kuroyanagi, N.; Miyachi, H.; Ochiai, S.; Kamiya, N.; Nagao, T.; Shimozato, K. Factors predictive of pterygoid process fractures after pterygomaxillary separation without using an osteotome in Le Fort I osteotomy. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2013, 115, 310–318. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.P.; Paik, K.S.; Kim, M.K. Anatomical study of the pyramidal process of the palatine bone in relation to implant placement in the posterior maxilla. J. Oral Rehabil. 2001, 28, 125–132. [Google Scholar] [CrossRef] [PubMed]
- Dargaud, J.; Cotton, F.; Buttin, R.; Morin, A. The maxillary sinus: Evolution and function in aging. Morphologie 2003, 87, 17–22. [Google Scholar] [PubMed]
- Ihde, S.; Pałka, Ł.; Jarząb, S.; Janeczek, M.; Goździewska-Harłajczuk, K.; Klećkowska-Nawrot, J.; Janus, I.; Dobrzyński, M. Three-dimensional determination of the fusion zone between the distal maxilla and the pterygoid plate of the sphenoid bone and considerations for implant Treatment Procedure. Appl. Sci. 2021, 11, 30. [Google Scholar] [CrossRef]
- Neema, B.; Olabu, B.O.; Butt, F.M.A.; Idenya, P.M.; Cheruiyot, I.; Misiani, M. Computed tomography scan assessment of the anatomy of the pterygomaxillary junction and its relevance in Le Fort I Osteotomy. J. Craniofac. Surg. 2020, 7, 2017–2020. [Google Scholar] [CrossRef] [PubMed]
- Uchida, Y.; Yamashita, Y.; Danjo, A.; Shibata, K.; Kuraoka, A. Computed tomography and anatomical measurements of critical sites for endosseous implants in the pterygomaxillary region: A cadaveric study. Int. J. Oral Maxillofac. Surg. 2017, 46, 798–804. [Google Scholar] [CrossRef] [PubMed]
- Odabaşı, O.; Erkmen, E.; Özlem Üçok, C.; Akif Bakir, M.; Yıldızer Keriş, E.; Şahin, O. Morphometric analysis of pterygomaxillary region by using cone beam computed tomography. J. Stomatol. Oral Maxillofac. Surg. 2021, 122, 273–277. [Google Scholar] [CrossRef] [PubMed]
- Icen, M.; Orhan, K.; Oz, U.; Horasan, S.; Avsever, H. Relationship between pterygomaxillary fissure morphology and maxillary/mandibular position: A cone beam computed tomography assessment. J. Orofac. Orthop. 2020, 81, 183–191. [Google Scholar] [CrossRef] [PubMed]
- Lentzen, M.P.; Safi, A.F.; Riekert, M.; Visser-Vandewalle, V.; Grandoch, A.; Zirk, M.; Zöller, J.E.; Kreppel, M. Analysis of the pterygomaxillary fissure for surgical approach to sphenopalatine ganglion by radiological examination of cone beeam computed tomography. J. Craniofac. Surg. 2020, 31, e95–e99. [Google Scholar] [CrossRef] [PubMed]
- Oliveira, G.Q.V.; Rossi, M.A.; Vasconcelos, T.V.; Neves, F.S.; Crusoé-Rebello, I. Cone beam computed tomography assessment of the pterygomaxillary region and palatine canal for Le Fort I osteotomy. Int. J. Oral Maxillofac. Surg. 2017, 46, 1017–1023. [Google Scholar] [CrossRef] [PubMed]
- Al-Imam, A.; Abdul-Wahaab, I.T.; Konuri, V.K.; Sahai, A. Reconciling artificial intelligence and non-Bayesian models for pterygomaxillary morphometrics. Folia Morphol. 2021. [Google Scholar] [CrossRef]
- Schatzker, J.; Horne, J.G.; Sumner-Smith, G. The reaction of cortical bone to compression by screw threads. Clin. Orthop. Relatt. Res. 1975, 111, 263–265. [Google Scholar] [CrossRef] [PubMed]
- Lazarov, A. Immediate functional loading: Results for the concept of the strategic implant®. Ann. Maxillofac. Surg. 2019, 9, 78–88. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameters | Mean | Median | SD |
|---|---|---|---|
| lateral [mm] | 18.28 | 18.81 | 3.38 |
| medial [mm] | 18.59 | 19.01 | 3.04 |
| rostral [mm] | 6.02 | 5.87 | 0.91 |
| caudal [mm] | 8.66 | 8.36 | 1.36 |
| area [mm2] | 150.99 | 151.52 | 39.76 |
| line-1 longitudinal [mm] | 19.9 | 20.14 | 3.25 |
| line-2 transverse [mm] | 7.58 | 7.63 | 0.93 |
| Parameters | Lateral | Medial | Rostral | Caudal | Area | Line-1 Longitudinal | Line-2 Transverse |
|---|---|---|---|---|---|---|---|
| lateral | 0.75 | 0.48 | 0.62 | 0.92 | 0.51 | ||
| medial | 0.75 | 0.51 | 0.59 | 0.90 | 0.41 | ||
| rostral | 0.59 | ||||||
| caudal | 0.48 | 0.51 | 0.60 | 0.42 | 0.76 | ||
| area | 0.62 | 0.59 | 0.60 | 0.65 | 0.62 | ||
| line-1 longitudinal | 0.92 | 0.90 | 0.42 | 0.65 | 0.46 | ||
| line-2 transverse | 0.51 | 0.41 | 0.59 | 0.76 | 0.62 | 0.46 |
| Parameters | Age | Lateral | Medial | Rostral | Caudal | Area | Line-1 Longitudinal | Line-2 Transverse |
|---|---|---|---|---|---|---|---|---|
| age | 0.36 | 0.27 | 0.31 | |||||
| lateral | 0.36 | 0.71 | 0.40 | 0.57 | 0.91 | 0.46 | ||
| medial | 0.27 | 0.71 | 0.49 | 0.89 | 0.40 | |||
| rostral | 0.49 | |||||||
| caudal | 0.40 | 0.59 | 0.30 | 0.89 | ||||
| area | 0.57 | 0.49 | 0.59 | 0.57 | 0.63 | |||
| line-1 longitudinal | 0.31 | 0.91 | 0.89 | 0.30 | 0.57 | 0.40 | ||
| line-2 transverse | 0.46 | 0.40 | 0.49 | 0.89 | 0.63 | 0.40 |
| Parameters | Age | Lateral | Medial | Rostral | Caudal | Area | Line-1 Longitudinal | Line-2Ttransverse |
|---|---|---|---|---|---|---|---|---|
| age | −0.30 | −0.38 | −0.45 | |||||
| lateral | −0.30 | 0.81 | 0.58 | 0.76 | 0.93 | 0.60 | ||
| medial | −0.38 | 0.81 | 0.56 | 0.82 | 0.92 | 0.50 | ||
| rostral | 0.76 | |||||||
| caudal | 0.58 | 0.56 | 0.63 | 0.56 | 0.49 | |||
| area | 0.76 | 0.82 | 0.63 | 0.83 | 0.66 | |||
| line-1 longitudinal | −0.45 | 0.93 | 0.92 | 0.56 | 0.83 | 0.57 | ||
| line-2 transverse | 0.60 | 0.50 | 0.76 | 0.49 | 0.66 | 0.57 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ihde, S.; Pałka, Ł.; Jarząb, S.; Janeczek, M.; Goździewska-Harłajczuk, K.; Klećkowska-Nawrot, J.; Janus, I.; Dobrzyński, M.; Karykowska, A. The Anatomy, Features and Sex Correlations (Dimorphism) of Tubero–Palato–Pterygoid Region among Adult Population—Single Center Study Based on 3D Printed Models. Appl. Sci. 2021, 11, 5450. https://0-doi-org.brum.beds.ac.uk/10.3390/app11125450
Ihde S, Pałka Ł, Jarząb S, Janeczek M, Goździewska-Harłajczuk K, Klećkowska-Nawrot J, Janus I, Dobrzyński M, Karykowska A. The Anatomy, Features and Sex Correlations (Dimorphism) of Tubero–Palato–Pterygoid Region among Adult Population—Single Center Study Based on 3D Printed Models. Applied Sciences. 2021; 11(12):5450. https://0-doi-org.brum.beds.ac.uk/10.3390/app11125450
Chicago/Turabian StyleIhde, Stefan, Łukasz Pałka, Sławomir Jarząb, Maciej Janeczek, Karolina Goździewska-Harłajczuk, Joanna Klećkowska-Nawrot, Izabela Janus, Maciej Dobrzyński, and Aleksandra Karykowska. 2021. "The Anatomy, Features and Sex Correlations (Dimorphism) of Tubero–Palato–Pterygoid Region among Adult Population—Single Center Study Based on 3D Printed Models" Applied Sciences 11, no. 12: 5450. https://0-doi-org.brum.beds.ac.uk/10.3390/app11125450