
Comparison of Accuracy of Alginate Impression and Intraoral Scanner in Model with and without Orthodontic Brackets


Abstract
:1. Introduction
2. Methodology
2.1. Fabrication of Dental Model
2.2. Alginate Impression
2.3. Scanning with TRIOS3 Intraoral Scanner (3Shape, Copenhagen, Denmark)
2.4. Attachment of Orthodontic Brackets
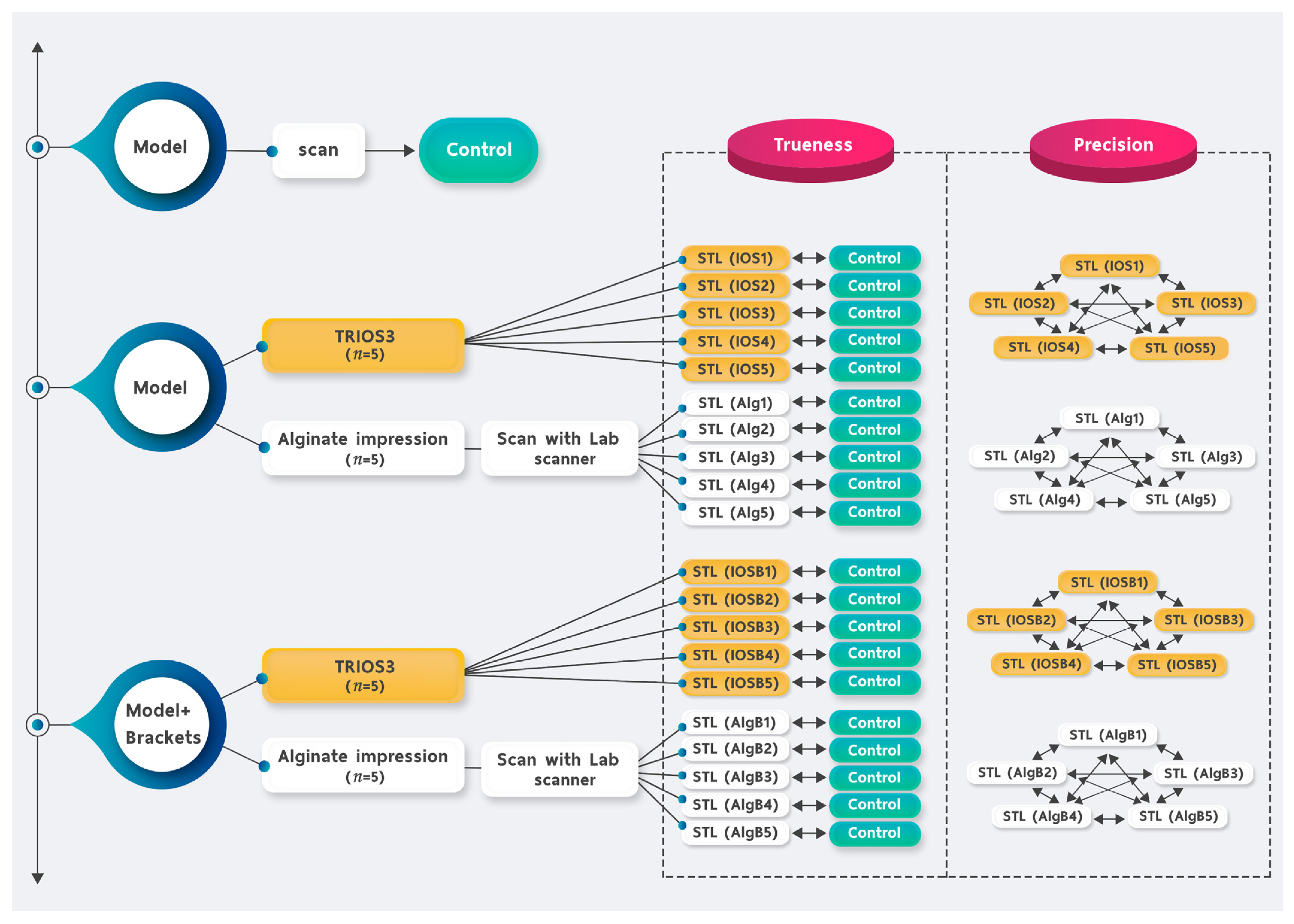
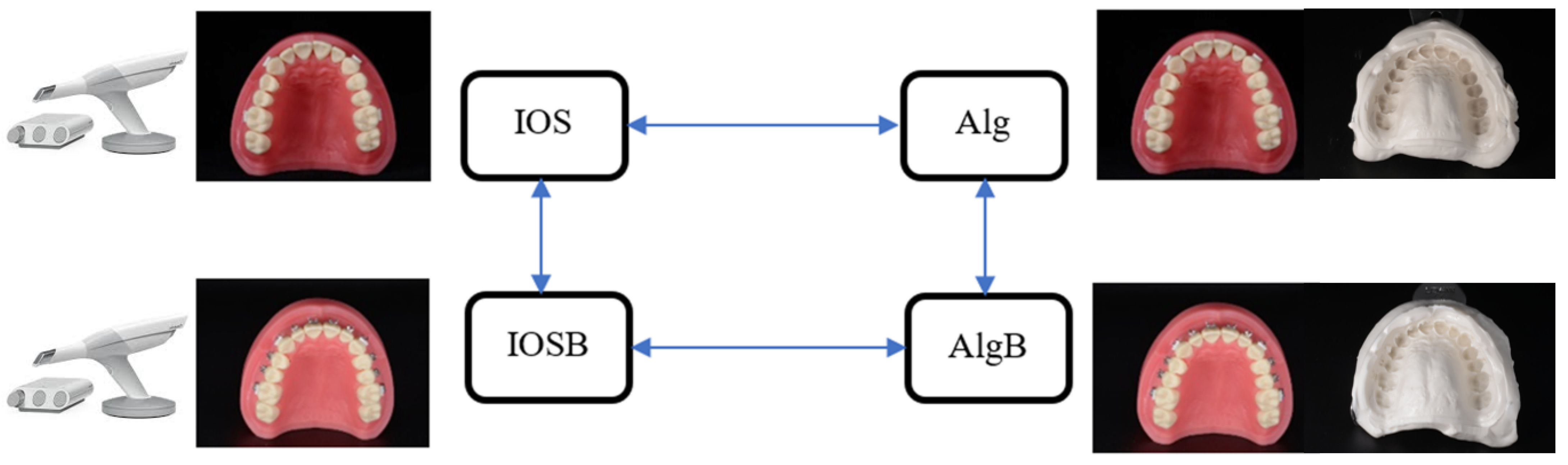
2.5. Measurements
2.6. Sample Size Calculation
2.7. Statistical Analysis
3. Results
3.1. Trueness
3.2. Precision
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Yuzbasioglu, E.; Kurt, H.; Turunc, R.; Bilir, H. Comparison of digital and conventional impression techniques: Evaluation of patients’ perception, treatment comfort, effectiveness and clinical outcomes. BMC Oral Health 2014, 14, 10. [Google Scholar] [CrossRef] [Green Version]
- Mangano, F.; Gandolfi, A.; Luongo, G.; Logozzo, S. Intraoral scanners in dentistry: A review of the current literature. BMC Oral Health 2017, 17, 149. [Google Scholar] [CrossRef] [Green Version]
- Keating, A.P.; Knox, J.; Bibb, R.; Zhurov, A.I. A comparison of plaster, digital and reconstructed study model accuracy. J. Orthod. 2008, 35, 191–201. [Google Scholar] [CrossRef]
- Ender, A.; Mehl, A. In-vitro evaluation of the accuracy of conventional and digital methods of obtaining full-arch dental impressions. Quintessence Int. 2015, 46, 9–17. [Google Scholar]
- Zimmermann, M.; Koller, C.; Rumetsch, M.; Ender, A.; Mehl, A. Precision of guided scanning procedures for full-arch digital impressions in vivo. J. Orofac. Orthop. 2017, 78, 466–471. [Google Scholar] [CrossRef] [PubMed]
- Ender, A.; Mehl, A. Accuracy in dental medicine, a new way to measure trueness and precision. J. Vis. Exp. 2014, 86, e51374. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Todd, J.A.; Oesterle, L.J.; Newman, S.M.; Shellhart, W.C. Dimensional changes of extended-pour alginate impression materials. Am. J. Orthod. Dentofac. Orthop. 2013, 143, S55–S63. [Google Scholar] [CrossRef]
- Andriessen, F.S.; Rijkens, D.R.; van der Meer, W.J.; Wismeijer, D.W. Applicability and accuracy of an intraoral scanner for scanning multiple implants in edentulous mandibles: A pilot study. J. Prosthet. Dent. 2014, 111, 186–194. [Google Scholar] [CrossRef] [PubMed]
- Giménez, B.; Özcan, M.; Martínez-Rus, F.; Pradíes, G. Accuracy of a digital impression system based on active wavefront sampling technology for implants considering operator experience, implant angulation, and depth. Clin. Implant. Dent. Relat. Res. 2015, 17, e54–e64. [Google Scholar] [CrossRef] [PubMed]
- Ender, A.; Mehl, A. Influence of scanning strategies on the accuracy of digital intraoral scanning systems. Int. J. Comput. Dent. 2013, 16, 11–21. [Google Scholar]
- Nedelcu, R.; Olsson, P.; Nyström, I.; Rydén, J.; Thor, A. Accuracy and precision of 3 intraoral scanners and accuracy of conventional impressions: A novel in vivo analysis method. J. Dent. 2018, 69, 110–118. [Google Scholar] [CrossRef] [PubMed]
- Hayama, H.; Fueki, K.; Wadachi, J.; Wakabayashi, N. Trueness and precision of digital impressions obtained using an intraoral scanner with different head size in the partially edentulous mandible. J. Prosthodont. Res. 2018, 62, 347–352. [Google Scholar] [CrossRef] [PubMed]
- Amornvit, P.; Sanohkan, S.; Peampring, C. Studying the Optical 3D Accuracy of Intraoral Scans: An In Vitro Study. J. Healthc. Eng. 2020, 2020, 5739312. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Park, J.M.; Choi, S.A.; Myung, J.Y.; Chun, Y.S.; Kim, M. Impact of Orthodontic Brackets on the Intraoral Scan Data Accuracy. BioMed Res. Int. 2016, 2016, 5075182. [Google Scholar] [CrossRef]
- Abduo, J.; Elseyoufi, M. Accuracy of Intraoral Scanners: A Systematic Review of Influencing Factors. Eur. J. Prosthodont. Restor. Dent. 2018, 26, 101–121. [Google Scholar]
- Liczmanski, K.; Stamm, T.; Sauerland, C.; Blanck-Lubarsch, M. Accuracy of intraoral scans in the mixed dentition: A prospective non-randomized comparative clinical trial. Head Face Med. 2020, 16, 11. [Google Scholar] [CrossRef]
- Tomita, Y.; Uechi, J.; Konno, M.; Sasamoto, S.; Iijima, M.; Mizoguchi, I. Accuracy of digital models generated by conventional impression/plaster-model methods and intraoral scanning. Dent. Mater. J. 2018, 37, 628–633. [Google Scholar] [CrossRef] [Green Version]
- Peutzfeldt, A.; Asmussen, E. Accuracy of alginate and elastomeric impression materials. Scand. J. Dent. Res. 1989, 97, 375–379. [Google Scholar] [CrossRef]
- Ender, A.; Attin, T.; Mehl, A. In vivo precision of conventional and digital methods of obtaining complete-arch dental impressions. J. Prosthet. Dent. 2016, 115, 313–320. [Google Scholar] [CrossRef] [Green Version]
- Malik, J.; Rodriguez, J.; Weisbloom, M.; Petridis, H. Comparison of Accuracy Between a Conventional and Two Digital Intraoral Impression Techniques. Int. J. Prosthodont. 2018, 31, 107–113. [Google Scholar] [CrossRef]
- Mangano, F.G.; Veronesi, G.; Hauschild, U.; Mijiritsky, E.; Mangano, C. Trueness and Precision of Four Intraoral Scanners in Oral Implantology: A Comparative in Vitro Study. PLoS ONE 2016, 11, e0163107. [Google Scholar] [CrossRef] [PubMed]
- Winkler, J.; Gkantidis, N. Trueness and precision of intraoral scanners in the maxillary dental arch: An in vivo analysis. Sci. Rep. 2020, 10, 1172. [Google Scholar] [CrossRef] [Green Version]
- Amornvit, P.; Rokaya, D.; Peampring, C.; Sanohkan, S. Confocal 3d optical intraoral scanners and comparison of image capturing accuracy. Comput. Mater. Contin. 2021, 66, 303–314. [Google Scholar] [CrossRef]
- Kang, S.J.; Kee, Y.J.; Lee, K.C. Effect of the presence of orthodontic brackets on intraoral scans. Angle Orthod. 2021, 91, 98–104. [Google Scholar] [CrossRef] [PubMed]
- Schirmer, U.R.; Wiltshire, W.A. Manual and computer-aided space analysis: A comparative study. Am. J. Orthod. Dentofac. Orthop. 1997, 112, 676–680. [Google Scholar] [CrossRef]
- Hiroki, Y.; Sohmura, T.; Satoh, H.; Takahashi, J.; Takada, K. Complete 3-D reconstruction of dental cast shape using perceptual grouping. IEEE Trans. Med. Imaging 2001, 20, 1093–1101. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Upper Arch | IOS Mean ± SD (Min-Max) (Micron) | Alginate Impression Mean ± SD (Min-Max) (Micron) | Repeated Measure ANOVA * (p-Value) |
|---|---|---|---|
| Without brackets | 86.80 ± 3.11 (85–101) | 89.60 ± 3.97 (88–96) | 0.606 |
| With brackets | 90.80 ± 1.64 (72–94) | 92.80 ± 2.49 (88–100) | 0.451 |
| Repeated measure ANOVA * (p-value) | 0.555 | 1.000 |
| Lower Arch | IOS Mean ± SD (Min-Max) (Micron) | Alginate Impression Mean ± SD (Min-Max) (Micron) | Repeated Measure ANOVA * (p-Value) |
|---|---|---|---|
| Without brackets | 88.00 ± 7.69 (78–104) | 92.40 ± 3.95 (87–97) | 1.000 |
| With brackets | 94.70 ± 6.43 (85–102) | 96.10 ± 5.99 (93–102) | 1.000 |
| Repeated measure ANOVA * (p-value) | 0.461 | 0.188 |
| Upper Arch | IOS Mean ± SD (Min-Max) (Micron) | Alginate Impression Mean ± SD (Min-Max) (Micron) | Repeated Measure ANOVA * (p-Value) |
|---|---|---|---|
| Without brackets | 90.80 ± 3.03 (79–98) | 92.00 ± 3.81 (80–93) | 1.000 |
| With brackets | 93.20 ± 2.39 (92–108) | 94.00 ± 5.24 (80–103) | 1.000 |
| Repeated measure ANOVA * (p-value) | 0.365 | 1.000 |
| Lower Arch | IOS Mean ± SD (Min-Max) (Micron) | Alginate Impression Mean ± SD (Min-Max) (Micron) | Repeated Measure ANOVA * (p-Value) |
|---|---|---|---|
| Without brackets | 94.90 ± 4.09 (85–100) | 92.40 ± 4.55 (87–99) | 1.000 |
| With brackets | 96.80 ± 4.69 (94–104) | 95.30 ± 1.95 (94–100) | 0.210 |
| Repeated measure ANOVA * (p-value) | 1.000 | 0.803 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Phudphong, P.; Amornvit, P.; Sirintawat, N. Comparison of Accuracy of Alginate Impression and Intraoral Scanner in Model with and without Orthodontic Brackets. Appl. Sci. 2021, 11, 6037. https://0-doi-org.brum.beds.ac.uk/10.3390/app11136037
Phudphong P, Amornvit P, Sirintawat N. Comparison of Accuracy of Alginate Impression and Intraoral Scanner in Model with and without Orthodontic Brackets. Applied Sciences. 2021; 11(13):6037. https://0-doi-org.brum.beds.ac.uk/10.3390/app11136037
Chicago/Turabian StylePhudphong, Pitchapa, Pokpong Amornvit, and Nattapong Sirintawat. 2021. "Comparison of Accuracy of Alginate Impression and Intraoral Scanner in Model with and without Orthodontic Brackets" Applied Sciences 11, no. 13: 6037. https://0-doi-org.brum.beds.ac.uk/10.3390/app11136037