
Assessing Movement Quality in Youth Footballers: The Relationship between Hip and Lower Limb Movement Screen and Functional Movement Screen

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Setting and Study Design
2.2. Sample
2.3. Functional Movement Screen
2.4. Hip and Lower Limb Movement Screen
2.5. Statistical Analysis
3. Results
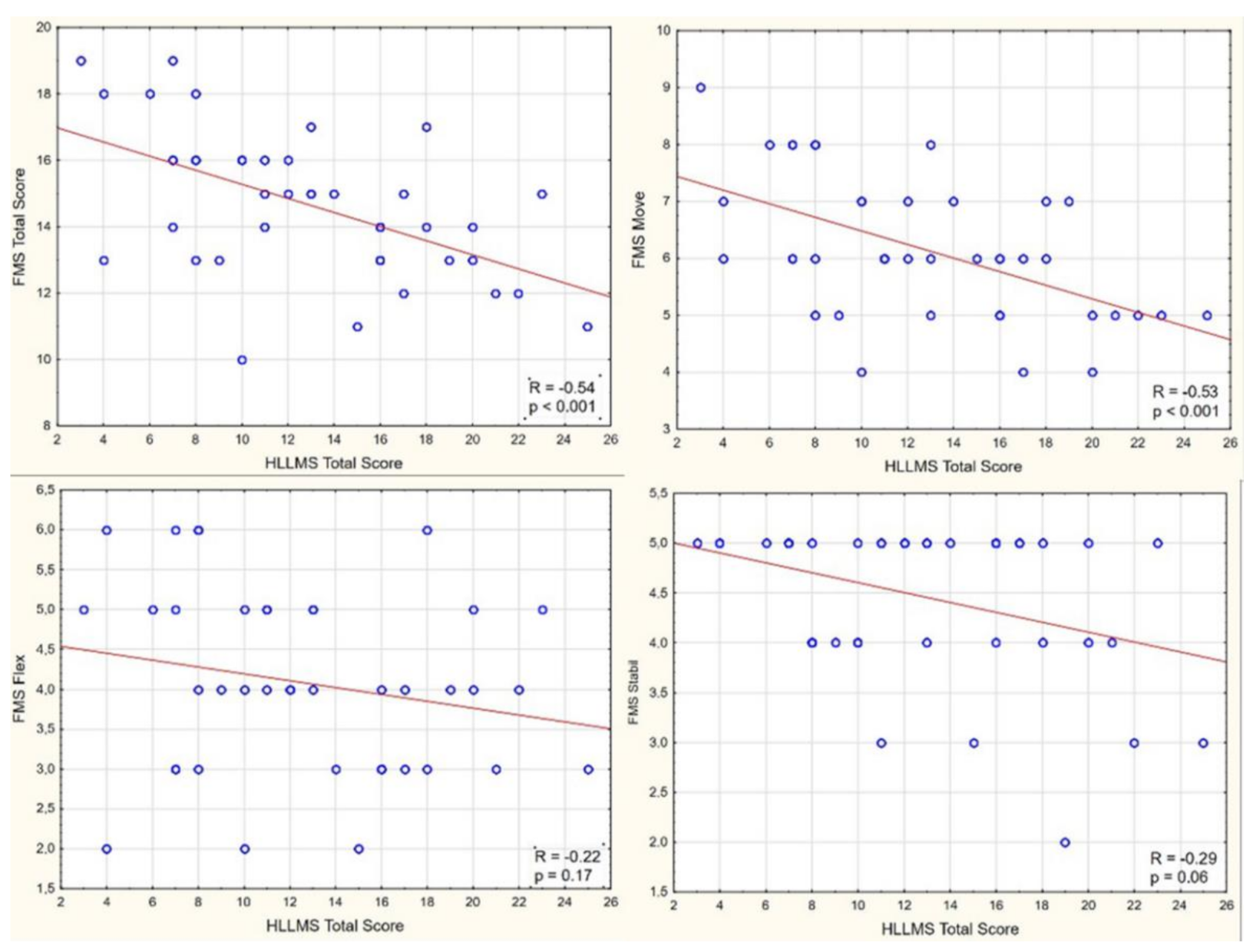
3.1. Total Score
3.2. Asymmetrical Tasks
3.3. Symmetrical Tasks
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Reiman, M.P.; Bolgla, L.A.; Lorenz, D. Hip functions influence on knee dysfunction: A proximal link to a distal problem. J. Sport Rehabil. 2009, 18, 33–46. [Google Scholar] [CrossRef] [PubMed]
- Hewett, T.E.; Myer, G.D.; Ford, K.; Heidt, R.S.; Colosimo, A.J.; McLean, S.G.; Bogert, A.V.D.; Paterno, M.V.; Succop, P. Biomechanical measures of neuromuscular control and valgus loading of the knee predict anterior cruciate ligament injury risk in female athletes: A prospective study. Am. J. Sports Med. 2005, 33, 492–501. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Powers, C.M. The influence of abnormal hip mechanics on knee injury: A biomechanical perspective. J. Orthop. Sports Phys. Ther. 2010, 40, 42–51. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chimera, N.J.; Warren, M. Use of clinical movement screening tests to predict injury in sport. World J. Orthop. 2016, 7, 202–217. [Google Scholar] [CrossRef]
- Booysen, N.; Wilson, D.A.; Lewis, C.L.; Warner, M.B.; Gimpel, M.; Mottram, S.; Comerford, M.; Stokes, M. Assessing movement quality using the hip and lower limb movement screen: Development, reliability and potential applications. J. Musculoskelet. Res. 2019, 22, 1950008. [Google Scholar] [CrossRef]
- Cook, G.; Burton, L.; Hoogenboom, B. Pre-participation screening: The use of fundamental movements as an assessment of function—Part 2. N. Am. J. Sports Phys. Ther. 2006, 1, 132–139. [Google Scholar]
- Cook, G.; Burton, L.; Hoogenboom, B. Pre-participation screening: The use of fundamental movements as an assessment of function—Part 1. N. Am. J. Sports Phys. Ther. 2006, 1, 62–72. [Google Scholar]
- Bonazza, N.A.; Smuin, D.; Onks, C.A.; Silvis, M.L.; Dhawan, A. Reliability, validity, and injury predictive value of the functional movement screen: A systematic review and meta-analysis. Am. J. Sports Med. 2016, 45, 725–732. [Google Scholar] [CrossRef]
- Cuchna, J.W.; Hoch, M.C.; Hoch, J.M. The interrater and intrarater reliability of the functional movement screen: A systematic review with meta-analysis. Phys. Ther. Sport 2016, 19, 57–65. [Google Scholar] [CrossRef] [PubMed]
- Moran, R.W.; Schneiders, A.G.; Mason, J.; Sullivan, S.J. Do Functional Movement Screen (FMS) composite scores predict subsequent injury? A systematic review with meta-analysis. Br. J. Sports Med. 2017, 51, 1661–1669. [Google Scholar] [CrossRef]
- Whittaker, J.; Booysen, N.; De La Motte, S.; Dennett, L.; Lewis, C.L.; Wilson, D.; McKay, C.; Warner, M.; Padua, D.; Emery, C.A.; et al. Predicting sport and occupational lower extremity injury risk through movement quality screening: A systematic review. Br. J. Sports Med. 2016, 51, 580–585. [Google Scholar] [CrossRef] [Green Version]
- Zeller, B.L.; McCrory, J.L.; Ben Kibler, W.; Uhl, T.L. Differences in kinematics and electromyographic activity between men and women during the single-legged squat. Am. J. Sports Med. 2003, 31, 449–456. [Google Scholar] [CrossRef] [PubMed]
- Bagwell, J.J.; Powers, C.M. The influence of squat kinematics and cam morphology on acetabular stress. Arthrosc. J. Arthrosc. Relat. Surg. 2017, 33, 1797–1803. [Google Scholar] [CrossRef] [PubMed]
- Ng, G.K.C.; Mantovani, G.; Lamontagne, M.; Labrosse, M.R.; Beaulé, P.E. Increased hip stresses resulting from a cam deformity and decreased femoral neck-shaft angle during level walking. Clin. Orthop. Relat. Res. 2017, 475, 998–1008. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bennell, K.; Hunter, D.J.; Vicenzino, B. Long-term effects of sport: Preventing and managing OA in the athlete. Nat. Rev. Rheumatol. 2012, 8, 747–752. [Google Scholar] [CrossRef]
- Kerbel, Y.E.; Smith, C.M.; Prodromo, J.P.; Nzeogu, M.I.; Mulcahey, M.K. Epidemiology of Hip and Groin Injuries in Collegiate Athletes in the United States. Orthop. J. Sports Med. 2018, 6, 2325967118771676. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Crow, J.F.; Pearce, A.J.; Veale, J.P.; Van der Westhuizen, D.; Coburn, P.T.; Pizzari, T. Hip adductor muscle strength is reduced preceding and during the onset of groin pain in elite junior Australian football players. J. Sci. Med. Sport 2010, 13, 202–204. [Google Scholar] [CrossRef]
- Lovell, G.; Galloway, H.; Hopkins, W.; Harvey, A. Osteitis pubis and assessment of bone marrow edema at the pubic symphysis with MRI in an elite junior male soccer squad. Clin. J. Sport Med. 2006, 16, 117–122. [Google Scholar] [CrossRef]
- Whittaker, J.; Woodhouse, L.; Nettel-Aguirre, A.; Emery, C. Outcomes associated with early post-traumatic osteoarthritis and other negative health consequences 3–10 years following knee joint injury in youth sport. Osteoarthr. Cartil. 2015, 23, 1122–1129. [Google Scholar] [CrossRef] [Green Version]
- Samar, Z.; Bansal, A. The relationship between self-reported and on field lower extremity functional assessment tools used for assessing functional status in hip dysfunction athletes. Int. J. Sports Sci. 2013, 3, 172–182. [Google Scholar]
- Linek, P.; Booysen, N.; Sikora, D.; Stokes, M. Functional movement screen and Y balance tests in adolescent footballers with hip/groin symptoms. Phys. Ther. Sport 2019, 39, 99–106. [Google Scholar] [CrossRef] [PubMed]
- Wilson, D.A.; Booysen, N.; Dainese, P.; Heller, M.O.; Stokes, M.; Warner, M.B. Accuracy of movement quality screening to document effects of neuromuscular control retraining exercises in a young ex-footballer with hip and groin symptoms: A proof of concept case study. Med. Hypotheses 2018, 120, 116–120. [Google Scholar] [CrossRef] [Green Version]
- Booysen, N.; Wilson, D.; Hawkes, R.; Dickenson, E.; Stokes, M.; Warner, M. Characterising movement patterns in elite male professional golfers using an observational hip and lower limb movement screen. Osteoarthr. Cartil. 2017, 25, S356. [Google Scholar] [CrossRef] [Green Version]
- Botha, N.; Warner, M.; Gimpel, M.; Mottram, S.; Comerford, M.; Stokes, M. Movement patterns during a small knee bend test in academy footballers with femoroacetabular impingement (FAI). Health Sci. Work. Pap. 2014, 1, 10. [Google Scholar]
- Kazman, J.B.; Galecki, J.M.; Lisman, P.; Deuster, P.A.; O’Connor, F.G. Factor structure of the functional movement screen in marine officer candidates. J. Strength Cond. Res. 2014, 28, 672–678. [Google Scholar] [CrossRef]
- Portas, M.D.; Parkin, G.; Roberts, J.; Batterham, A. Maturational effect on functional movement Screen™ score in adolescent soccer players. J. Sci. Med. Sport 2015, 19, 854–858. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schober, P.; Boer, C.; Schwarte, L.A. Correlation coefficients. Anesth. Analg. 2018, 126, 1763–1768. [Google Scholar] [CrossRef] [PubMed]
- Agresta, C.; Slobodinsky, M.; Tucker, C. Functional Movement Screen™—Normative values in healthy distance runners. Int. J. Sports Med. 2014, 35, 1203–1207. [Google Scholar] [CrossRef]
- Noehren, B.; Davis, I.; Hamill, J. ASB clinical biomechanics award winner 2006: Prospective study of the biomechanical factors associated with iliotibial band syndrome. Clin. Biomech. 2007, 22, 951–956. [Google Scholar] [CrossRef] [PubMed]
- Powers, C.M. The influence of altered lower-extremity kinematics on patellofemoral joint dysfunction: A theoretical perspective. J. Orthop. Sports Phys. Ther. 2003, 33, 639–646. [Google Scholar] [CrossRef]
- Lamontagne, M.; Kennedy, M.J.; Beaulé, P.E. The effect of cam FAI on hip and pelvic motion during maximum squat. Clin. Orthop. Relat. Res. 2009, 467, 645–650. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hammond, C.A.; Hatfield, G.L.; Gilbart, M.K.; Garland, S.J.; Hunt, M.A. Trunk and lower limb biomechanics during stair climbing in people with and without symptomatic femoroacetabular impingement. Clin. Biomech. 2017, 42, 108–114. [Google Scholar] [CrossRef] [PubMed]
- Diamond, L.E.; Bennell, K.L.; Wrigley, T.V.; Hinman, R.S.; Hall, M.; O’Donnell, J.; Hodges, P.W. Trunk, pelvis and hip biomechanics in individuals with femoroacetabular impingement syndrome: Strategies for step ascent. Gait Posture 2018, 61, 176–182. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- King, M.G.; Lawrenson, P.; Semciw, A.; Middleton, K.; Crossley, K.M. Lower limb biomechanics in femoroacetabular impingement syndrome: A systematic review and meta-analysis. Br. J. Sports Med. 2018, 52, 566–580. [Google Scholar] [CrossRef] [Green Version]
- Lewis, C.L.; Loverro, K.L.; Khuu, A. Kinematic differences during single-leg step-down between individuals with femoroacetabular impingement syndrome and individuals without hip pain. J. Orthop. Sports Phys. Ther. 2018, 48, 270–279. [Google Scholar] [CrossRef] [PubMed]
- Neal, B.S.; Barton, C.; Gallie, R.; O’Halloran, P.; Morrissey, D. Runners with patellofemoral pain have altered biomechanics which targeted interventions can modify: A systematic review and meta-analysis. Gait Posture 2015, 45, 69–82. [Google Scholar] [CrossRef]
- Warner, M.B.; Wilson, D.A.; Herrington, L.; Dixon, S.; Power, C.; Jones, R.; Heller, M.O.; Carden, P.; Lewis, C.L. A systematic review of the discriminating biomechanical parameters during the single leg squat. Phys. Ther. Sport 2019, 36, 78–91. [Google Scholar] [CrossRef]
- Sahrmann, S.; Azevedo, D.C.; Van Dillen, L. Diagnosis and treatment of movement system impairment syndromes. Braz. J. Phys. Ther. 2017, 21, 391–399. [Google Scholar] [CrossRef]
- Lee, R.Y.; Wong, T.K. Relationship between the movements of the lumbar spine and hip. Hum. Mov. Sci. 2002, 21, 481–494. [Google Scholar] [CrossRef]
- Newton, F.; McCall, A.; Ryan, D.; Blackburne, C.; Der Fünten, K.A.; Meyer, T.; Lewin, C.; McCunn, R. Functional movement screen (fms™) score does not predict injury in English Premier League youth academy football players. Sci. Med. Footb. 2017, 1, 102–106. [Google Scholar] [CrossRef]
- Walbright, P.D.; Walbright, N.; Ojha, H.; Davenport, T. Validity of functional screening tests to predict lost-time lower quarter injury in a cohort of female collegiate athletes. Int. J. Sports Phys. Ther. 2017, 12, 948–959. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bailey, R.; Selfe, J.; Richards, J. The role of the Trendelenburg Test in the examination of gait. Phys. Ther. Rev. 2009, 14, 190–197. [Google Scholar] [CrossRef]
- Malloy, P.; Neumann, D.A.; Kipp, K. Hip biomechanics during a single-leg squat: 5 key differences between people with femoroacetabular impingement syndrome and those without hip pain. J. Orthop. Sports Phys. Ther. 2019, 49, 908–916. [Google Scholar] [CrossRef] [Green Version]
- Butler, R.J.; Lehr, M.E.; Fink, M.L.; Kiesel, K.B.; Plisky, P.J. Dynamic balance performance and noncontact lower extremity injury in college football players. Sports Health A Multidiscip. Approach 2013, 5, 417–422. [Google Scholar] [CrossRef] [Green Version]
- Kang, M.-H.; Kim, G.-M.; Kwon, O.-Y.; Weon, J.-H.; Oh, J.-S.; An, D.-H. Relationship between the kinematics of the trunk and lower extremity and performance on the Y-balance test. PM&R 2015, 7, 1152–1158. [Google Scholar] [CrossRef]
- Ko, J.; Rosen, A.B.; Brown, C.N. Functional performance deficits in adolescent athletes with a history of lateral ankle sprain(s). Phys. Ther. Sport 2018, 33, 125–132. [Google Scholar] [CrossRef] [PubMed]
- McCann, R.S.; Kosik, K.B.; Terada, M.; Beard, M.Q.; Buskirk, G.E.; Gribble, P.A. Associations between functional and isolated performance measures in college women’s soccer players. J. Sport Rehabil. 2017, 26, 376–385. [Google Scholar] [CrossRef] [PubMed]
- Jensen, U.; Weilbrenner, F.; Rott, F.; Eskofier, B. Sensor-based mobile functional movement screening. In Wireless Mobile Communication and Healthcare; Springer: Berlin/Heidelberg, Germany, 2013; Volume 61, pp. 215–223. [Google Scholar]
- Whiteside, D.; Deneweth, J.M.; Pohorence, M.A.; Sandoval, B.; Russell, J.R.; McLean, S.G.; Zernicke, R.F.; Goulet, G.C. Grading the functional movement screen. J. Strength Cond. Res. 2016, 30, 924–933. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, W.-L.; Lee, M.-H.; Hsu, H.-T.; Ho, W.-H.; Liang, J.-M. Development of an automatic functional movement screening system with inertial measurement unit sensors. Appl. Sci. 2020, 11, 96. [Google Scholar] [CrossRef]


{kind=link}
| Test | Number of Criteria | Total Possible Score 1 | |
|---|---|---|---|
| Right | Left | ||
| SKB | 5 | 5 | 5 |
| Standing hip flexion | 5 | 5 | 5 |
| Hip abduction lateral rotation | 5 | 5 | 5 |
| SKB with trunk rotation | 4 | 4 | 4 |
| Deep squat | 2 | 2 | |
| Total Score | 40 | ||
| HIP AND LOWER LIMB MOVEMENT SCREEN | |||||
|---|---|---|---|---|---|
| Standing Hip Flexion | Hip Abduction with Lateral Rotation | Small Knee Bend | Small Knee Bend with Trunk Rotation | ||
| FUNCTIONAL MOVEMENT SCREEN | In-line lunge | R = −0.19 p = 0.24 | R = 0.01 p = 0.93 | R = −0.28 p = 0.08 | R = −0.15 p = 0.33 |
| Active straight-leg raise | R = −0.13 p = 0.42 | R = −0.02 p = 0.91 | R = −0.08 p = 0.60 | R = −0.25 p = 0.12 | |
| Hurdle step | R = −0.37 p = 0.02* | R = −0.34 p = 0.03* | R = −0.22 p = 0.17 | R = −0.20 p = 0.22 | |
| Shoulder mobility | R = −0.17 p = 0.29 | R = −0.03 p = 0.87 | R = −0.11 p = 0.49 | R = −0.12 p = 0.44 | |
| Trunk rotary stability | R = −0.17 p = 0.30 | R = 0.01 p = 0.96 | R = −0.26 p = 0.10 | R = −0.50 p = 0.001 * | |
| HIP AND LOWER LIMB MOVEMENT SCREEN | ||
|---|---|---|
| Deep Squat | ||
| FUNCTIONAL MOVEMENT SCREEN | Deep squat | R = −0.46 p = 0.003 * |
| Trunk stability push-up | R = 0.15 p = 0.34 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Linek, P.; Muckelt, P.E.; Sikora, D.; Booysen, N.; Stokes, M. Assessing Movement Quality in Youth Footballers: The Relationship between Hip and Lower Limb Movement Screen and Functional Movement Screen. Appl. Sci. 2021, 11, 9298. https://0-doi-org.brum.beds.ac.uk/10.3390/app11199298
Linek P, Muckelt PE, Sikora D, Booysen N, Stokes M. Assessing Movement Quality in Youth Footballers: The Relationship between Hip and Lower Limb Movement Screen and Functional Movement Screen. Applied Sciences. 2021; 11(19):9298. https://0-doi-org.brum.beds.ac.uk/10.3390/app11199298
Chicago/Turabian StyleLinek, Pawel, Paul E. Muckelt, Damian Sikora, Nadine Booysen, and Maria Stokes. 2021. "Assessing Movement Quality in Youth Footballers: The Relationship between Hip and Lower Limb Movement Screen and Functional Movement Screen" Applied Sciences 11, no. 19: 9298. https://0-doi-org.brum.beds.ac.uk/10.3390/app11199298