
Use of Covariance Analysis in Electroencephalogram Reveals Abnormalities in Parkinson’s Disease


Abstract
:1. Introduction
2. Materials
2.1. Electroencephalographic Records
2.2. Electroencephalographic Technique
3. Mathematical Background for Cross Wavelet Analysis
3.1. Wavelet Transform
3.2. Continuous Wavelet Transform
3.3. Wavelet Filtering
3.4. Individual Continuous Wavelet Profiles
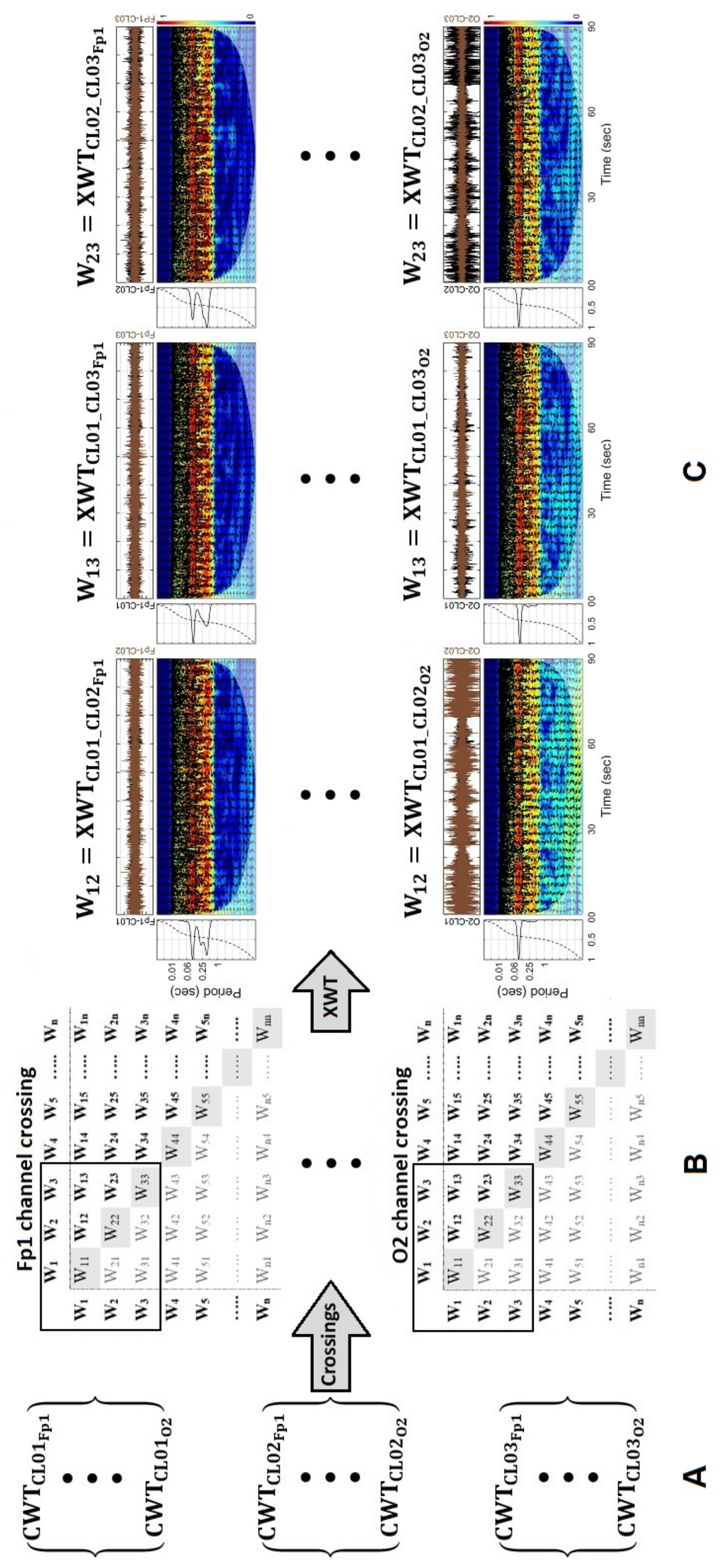
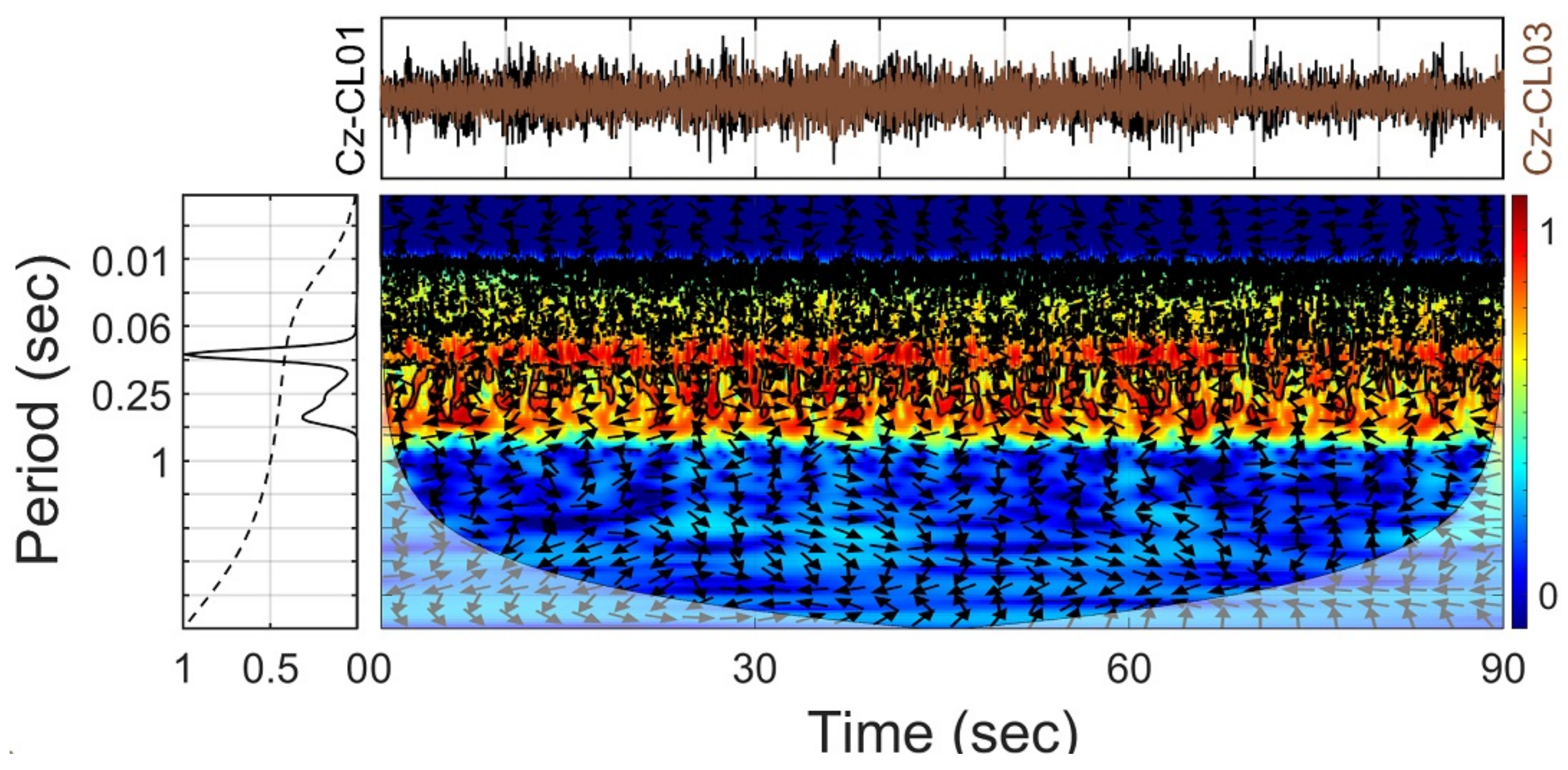
3.5. Cross Wavelet Transform
3.6. Extraction of the Global Wavelet Spectra Information and Cross Wavelets Profiles
4. Results
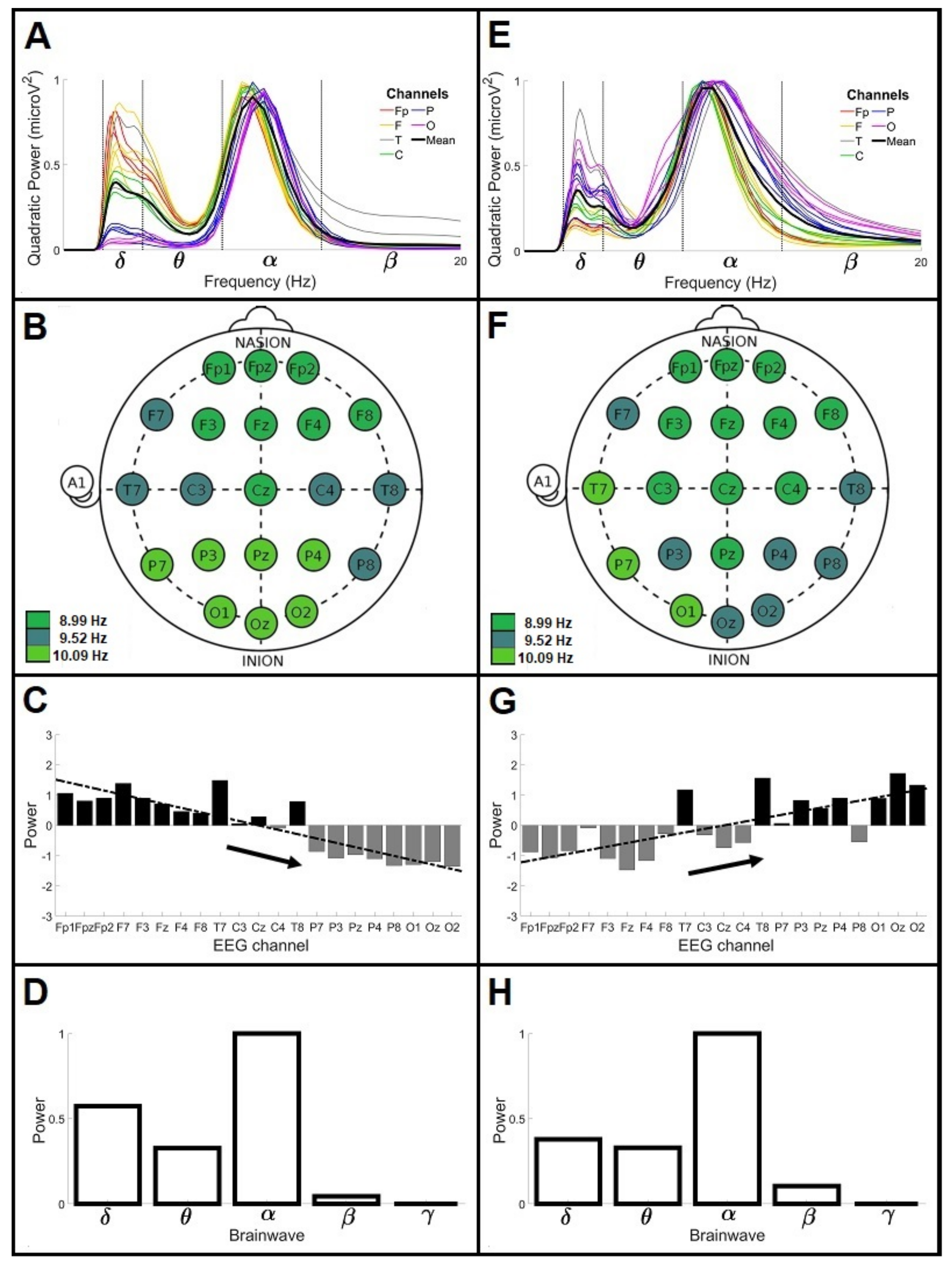
4.1. General Wavelet Profiles of Control and Parkinson’s Disease Patients under 60 Years Old (<60)
4.2. General Wavelet Profiles of Control and Parkinson’s Disease Patients over 60 Years Old (>60)
4.3. Outlier Controls of Average Profile: Are They Potential Subjects of Risk?
5. Discussion
5.1. Global Wavelet Curves Profile of CL and PD Patients under 60 Years of Age (<60)
5.2. Global Wavelet Curves Profile of PD Patients over 60 Years of Age (>60)
5.3. Differential Anteroposterior Power Gradient between CL and PD Patient Groups
5.4. Identification of Outliers
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| PD | Parkinson’s disease |
| EEG | electroencephalographic records |
| MDS-UPDRS | Movement Disorder Society—Unified Parkinson’s Disease Rating Scale |
| H&Y | Hoehn & Yahr Scale |
| BDI-II | Beck Depression Inventory |
| BAI | Beck Anxiety Inventory |
| CASI | Cognitive Abilities Screening Instrument |
| MMSE | Mini Mental State Examination |
| MoCA | Montreal Cognitive Assessment |
| Fp | Frontopolar |
| F | Frontal |
| T | Temporal |
| C | Central |
| P | Parietal |
| O | Occipital |
| CWT | Continuous Wavelet Transform |
| XWT | Cross Wavelet Transform |
| COI | Cone of Influence |
| PWS | Power Wavelet Spectrum |
| GWS | Global Wavelet Spectrum |
References
- Kalia, L.V.; Lang, A.E. Parkinson’s disease. Lancet 2015, 386, 896–912. [Google Scholar] [CrossRef]
- Brooks, D.J.; Pavese, N. Imaging biomarkers in Parkinson’s disease. Prog. Neurobiol. 2011, 95, 614–628. [Google Scholar] [CrossRef] [PubMed]
- Lehéricy, S.; Bardinet, E.; Poupon, C.; Vidailhet, M.; François, C. 7 Tesla magnetic resonance imaging: A closer look at substantia nigra anatomy in Parkinson’s disease. Mov. Disord. 2014, 29, 1574–1581. [Google Scholar] [CrossRef] [PubMed]
- Colombo, D.; Abbruzzese, G.; Antonini, A.; Barone, P.; Bellia, G.; Franconi, F.; Simoni, L.; Attar, M.; Zagni, E.; Haggiag, S.; et al. The “gender factor” in wearing-off among patients with Parkinson’s disease: A post hoc analysis of DEEP study. Sci. World J. 2015, 2015, 787451. [Google Scholar] [CrossRef] [Green Version]
- Gallagher, D.A.; Lees, A.J.; Schrag, A. What are the most important nonmotor symptoms in patients with Parkinson’s disease and are we missing them? Mov. Disord. 2010, 25, 2493–2500. [Google Scholar] [CrossRef] [PubMed]
- Shulman, L.M.; Taback, R.L.; Bean, J.; Weiner, W.J. Comorbidity of the nonmotor symptoms of Parkinson’s disease. Mov. Disord. 2001, 16, 507–510. [Google Scholar] [CrossRef] [PubMed]
- Postuma, R.B.; Aarsland, D.; Barone, P.; Burn, D.J.; Hawkes, C.H.; Oertel, W.; Ziemssen, T. Identifying prodromal Parkinson’s disease: Pre-motor disorders in Parkinson’s disease. Mov. Disord. 2012, 27, 617–626. [Google Scholar] [CrossRef] [PubMed]
- Martinez-Martin, P.; Rodriguez-Blazquez, C.; Abe, K.; Bhattacharyya, K.B.; Bloem, B.R.; Carod-Artal, F.J.; Prakash, R.; Esselink, R.A.; Falup-Pecurariu, C.; Gallardo, M.; et al. International study on the psychometric attributes of the non-motor symptoms scale in Parkinson disease. Neurology 2009, 73, 1584–1591. [Google Scholar] [CrossRef] [PubMed]
- Phillipson, O.T. Management of the aging risk factor for Parkinson’s disease. Neurobiol. Aging 2014, 35, 847–857. [Google Scholar] [CrossRef] [Green Version]
- Reeve, A.; Simcox, E.; Turnbull, D. Ageing and Parkinson’s disease: Why is advancing age the biggest risk factor? Ageing Res. Rev. 2014, 14, 19–30. [Google Scholar] [CrossRef] [PubMed]
- De Lau, L.M.; Breteler, M.M. Epidemiology of Parkinson’s disease. Lancet Neurol. 2006, 5, 525–535. [Google Scholar] [CrossRef]
- Ortiz-Ospina, E.; Beltekian, D. Why do Women Live Longer Than Men? Our World in Data. Available online: https://ourworldindata.org/why-do-women-live-longer-than-men (accessed on 22 June 2021).
- Peelaerts, W.; Bousset, L.; Van der Perren, A.; Moskalyuk, A.; Pulizzi, R.; Giugliano, M.; Van den Haute, C.; Melki, R.; Baekelandt, V. α-Synuclein strains cause distinct synucleinopathies after local and systemic administration. Nature 2015, 522, 340–344. [Google Scholar] [CrossRef] [PubMed]
- Teravskis, P.J.; Covelo, A.; Miller, E.C.; Singh, B.; Martell-Martínez, H.A.; Benneyworth, M.A.; Gallardo, C.; Oxnard, B.R.; Araque, A.; Lee, M.K.; et al. A53T mutant alpha-synuclein induces Tau-dependent postsynaptic impairment independently of neurodegenerative changes. J. Neurosci. 2018, 38, 9754–9767. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- DeLong, M.R.; Wichmann, T. Circuits and circuit disorders of the basal ganglia. Arch. Neurol. 2007, 64, 20–24. [Google Scholar] [CrossRef] [PubMed]
- Mantri, S.; Dukare, V.; Yeole, S.; Patil, D.; Wadhai, V.M. A survey: Fundamental of EEG. Int. J. Adv. Res. Comput. Sci. Manag. Stud. 2013, 1, 83–89. [Google Scholar]
- Cozac, V.V.; Gschwandtner, U.; Hatz, F.; Hardmeier, M.; Rüegg, S.; Fuhr, P. Quantitative EEG and cognitive decline in Parkinson’s disease. Parkinson’s Dis. 2016, 2016, 9060649. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shirahige, L.; Berenguer-Rocha, M.; Mendonça, S.; Rocha, S.; Rodrigues, M.C.; Monte-Silva, K. Quantitative electroencephalography characteristics for Parkinson’s disease: A systematic review. J. Parkinsons Dis. 2020, 10, 455–470. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Han, C.X.; Wang, J.; Yi, G.S.; Che, Y.Q. Investigation of EEG abnormalities in the early stage of Parkinson’s disease. Cogn. Neurodyn. 2013, 7, 351–359. [Google Scholar] [CrossRef] [PubMed]
- Weinberger, M.; Hutchison, W.D.; Lozano, A.M.; Hodaie, M.; Dostrovsky, J.O. Increased gamma oscillatory activity in the subthalamic nucleus during tremor in Parkinson’s disease patients. J. Neurophysiol. 2009, 101, 789–802. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Johnsen, K.; Snædal, J.; Jóhannesson, G.H.; Guðmundsson, Þ.; Blin, N.; Emilsdóttir, Á.; Einarsson, B.; Johannsson, M. O3-13-06: EEG as a biological marker in Parkinson’s disease dementia and dementia of lewy bodies (PDD/DLB). Alzheimer’s Dement. 2014, 10, P236. [Google Scholar] [CrossRef]
- Klassen, B.T.; Hentz, J.G.; Shill, H.A.; Driver-Dunckley, E.; Evidente, V.G.; Sabbagh, M.N.; Adler, C.H.; Caviness, J.N. Quantitative EEG as a predictive biomarker for Parkinson disease dementia. Neurology 2011, 77, 118–124. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hramov, A.E.; Koronovskii, A.A.; Makarov, V.A.; Pavlov, A.N.; Sitnikova, E. Wavelets in Neuroscience; Springer: Berlin/Heidelberg, Germany, 2015. [Google Scholar] [CrossRef]
- Holschneider, M. Wavelets: An Analysis Tool; Oxford University Press: Oxford, UK, 1995; ISBN 0-19-853481-7. [Google Scholar]
- Sheng, Y. Wavelet transform. In The Transforms and Applications Handbook; Poularikas, A.D., Ed.; CRC Press: Boca Raton, FL, USA, 1996; pp. 747–827. ISBN 978-0849383427. [Google Scholar]
- Torrence, C.; Compo, G.P. A practical guide to wavelet analysis. Bull. Am. Meteorol Soc. 1998, 79, 61–78. [Google Scholar] [CrossRef] [Green Version]
- Goetz, C. MDS-UPDRS; Rush University Medical Center: Chicago, IL, USA, 2008. [Google Scholar]
- Hoehn, M.M.; Yahr, M.D. Parkinsonism: Onset, progression, and mortality. Neurology 1967, 17, 427–442. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jurado, S.; Villegas, M.E.; Méndez, L.; Rodríguez, F.; Loperena, V.; Varela, R. La estandarización del inventario de depresión de Beck para los residentes de Ciudad de México. Salud. Ment. 1998, 21, 26–32. [Google Scholar]
- Robles, R.; Varela, R.; Jurado, S.; Páez, F. Versión mexicana del inventario de ansiedad de Beck: Propiedades psicométricas. Rev. Mex. Psicol. 2001, 18, 211–217. [Google Scholar]
- Teng, E.L.; Hasegawa, K.; Homma, A.; Imai, Y.; Larson, E.; Graves, A.; Sugimoto, K.; Yamaguchi, T.; Sasaki, H.; Chiu, D.; et al. The Cognitive Abilities Screening Instrument (CASI): A practical test for cross-cultural epidemiological studies of dementia. Int. Psychogeriatr. 1994, 6, 45–58. [Google Scholar] [CrossRef] [PubMed]
- Ostrosky, F.; López, G.; Ardila, A. Influencias de la edad y de la escolaridad en el examen breve del estado mental (Mini-Mental State Examination) en una población hispano-hablante. Salud. Ment. 1999, 22, 20–26. [Google Scholar]
- Palacios, A. Validez y Confiabilidad del Montreal Cognitive Assesssment (MoCA) en su Versión Traducida al Español para el Cribaje del Deterioro Cognitivo Leve en Adultos Mayores. Ph.D. Dissertation, School of Medicine, UNAM, Mexico City, Mexico, 2015. [Google Scholar]
- Iwaki, H.; Nishikawa, N.; Nagai, M.; Tsujii, T.; Yabe, H.; Kubo, M.; Ieiri, I.; Nomoto, M. Pharmacokinetics of levodopa/benserazide versus levodopa/carbidopa in healthy subjects and patients with Parkinson’s disease. Neurol. Clin. Neurosci. 2015, 3, 68–73. [Google Scholar] [CrossRef] [Green Version]
- Stathis, P.; Konitsiotis, S.; Antonini, A. Dopamine agonists early monotherapy for the delay of development of levodopa-induced dyskinesias. Expert Rev. Neurother. 2015, 15, 207–213. [Google Scholar] [CrossRef] [PubMed]
- Rascol, O.; Fitzer-Attas, C.J.; Hauser, R.; Jankovic, J.; Lang, A.; Langston, J.W.; Melamed, E.; Poewe, W.; Stocchi, F.; Tolosa, E.; et al. A double-blind, delayed-start trial of rasagiline in Parkinson’s disease (the ADAGIO study): Prespecified and post-hoc analyses of the need for additional therapies, changes in UPDRS scores, and non-motor outcomes. Lancet Neurol. 2011, 10, 415–423. [Google Scholar] [CrossRef]
- Crosby, N.J.; Deane, K.H.; Clarke, C.E. Amantadine for dyskinesia in Parkinson’s disease. Cochrane Database Syst. Rev. 2003, 2, CD003467. [Google Scholar] [CrossRef]
- Grinsted, A.; Moore, J.C.; Jevrejeva, S. Application of the cross wavelet transform and wavelet coherence to geophysical time series. Nonlinear Process. Geophys. 2004, 11, 561–566. [Google Scholar] [CrossRef]
- Gilman, D.L.; Fuglister, F.J.; Mitchell, J.M. On the power spectrum of “Red Noise”. J. Atmos. Sci. 1963, 20, 182–184. [Google Scholar] [CrossRef] [Green Version]
- Jevrejeva, S.; Moore, J.C.; Grinsted, A. Influence of the arctic oscillation and El Nino-Southern Oscillation (ENSO) on ice conditions in the Baltic Sea: The wavelet approach. J. Geophys. Res. Space Phys. 2003, 108, 4677. [Google Scholar] [CrossRef] [Green Version]
- Hudgins, L.; Friehe, C.A.; Mayer, M.E. Wavelet transform and atmospheric turbulence. Phys. Rev. Lett. 1993, 71, 3279–3282. [Google Scholar] [CrossRef] [PubMed]
- Soon, W.; Velasco, V.M.; Selvaraj, K.; Traversi, R.; Usoskin, I.; Chen, C.T.A.; Lou, J.Y.; Kao, S.J.; Carter, R.M.; Pipin, V.; et al. A review of Holocene solar-linked climatic variation on centennial to millennial timescales: Physical processes, interpretative frameworks and a new multiple cross-wavelet transform algorithm. Earth Sci. Rev. 2014, 134, 1–15. [Google Scholar] [CrossRef]
- Velasco, V.M.; Soon, W.; Velasco, G.; Traversi, R.; Horiuchi, K. Generalization of the cross-wavelet function. New Astron. 2017, 56, 86–93. [Google Scholar] [CrossRef]
- Jenkins, G.M.; Watts, D.G. Spectral Analysis and Its Applications; Holden-Day: San Francisco, CA, USA, 1968; p. 525. ISBN 0816244642. [Google Scholar]
- Kan, D.P.X.; Croarkin, P.E.; Phang, C.K.; Lee, P.F. EEG differences between eyes-closed and eyes-open conditions at the resting stage for euthymic participants. Neurophysiology 2017, 49, 432–440. [Google Scholar] [CrossRef]
- Hughes, S.W.; Crunelli, V. Thalamic mechanisms of EEG alpha rhythms and their pathological implications. Neuroscientist 2005, 11, 357–372. [Google Scholar] [CrossRef]
- Melgari, J.M.; Curcio, G.; Mastrolilli, F.; Salomone, G.; Trotta, L.; Tombini, M.; di Biase, L.; Scrascia, F.; Fini, R.; Fabrizio, E.; et al. Alpha and beta EEG power reflects L-dopa acute administration in parkinsonian patients. Front. Aging Neurosci. 2014, 6, 302. [Google Scholar] [CrossRef] [PubMed]
- Dimpfel, W.; Oehlwein, C.; Hoffmann, J.A.; Müller, T. Quantitative EEG changes in patients with Parkinson’s disease during therapy with Rasagiline. Adv. Parkinsons Dis. 2014, 3, 22–34. [Google Scholar] [CrossRef] [Green Version]
- Choi, J.W.; Jeong, M.H.; Her, S.J.; Lee, B.U.; Cha, K.S.; Jung, K.Y.; Kim, K.H. Abnormal sleep delta rhythm and interregional phase synchrony in patients with restless legs syndrome and their reversal by dopamine agonist treatment. J. Clin. Neurol. 2017, 13, 340–350. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Steriade, M.; Gloor, P.; Llinás, R.R.; Lopes da Silva, F.H.; Mesulam, M.M. Basic mechanisms of cerebral rhythmic activities. Electroencephalogr. Clin. Neurophysiol. 1990, 76, 481–508. [Google Scholar] [CrossRef]
- Amzica, F.; Massimini, M. Glial and neuronal interactions during slow wave and paroxysmal activities in the neocortex. Cereb. Cortex 2002, 12, 1101–1113. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Duffy, F.H.; Albert, M.S.; McAnulty, G.; Garvey, A.J. Age-related differences in brain electrical activity of healthy subjects. Ann. Neurol. 1984, 16, 430–438. [Google Scholar] [CrossRef]
- Peters, R. Ageing and the brain. Postgrad. Med. J. 2006, 82, 84–88. [Google Scholar] [CrossRef] [PubMed]
- Raz, N.; Rodrigue, K.M.; Acker, J.D. Hypertension and the Brain: Vulnerability of the prefrontal regions and executive functions. Behav. Neurosci. 2003, 117, 1169–1180. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Chan, G.L.Y.; Holden, J.E.; Dobko, T.; Mak, E.; Schulzer, M.; Huser, J.M.; Snow, B.J.; Ruth, T.J.; Calne, D.B.; et al. Age-dependent decline of dopamine D1 receptors in human brain: A PET study. Synapse 1998, 30, 56–61. [Google Scholar] [CrossRef]
- Braak, H.; Braak, E.; Yilmazer, D.; Schultz, C.; de Vos, R.A.; Jansen, E.N. Nigral and extranigral pathology in Parkinson’s disease. J. Neural Transm. Suppl. 1995, 46, 15–31. [Google Scholar]
- Juárez, J.; Corsi, M. Sex differences in interhemispheric correlation and spectral power of EEG activity. Brain Res. Bull. 1995, 38, 149–151. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Group | Main Frequencies (Hz)÷ | Global Wavelet Curves | Power Anomalies (Brain Regions) | Linear Regression (Slope/y-Intercept) | Normalized Brainwave Power | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| α and δ Mean Frequencies (Hz; Mean ± SD) | α and δ Power (microV2) | ||||||||||
| + | − | ~0 | δ | θ | α | β | |||||
| CL <60 | 8.99 9.52 10.09 | 9.52 ± 1.81 2.67 ± 0.55 | 0.89 0.39 | Fp F T | P O | C | −0.14/1.6 | 0.57 | 0.32 | 1 | 0.04 |
| CL >60 | 8.48 8.99 | 8.99 ± 1.36 2.52 ± 0.46 | 0.93 0.33 | Fp T O | F C P | - | −0.03/0.42 | 0.46 | 0.29 | 1 | 0.04 |
| PD-Patients <60 | 8.99 9.52 10.09 | 9.52 ± 1.96 2.67 ± 0.49 | 0.95 0.35 | T P O | Fp F C | - | 0.12/−1.3 | 0.37 | 0.32 | 1 | 0.10 |
| PD-Patients >60 | 2.38 2.52 2.67 8.99 | 8.99 ± 2.41 2.67 ± 0.61 | 0.49 0.90 | T P O | Fp | F C | 0.12/−1.4 | 1 | 0.42 | 0.52 | 0.07 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
González-González, G.; Velasco-Herrera, V.M.; Ortega-Aguilar, A. Use of Covariance Analysis in Electroencephalogram Reveals Abnormalities in Parkinson’s Disease. Appl. Sci. 2021, 11, 9633. https://0-doi-org.brum.beds.ac.uk/10.3390/app11209633
González-González G, Velasco-Herrera VM, Ortega-Aguilar A. Use of Covariance Analysis in Electroencephalogram Reveals Abnormalities in Parkinson’s Disease. Applied Sciences. 2021; 11(20):9633. https://0-doi-org.brum.beds.ac.uk/10.3390/app11209633
Chicago/Turabian StyleGonzález-González, Gabriela, Víctor M. Velasco-Herrera, and Alicia Ortega-Aguilar. 2021. "Use of Covariance Analysis in Electroencephalogram Reveals Abnormalities in Parkinson’s Disease" Applied Sciences 11, no. 20: 9633. https://0-doi-org.brum.beds.ac.uk/10.3390/app11209633