
Biochemical Mapping of the Inflamed Human Dental Pulp

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients and Sample Collection
2.2. Pulp Lysates
2.3. Enzyme-Linked Immunosorbent Assay (ELISA)
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Available online: https://www.who.int/news-room/fact-sheets/detail/oral-health (accessed on 23 September 2021).
- Zero, D.T.; Zandona, A.F.; Vail, M.M.; Spolnik, K.J. Dental caries and pulpal disease. Dent. Clin. N. Am. 2011, 55, 29–46. [Google Scholar] [CrossRef]
- Hahn, C.L.; Liewehr, F.R. Relationships between caries bacteria, host responses, and clinical signs and symptoms of pulpitis. J. Endod. 2007, 33, 213–219. [Google Scholar] [CrossRef]
- Zanini, M.; Meyer, E.; Simon, S. Pulp Inflammation Diagnosis from Clinical to Inflammatory Mediators: A Systematic Review. J. Endod. 2017, 43, 1033–1051. [Google Scholar] [CrossRef]
- Conrads, G.; About, I. Pathophysiology of Dental Caries. Monogr. Oral Sci. 2018, 27, 1–10. [Google Scholar] [CrossRef]
- Hahn, C.L.; Liewehr, F.R. Innate immune responses of the dental pulp to caries. J. Endod. 2007, 33, 643–651. [Google Scholar] [CrossRef]
- Kritikou, K.; Greabu, M.; Imre, M.; Miricescu, D.; Ripszky Totan, A.; Burcea, M.; Stanescu, S., II; Spinu, T. ILs and MMPs Levels in Inflamed Human Dental Pulp: A Systematic Review. Molecules 2021, 26, 4129. [Google Scholar] [CrossRef]
- Okamoto, T.; Takahashi, S.; Nakamura, E.; Nagaya, K.; Hayashi, T.; Shirai, M.; Fujieda, K. Increased expression of matrix metalloproteinase-9 and hepatocyte growth factor in the cerebrospinal fluid of infants with posthemorrhagic hydrocephalus. Early Hum. Dev. 2010, 86, 251–254. [Google Scholar] [CrossRef]
- Grossi, G.B.; Borrello, S.; Giuliani, M.; Galeotti, T.; Miani, C. Copper-zinc superoxide dismutase in human and animal dental pulp. J. Dent. 1991, 19, 319–321. [Google Scholar] [CrossRef]
- Farges, J.C.; Alliot-Licht, B.; Renard, E.; Ducret, M.; Gaudin, A.; Smith, A.J.; Cooper, P.R. Dental Pulp Defence and Repair Mechanisms in Dental Caries. Mediat. Inflamm. 2015, 2015, 230251. [Google Scholar] [CrossRef] [Green Version]
- Leone, A.; Angelova Volponi, A.; Uzzo, M.L.; Spatola, G.F.; Jurjus, A.; Vandevska-Radunovic, V. Dental pulp in mature replanted human teeth: Morphological alterations and metalloproteineses-2 and -9, Annexin-5, BCL-2 and iNOS modulation. J. Biol. Regul. Homeost. Agents 2015, 29, 961–967. [Google Scholar]
- Yamasaki, M.; Morimoto, T.; Tsuji, M.; Akihiro, I.; Maekawa, Y.; Nakamura, H. Role of IL-2 and helper T-lymphocytes in limiting periapical pathosis. J. Endod. 2006, 32, 24–29. [Google Scholar] [CrossRef]
- Gaffen, S.L.; Liu, K.D. Overview of interleukin-2 function, production and clinical applications. Cytokine 2004, 28, 109–123. [Google Scholar] [CrossRef]
- Rauschenberger, C.R.; Bailey, J.C.; Cootauco, C.J. Detection of human IL-2 in normal and inflamed dental pulps. J. Endod. 1997, 23, 366–370. [Google Scholar] [CrossRef]
- Anderson, L.M.; Dumsha, T.C.; McDonald, N.J.; Spitznagel, J.K., Jr. Evaluating IL-2 levels in human pulp tissue. J. Endod. 2002, 28, 651–655. [Google Scholar] [CrossRef]
- Elsalhy, M.; Azizieh, F.; Raghupathy, R. Cytokines as diagnostic markers of pulpal inflammation. Int. Endod. J. 2013, 46, 573–580. [Google Scholar] [CrossRef]
- Wei, L.; Liu, M.; Xiong, H.; Peng, B. Up-regulation of IL-23 expression in human dental pulp fibroblasts by IL-17 via activation of the NF-kappaB and MAPK pathways. Int. Endod. J. 2018, 51, 622–631. [Google Scholar] [CrossRef]
- Cardoso, C.R.; Garlet, G.P.; Crippa, G.E.; Rosa, A.L.; Junior, W.M.; Rossi, M.A.; Silva, J.S. Evidence of the presence of T helper type 17 cells in chronic lesions of human periodontal disease. Oral Microbiol. Immunol. 2009, 24, 1–6. [Google Scholar] [CrossRef]
- Yu, J.J.; Gaffen, S.L. Interleukin-17: A novel inflammatory cytokine that bridges innate and adaptive immunity. Front. Biosci. 2008, 13, 170–177. [Google Scholar] [CrossRef]
- Johnson, R.B.; Wood, N.; Serio, F.G. Interleukin-11 and IL-17 and the pathogenesis of periodontal disease. J. Periodontol. 2004, 75, 37–43. [Google Scholar] [CrossRef]
- Colic, M.; Vasilijic, S.; Gazivoda, D.; Vucevic, D.; Marjanovic, M.; Lukic, A. Interleukin-17 plays a role in exacerbation of inflammation within chronic periapical lesions. Eur. J. Oral Sci. 2007, 115, 315–320. [Google Scholar] [CrossRef]
- Xiong, H.; Wei, L.; Peng, B. Immunohistochemical localization of IL-17 in induced rat periapical lesions. J. Endod. 2009, 35, 216–220. [Google Scholar] [CrossRef]
- Marcal, J.R.; Samuel, R.O.; Fernandes, D.; de Araujo, M.S.; Napimoga, M.H.; Pereira, S.A.; Clemente-Napimoga, J.T.; Alves, P.M.; Mattar, R.; Rodrigues, V., Jr.; et al. T-helper cell type 17/regulatory T-cell immunoregulatory balance in human radicular cysts and periapical granulomas. J. Endod. 2010, 36, 995–999. [Google Scholar] [CrossRef]
- Xiong, H.; Wei, L.; Peng, B. IL-17 stimulates the production of the inflammatory chemokines IL-6 and IL-8 in human dental pulp fibroblasts. Int. Endod. J. 2015, 48, 505–511. [Google Scholar] [CrossRef]
- Liu, M.; Zhao, Y.; Wang, C.; Luo, H.; Peng, A.; Ye, L. Interleukin-17 plays a role in pulp inflammation partly by WNT5A protein induction. Arch. Oral Biol. 2019, 103, 33–39. [Google Scholar] [CrossRef]
- Kokkas, A.B.; Goulas, A.; Varsamidis, K.; Mirtsou, V.; Tziafas, D. Irreversible but not reversible pulpitis is associated with up-regulation of tumour necrosis factor-alpha gene expression in human pulp. Int. Endod. J. 2007, 40, 198–203. [Google Scholar] [CrossRef] [PubMed]
- O’Boskey, F.J., Jr.; Panagakos, F.S. Cytokines stimulate matrix metalloproteinase production by human pulp cells during long-term culture. J. Endod. 1998, 24, 7–10. [Google Scholar] [CrossRef]
- Pezelj-Ribaric, S.; Anic, I.; Brekalo, I.; Miletic, I.; Hasan, M.; Simunovic-Soskic, M. Detection of tumor necrosis factor alpha in normal and inflamed human dental pulps. Arch. Med. Res. 2002, 33, 482–484. [Google Scholar] [CrossRef]
- Abd-Elmeguid, A.; Abdeldayem, M.; Kline, L.W.; Moqbel, R.; Vliagoftis, H.; Yu, D.C. Osteocalcin expression in pulp inflammation. J. Endod. 2013, 39, 865–872. [Google Scholar] [CrossRef] [PubMed]
- Bodor, C.; Matolcsy, A.; Bernath, M. Elevated expression of Cu, Zn-SOD and Mn-SOD mRNA in inflamed dental pulp tissue. Int. Endod. J. 2007, 40, 128–132. [Google Scholar] [CrossRef] [PubMed]
- Davis, W.L.; Jacoby, B.H.; Craig, K.R.; Wagner, G.; Harrison, J.W. Copper-zinc superoxide dismutase activity in normal and inflamed human dental pulp tissue. J. Endod. 1991, 17, 316–318. [Google Scholar] [CrossRef]
- Tulunoglu, O.; Alacam, A.; Bastug, M.; Yavuzer, S. Superoxide dismutase activity in healthy and inflamed pulp tissues of permanent teeth in children. J. Clin. Pediatric Dent. 1998, 22, 341–345. [Google Scholar]
- Baumgardner, K.R.; Sulfaro, M.A. The anti-inflammatory effects of human recombinant copper-zinc superoxide dismutase on pulp inflammation. J. Endod. 2001, 27, 190–195. [Google Scholar] [CrossRef]
- Varvara, G.; Traini, T.; Esposito, P.; Caputi, S.; Perinetti, G. Copper-zinc superoxide dismutase activity in healthy and inflamed human dental pulp. Int. Endod. J. 2005, 38, 195–199. [Google Scholar] [CrossRef]
- Cantatore, F.P.; Crivellato, E.; Nico, B.; Ribatti, D. Osteocalcin is angiogenic in vivo. Cell Biol. Int. 2005, 29, 583–585. [Google Scholar] [CrossRef]
- Wei, X.; Ling, J.; Wu, L.; Liu, L.; Xiao, Y. Expression of mineralization markers in dental pulp cells. J. Endod. 2007, 33, 703–708. [Google Scholar] [CrossRef]
- Hirata, M.; Yamaza, T.; Mei, Y.F.; Akamine, A. Expression of osteocalcin and Jun D in the early period during reactionary dentin formation after tooth preparation in rat molars. Cell Tissue Res. 2005, 319, 455–465. [Google Scholar] [CrossRef]
- Tziafas, D.; Papadimitriou, S. Role of exogenous TGF-beta in induction of reparative dentinogenesis in vivo. Eur. J. Oral Sci. 1998, 106 (Suppl. 1), 192–196. [Google Scholar] [CrossRef]
- Sporn, M.B.; Roberts, A.B. A major advance in the use of growth factors to enhance wound healing. J Clin. Investig. 1993, 92, 2565–2566. [Google Scholar] [CrossRef] [Green Version]
- Pierce, G.F.; Tarpley, J.E.; Yanagihara, D.; Mustoe, T.A.; Fox, G.M.; Thomason, A. Platelet-derived growth factor (BB homodimer), transforming growth factor-beta 1, and basic fibroblast growth factor in dermal wound healing. Neovessel and matrix formation and cessation of repair. Am. J. Pathol. 1992, 140, 1375–1388. [Google Scholar]
- Sloan, A.J.; Perry, H.; Matthews, J.B.; Smith, A.J. Transforming growth factor-beta isoform expression in mature human healthy and carious molar teeth. Histochem. J. 2000, 32, 247–252. [Google Scholar] [CrossRef]
- Piattelli, A.; Rubini, C.; Fioroni, M.; Tripodi, D.; Strocchi, R. Transforming growth factor-beta 1 (TGF-beta 1) expression in normal healthy pulps and in those with irreversible pulpitis. Int. Endod. J. 2004, 37, 114–119. [Google Scholar] [CrossRef]
- Durand, S.H.; Flacher, V.; Romeas, A.; Carrouel, F.; Colomb, E.; Vincent, C.; Magloire, H.; Couble, M.L.; Bleicher, F.; Staquet, M.J.; et al. Lipoteichoic acid increases TLR and functional chemokine expression while reducing dentin formation in in vitro differentiated human odontoblasts. J. Immunol. 2006, 176, 2880–2887. [Google Scholar] [CrossRef]
- Sloan, A.J.; Matthews, J.B.; Smith, A.J. TGF-beta receptor expression in human odontoblasts and pulpal cells. Histochem. J. 1999, 31, 565–569. [Google Scholar] [CrossRef]
- Goldberg, M.; Smith, A.J. Cells and Extracellular Matrices of Dentin and Pulp: A Biological Basis for Repair and Tissue Engineering. Crit. Rev. Oral Biol. Med. 2004, 15, 13–27. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Melin, M.; Joffre-Romeas, A.; Farges, J.C.; Couble, M.L.; Magloire, H.; Bleicher, F. Effects of TGFbeta1 on dental pulp cells in cultured human tooth slices. J. Dent. Res. 2000, 79, 1689–1696. [Google Scholar] [CrossRef]
- Forman, H.J.; Torres, M. Redox signaling in macrophages. Mol. Asp. Med. 2001, 22, 189–216. [Google Scholar] [CrossRef]
- Esposito, P.; Varvara, G.; Caputi, S.; Perinetti, G. Catalase activity in human healthy and inflamed dental pulps. Int. Endod. J. 2003, 36, 599–603. [Google Scholar] [CrossRef]
- He, J.; Qin, M.; Chen, Y.; Hu, Z.; Xie, F.; Ye, L.; Hui, T. Epigenetic regulation of matrix metalloproteinases in inflammatory diseases: A narrative review. Cell Biosci. 2020, 10, 86. [Google Scholar] [CrossRef]
- Letra, A.; Ghaneh, G.; Zhao, M.; Ray, H., Jr.; Francisconi, C.F.; Garlet, G.P.; Silva, R.M. MMP-7 and TIMP-1, new targets in predicting poor wound healing in apical periodontitis. J. Endod. 2013, 39, 1141–1146. [Google Scholar] [CrossRef]
- Gusman, H.; Santana, R.B.; Zehnder, M. Matrix metalloproteinase levels and gelatinolytic activity in clinically healthy and inflamed human dental pulps. Eur. J. Oral Sci. 2002, 110, 353–357. [Google Scholar] [CrossRef]
- Tsai, C.H.; Chen, Y.J.; Huang, F.M.; Su, Y.F.; Chang, Y.C. The upregulation of matrix metalloproteinase-9 in inflamed human dental pulps. J. Endod. 2005, 31, 860–862. [Google Scholar] [CrossRef] [PubMed]
- Suwanchai, A.; Theerapiboon, U.; Chattipakorn, N.; Chattipakorn, S.C. NaV 1.8, but not NaV 1.9, is upregulated in the inflamed dental pulp tissue of human primary teeth. Int. Endod. J. 2012, 45, 372–378. [Google Scholar] [CrossRef] [PubMed]
- Accorsi-Mendonca, T.; Silva, E.J.; Marcaccini, A.M.; Gerlach, R.F.; Duarte, K.M.; Pardo, A.P.; Line, S.R.; Zaia, A.A. Evaluation of gelatinases, tissue inhibitor of matrix metalloproteinase-2, and myeloperoxidase protein in healthy and inflamed human dental pulp tissue. J. Endod. 2013, 39, 879–882. [Google Scholar] [CrossRef] [PubMed]
- Seltzer, S.; Bender, I.B.; Ziontz, M. The Dynamics of Pulp Inflammation: Correlations between Diagnostic Data and Actual Histologic Findings in the Pulp. Oral Surg. Oral Med. Oral Pathol. 1963, 16, 969–977. [Google Scholar] [CrossRef]
- American Association of Endodontists. Glossary of Endodontic Terms; 180 N. Stetson Ave. Suite 1500; AAE: Chicago, IL, USA, 2020. [Google Scholar]
- Murray, P.E.; Smith, A.J. Saving pulps—a biological basis. An overview. Prim. Dent. Care 2002, 9, 21–26. [Google Scholar] [CrossRef] [Green Version]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Biomarker | Healthy Dental Pulp Samples (n = 19), Mean ± Standard | Irreversibly Inflamed Dental Pulp Samples (n = 23), Mean ± Standard | p Value |
|---|---|---|---|
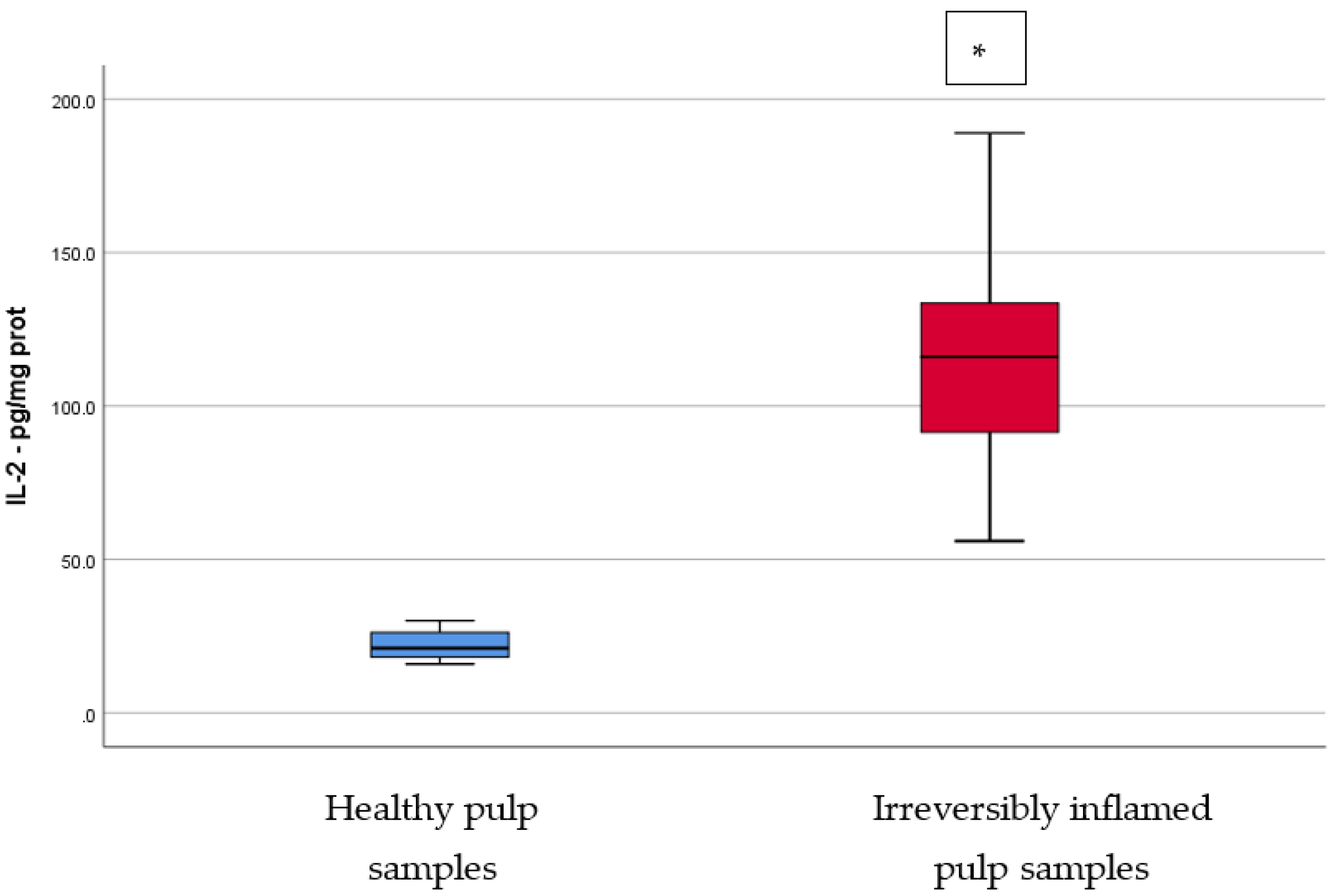
| IL-2 (pg/mg protein) | 22.23 ± 4.66 | 113.21 ± 29.14 | <0.001 |
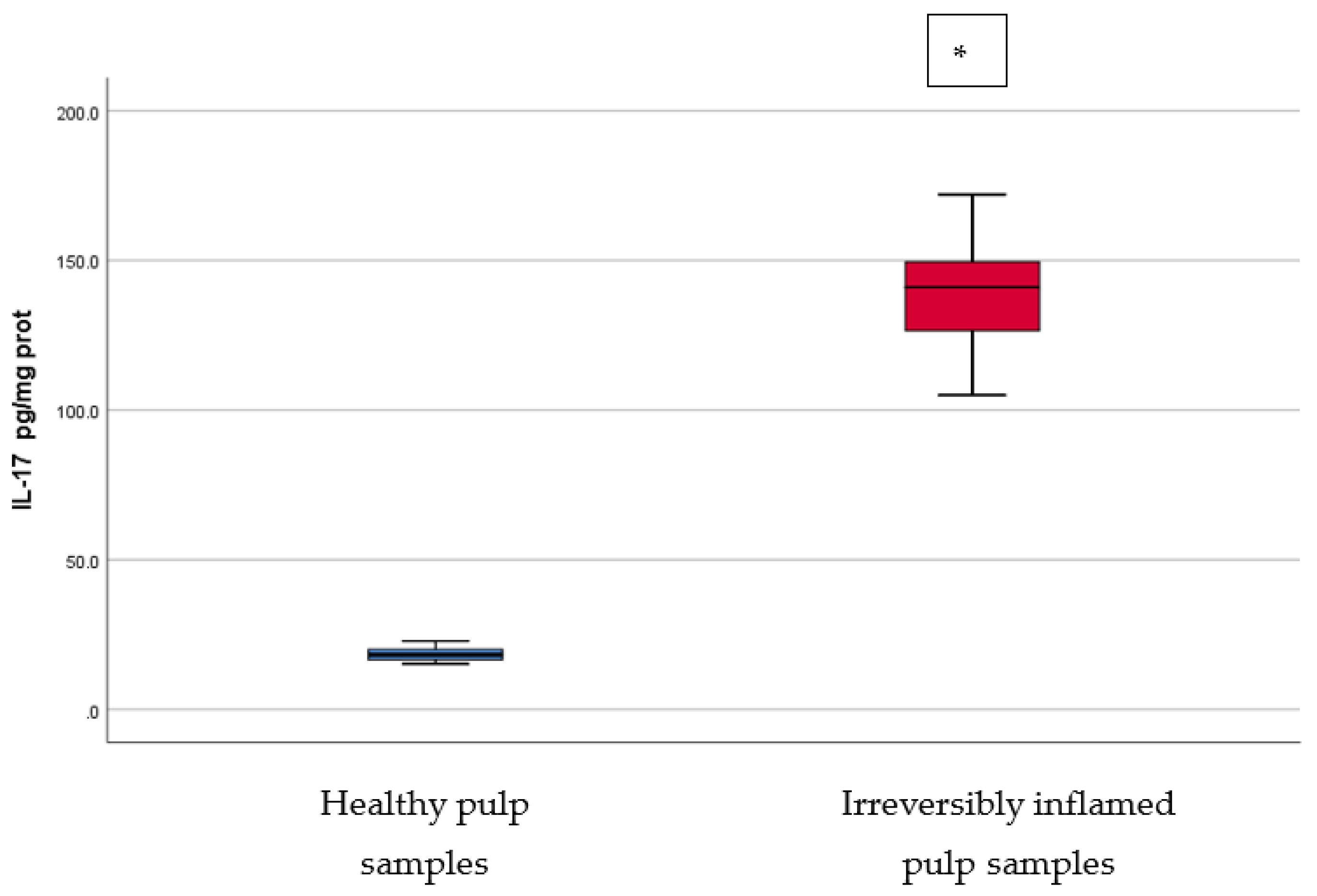
| IL-17 (pg/mg protein) | 18.2 ± 2.04 | 138.04 ± 16.54 | <0.001 |
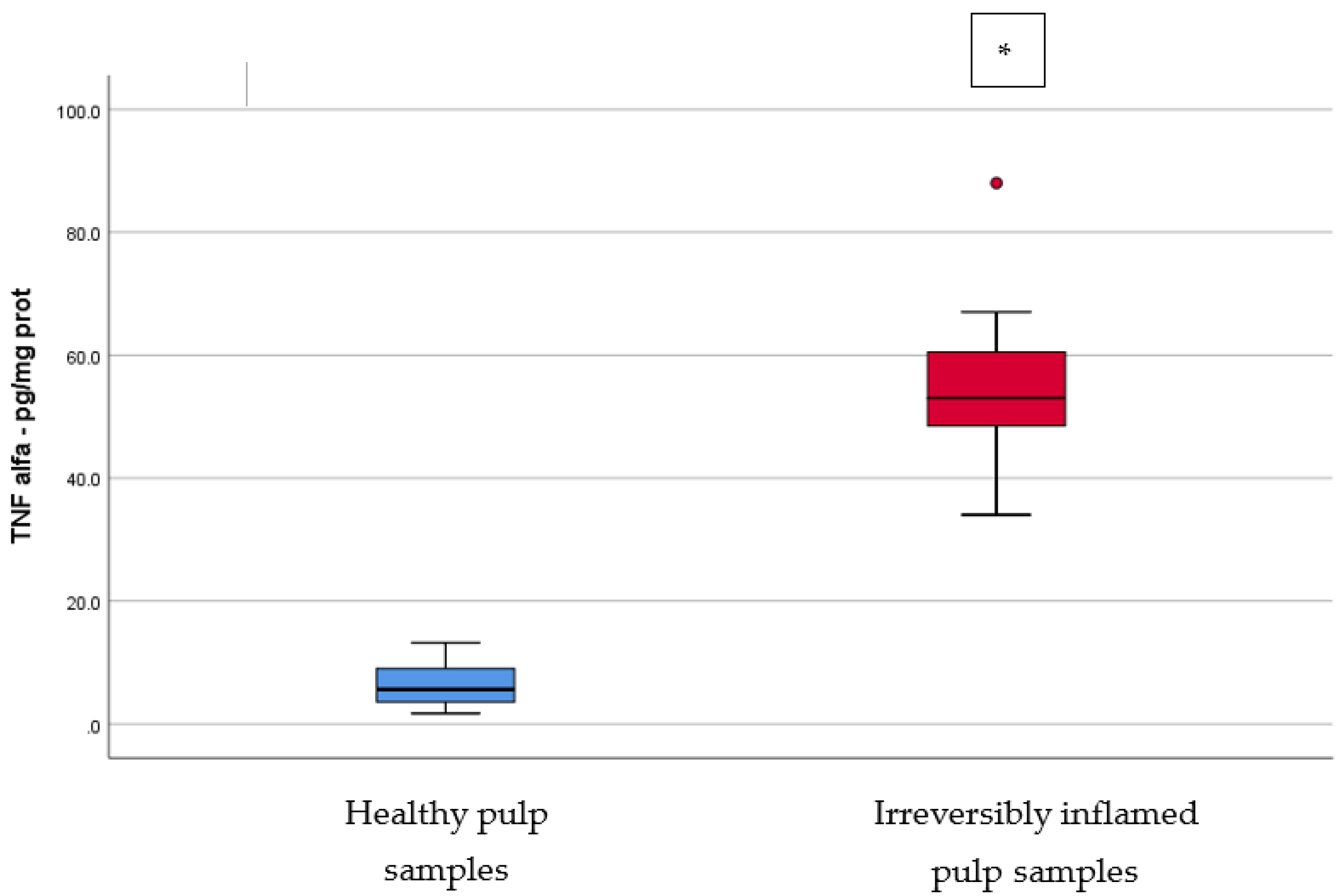
| TNF-α (pg/mg protein) | 6.342 ± 3.429 | 54.435 ± 11.195 | <0.001 |
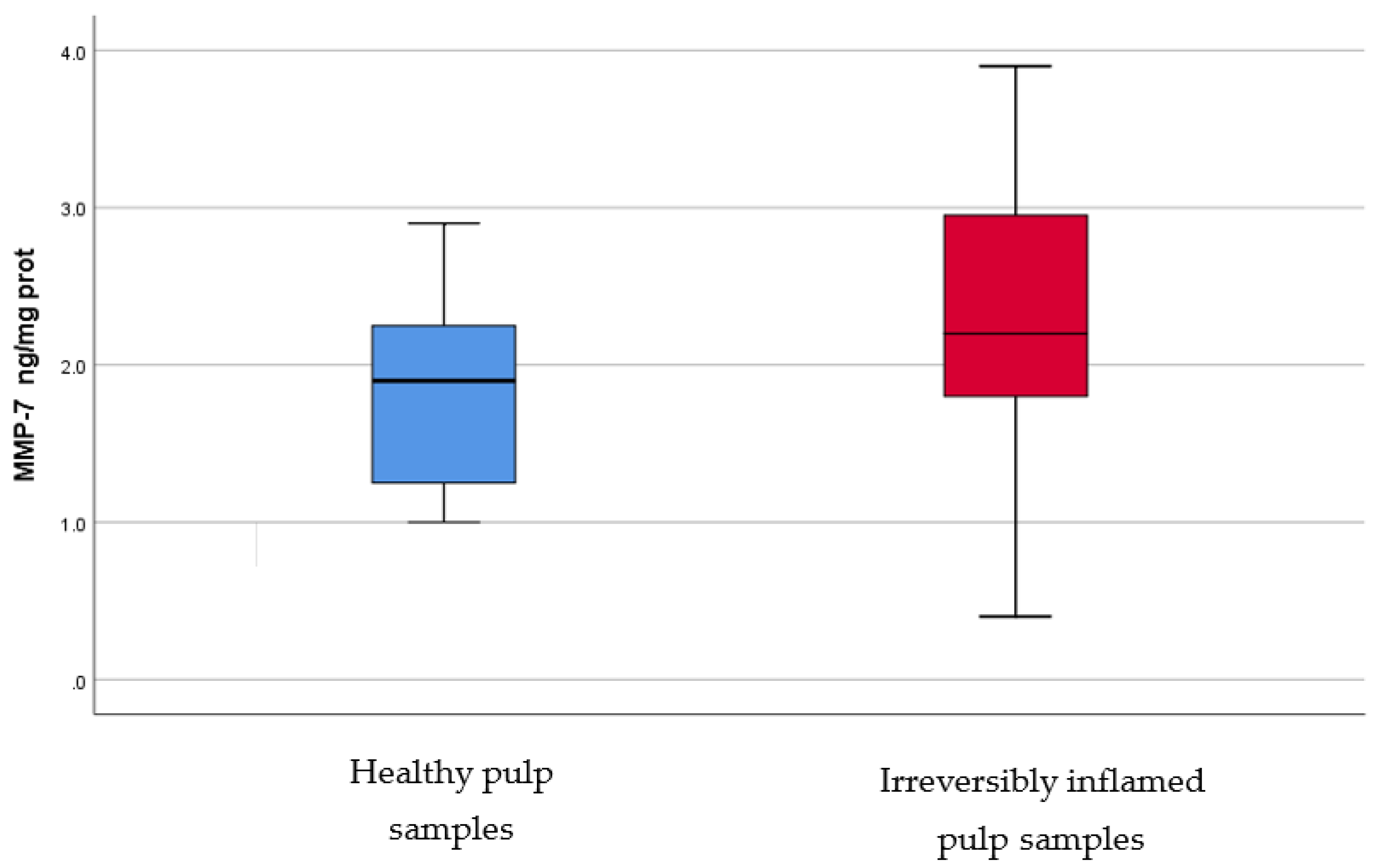
| MMP-7 (ng/mg protein) | 1.853 ± 0.59 | 2.3 ± 0.85 | 0.061 |
| MMP-9 (ng/mg protein) | 1.568 ± 0.44 | 1.496 ± 0.5 | 0.625 |
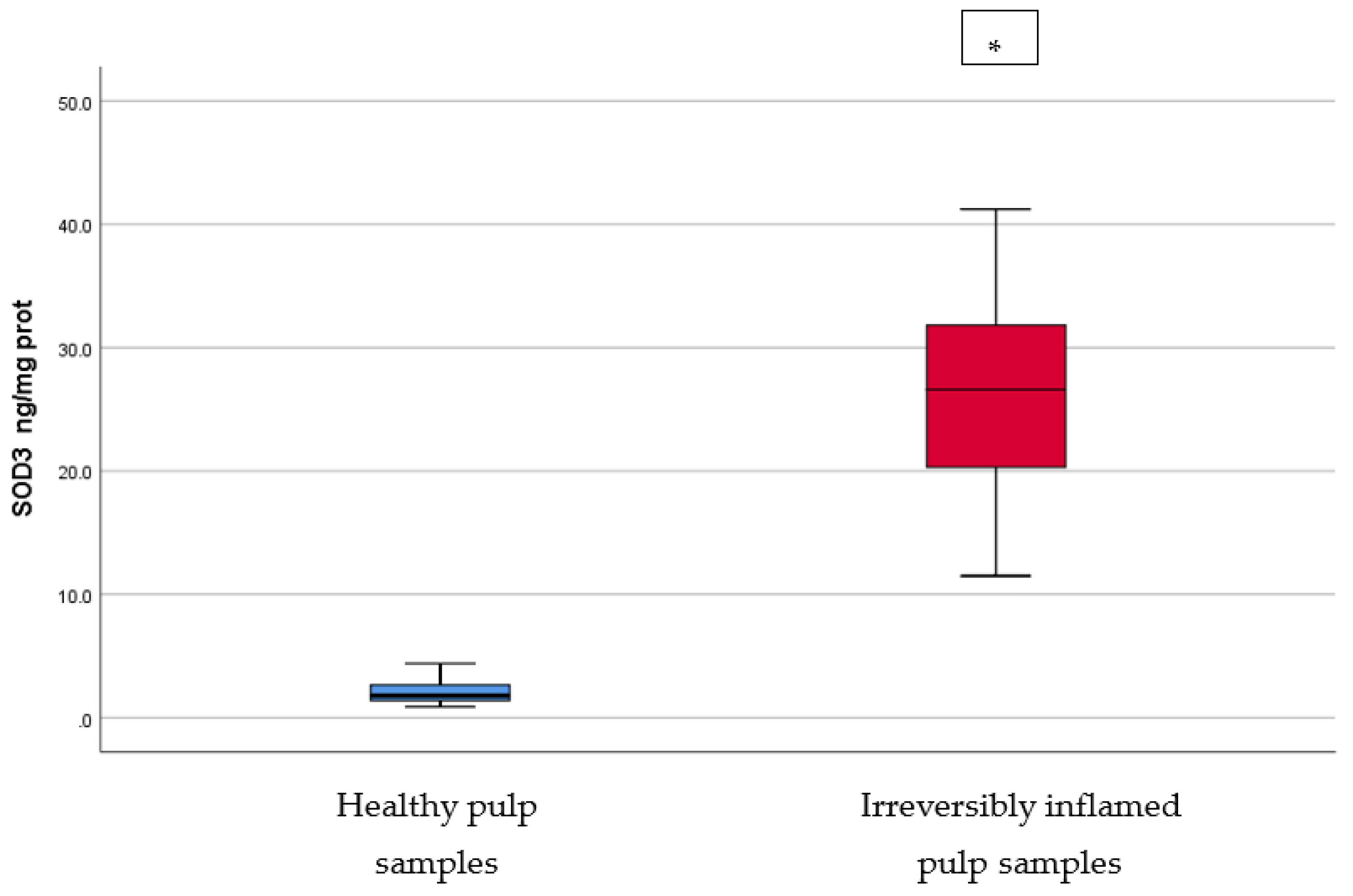
| SOD3 (ng/mg protein) | 2.142 ± 0.97 | 26.32 ± 7.71 | <0.001 |
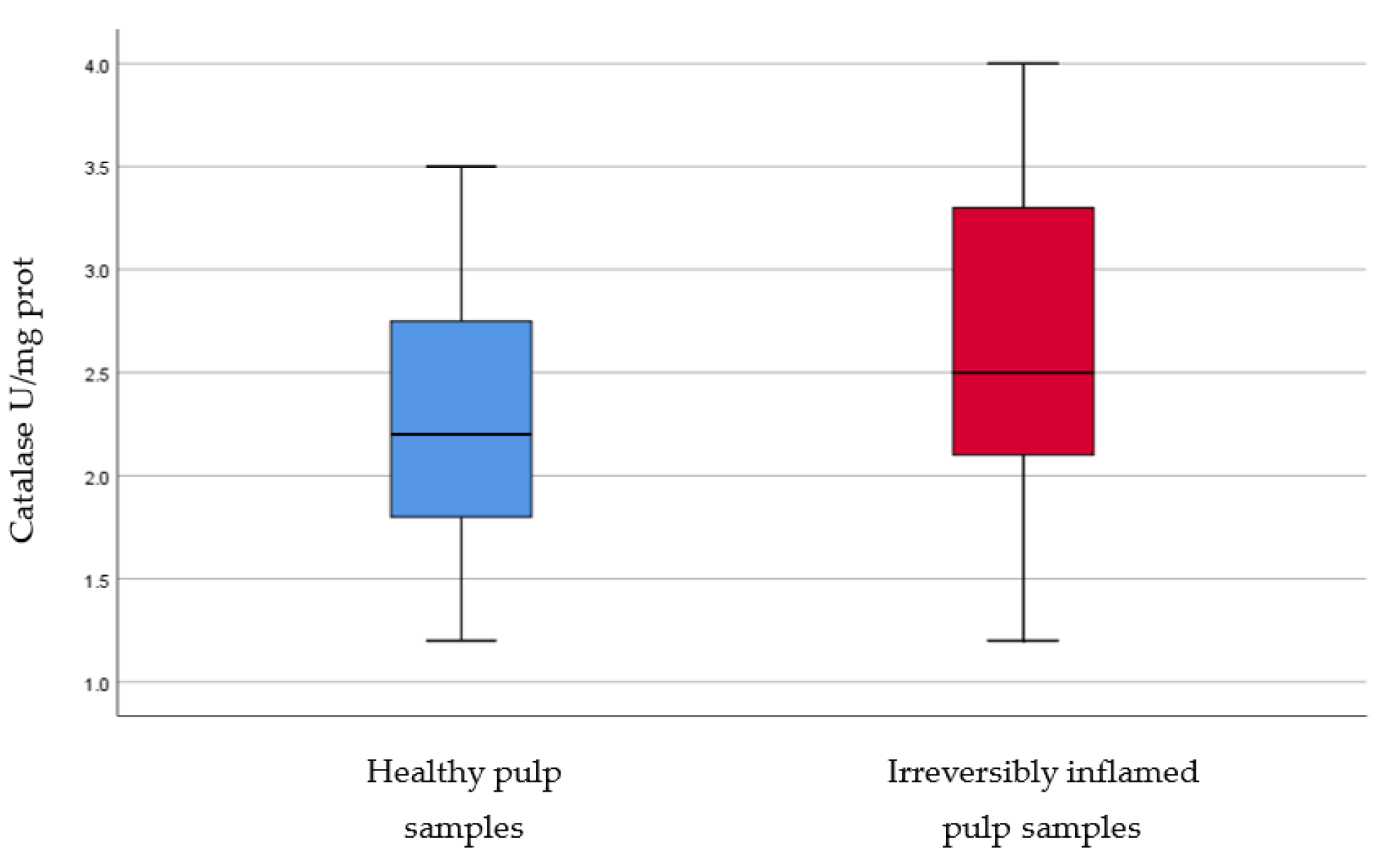
| Catalase (U/mg protein) | 2.258 ± 0.66 | 2.67 ± 0.74 | 0.064 |
| Osteocalcin (ng/mg protein) | 2.816 ± 1 | 7.97 ± 4 | <0.001 |
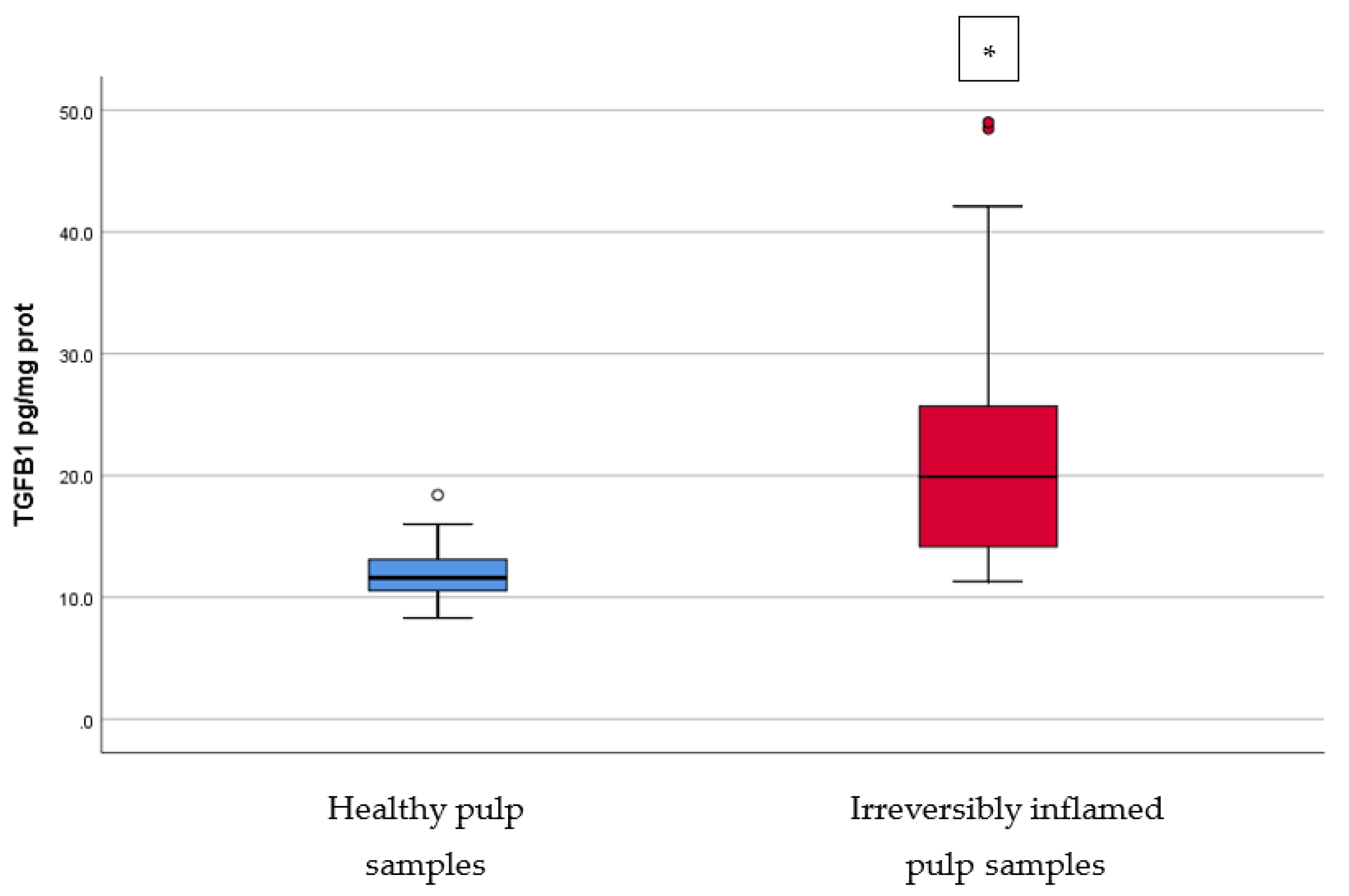
| TGF-β1 (pg/mg protein) | 12.12 ± 2.54 | 23.16 ± 11.79 | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kritikou, K.; Imre, M.; Tanase, M.; Vinereanu, A.; Totan, A.R.; Spinu, T.-C.; Ilinca, R.; Miricescu, D.; Stanescu-Spinu, I.-I.; Greabu, M. Biochemical Mapping of the Inflamed Human Dental Pulp. Appl. Sci. 2021, 11, 10395. https://0-doi-org.brum.beds.ac.uk/10.3390/app112110395
Kritikou K, Imre M, Tanase M, Vinereanu A, Totan AR, Spinu T-C, Ilinca R, Miricescu D, Stanescu-Spinu I-I, Greabu M. Biochemical Mapping of the Inflamed Human Dental Pulp. Applied Sciences. 2021; 11(21):10395. https://0-doi-org.brum.beds.ac.uk/10.3390/app112110395
Chicago/Turabian StyleKritikou, Konstantina, Marina Imre, Mihaela Tanase, Arina Vinereanu, Alexandra Ripszky Totan, Tudor-Claudiu Spinu, Radu Ilinca, Daniela Miricescu, Iulia-Ioana Stanescu-Spinu, and Maria Greabu. 2021. "Biochemical Mapping of the Inflamed Human Dental Pulp" Applied Sciences 11, no. 21: 10395. https://0-doi-org.brum.beds.ac.uk/10.3390/app112110395