
Subclinical Atherosclerosis Progression in Obese Children with Relevant Cardiometabolic Risk Factors Can Be Assessed through Carotid Intima Media Thickness

 ,
,  and
and 
Abstract
:Featured Application
Abstract
1. Introduction
2. Materials and Methods
2.1. Inclusion Criteria
- Obese group—patients with a BMI score ≥ 95th percentile for age and sex, overweight group—BMI ranging from the 85th percentile to 95th percentile, and the control group—BMI ranging from the 5th percentile to the 85th.
- Both sexes were included, and ages ranged from 6 to 17.
2.2. Exclusion Criteria
- Secondary obesity causes: Cushing syndrome, thyroid disfunctions with hypothyroidism, insulin-dependent diabetes mellitus, polycystic ovarian syndrome, hypothalamic injury/disorders, genetic syndromes like Prader–Willi syndrome [32], grelin–leptin dysfunction [33], and use of medication that can induce weight gain (glucocorticosteroids, sulphonylureas, tricyclic antidepressants, antipsychotics) [34].
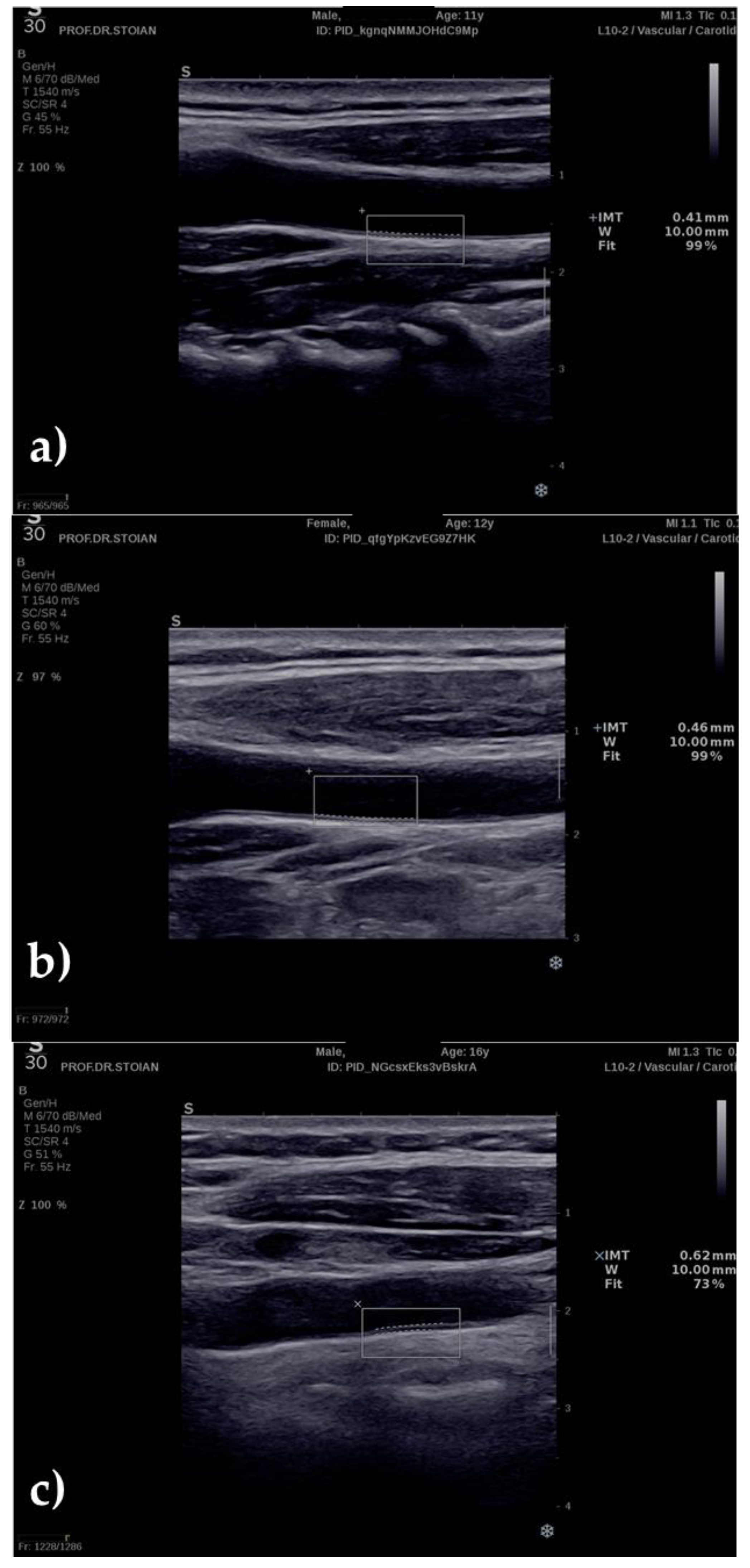
2.3. Ultrasonography Technique
2.4. Statistical Analysis
3. Results
3.1. CIMT with Regard to Age
3.2. CIMT with Regard to Gender
3.3. Assessment of Risk Factors
3.3.1. Obese Patients
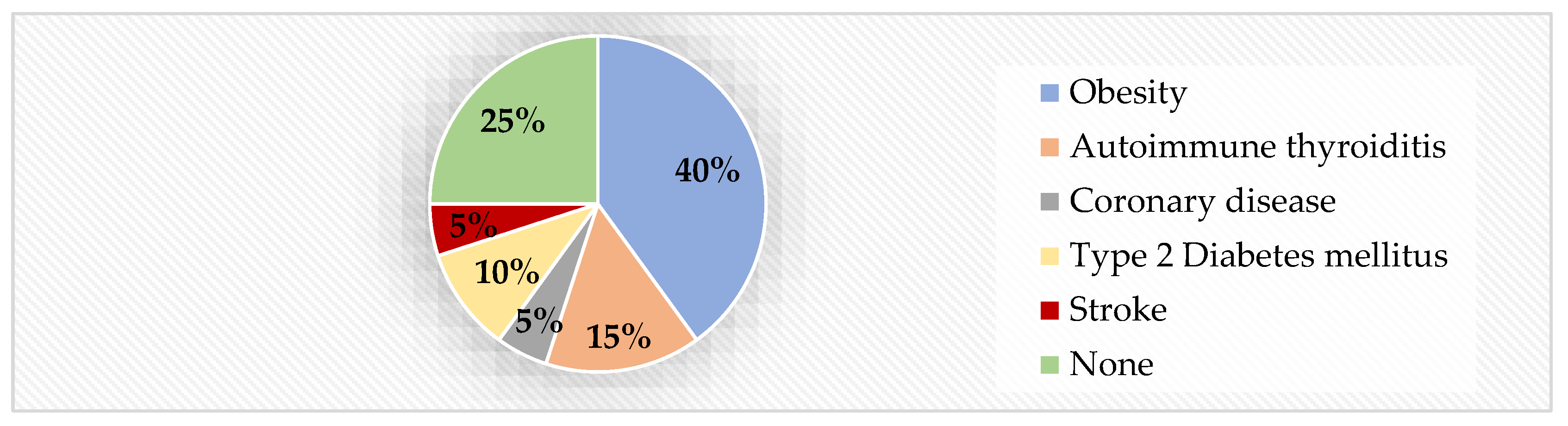
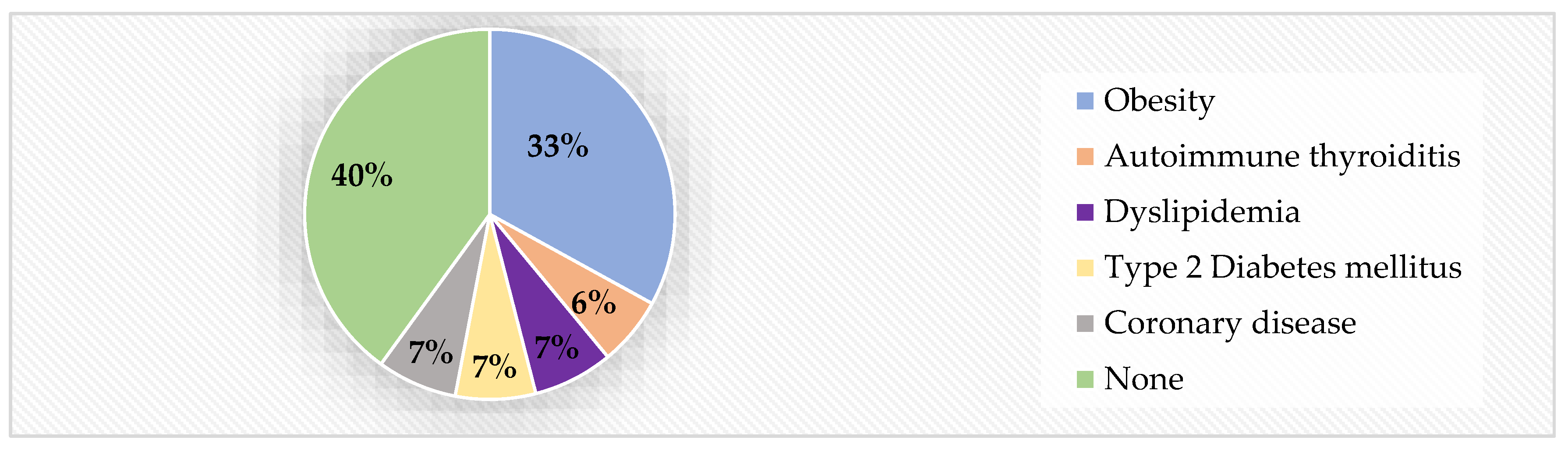
- Family history. Family history was an important context for the obese group: 75% of obese children had at least one significant cardiometabolic risk factor within their close family history (Figure 3). Obesity was present in 40% of the cases, followed by autoimmune thyroiditis and type 2 diabetes. CIMT reached statistically significant higher values in children with positive family history than in those without (p = 0.049).
- High blood pressure. High blood pressure was detected in 20% of the obese patients. Although CIMT scored higher values in this group than in the one with healthy blood pressure levels, the difference was not statistically significant (p = 0.102).
- Smoking. Smoking proved to be a significant risk factor. Only 15% of the adolescents pertaining to the obese group declared that they were smokers. Their CIMT mean was highest than any of the analyzed subgroups and the differences were statistically significant (p = 0.015). Moreover, smoking was strongly and positively correlated with higher values of CIMT (r = 0.53).
- Lifestyle. In the obese group, 65% of children declared a sedentary lifestyle (practicing no sport and having less than an hour/day of physical activity). CIMT values were higher than in children with healthy physical activity, but the differences were not statistically significant.
3.3.2. Overweight Patients
- Postnatal nutrition. In the overweight group, the nutrition factor was divided almost equally between children, with 47% having received formula as nurslings. However, the mean CIMT was significantly higher in children fed with formula ( = 0.5 mm) than in breastfed children ( = 0.44 mm), p = 0.023.
- Birth weight. Exactly one third of the overweight patients were born with a birth weight higher than 3500 g and scored higher CIMT values ( = 0.5 mm) than the low BW and normal BW groups ( = 0.45 mm and = 0.46 mm, respectively). No statistical differences were detected between subgroups.
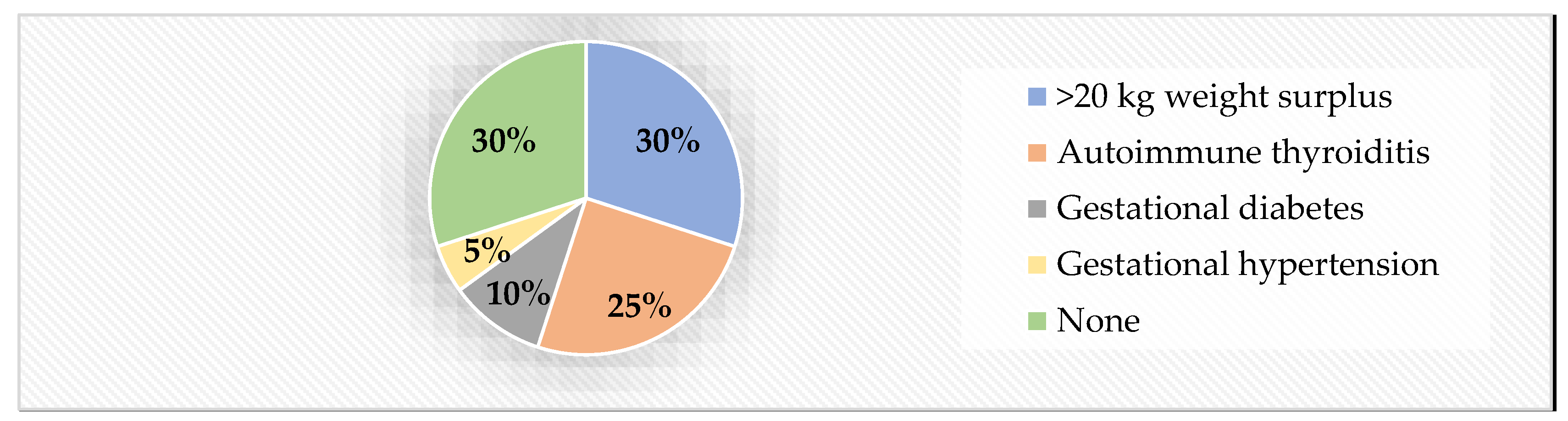
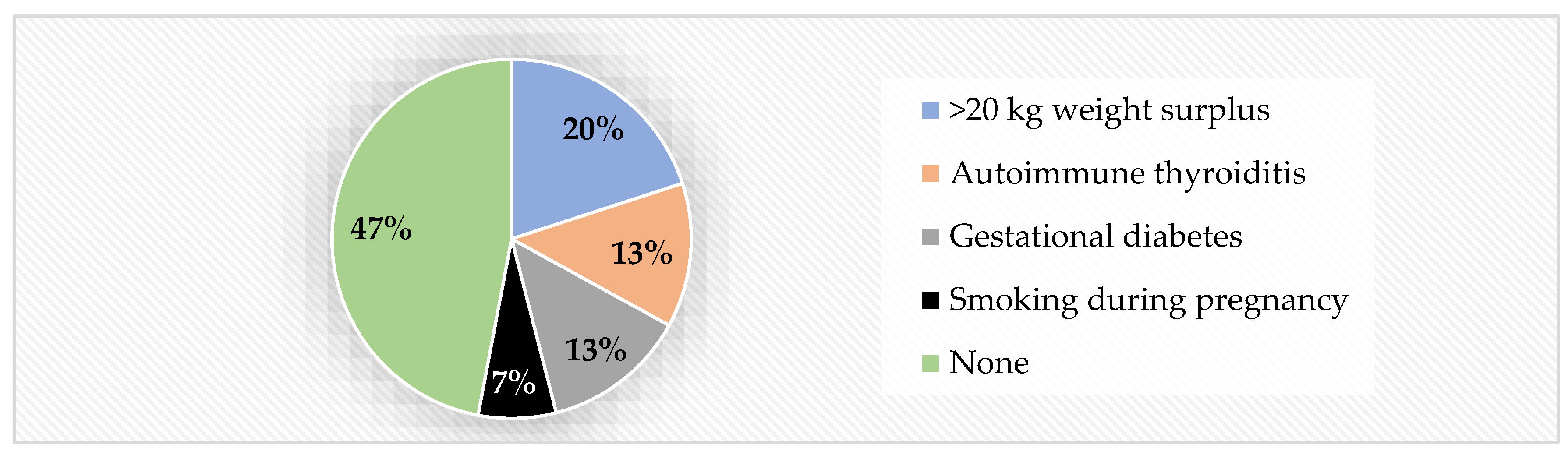
- Biological mother’s health during pregnancy. A total of 53% of overweight patients were born to mothers who had problematic pregnancies. These children showed higher CIMT values than those who were born to healthy mothers (Table 4) and the differences between them were statistically significant (p = 0.042). The most encountered risk factor was weight gain of over 20 kg during pregnancy (20% of cases), followed by autoimmune thyroiditis and gestational diabetes in equal percentages (13%). A total of 7% of mothers admitted to smoking during pregnancy in this group (Figure 4).
- Family history. A total of 60% of overweight kids had an at-risk medical family history (Figure 5). Statistically significantly higher CIMT values were detected in the group with such risk factors within the immediate family, compared to children with negative family history (p = 0.049).
- High blood pressure. Even fewer children presented high blood pressure in the overweight group (13%, compared to 20% in the obese group). However, the CIMT values were significantly higher in hypertensive children than in non-hypertensive ones (p = 0.012).
- Smoking. CIMT mean was higher in smoking overweight children, but the differences were not statistically significant due to the small case sample (p = 0.06). Even so, smoking remains a solid risk factor for increased CIMT, in overweight children as well.
- Lifestyle. A total of 40% of overweight children admitted to leading a sedentary lifestyle, with less than 1 h of physical activity per day. However, the higher values of CIMT in the risk group were not statistically significant (p = 0.324).
3.3.3. Normal-Weight Patients
- Postnatal nutrition. Only 36% of normal-weight children received formula as nurslings, and their CIMT mean values scored higher than in the breastfed group ( = 0.41 mm vs. = 0.37 mm).
- Birthweight. Birth weight had no influence on the outcome of CIMT; 52% of children had normal BW and a = 0.38 mm CIMT, whereas 48% had abnormal BW (8% <2500 g and = 0.39 mm CIMT, and 40% >3500 g and = 0.4 mm CIMT, respectively).
- Biological mother’s health during pregnancy. Unhealthy pregnancy seemed to be a valid risk factor for higher CIMT ( = 0.43 mm vs. = 0.37 mm) even in normal-weight children; however, only 32% of normal-weight children were born from unhealthy pregnancies, compared to 70% in the case of obese children and 53% in the case of overweight children, respectively. A total of 12% of unhealthy pregnancies were due to >20 kg weight gain and 8% due to autoimmune thyroiditis, whereas gestational diabetes, gestational hypertension, and smoking during pregnancy added up to 4% each. A total of 68% of pregnancies that resulted in normal-weight children were declared completely physiological.
- Family history. Up to 72% of normal-weight children had no family history of cardiometabolic diseases. CIMT mean values scored higher in children with at-risk family history, but the differences were not statistically significant ( = 0.42 mm vs. = 0.3 mm, p = 0.2). Out of the 28% of children with a history of cardiometabolic diseases in their immediate family, 16% declared obesity, whereas autoimmune thyroiditis, high blood pressure, and type 2 diabetes each added up 4%.
- High blood pressure. Out of the 25 overall subjects with high blood pressure, only one patient belonged to the normal-weight group.
- Smoking. The same situation was detected for the risk factor of smoking: One patient out of the 25 smoking patients belonged to the normal-weight group.
- Lifestyle. Up to 68% of normal-weight controls led healthy lifestyles with regard to physical activity (>1 h of exercise/day and/or practicing an organized sport). Those patients presented lower values for CIMT than children with sedentary lifestyles, but the differences were not statistically significant (p = 0.24).
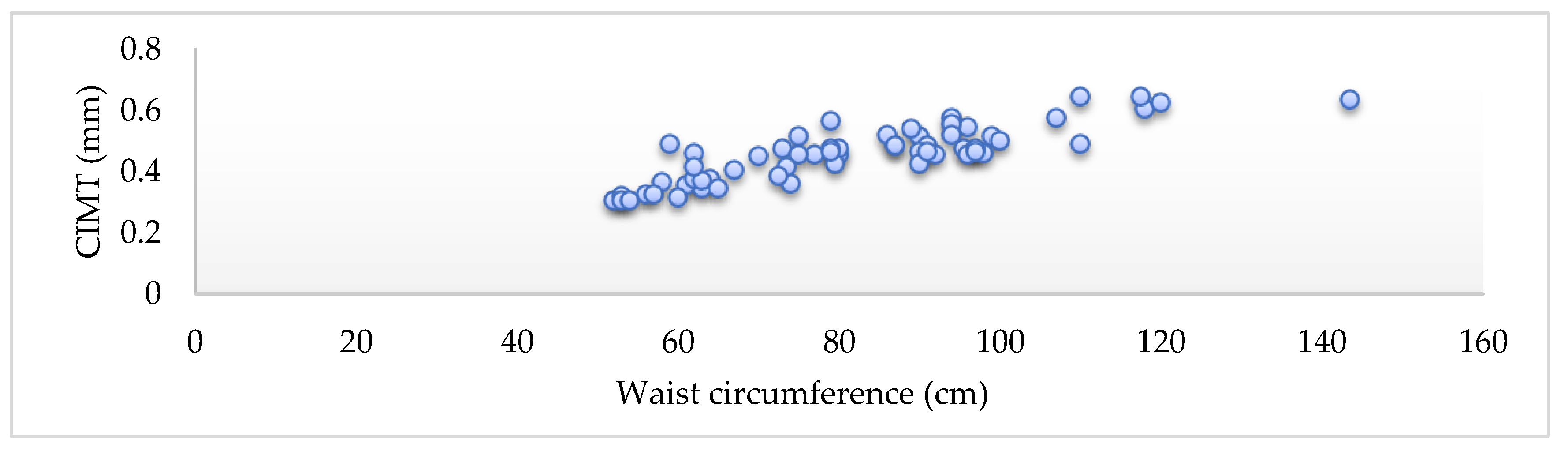
3.4. Assessment of Waist Circumference and CIMT
3.4.1. Waist Circumference in Obese Children
3.4.2. Waist Circumference in Overweight Children
3.4.3. Waist Circumference in Normal-Weight Children
- Mean waist circumference was = 63.9 cm, with no difference between girls and boys (p = 0.96).
3.5. Assessment of Blood Parameters and CIMT
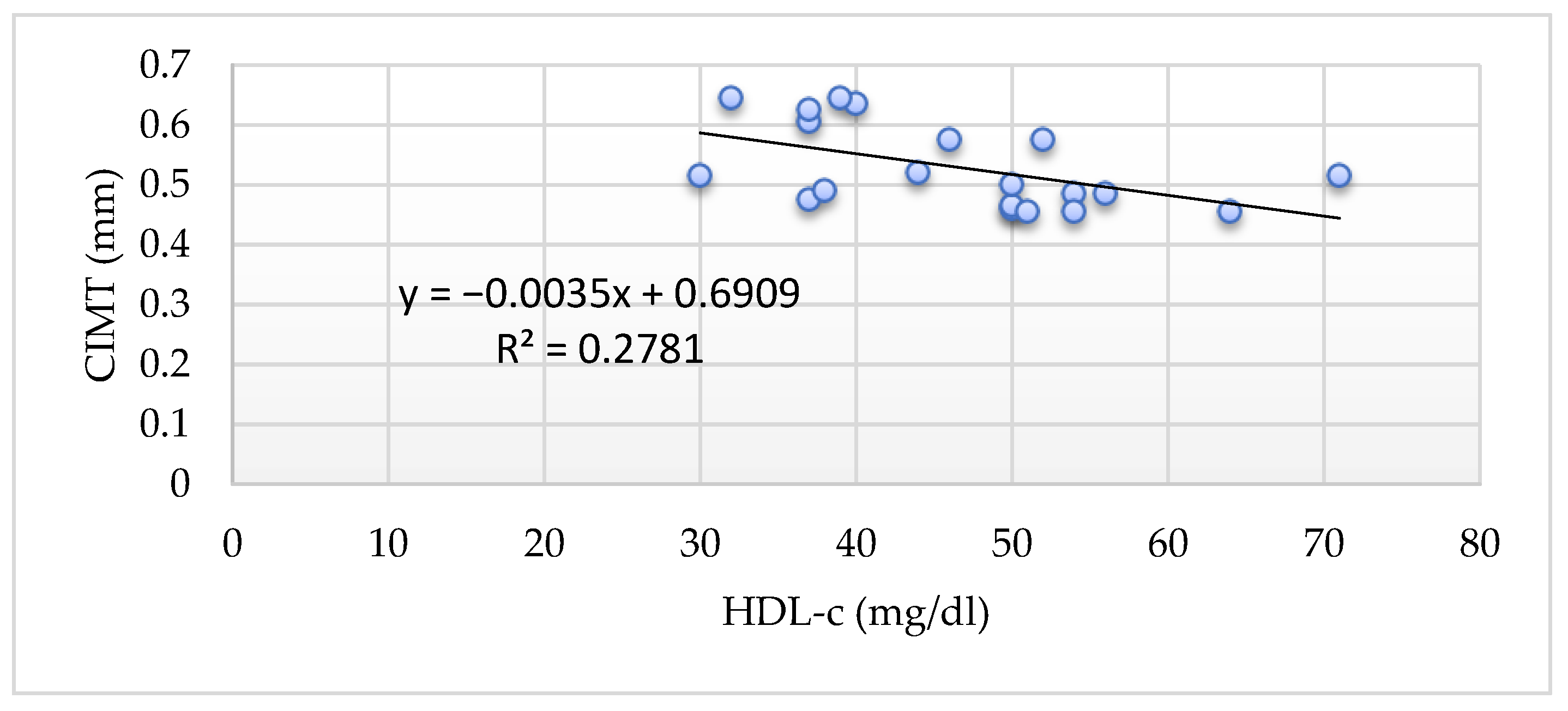
3.5.1. HDL Cholesterol and CIMT
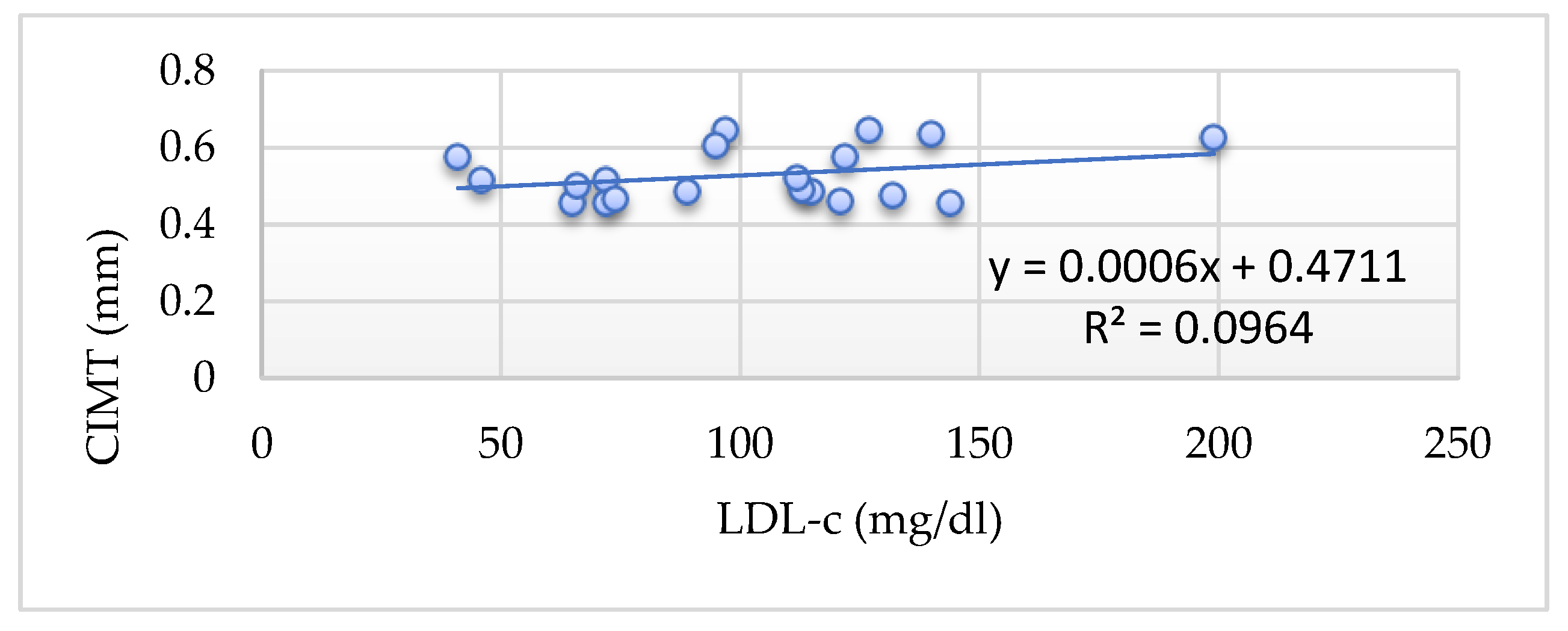
3.5.2. LDL-Cholesterol and CIMT
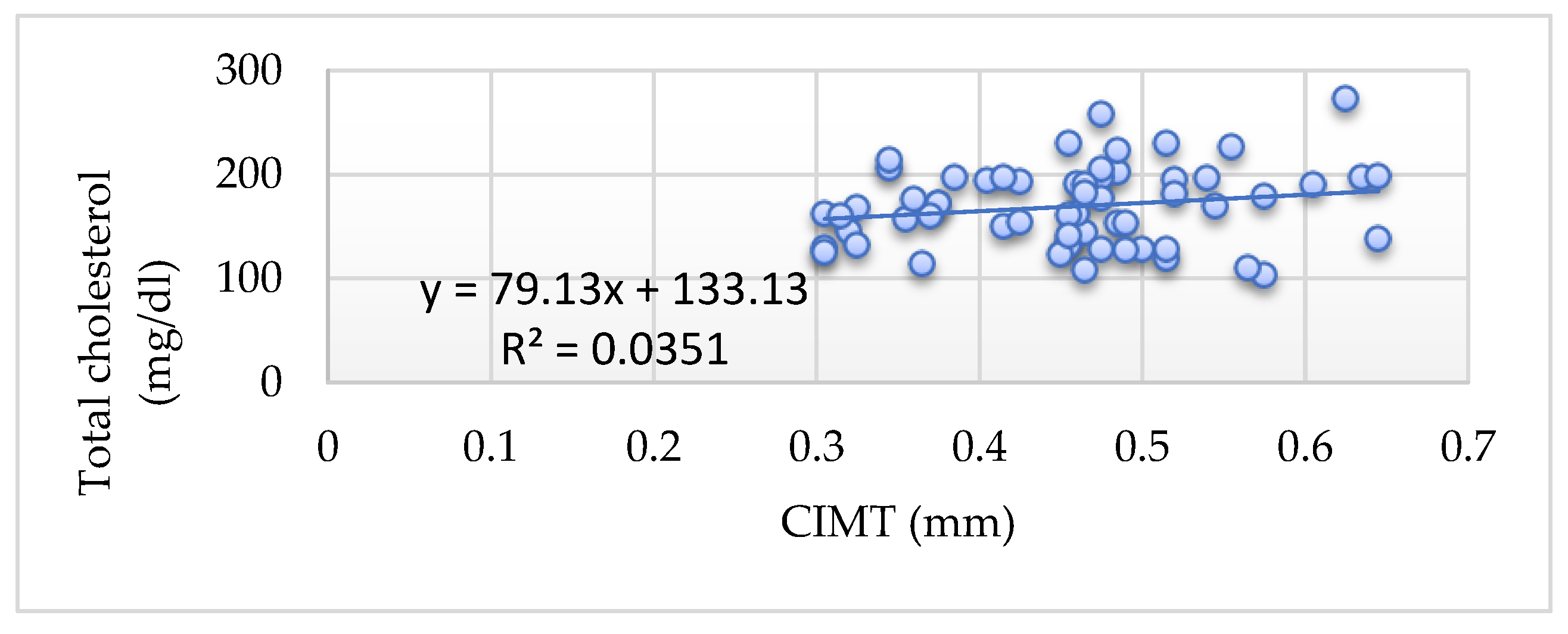
3.5.3. Total Cholesterol and CIMT
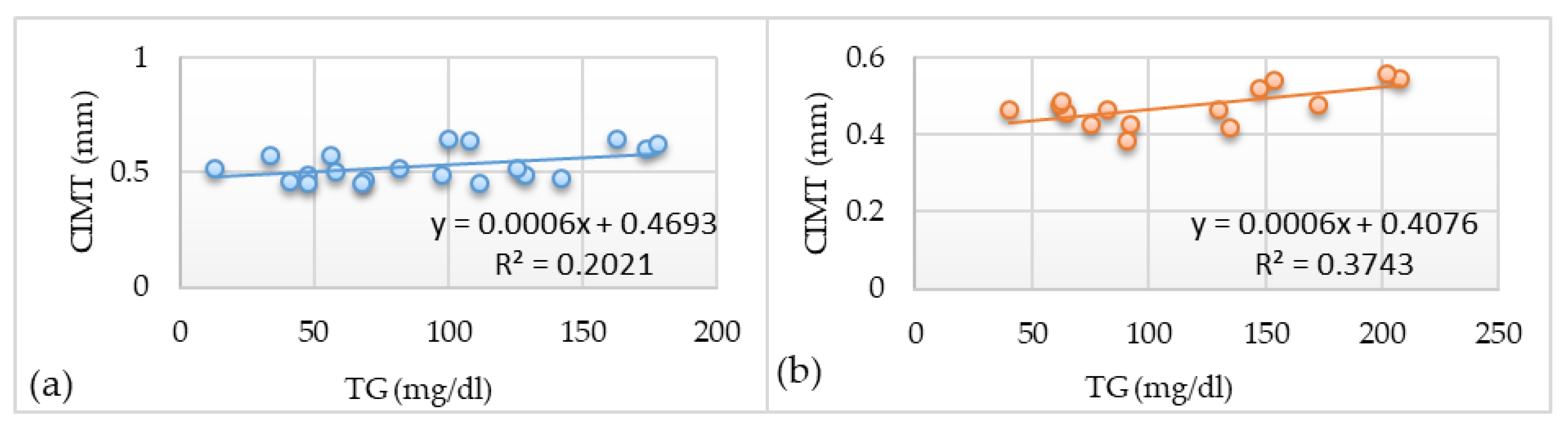
3.5.4. Triglycerides and CIMT
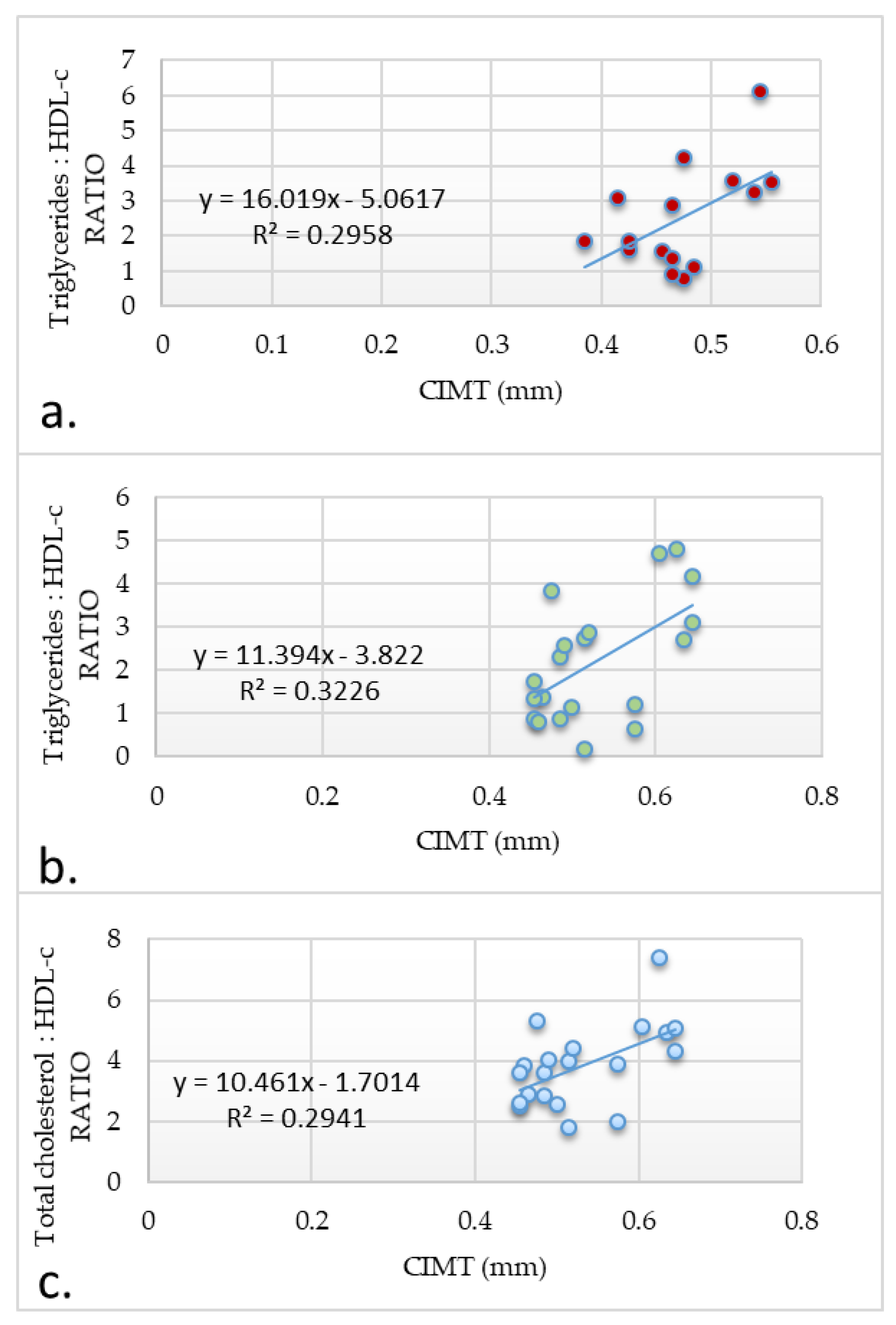
3.5.5. Non-HDL Cholesterol, Total Cholesterol/HDL-c Ratio, Triglyceride/HDL-c Ratio, and CIMT
3.5.6. Fasting Glucose and CIMT
3.6. Multivariate Regression Linear Model
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Browne, N.T.; Snethen, J.A.; Greenberg, C.S.; Frenn, M.; Kilanowski, J.F.; Gance-Cleveland, B.; Burke, P.; Lewandowski, L. When Pandemics Collide: The Impact of COVID-19 on Childhood Obesity. J. Pediatr. Nurs. 2021, 56, 90–98. [Google Scholar] [CrossRef] [PubMed]
- Stavridou, A.; Kapsali, E.; Panagouli, E.; Thirios, A.; Polychronis, K.; Bacopoulou, F.; Psaltopoulou, T.; Tsolia, M.; Sergentanis, T.N.; Tsitsika, A. Obesity in Children and Adolescents during COVID-19 Pandemic. Children 2021, 8, 135. [Google Scholar] [CrossRef] [PubMed]
- Thompson, M.; Mansfield, B.; Stringer, M.; Stewart, B.; Potter, J.; Fernengel, K. An evidence-based resource for the management of comorbidities associated with childhood overweight and obesity. J. Am. Assoc. Nurse Pract. 2016, 28, 559–570. [Google Scholar] [CrossRef] [PubMed]
- Downing, R., 2nd; Michael, T.; Place, R.; Hoffman, E.; Visich, P. The Influence of Metabolic Syndrome Risk Factors on Carotid Intima Media Thickness in Children. Glob. Pediatr. Health 2021, 8, 2333794X20987453. [Google Scholar] [CrossRef] [PubMed]
- Beauloye, V.; Zech, F.; Tran, H.T.; Clapuyt, P.; Maes, M.; Brichard, S.M. Determinants of early atherosclerosis in obese children and adolescents. J. Clin. Endocrinol. Metab. 2007, 92, 3025–3032. [Google Scholar] [CrossRef] [Green Version]
- Farello, G.; Antenucci, A.; Stagi, S.; Mazzocchetti, C.; Ciocca, F.; Verrotti, A. Metabolically healthy and metabolically unhealthy obese children both have increased carotid intima-media thickness: A case control study. BMC Cardiovasc. Disord. 2018, 18, 1–6. [Google Scholar] [CrossRef] [Green Version]
- Wilson, D.P. Is Atherosclerosis a Pediatric Disease? 2000. In Endotext. South Dartmouth (MA); Feingold, K.R., Anawalt, B., Boyce, A., Chrousos, G., de Herder, W.W., Dhatariya, K., Dungan, K., Hershman, J.M., Hofland, J., Kalra, S., et al., Eds.; MDText.com, Inc.: South Dartmouth, MA, USA, 2000. Available online: https://0-www-ncbi-nlm-nih-gov.brum.beds.ac.uk/books/NBK395576/ (accessed on 3 February 2020).
- Sinning, C.; Wild, P.S.; Echevarria, F.M.; Wilde, S.; Schnabel, R.; Lubos, E.; Herkenhoff, S.; Bickel, C.; Klimpe, S.; Gori, T.; et al. Gutenberg-Heart Study. Sex differences in early carotid atherosclerosis (from the community-based Gu-tenberg-Heart Study). Am. J. Cardiol. 2011, 107, 1841–1847. [Google Scholar] [CrossRef]
- Van den Oord, S.C.; Sijbrands, E.J.; ten Kate, G.L.; van Klaveren, D.; van Domburg, R.T.; van der Steen, A.F.; Schinket, A.F.L. Carotid intima-media thickness for cardiovascular risk assessment: Systematic review and meta-analysis. Atherosclerosis 2013, 228, 1–11. [Google Scholar] [CrossRef]
- Fall, C.H.D.; Barker, D.J.P.; Osmond, C.; Winter, P.D.; Clark, P.M.S.; Hales, C.N. Relation of infant feeding to adult serum cholesterol concentration and death from ischaemic heart disease. BMJ 1992, 304, 801–805. [Google Scholar] [CrossRef] [Green Version]
- Lurbe, E.; Aguilar, F.; Álvarez, J.; Redon, P.; Torró, M.I.; Redon, J. Determinants of Cardiometabolic Risk Factors in the First Decade of Life: A Longitudinal Study Starting at Birth. Hypertension 2018, 71, 437–443. [Google Scholar] [CrossRef]
- Oddy, W.H.; Mori, T.A.; Huang, R.C.; Marsh, J.A.; Pennell, C.E.; Chivers, P.T.; Hands, B.P.; Jacoby, P.; Rzehak, P.; Koletzko, B.V.; et al. Early infant feeding and adiposity risk: From infancy to adulthood. Ann. Nutr. Metab. 2014, 64, 262–270. [Google Scholar] [CrossRef] [Green Version]
- Martin, R.M.; Ebrahim, S.; Griffin, M.; Davey-Smith, G.; Nicolaides, A.N.; Georgiou, N. Breastfeeding and atherosclerosis: Intima-media thickness and plaques at 65-year follow-up of the Boyd Orr cohort. Arterioscler. Thromb. Vasc. Biol. 2005, 25, 1482–1488. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martin, R.M.; McCarthy, A.; Davies, D.P.; Davey Smith, G.; Ben-Shlomo, Y. Association between infant nutrition and blood pressure in early adulthood: The Barry Caerphilly Growth cohort study. Am. J. Clin. Nutr. 2003, 77, 1489–1497. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ravelli, A.C.J.; van der Meulen, J.H.; Osmond, C.; Barker, D.J.P.; Bleker, O.P. Infant feeding and adult glucose tolerance, lipid profile, blood pressure, and obesity. Arch. Dis. Child. 2000, 82, 248–252. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Belbasis, L.; Savvidou, M.D.; Kanu, C.; Evangelou, E.; Tzoulaki, I. Birth weight in relation to health and disease in later life: An umbrella review of systematic reviews and meta-analyses. BMC Med. 2016, 14, 147. [Google Scholar] [CrossRef] [Green Version]
- Skilton, M.R.; Siitonen, N.; Würtz, P.; Viikari, J.S.; Juonala, M.; Seppälä, I.; Laitinen, T.; Lehtimäki, T.; Taittonen, L.; Kähönen, M.; et al. High birth weight is associated with obesity and increased carotid wall thickness in young adults: The cardiovascular risk in young Finns study. Arterioscler. Thromb. Vasc. Biol. 2014, 34, 1064–1068. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Di Bernardo, S.; Mivelaz, Y.; Epure, A.M.; Vial, Y.; Simeoni, U.; Bovet, P.; Younes, S.E.; Chiolero, A.; Sekarski, N. Assessing the consequences of gestational diabetes mellitus on offspring’s cardiovascular health: MySweetHeart Cohort study protocol. BMJ Open 2017, 7, e016972. [Google Scholar]
- Benschop, L.; Schalekamp-Timmermans, S.; Roeters van Lennep, J.E.; Jaddoe, V.W.V.; Steegers, E.A.P.; Ikram, M.K. Cardiovascular Risk Factors Track from Mother to Child. JAHA 2018, 7, e009536. [Google Scholar] [CrossRef] [Green Version]
- Jølving, L.R.; Nielsen, J.; Kesmodel, U.S.; Nielsen, R.G.; Nørgård, B.M.; Beck-Nielsen, S.S. Chronic diseases in the children of women with maternal thyroid dysfunction: A nationwide cohort study. Clin. Epidemiol. 2018, 10, 1381–1390. [Google Scholar] [CrossRef] [Green Version]
- İşgüven, P.; Gündüz, Y.; Kılıç, M. Effects of Thyroid Autoimmunity on Early Atherosclerosis in Euthyroid Girls with Hashimoto’s Thyroiditis. J. Clin. Res. Pediatr. Endocrinol. 2016, 8, 150–156. [Google Scholar] [CrossRef]
- De Giorgis, T.; Giannini, C.; Scarinci, A.; D’Adamo, E.; Agostinelli, S.; Chiarelli, F.; Mohn, A. Family history of premature cardiovascular disease as a sole and independent risk factor for increased carotid intima-media thickness. J. Hypertens. 2009, 27, 822–828. [Google Scholar] [CrossRef]
- Li, S.; Yun, M.; Fernandez, C.; Xu, J.; Srinivasan, S.R.; Chen, W.; Berenson, G.S. Cigarette smoking exacerbates the adverse effects of age and metabolic syndrome on subclinical atherosclerosis: The Bogalusa Heart Study. PLoS ONE 2014, 9, e96368. [Google Scholar] [CrossRef]
- Mozos, I.; Maidana, J.P.; Stoian, D.; Stehlik, M. Gender Differences of Arterial Stiffness and Arterial Age in Smokers. Int. J. Environ. Res. Public Health 2017, 14, 565. [Google Scholar] [CrossRef] [PubMed]
- Burton, A. Parental smoking may set up children for atherosclerosis. Environ. Health Perspect. 2010, 118, A200. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, B.; Li, M.; Chen, B.; Xu, Y.; Li, T.D. Deterioration of endothelial function and carotid intima-media thickness in Tibetan male adolescents exposed to second-hand smoke. JRAAS 2012, 13, 413–419. [Google Scholar] [CrossRef]
- Vuolo, M.; Staff, J. Parent and child cigarette use: A longitudinal, multigenerational study. Pediatrics 2013, 132, e568–e577. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khalil, A.; Huffman, M.D.; Prabhakaran, D.; Osmond, C.; Fall, C.H.D.; Tandon, N.; Lakshmy, R.; Prabhakaran, P.; Biswas, S.K.; Ramji, S.; et al. New Delhi Birth Cohort. Predictors of carotid intima-media thickness and carotid plaque in young Indian adults: The New Delhi birth cohort. Int. J. Cardiol. 2013, 167, 1322–1328. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Magnussen, C.G.; Venn, A.; Thomson, R.; Juonala, M.; Srinivasan, S.R.; Viikari, J.S.; Berenson, G.S.; Dwyer, T.; Raitakari, O.T. The association of pediatric low- and high-density lipoprotein cholesterol dyslipidemia classifications and change in dyslipidemia status with carotid intima-media thickness in adulthood evidence from the cardiovascular risk in Young Finns study, the Bogalusa Heart study, and the CDAH (Childhood Determinants of Adult Health) study. J. Am. Coll. Cardiol. 2009, 53, 860–869. [Google Scholar]
- Santos, I.S.; Bittencourt, M.S.; Goulart, A.C.; Schmidt, M.I.; Diniz, M.F.H.S.; Lotufo, P.A.; Benseñor, I.M. Insulin resistance is associated with carotid intima-media thickness in non-diabetic subjects. A cross-sectional analysis of the ELSA-Brasil cohort baseline. Atherosclerosis 2017, 260, 34–40. [Google Scholar] [CrossRef]
- Mozos, I.; Malainer, C.; Horbańczuk, J.; Gug, C.; Stoian, D.; Luca, C.T.; Atanasov, A.G. Inflammatory Markers for Arterial Stiffness in Cardiovascular Diseases. Front. Immunol. 2017, 8, 1058. [Google Scholar] [CrossRef] [Green Version]
- Velea, I.P.; Albulescu, R.; Arghirescu, S.T. Obezitatea la copil. In Pediatrie-Curs Pentru Studenții Facultății de Medicină: Obezitatea la Copil; Velea, I., Ed.; Editura Victor Babes: Timisoara, Romania, 2016; pp. 289–297. [Google Scholar]
- Bennett, W.E., Jr.; Hendrix, K.S.; Thompson, R.T.; Carroll, A.E.; Downs, S.M. The natural history of weight percentile changes in the first year of life. JAMA Pediatr. 2014, 168, 681–682. Available online: http://jamanetwork.com/journals/jamapediatrics/fullarticle/1867333 (accessed on 15 May 2020). [CrossRef] [PubMed] [Green Version]
- Kumar, S.; Kelly, A.S. Review of Childhood Obesity: From Epidemiology, Etiology, and Comorbidities to Clinical Assessment and Treatment. In Mayo Clinic Proceedings; Elsevier: Amsterdam, The Netherlands, 2017; Volume 92, pp. 251–265. Available online: http://www.mayoclinicproceedings.org/article/S0025-6196(16)30595-X/fulltext (accessed on 5 June 2020).
- Casella, I.B.; Presti, C.; Porta, R.M.; Sabbag, C.R.; Bosch, M.A.; Yamazaki, Y. A practical protocol to measure common carotid artery intima-media thickness. Clinics 2008, 63, 515–520. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gómez-Marcos, M.A.; Recio-Rodríguez, J.I.; Patino-Alonso, M.C.; Agudo-Conde, C.; Gómez-Sanchez, L.; Gómez-Sanchez, M.; Rodríguez-Sánchez, E.; García-Ortiz, L. Protocol for measuring carotid intima-media thickness that best correlates with cardiovascular risk and target organ damage. Am. J. Hypertens. 2012, 25, 955–961. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- El Jalbout, R. Intima-Media Thickness Measurement in Children; Techniques and Reference Values. Am. J. Biomed. Sci. Res. 2020, 7, 101–103. [Google Scholar] [CrossRef] [Green Version]
- Freire, C.M.; Ribeiro, A.L.; Barbosa, F.B.; Lana, A.M.; e Silva, A.C.; Ribeiro-Oliveira, A. Comparison between automated and manual measurements of carotid intima-media thickness in clinical practice. Vasc. Health Risk Manag. 2009, 5, 811–817. [Google Scholar]
- Vermeersch, S.; Rietzschel, E.; De Buyzere, M.; Van Bortel, L.M.; D’Asseler, Y.; Gillebert, T.C.; Verdonck, P.R.; Segers, P. Validation of a new automated IMT measurement algorithm. J. Hum. Hypertens. 2007, 21, 976–978. [Google Scholar] [CrossRef] [Green Version]
- Aydin, Y.; Berker, D.; Ustun, I.; Gul, K.; Erden, G.; Kutlucan, A.; Yilmaz, L.; Guler, S. Evaluation of carotid intima media thickness in impaired fasting glucose and impaired glucose tolerance. Minerva Endocrinol. 2011, 36, 171–179. [Google Scholar] [CrossRef]
- FOR, E.P.O.I.G.; CHILDREN, R.R.I. Expert Panel on Integrated Guidelines for Cardiovascular Health and Risk Reduction in Children and Adolescents; National Heart, Lung, and Blood Institute. Expert panel on integrated guidelines for cardiovascular health and risk reduction in children and adolescents: Summary report. Pediatrics 2011, 128, S213–S256. [Google Scholar] [CrossRef] [Green Version]
- Iwani, N.A.K.Z.; Jalaludin, M.Y.; Zin, R.M.W.M.; Fuziah, M.Z.; Hong, J.Y.H.; Abqariyah, Y.; Mokhtar, A.H.; Nazaimoon, W.M.W. TG : HDL-C Ratio Is a Good Marker to Identify Children Affected by Obesity with Increased Cardiometabolic Risk and Insulin Resistance. Int. J. Endocrinol. 2019, 2019, 8586167. [Google Scholar] [CrossRef]
- Di Giorgis, T.; Marcovecchio, M.L.; Di Giovanni, I.; Giannini, C.; Chiavaroli, V.; Chiarelli, F.; Mohn, A. Triglycerides-to-HDL ratio as a new marker of endothelial dysfunction in obese prepubertal children. Eur. J. Endocrinol. 2013, 170, 173–180. [Google Scholar] [CrossRef]
- Iwani, N.A.K.Z.; Jalaludin, M.Y.; Zin, R.M.W.M.; Fuziah, M.Z.; Hong, J.Y.H.; Abqariyah, Y.; Mokhtar, A.H.; Nazaimoon, W.M.W. Triglyceride to HDL-C ratio is associated with insulin resistance in overweight and obese children. Sci. Rep. 2007, 7, 40055. [Google Scholar] [CrossRef] [Green Version]
- Chakarova, N.; Dimova, R.; Grozeva, G.; Tankova, T. Assessment of glucose variability in subjects with prediabetes. Diabetes Res. Clin. Pract. 2019, 151, 56–64. [Google Scholar] [CrossRef] [Green Version]
- Skilton, M.R.; Boussel, L.; Bonnet, F.; Bernard, S.; Douek, P.C.; Moulin, P.; Serusclat, A. Carotid intima–media and adventitial thickening: Comparison of new and established ultrasound and magnetic resonance imaging techniques. Atherosclerosis 2011, 215, 405–410. [Google Scholar] [CrossRef]
- Zhang, Y.; Guallar, E.; Qiao, Y.; Wasserman, B.A. Arterioscler. Is Carotid Intima-Media Thickness as Predictive as Other Noninvasive Techniques for the Detection of Coronary Artery Disease? Arterioscler. Thromb. Vasc. Biol. 2014, 34, 1341–1345. [Google Scholar] [CrossRef] [Green Version]
- Rudd, J.H.; Narula, J.; Strauss, H.W.; Virmani, R.; Machac, J.; Klimas, M.; Tahara, N.; Fuster, V.; Warburton, E.A.; Fayad, Z.A.; et al. Imaging atherosclerotic plaque inflammation by fluorodeoxyglucose with positron emission tomography: Ready for prime time? J. Am. Coll. Cardiol. 2010, 55, 2527–2535. [Google Scholar] [CrossRef] [Green Version]
- Chirita-Emandi, A.; Papa, M.C.; Abrudan, L.; Dobrescu, M.A.; Puiu, M.; Velea, I.P.; Paul, C. A novel method for measuring subcutaneous adipose tissue using ultrasound in children-interobserver consistency. Rom J. Morphol. Embryol. 2017, 58, 115–123. [Google Scholar]
- Oren, A.; Vos, L.E.; Uiterwaal, C.S.; Gorissen, W.H.; Grobbee, D.E.; Bots, M.L. Birth weight and carotid intima-media thickness: New perspectives from the atherosclerosis risk in young adults (ARYA) study. Ann. Epidemiol. 2004, 14, 8–16. [Google Scholar] [CrossRef] [Green Version]
- Epure, A.M.; Rios-Leyvraz, M.; Anker, D.; Di Bernardo, S.; Da Costa, B.R.; Chiolero, A.; Sekarski, N. Risk factors during first 1,000 days of life for carotid intima-media thickness in infants, children, and adolescents: A systematic review with meta-analyses. PLoS Med. 2020, 17, e1003414. [Google Scholar] [CrossRef]
- Verburg, B.O.; Jaddoe, V.W.; Wladimiroff, J.W.; Hofman, A.; Witteman, J.C.; Steegers, E.A. Fetal hemodynamic adaptive changes related to intrauteringrowth: The Generation R Study. Circulation 2008, 117, 649–659. [Google Scholar] [CrossRef] [Green Version]
- Golab, B.; Santos, S.; Voerman, E.; Lawlor, D.; Jaddoe, V.; Gaillard, R. Common pregnancy complications and risk of childhood obesity-influence of maternal obesity: An individual participant data. Lancet Child Adolesc. Health 2019, 2, 812. [Google Scholar] [CrossRef] [Green Version]
- Grieger, J.A.; Clifton, V.L. A review of the impact of dietary intakes in human pregnancy on infant birthweight. Nutrients 2015, 7, 153–178. [Google Scholar] [CrossRef] [Green Version]
- Crispi, F.; Bijnens, B.; Figueras, F.; Bartrons, J.; Eixarch, E.; Le Noble, F.; Ahmed, A.; Gratacós, E. Fetal growth restriction results in remodeled and less efficient hearts in children. Circulation 2010, 121, 2427–2436. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Crispi, F.; Miranda, J.; Gratacós, E. Long-term cardiovascular consequences of fetal growth restriction: Biology, clinical implications, and opportunities for prevention of adult disease. Am. J. Obstet. Gynecol. 2018, 218, S869–S879. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Corica, D.; Aversa, T.; Valenzise, M.; Messina, M.F.; Alibrandi, A.; De Luca, F.; Wasniewska, M. Does family history of obesity, cardiovascular, and metabolic diseases influence onset and severity of childhood obesity? Front. Endocrinol. 2018, 9, 187. [Google Scholar] [CrossRef]
- Ambrose, J.A.; Barua, R.S. The pathophysiology of cigarette smoking and cardiovascular disease: An update. J. Am. Coll. Cardiol. 2004, 43, 1731–1737. [Google Scholar] [CrossRef] [Green Version]
- Costopoulos, C.; Liew, T.V.; Bennett, M. Ageing and atherosclerosis: Mechanisms and therapeutic options. Biochem. Pharmacol. 2008, 75, 1251–1261. [Google Scholar] [CrossRef] [PubMed]
- Sorof, J.; Danies, S. Obesity Hypertension in Children-A Problem of Epidemic Proportions. Hypertension 2002, 40, 441–447. [Google Scholar] [CrossRef] [Green Version]
- National High Blood Pressure Education Program Working Group on High Blood Pressure in Children and Adolescents. The fourth report on the diagnosis, evaluation, and treatment of high blood pressure in children and adolescents. Pediatrics 2004, 114, 1–22. [Google Scholar]
- Lande, M.B.; Carson, N.L.; Roy, J.; Meagher, C.C. Effects of Childhood Primary Hypertension on Carotid Intima Media Thickness-A Matched Controlled Study. Hypertension 2006, 48, 40–44. [Google Scholar] [CrossRef] [Green Version]
- Keane, E.; Li, X.; Harrington, J.M.; Fitzgerald, A.P.; Perry, I.J.; Kearney, P.M. Physical Activity, Sedentary Behavior and the Risk of Overweight and Obesity in School-Aged Children. Pediatr. Exerc. Sci. 2017, 29, 408–418. [Google Scholar] [CrossRef]
- Bassali, R.; Waller, J.L.; Gower, B.; Allison, J.; Davis, C.L. Utility of waist circumference percentile for risk evaluation in obese children. Int. J. Pediatr. Obes. 2010, 5, 97–101. [Google Scholar] [CrossRef]
- Freedman, D.S.; Kahn, H.S.; Mei, Z.; Grummer-Strawn, L.M.; Dietz, W.H.; Srinivasan, S.R.; Berenson, G.S. Relation of body mass index and waist-to-height ratio to cardiovascular disease risk factors in children and adolescents: The Bogalusa Heart Study. Am. J. Clin. Nutr. 2007, 86, 33–40. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stefan, N.; Kantartzis, K.; Machannm, J.; Schick, F.; Thamer, C.; Rittig, K.; Balletshofer, B.; Machicao, F.; Fritsche, A.; Häring, H.U. Identification and characterization of metabolically benign obesity in humans. Arch. Intern. Med. 2008, 168, 1609–1616. [Google Scholar] [CrossRef] [PubMed]
- Kamon, T.; Kaneko, H.; Itoh, H.; Kiriyama, H.; Mizuno, Y.; Morita, H.; Yamamichi, N.; Komuro, I. Association Between Waist Circumference and Carotid Intima-Media Thickness in the General Population. Int. Heart J. 2020, 61, 103–108. [Google Scholar] [CrossRef] [Green Version]
- Toth, P.P. Reverse cholesterol transport: High-density lipoprotein’s magnificent mile. Curr. Atheroscler. Rep. 2003, 5, 386–393. [Google Scholar] [CrossRef]
- Kosmas, C.E.; Martinez, I.; Sourlas, A.; Bouza, K.V.; Campos, F.N.; Torres, V.; Montan, P.D.; Guzman, E. High-density lipoprotein (HDL) functionality and its relevance to atherosclerotic cardiovascular disease. Drugs Context 2018, 7, 212525. [Google Scholar] [CrossRef]
- O’Donovan, G.; Stensel, D.; Hamer, M.; Stamatakis, E. The association between leisure-time physical activity, low HDL-cholesterol and mortality in a pooled analysis of nine population-based cohorts. Eur. J. Epidemiol. 2017, 32, 559–566. [Google Scholar] [CrossRef] [Green Version]
- Nicholls, S.J.; Lundman, P.; Harmer, J.A.; Cutri, B.; Griffiths, K.A.; Rye, K.A.; Barter, P.J.; Celermajer, D.S. Consumption of saturated fat impairs the anti-inflammatory properties of high-density lipoproteins and endothelial function. J. Am. Coll. Cardiol. 2006, 48, 715–720. [Google Scholar] [CrossRef]
- Peterson, J.; Bihain, B.E.; Bengtsson-Olivecrona, G.; Deckelbaum, R.J.; Carpentier, Y.A.; Olivecrona, T. Fatty acid control of lipoprotein lipase: A link between energy metabolism and lipid transport. Proc. Natl. Acad. Sci. USA 1990, 87, 909–913. [Google Scholar] [CrossRef] [Green Version]
- Hatami, M.; Tohidi, M.; Mohebi, R.; Khalili, D.; Azizi, F.; Hadaegh, F. Adolescent lipoprotein classifications according to National Health and Nutrition Examination Survey (NHANES) vs. National Cholesterol Education Program (NCEP) for predicting abnormal lipid levels in adulthood in a Middle East population. Lipids Health Dis. 2012, 11, 107. [Google Scholar] [CrossRef] [Green Version]
- Kusters, D.M.; Wiegman, A.; Kastelein, J.J.P.; Hutten, B.A. Carotid Intima-Media Thickness in Children With Familial Hypercholesterolemia. Circ. Res. 2014, 114, 307–310. [Google Scholar] [CrossRef] [Green Version]
- Gortmaker, S.L.; Swinburn, B.A.; Levy, D.; Carter, R.; Mabry, P.L.; Finegood, D.T.; Huang, T.; Marsh, T.; Moodie, M.L. Changing the future of obesity: Science, policy, and action. Lancet 2011, 378, 838–847. [Google Scholar] [CrossRef] [Green Version]
- May, A.L.; Kuklina, E.V.; Yoon, P.W.; Centers for Disease Control and Prevention (CDC). Prevalence of abnormal lipid levels among youths–United States, 1999–2006. Morb. Mortal. Wkly. Rep. 2010, 59, 29–33. [Google Scholar]
- Boullart, A.C.; de Graaf, J.; Stalenhoef, A.F. Serum triglycerides and risk of cardiovascular disease. Biochim. Et Biophys. Acta (BBA)-Mol. Cell Biol. Lipids 2012, 1821, 867–875. [Google Scholar] [CrossRef] [PubMed]
- Gardener, H.; Della Morte, D.; Elkins, M.S.; Sacco, R.L.; Rundek, T. Lipids and carotid plaque in the Northern Manhattan Study. BMC Cardiovasc. Disord. 2009, 9, 55. [Google Scholar] [CrossRef] [Green Version]
- Touboul, P.J.; Labreuche, J.; Bruckert, E.; Schargrodsky, H.; Prati, P.; Tosetto, A.; Hernandez-Hernandez, R.; Woo, K.S.; Silva, H.; Vicaut, E.; et al. HDL-C, triglycerides and carotid IMT: A meta-analysis of 21,000 patients with automated edge detection IMT measurement. Atherosclerosis 2014, 232, 65–71. [Google Scholar] [CrossRef]
- Durrington, P. Triglycerides are more important in atherosclerosis than epidemiology suggested. Atherosclerosis 1998, 141, S57–S62. [Google Scholar] [CrossRef]
- Karpe, F.; Boquist, S.; Tang, R.; Bond, G.M.; de Faire, U.; Hamsten, A. Remnant lipoproteins are related to intima-media thickness of the carotid artery independently of LDL cholesterol and plasma triglycerides. J. Lipid Res. 2001, 42, 17–21. [Google Scholar] [CrossRef]
- Ander, B.P.; Dupasquier, C.M.; Prociuk, M.A.; Pierce, G.N. Polyunsaturated fatty acids and their effects on cardiovascular disease. Exp. Clin. Cardiol. 2003, 8, 164–172. [Google Scholar]
- Serafim, V.; Chirita-Emandi, A.; Andreescu, N.; Tiugan, D.A.; Tutac, P.; Paul, C.; Velea, I.; Mihailescu, A.; Șerban, C.L.; Zimbru, C.G.; et al. Single Nucleotide Polymorphisms in PEMT and MTHFR Genes are Associated with Omega 3 and 6 Fatty Acid Levels in the Red Blood Cells of Children with Obesity. Nutrients 2019, 11, 2600. [Google Scholar] [CrossRef] [Green Version]
- Frontini, M.G.; Srinivasan, S.R.; Xu, J.; Tang, R.; Bond, M.G.; Berenson, G.S. Usefulness of childhood non-high density lipoprotein cholesterol levels versus other lipoprotein measures in predicting adult subclinical atherosclerosis: The Bogalusa Heart Study. Pediatrics 2008, 121, 924–929. [Google Scholar] [CrossRef] [PubMed]
- Juonala, M.; Wu, F.; Sinaiko, A.; Woo, J.G.; Urbina, E.M.; Jacobs, D.; Steinberger, J.; Prineas, R.; Koskinen, J.; Sabin, M.A.; et al. Non-HDL Cholesterol Levels in Childhood and Carotid Intima-Media Thickness in Adulthood. Pediatrics 2020, 145, e20192114. [Google Scholar] [CrossRef]
- Lemieux, I.; Lamarche, B.; Couillard, C.; Pascot, A.; Cantin, B.; Bergeron, J.; Dagenais, G.R.; Després, J.P. Total Cholesterol/HDL Cholesterol Ratio vs LDL Cholesterol/HDL Cholesterol Ratio as Indices of Ischemic Heart Disease Risk in Men: The Quebec Cardiovascular Study. Arch. Intern. Med. 2001, 161, 2685–2692. [Google Scholar] [CrossRef]
- Krawczyk, M.; Rumińska, M.; Witkowska-Sędek, E.; Majcher, A.; Pyrżak, B. Usefulness of the triglycerides to high-density lipoprotein cholesterol ratio (TG/HDL-C) in prediction of metabolic syndrome in polish obese children and adolescents. Acta Biochim. Pol. 2018, 65, 605–611. [Google Scholar] [CrossRef] [PubMed]
- Hagman, E.; Ighani Arani, P.; Fischer, M.; Danielsson, P.; Marcinkiewicz, K.; Petriczko, E.; Marcus, C. Blood sugar levels are higher in young obese children in Sweden than in Poland. Acta Paediatr. 2014, 103, 1174–1178. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Amer Diabet, A. Diagnosis and classification of diabetes mellitus American Diabetes Association. Diabetes Care 2011, 34, S62–S69. [Google Scholar]
- Hagman, E.; Reinehr, T.; Kowalski, J.; Ekbom, A.; Marcus, C.; Holl, R.W. Impaired fasting glucose prevalence in two nationwide cohorts of obese children and adolescents. Int. J. Obes. 2014, 38, 40–45. [Google Scholar] [CrossRef] [Green Version]












{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Obese Group | Group Number | % of Entire Group | Mean CIMT (mm) |
| <12 years | I | 55% | 0.48 |
| 12–15 years | II | 25% | 0.49 |
| ≥16 years | III | 20% | 0.50 |
| Comparison | I vs. II | I vs. III | II vs. III |
| p-value | 0.71 | 0.59 | 0.88 |
| Overweight Group | Group Number | % of Entire Group | Mean CIMT (mm) |
| <12 years | I | 34% | 0.43 |
| 12–15 years | II | 53% | 0.48 |
| ≥16 years | III | 13% | 0.54 |
| Comparison | I vs. II | I vs. III | II vs. III |
| p-value | 0.11 | 0.024 | 0.21 |
| Normal-Weight Group | Group Number | % of Entire Group | Mean CIMT (mm) |
| <12 years | I | 48% | 0.35 |
| 12–15 years | II | 40% | 0.4 |
| ≥16 years | III | 12% | 0.51 |
| Comparison | I vs. II | I vs. III | II vs. III |
| p-value | 0.042 | 0.0006 | 0.012 |
| Group | Sex | % of Entire Group | Mean CIMT (mm) | p-Value |
|---|---|---|---|---|
| Obese | Girls | 35% | 0.5135 | 0.99 |
| Boys | 65% | 0.5134 | ||
| Overweight | Girls | 33% | 0.43 | 0.043 |
| Boys | 67% | 0.49 | ||
| Normal | Girls | 52% | 0.38 | 0.55 |
| Boys | 48% | 0.4 |
| Risk Factor | % of Total Obese Children | Mean CIMT (mm) | p-Value | |
|---|---|---|---|---|
| Postnatal food | Formula | 65% | 0.53 | 0.99 |
| Breastmilk | 35% | 0.53 | ||
| Birth weight | <2500 g | 25% | 0.54 | 0.62 |
| >3500 g | 25% | 0.53 | ||
| normal | 50% | 0.52 | ||
| Biological mother’s health | Risk factors present | 70% | 0.55 | 0.047 |
| No risk factors | 30% | 0.48 | ||
| Family history | Risk factors present | 75% | 0.54 | 0.11 |
| No risk factors | 25% | 0.48 | ||
| Smoking | Smoker | 15% | 0.61 | 0.015 |
| Non-smoker | 85% | 0.51 | ||
| High blood pressure | Yes | 20% | 0.58 | 0.1 |
| No | 80% | 0.51 | ||
| Lifestyle | Sedentary | 65% | 0.55 | 0.89 |
| Normal | 35% | 0.49 | ||
| CIMT median for entire obese group (mm) | 0.50 |
| Risk Factor | % of Total Overweight Children | Mean CIMT (mm) | p-Value | |
|---|---|---|---|---|
| Postnatal food | Formula | 47% | 0.5 | 0.023 |
| Breast milk | 53% | 0.44 | ||
| Birth weight | <2500 g | 20% | 0.45 | 0.48 |
| >3500 g | 33% | 0.5 | ||
| Normal | 47% | 0.46 | ||
| Biological mother’s health | Risk factors present | 53% | 0.49 | 0.042 |
| No risk factors | 47% | 0.44 | ||
| Family history | Risk factors present | 60% | 0.49 | 0.049 |
| No risk factors | 40% | 0.44 | ||
| Smoking | Smoker | 13% | 0.53 | 0.06 |
| Non-smoker | 87% | 0.46 | ||
| High blood pressure | Yes | 13% | 0.55 | 0.012 |
| No | 87% | 0.46 | ||
| Lifestyle | Sedentary | 40% | 0.49 | 0.32 |
| Normal | 60% | 0.46 | ||
| for entire overweight group (mm) | 0.47 |
| Risk Factor | % of Total Normal-Weight Children | Mean CIMT (mm) | p-Value | |
|---|---|---|---|---|
| Postnatal food | Formula | 36% | 0.41 | 0.25 |
| Breastmilk | 64% | 0.38 | ||
| Birth weight | <2500 g | 8% | 0.39 | 0.5 |
| >3500 g | 40% | 0.40 | ||
| Normal | 52% | 0.38 | ||
| Biological mother’s health | Abnormal | 32% | 0.43 | 0.09 |
| Normal | 68% | 0.37 | ||
| Family history | Abnormal | 28% | 0.42 | 0.2 |
| Normal | 72% | 0.38 | ||
| Smoking | Smoker | 4% | 0.56 | N/A |
| Non-smoker | 96% | 0.38 | ||
| Hypertension | Yes | 4% | 0.47 | N/A |
| No | 96% | 0.39 | ||
| Lifestyle | Sedentary | 32% | 0.42 | 0.24 |
| Normal | 68% | 0.38 | ||
| CIMT median for entire normal-weight group (mm) | 0.37 |
| CIMT Median (mm) | BMI (kg/m2) | LDL-c (mg/dL) | Total Cholesterol (mg/dL) | Triglycerides (mg/dL) | Blood Pressure (mmHg) | ||
|---|---|---|---|---|---|---|---|
| Spearman’s ρ | 0.69 ** | Pearson’s r | 0.88 * | 0.43 | 0.34 | 0.42 | 0.61 * |
| p-value | 0.0006 | p-value | <0.001 | 0.06 | 0.14 | 0.06 | 0.004 |
| CIMT Median (mm) | BMI (kg/m2) | Triglycerides (mg/dL) | LDL-c (mg/dL) | Total Cholesterol (mg/dL) | Blood Pressure (mmHg) | ||
|---|---|---|---|---|---|---|---|
| Spearman’s ρ | 0.77 ** | 0.88 ** | 0.23 | Pearson’s r | 0.375 | 0.38 | 0.405 * |
| p-value | <0.001 | <0.001 | 0.26 | p-value | 0.065 | 0.06 | 0.044 |
| Obese Group | Overweight Group | Normal-Weight Group | |
|---|---|---|---|
| HDL-c—CIMT | −0.53 | −0.031 | −0.25 |
| LDL-c—CIMT | 0.31 | 0.04 | 0.07 |
| Total Cholesterol—CIMT | 0.23 | 0.151 | 0.07 |
| Triglycerides—CIMT | 0.45 | 0.6 | 0.08 |
| Non-HDL-c—CIMT | 0.14 | 0.19 | 0.34 |
| TC:HDL-c ratio—CIMT | 0.29 | 0.27 | 0.54 |
| TG:HDL-c ratio—CIMT | 0.16 | 0.54 | 0.56 |
| Fasting glucose—CIMT | −0.3 | 0.21 | −0.1 |
| Normal Weight | Overweight | Obese | |
|---|---|---|---|
| Values | |||
| Non-HDL-c (mg/dL) | 119 | 134 | 122.7 |
| TC/HDL-c ratio | 4 | 3.8 | 3.8 |
| TG/HDL-c ratio | 2 | 2.5 | 2.2 |
| Model | R | R-Square | Adjusted R-Square | Std. Error of the Estimate | Change Statistics | ||||
|---|---|---|---|---|---|---|---|---|---|
| R-Square Change | F-Change | df1 | df2 | Sig. F-Change | |||||
| 1 | 0.855 | 0.732 | 0.727 | 0.04679 | 0.732 | 158.266 | 1 | 58 | 0.000 |
| 2 | 0.284 | 0.081 | 0.065 | 0.08663 | 0.081 | 5.097 | 1 | 58 | 0.028 |
| Beta In | t | Sig. | Partial Correlation | Collinearity Statistics | |||
|---|---|---|---|---|---|---|---|
| Tolerance | VIF | Minimum Tolerance | |||||
| LDL-c | 0.005 | 0.069 | 0.945 | 0.009 | 0.981 | 1.020 | 0.981 |
| HDL-c | −0.078 | −1.151 | 0.255 | −0.151 | 1.000 | 1.000 | 1.000 |
| TG | 0.068 | 0.964 | 0.339 | 0.127 | 0.941 | 1.063 | 0.941 |
| TC | 0.010 | 0.148 | 0.883 | 0.020 | 0.957 | 1.045 | 0.957 |
| Non-HDL-c | 0.081 | 0.537 | 0.594 | 0.071 | 0.701 | 1.427 | 0.701 |
| TC/HDL-c ratio | 0.059 | 0.312 | 0.756 | 0.041 | 0.447 | 2.235 | 0.447 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mihuta, M.-S.; Paul, C.; Ciulpan, A.; Dacca, F.; Velea, I.P.; Mozos, I.; Stoian, D. Subclinical Atherosclerosis Progression in Obese Children with Relevant Cardiometabolic Risk Factors Can Be Assessed through Carotid Intima Media Thickness. Appl. Sci. 2021, 11, 10721. https://0-doi-org.brum.beds.ac.uk/10.3390/app112210721
Mihuta M-S, Paul C, Ciulpan A, Dacca F, Velea IP, Mozos I, Stoian D. Subclinical Atherosclerosis Progression in Obese Children with Relevant Cardiometabolic Risk Factors Can Be Assessed through Carotid Intima Media Thickness. Applied Sciences. 2021; 11(22):10721. https://0-doi-org.brum.beds.ac.uk/10.3390/app112210721
Chicago/Turabian StyleMihuta, Monica-Simina, Corina Paul, Adrian Ciulpan, Farah Dacca, Iulian Puiu Velea, Ioana Mozos, and Dana Stoian. 2021. "Subclinical Atherosclerosis Progression in Obese Children with Relevant Cardiometabolic Risk Factors Can Be Assessed through Carotid Intima Media Thickness" Applied Sciences 11, no. 22: 10721. https://0-doi-org.brum.beds.ac.uk/10.3390/app112210721