Virtual Surgical Planning and the “In-House” Rapid Prototyping Technique in Maxillofacial Surgery: The Current Situation and Future Perspectives

 , , ,
, , ,  , and
, and
Abstract
:1. Introduction
2. Materials and Methods
- A.
- Reconstructive surgery
- B.
- Traumatology:
- B.1:
- Fractures of the orbital floor
- B.2:
- Fractures of the zygomatic arch
- C.
- The COVID-19 pandemic
- A. Reconstructive surgery in oncological cases
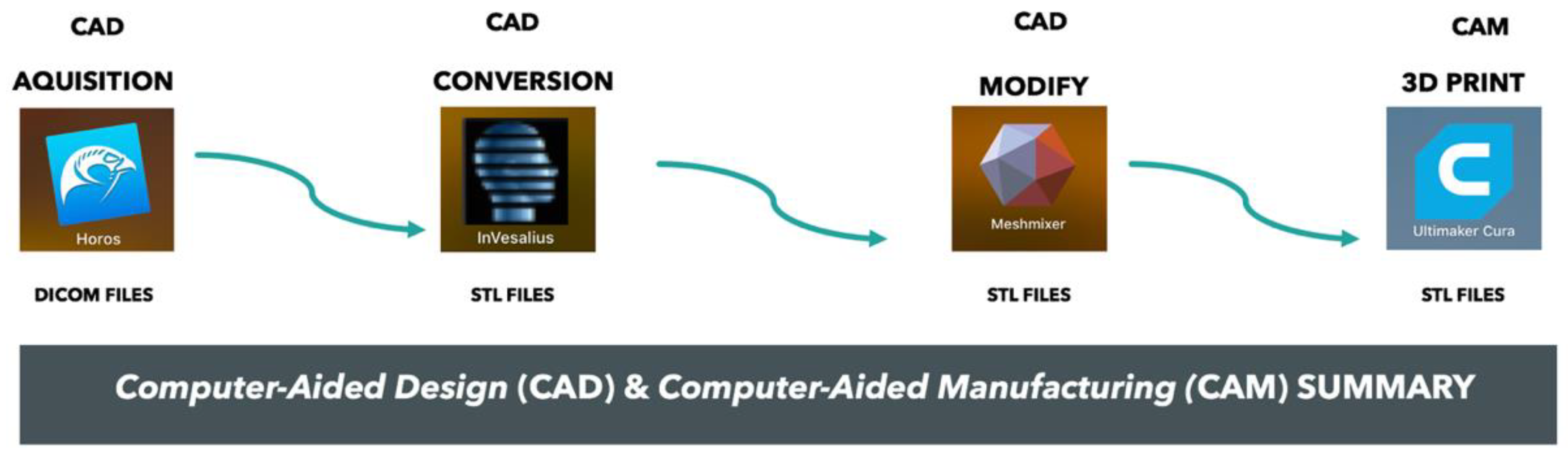
- (1)
- Transformation of the DICOM data into STL files.
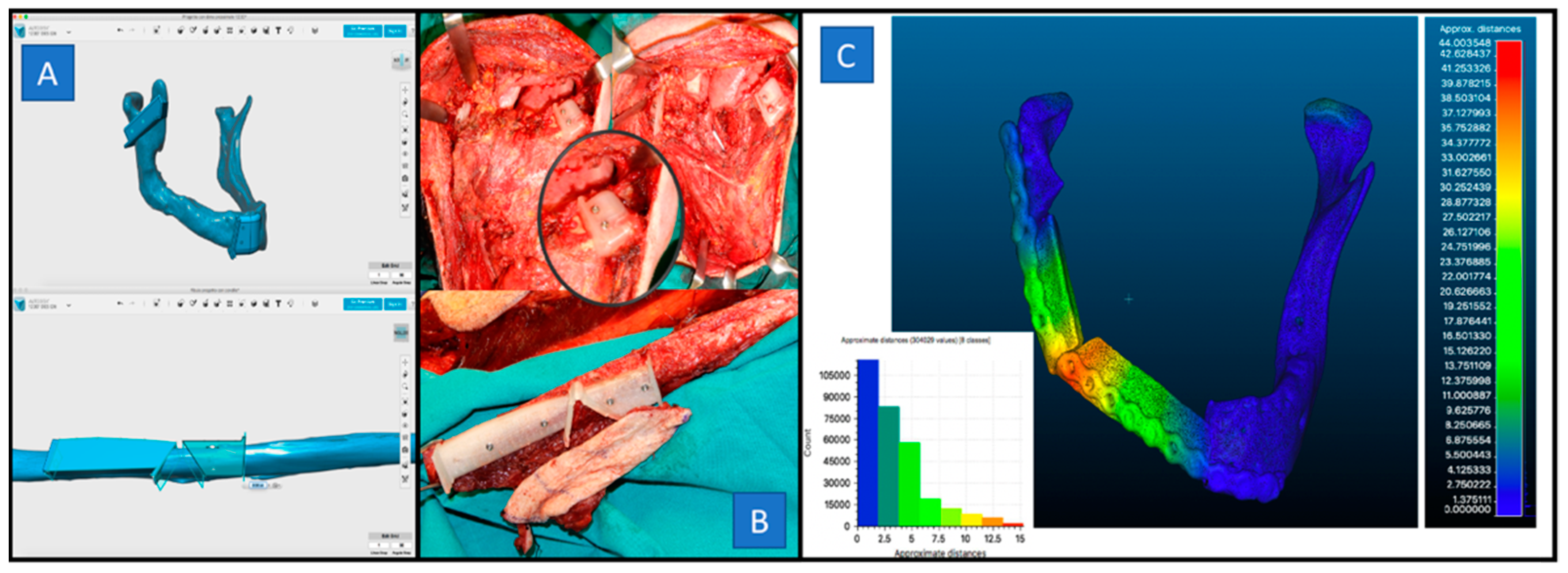
- (2)
- Design of virtual osteotomies and surgical guides. The surgical guides were molded directly on the mandibular surface in correspondence with the defined osteotomy lines under control CT recurring to the margin of oncological radicality.
- (3)
- Production of surgical guides. Virtual cutting guides for both the jaw and fibula were exported as STL files. These STL files were imported into the CURA software and optimized for an ULTIMAKER 2 3D printer. The material used was 2.85 mm Bioflex medical PLA flexible filament (polylactic acid) (ISO 10993-5: 2009).
- (4)
- Surgery. This involved a modified radical lymphadenectomy in all cases ipsilateral to the lesion. The mandibular osteotomy was performed along the flange of the guide using a surgical saw. The fibular osteotomy was performed after attaching the cutting guide on the fibula. The plates were molded manually following the outline of the segments of the fibula positioned to fill the surgical gap, as previously digitally programmed.
- B.1 Traumatology: Orbital floor fractures
- (1)
- Orbital segmentation and mirroring. The DICOM data of the specular contralateral orbit were used as a reference for the reconstruction of the bone defect.
- (2)
- Processing. Through editing tools, a virtual printing machine with inlays was created to perfectly overlap the upper and lower surfaces of the eye.
- (3)
- Slicing 3D. The virtual printing machine was exported as an STL file and optimized for the 3D jet printer extrusion with a 0.6 mm nozzle. The material used was filament 2.85 mm Bioflex medical PLA (polylactic acid) (ISO 10993-5: 2009).
- (4)
- Mesh modeling. A 0.6 mm linear titanium mesh was modeled inside the virtual mold by applying manual pressure on the press to obtain a customized device for each patient.
- (5)
- Surgery. All the patients underwent orbital floor reconstruction surgery under general anesthesia through a sub-ciliary incision. The mesh, previously shaped, was positioned to fill the surgical gap. The correct placement of the mesh was tested under the navigator control from the probe device.
- B.2 Traumatology: Zygomatic arch fractures
- (1)
- Segmentation and mirroring of the skin surface.
- (2)
- Processing. Through the “mirroring” tool, we used the contralateral zygomatic surface as a reference to develop a protective device. To ensure an adequate support for the device, we designed two slots in the upper and lower edges and two anchors in the nasal and auricular region. This volume was then exported as an STL file.
- (3)
- Slicing. The virtual device was optimized for 3D with an extrusion jet with a 0.6 mm nozzle. The material used was 2.85 mm medical PLA bioflex filament (polylactic acid) (ISO 10993-5: 2009).
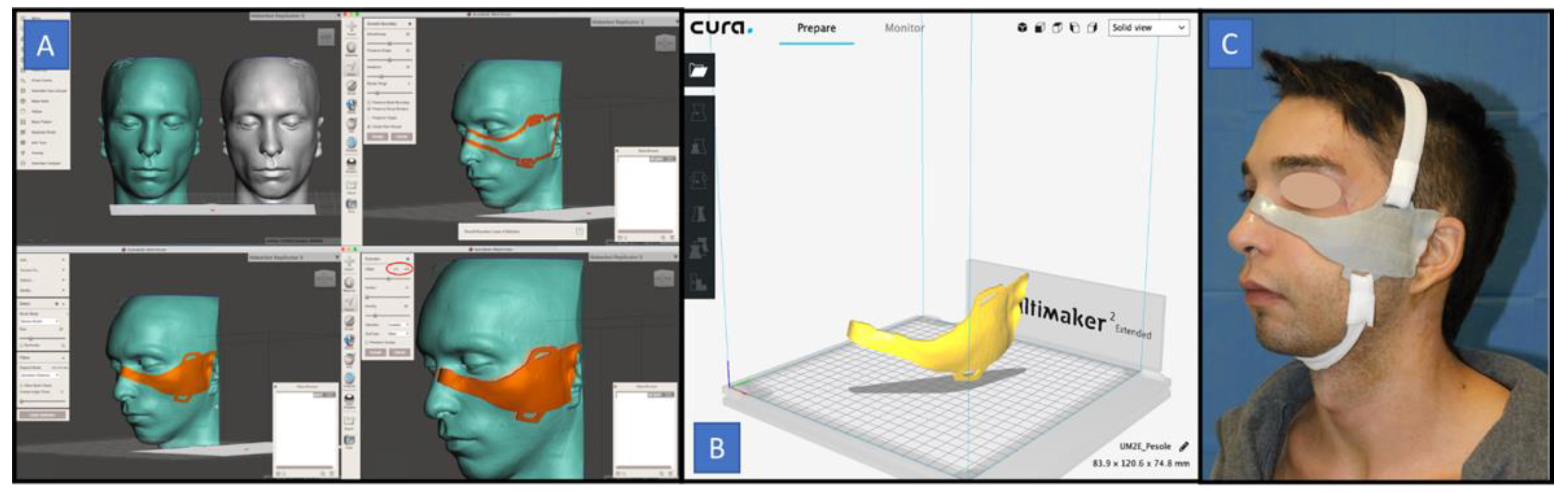
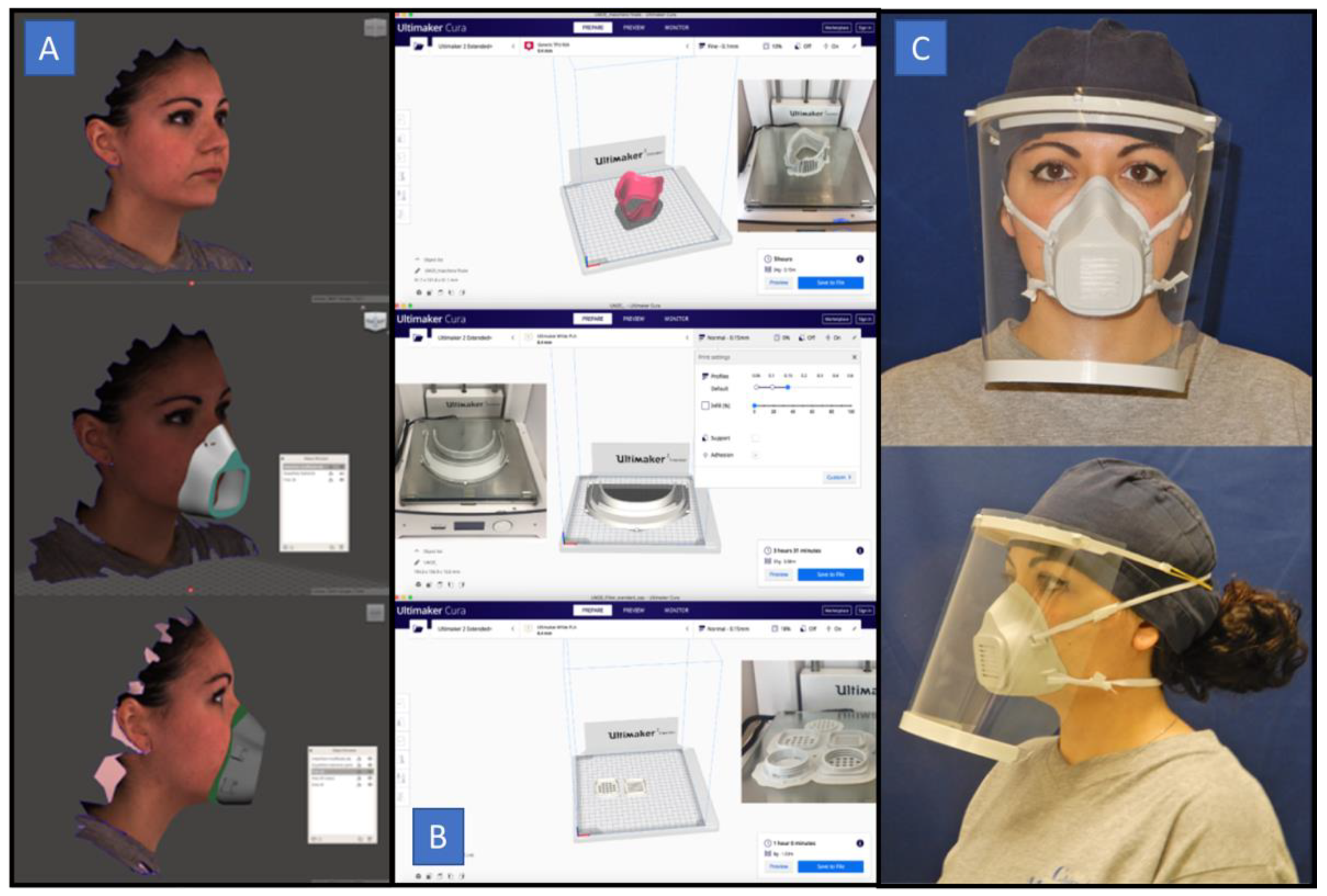
- C: The COVID-19 Pandemic: Face masks and face shields
- (1)
- Facial scanning. A facial scan was conducted using a free smartphone application (Bellus 3D, Campbell, CA, USA), obtaining an OBJ file. This application works with high-definition scanning in order to generate a ~6 MB file size (OBJ) with 60,000 triangles and a 2 K (width) color texture map. It can be used with a smartphone camera, without needing any external accessories.
- (2)
- Editing. The OBJ file was then modified with the freeware Meshmixer Software. Using this specific tool, a customized mask for each healthcare worker was designed. Finally, this project was exported as an STL file.
- (3)
- Slicing. The STL file was then imported into Ultimaker Cura to be printable on a 3D printer.
- (4)
- Printing. Three elements (a mask, filter slot, and face-shield) of the Mask3d were printed using the Ultimaker 2 Extended+ 3D printer. Two types of filament were used: thermoplastic polyurethane (TPU) (Rubber TPU D27, Bioflex, Bioalfa, Soria Vecchia, Milan, Italy) and polylactic acid (PLA) (Eco PLA, 3DJake Italia, Niceshops GmbH, Paldau, Austria). A 2.85 mm TPU filament was used for the realization of the mask. The print resolution was set to 0.1 mm (fine), using a nozzle of 0.4 mm. For the filter slot and the shield, a 2.85 mm PLA filament was used, with the resolution set to 0.15 mm, using a 0.6 mm nozzle.
3. Results
- A Reconstructive surgery
- B.1 Traumatology: Orbital floor fractures
- B.2 Traumatology: Fractures of the zygomatic arch
- C The COVID-19 Pandemic: Face masks and face shields
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Lee, K. Principles of CAD/CAM/CAE Systems; Addison-Wesley Longman Publishing Co., Inc.: Boston, MA, USA, 1999. [Google Scholar]
- Vannier, M.W.; Marsh, J.L.; Warren, J.O. Three-dimensional CT reconstruction images for craniofacial surgical planning and evaluation. Radiology 1984, 150, 179–184. [Google Scholar] [CrossRef]
- Toth, B.A.; Ellis, D.S.; Stewart, W.B. Computer-designed prostheses for orbitocranial reconstruction. Plast. Reconstr. Surg. 1988, 81, 315–324. [Google Scholar] [CrossRef] [PubMed]
- Robb, R.A. Biomedical Imaging, Visualization, and Analysis; Wiley-Liss: New York, NY, USA, 2000. [Google Scholar]
- Avraham, T.; Franco, P.; Brecht, L.E.; Ceradini, J.D.; Saadeh, P.B.; Hirsch, D.L.; Levine, J.P. Functional outcomes of virtually planned free fibula flap reconstruction of the mandible. Plast. Reconstr. Surg. 2014, 134, 628–634. [Google Scholar] [CrossRef] [PubMed]
- Toto, J.M.; Chang, E.I.; Agag, R.; Devarajan, K.; Patel, S.A.; Topham, N.S. Improved operative efficiency of free fibula flap mandible reconstruction with patient-specific, computer-guided preoperative planning. Head Neck 2015, 37, 1660–1664. [Google Scholar] [CrossRef]
- Antony, A.K.; Chen, W.F.; Kolokythas, A.; Weimer, K.A.; Cohen, M.N. Use of virtual surgery and stereolithography-guided osteotomy for mandibular reconstruction with the free fibula. Plast. Reconstr. Surg. 2011, 128, 1080–1084. [Google Scholar] [CrossRef]
- Marchetti, C.; Bianchi, A.; Mazzoni, S.; Cipriani, R.; Campobassi, A. Oromandibular reconstruction using a fibula osteocutaneous free flap: Four different “preplating” techniques. Plast. Reconstr. Surg. 2006, 118, 643–651. [Google Scholar] [CrossRef]
- Hammoudeh, J.A.; Howell, L.K.; Boutros, S.; Scott, M.A.; Urata, M.N. Current status of surgical planning for orthognathic surgery: Traditional methods versus 3D surgical planning. Plast. Reconstr. Surg. Glob. Open 2015, 3, 307–309. [Google Scholar] [CrossRef]
- Swennen, G.R. Timing of three-dimensional virtual treatment planning of orthognathic surgery: A prospective single-surgeon evaluation on 350 consecutive cases. Oral Maxillofac. Surg. Clin. N. Am. 2014, 26, 475–485. [Google Scholar] [CrossRef]
- Shaheen, E.; Sun, Y.; Jacobs, R. Three-dimensional printed final occlusal splint for orthognathic surgery: Design and validation. Int. J. Oral Maxillofac. Surg. 2017, 46, 67–71. [Google Scholar] [CrossRef]
- Steinbacher, D.M. Three-dimensional analysis and surgical planning in craniomaxillofacial surgery. J. Oral Maxillofac. Surg. 2015, 73, 40–56. [Google Scholar] [CrossRef]
- Mommaerts, M.Y.; Jans, G.; Vander Sloten, J.; Staels, P.F.; Van der Perre, G.; Gobin, R. On the assets of CAD planning for craniosynostosis surgery. J. Craniofac. Surg. 2001, 12, 547–554. [Google Scholar] [CrossRef] [PubMed]
- Doscher, M.E.; Garfein, E.S.; Bent, J.; Tepper, O.M. Neonatal mandibular distraction osteogenesis: Converting virtual surgical planning into an operative reality. Int. J. Pediatr. Otorhinolaryngol. 2014, 78, 381–384. [Google Scholar] [CrossRef] [PubMed]
- Varol, A.; Basa, S. The role of computer-aided 3D surgery and stereolithographic modelling for vector orientation in premaxillary and trans-sinusoidal maxillary distraction osteogenesis. Int. J. Med. Robot. 2009, 5, 198–206. [Google Scholar] [CrossRef] [PubMed]
- Sosin, M.; Ceradini, D.J.; Hazen, A.; Levine, J.P.; Staffenberg, D.A.; Saadeh, P.B.; Flores, R.L.; Brecht, L.E.; Bernstein, G.L.; Rodriguez, E.D. Total face, eyelids, ears, scalp, and skeletal subunit transplant cadaver simulation: The culmination of aesthetic, craniofacial, and microsurgery principles. Plast. Reconstr. Surg. 2016, 137, 1569–1581. [Google Scholar] [CrossRef]
- Sailer, H.F.; Haers, P.E.; Zollikofer, C.P.; Warnke, T.; Carls, F.R.; Stucki, P. The value of stereolithographic models for preoperative diagnosis of craniofacial deformities and planning of surgical corrections. Int. J. Oral Maxillofac. Surg. 1998, 27, 327–333. [Google Scholar] [CrossRef]
- Baker, S.B.; Goldstein, J.A.; Seruya, M. Outcomes in computer-assisted surgical simulation for orthognathic surgery. J. Craniofac. Surg. 2012, 23, 509–513. [Google Scholar] [CrossRef]
- Edwards, S.P. Computer-assisted craniomaxillofacial surgery. Oral Maxillofac. Surg. Clin. N. Am. 2010, 22, 117–134. [Google Scholar] [CrossRef]
- Hsu, S.S.-P.; Gateno, J.; Bell, R.B.; Hirsch, D.L.; Markiewicz, M.R.; Teichgraeber, J.F.; Zhou, X.; Xia, J.J. Accuracy of a Computer-Aided Surgical Simulation Protocol for Orthognathic Surgery: A Prospective Multicenter Study. J. Oral Maxillofac. Surg. 2013, 71, 128–142. [Google Scholar] [CrossRef] [Green Version]
- Li, B.; Zhang, L.; Sun, H.; Yuan, J.; Shen, S.G.; Wang, X. A novel method of computer aided orthognathic surgery using individual CAD/CAM templates: A combination of osteotomy and reposi- tioning guides. Br. J. Oral Maxillofac. Surg. 2013, 51, e239–e244. [Google Scholar] [CrossRef]
- Mazzoni, S.; Bianchi, A.; Schiariti, G.; Badiali, G.; Marchetti, C. Computer-aided design and computer-aided manufacturing cutting guides and customized titanium plates are useful in upper maxilla waferless repositioning. J. Oral Maxillofac. Surg. Off. J. Am. Assoc. Oral Maxillofac. Surg. 2015, 73, 701–707. [Google Scholar] [CrossRef]
- Hanasono, M.M.; Skoracki, R.J. Computer-assisted design and rapid prototype modeling in microvascular mandible reconstruction. Laryngoscope 2013, 4, 597–604. [Google Scholar] [CrossRef] [PubMed]
- Ayoub, N.; Ghassemi, A.; Rana, M.; Gerressen, M.; Riediger, D.; Hölzle, F.; Modabber, A. Evaluation of computer-assisted mandibular reconstruction with vascularized iliac crest bone graft compared to conventional surgery: A randomized prospective clinical trial. Trials 2014, 1, 114–118. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dell’Aversana Orabona, G.; Abbate, V.; Maglitto, F.; Bonavolontà, P.; Salzano, G.; Romano, A.; Reccia, A.; Committeri, U.; Iaconetta, G.; Califano, L. Low-cost, self-made CAD/CAM-guiding system for mandibular reconstruction. Surg. Oncol. 2018, 27, 200–207. [Google Scholar] [CrossRef] [PubMed]
- Dell’Aversana Orabona, G.; Abbate, V.; Maglitto, F.; Committeri, U.; Improta, G.; Bonavolontà, P.; Reccia, A.; Somma, T.; Iaconetta, G.; Califano, L. Postoperative Management of Zygomatic Arch Fractures: In-House Rapid Prototyping System for the Manufacture of Protective Facial Shields. J. Craniofac. Surg. 2019, 30, 2057–2060. [Google Scholar] [CrossRef]
- Belli, E.; Liberatore, G.; Elidon, M.; Dell’Aversana Orabona, G.; Piombino, P.; Maglitto, F.; Catalfamo, L.; De Riu, G. Surgical evolution in the treatment of mandibular condyle fractures. BMC Surg. 2015, 8, 1–6. [Google Scholar]
- Cascone, P.; Petrucci, B.; Ramieri, V.; Marianetti, T.M. Security Hi-tech Individual Extra-light Device Mask: A new protection for [soccer] players. J. Craniofac. Surg. 2008, 19, 772–776. [Google Scholar] [CrossRef]
- Heise, M.; Eufinger, H.; Rarreck, T. Individualized facial protection after fracture Management of the nasal bone and zygomatic arch in professional soccer players. Mund Kiefer Gesichtschir. 2001, 5, 320–322. [Google Scholar] [CrossRef]
- Chang, E.I.; Jenkins, M.P.; Patel, S.A.; Topham, N.S. Long-term operative outcomes of preoperative computed tomography-guided virtual surgical planning for osteocutaneous free flap mandible reconstruction. Plast. Reconstr. Surg. 2016, 137, 619–623. [Google Scholar] [CrossRef]
- Pucci, R.; Weyh, A.; Smotherman, C.; Valentini, V.; Bunnell, A.; Fernandes, R. Fernandes: Accuracy of virtual planned surgery versus conventional free-hand surgery for reconstruction of the mandible with osteocutaneous free flaps. Int. J. Oral Maxillofac. Surg. 2019, 49, 1153–1161. [Google Scholar] [CrossRef]
- Zhang, L.; Liu, Z.; Li, B.; Yu, H.; Shen, S.G.; Wang, X. Evaluation of computer-assisted mandibular reconstruction with vascular- ized fibular flap compared to conventional surgery. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2016, 121, 139–148. [Google Scholar] [CrossRef]
- Wilde, F.; Hanken, H.; Probst, F.; Schramm, A.; Heiland, M.; Cornelius, C.P. Multicenter study on the use of patient-specific CAD/CAM reconstruction plates for mandibular reconstruction. Int. J. Comput. Assist. Radiol. Surg. 2015, 10, 2035–2051. [Google Scholar] [CrossRef] [PubMed]
- Bosc, R.; Hersant, B.; Carloni, R.; Niddam, J.; Bouhassira, J.; De Kermadec, H.; Bequignon, E.; Wojcik, T.; Julieron, M.; Meningaud, J.P. Mandibular reconstruction after cancer: An in-house approach to manufacturing cutting guides. Int. J. Oral Maxillofac. Surg. 2017, 46, 24–31. [Google Scholar] [CrossRef] [PubMed]
- Ibrahim, D.; Broilo, T.L.; Heitz, C.; de Oliveira, M.G.; de Oliveira, H.W.; Nobre, S.M.; Dos Santos Filho, J.H.; Silva, D.N. Dimensional error of selective laser sintering, three-dimensional printing and PolyJet models in the reproduction of mandibular anatomy. J. Craniomaxillofac. Surg. 2009, 37, 167–173. [Google Scholar] [CrossRef] [PubMed]
- Choi, J.Y.; Choi, J.H.; Kim, N.K.; Kim, Y.; Lee, J.K.; Kim, M.K.; Lee, J.H.; Kim, M.J. Analysis of errors in medical rapid prototyping models. Int. J. Oral Maxillofac. Surg. 2002, 31, 23–32. [Google Scholar] [CrossRef] [PubMed]
- Ghai, S.; Sharma, Y.; Jain, N.; Satpathy, M.; Pillai, A.K. Use of 3-D printing technologies in craniomaxillofacial surgery: A review. J. Oral Maxillofac. Surg. 2018, 22, 249–259. [Google Scholar] [CrossRef]
- Beliakin, S.A.; Khyshov, V.B.; Khyshov, M.B. Reconstruction of post-traumatic skull and facial bones injuries with the use of perforated titanium plates and meshes. Voen Med. Zh. 2012, 333, 12–17. [Google Scholar]
- Chen, S.T.; Chang, C.J.; Su, W.C. 3-D titanium mesh reconstruction of defective skull after frontal craniectomy in traumatic brain injury. Injury 2015, 46, 80–85. [Google Scholar] [CrossRef]
- Pertile, D.; Gallo, G.; Barra, F.; Pasculli, A.; Batistotti, P.; Sparavigna, M.; Vizzielli, G.; Soriero, D.; Graziano, G.; Di Saverio, S.; et al. The impact of COVID-19 pandemic on surgical residency programmes in Italy: A nationwide analysis on behalf of the Italian Polyspecialistic Young Surgeons Society (SPIGC). Updates Surg. 2020, 72, 269–280. [Google Scholar] [CrossRef]
- Maglitto, F.; Salzano, G.; Vaira, L.A.; Salzano, F.A.; De Riu, G. Anosmia: A COVID-19 symptom that must be investigated by rhinoplasty surgeons. Eur. J. Plast. Surg. 2020, 13, 1–2. [Google Scholar] [CrossRef]
- Piedra-Cascón, W.; Meyer, M.J.; Methani, M.M.; Revilla-León, M. Accuracy (trueness and precision) of a dual-structured light facial scanner and interexaminer reliability. J. Prosthet. Dent. 2020, 124, 567–574. [Google Scholar]
- Piombino, P.; Committeri, U.; Norino, G.; Vaira, L.A.; Troise, S.; Maglitto, F.; Mariniello, D.; De Riu, G.; Califano, L. Facing COVID-19 pandemic: Development of custom-made face mask with rapid prototyping system. J. Infect. Dev. Ctries. in press. [CrossRef]
- Swennen, G.R.; Pottel, L.; Haers, P.E. Custom-made 3D-printed face masks in case of pandemic crisis situations with a lack of commercially available FFP2/3 masks. Int. J. Oral Maxillofac. Surg. 2020, 49, 673–677. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Our experience in CAD/CAM applications in Maxillofacial Surgery | ||
|---|---|---|
| Ordinary activities | ||
| Application field | Specific application | Cases |
| Reconstructive surgery | Cutting-guide | 4 |
| Traumatology | Orbital mesh conformer | 9 |
| Zygomatic shield | 16 | |
| Extraordinary activities | ||
| Application field | Specific application | Cases |
| Covid-19 pandemic | Ffp2-n95 face mask | 6 |
| Covid-19 face shield | 6 | |
| Author | Year of Publication | Kind of Study | Population | Application Field | 3D Application |
|---|---|---|---|---|---|
| Mommaerts MY | 2001 | Retrospective study | 2 | Malformative | Planning for malformative surgery |
| Heise M | 2001 | Technical notes and review | 2 | Traumatological surgery | Protective facial shield |
| Marchetti C | 2006 | Retrospective study | 18 | Reconstructive surgery | Free fibula flap mandible reconstruction |
| Cascone P | 2008 | Technical notes and review | 1 | Traumatological surgery | Protective facial shield |
| Varol A | 2009 | Retrospective study | 5 | Osteodistraction | Planning for osteodistraction surgery |
| Edwards SP | 2010 | Systematic review | / | Imaging, reconstructive surgery, malformation surgery, orthognathic surgery, osteodistraction | Surgical planning in maxillofacial surgery |
| Antony AK | 2011 | Technical notes and review | 5 | Reconstructive surgery | Free fibula flap mandible reconstruction |
| Baker SB | 2012 | Retrospective study | 11 | Orthognathic surgery | Planning for orthognathic surgery |
| Beliakin SA | 2012 | Technical notes and review | 1 | Traumatological surgery | Virtual surgical planning |
| Doscher ME | 2013 | Retrospective study | 1 | Osteodistraction | Planning for osteodistraction surgery |
| Hsu SS | 2013 | Retrospective study | 65 | Orthognathic surgery | Planning for orthognathic surgery |
| Hanasono MM | 2013 | Retrospective study | 38 | Reconstructive surgery | Virtual surgical planning |
| Avraham T | 2014 | Retrospective review | 52 | Reconstructive surgery | Free fibula flap mandible reconstruction |
| Swennen GR | 2014 | Retrospective study | 350 | Orthognathic surgery | Planning for orthognathic surgery |
| Robdy KA | 2014 | Systematic review | / | Reconstructive surgery | Virtual surgical planning |
| Ayoub N | 2014 | Retrospective study | 20 | Reconstructive surgery | Iliac crest bone flap mandible reconstruction |
| Toto JM | 2015 | Retrospective review | 57 | Reconstructive surgery | Free fibula flap mandible reconstruction |
| Hammoudeh JA | 2015 | Systematic review | / | Orthognathic surgery | Planning for orthognathic surgery |
| Steinbacher DM | 2015 | Retrospective study | 6 | Reconstructive surgery, malformation surgery, orthognathic surgery, osteodistraction | Surgical planning in maxillofacial surgery |
| Mendez BM | 2015 | Retrospective study | 2 | Reconstructive surgery | Virtual surgical planning |
| Wilde F | 2015 | Retrospective study | 30 | Reconstructive surgery | Free fibula flap mandible reconstruction |
| Chen ST | 2015 | Retrospective study | 7 | Traumatological surgery | Virtual surgical planning |
| Chang EI | 2016 | Technical notes and review | 1 | Reconstructive surgery | Free fibula flap mandible reconstruction |
| Resnick | 2016 | Retrospective study | 43 | Orthognathic surgery | Planning for orthognathic surgery |
| Shaheen E | 2017 | Retrospective study | 20 | Orthognathic surgery | Planning for orthognathic surgery |
| Bosc R | 2017 | Retrospective study | 18 | Reconstructive surgery | Cutting guide VPS mandible reconstruction |
| Swennen GR | 2020 | Technical notes and review | 1 | COVID-19 Mask | 3D-printed mask |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Maglitto, F.; Dell’Aversana Orabona, G.; Committeri, U.; Salzano, G.; De Fazio, G.R.; Vaira, L.A.; Abbate, V.; Bonavolontà, P.; Piombino, P.; Califano, L. Virtual Surgical Planning and the “In-House” Rapid Prototyping Technique in Maxillofacial Surgery: The Current Situation and Future Perspectives. Appl. Sci. 2021, 11, 1009. https://0-doi-org.brum.beds.ac.uk/10.3390/app11031009
Maglitto F, Dell’Aversana Orabona G, Committeri U, Salzano G, De Fazio GR, Vaira LA, Abbate V, Bonavolontà P, Piombino P, Califano L. Virtual Surgical Planning and the “In-House” Rapid Prototyping Technique in Maxillofacial Surgery: The Current Situation and Future Perspectives. Applied Sciences. 2021; 11(3):1009. https://0-doi-org.brum.beds.ac.uk/10.3390/app11031009
Chicago/Turabian StyleMaglitto, Fabio, Giovanni Dell’Aversana Orabona, Umberto Committeri, Giovanni Salzano, Gianluca Renato De Fazio, Luigi Angelo Vaira, Vincenzo Abbate, Paola Bonavolontà, Pasquale Piombino, and Luigi Califano. 2021. "Virtual Surgical Planning and the “In-House” Rapid Prototyping Technique in Maxillofacial Surgery: The Current Situation and Future Perspectives" Applied Sciences 11, no. 3: 1009. https://0-doi-org.brum.beds.ac.uk/10.3390/app11031009